Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
204 Cards in this Set
- Front
- Back
|
causes of acute pancreatitis? (3)
|
1. pancreatic obstruction (gallstones)
2. drugs (etoh) 3. hypertrigliceremia |
|
|
what drugs can cause pancreatitis? (5)
|
1. azathioprine (imuran)-immunosupressant to tx ra
2. didanisine (ddl)-HIV 3. furosemide 4. ACE-I 5. estrogen |
|
|
epigastric pain radiating to the mid-back, n/v
|
acute pancreatitis
|
|

ecchymoses on the flanks from necrotizing pancreatitis
|
grey turner's sign
|
|

periumbilical ecchymoses
|
cullen's sign
|
|
|
diagnostic procedure that increases the risk of acute pancreatitis
|
ERCP
|
|
|
alcoholic pt with epigastric pain initially improves but then gets worse, septic, leukocytosis and positive blood cultures
|
pancreatic necrosis
|
|
|
tx for pancreatic necrosis
|
ct guided fluid aspiration
abx: imipenem, quinolones and flagyl |
|
|
systemic complications of acute pancreatitis
|
renal failure from hypovolemia
respiratory failure from ARDS |
|
|
major cause of chronic pancreatitis
|
etoh
|
|
|
abdominal pain, weight loss, steatorrhea, diabetes
|
chronic pancreatitis
|
|
|
tests to dx chronic pancreatitis
|
72 hour fecal fat
secretin stimulation test |
|
|
most sensitive and specific test to dx chronic pancreatitis
|
ERCP
|
|
|
Most common pancreas neoplasm
|
ductal adenocarcinoma
|
|
|
epigastric pain, obstructive jaundice and weight loss
|
ductal adenocarcinoma of the pancreas
|
|
|
tumor markers elevated in pancreatic ca
|
ca 19-9 and CEA
|
|
|
most common causes of infectious esophagitis
|
cmv
hsv candida |
|
|
pt presents with weight loss, dysphagia and upper gi bleeding
|
esophagitis
|
|

on barium swallow, a flat large ulcer with satellite ulcers nearby
|
cmv esophagitis
|
|
|
on barium swallow, volcanic ulcers
|
hsv esophagitis
|
|

on barium swallow, "shaggy" mucosa
|
candida esophagitis
|
|
|
tx for candida esophagitis in AIDS and non-AIDS pts
|
AIDS= fluconazole po or iv
non-AIDS= nystatin or clotrimazole po |
|
|
tx for refractory hsv esphagitis
|
forscarnet (foscavir) iv
|
|
|
medications that can cause esophagitis (7)
|
NSAIDS
tetracyclines Fe K vit C supplements alendronate quinidine |
|
|
pt presents with trouble swallowing both fluids and solids, nasal regurgitation and coughing when swallowing. dx?
|
oropharyngeal dysphagia. seen after stroke, in parkinson's, als, ms and mg
|
|
|
test of choice to dx oropharyngeal dysphagia
|
barium swallow w/ video-fluoroscopy
|
|
|
causes of esophageal dysphagia (3)
|
ca
strictures schatzki's ring |
|
|
narrowing of the grastro-esophageal junction w/ mucosal or muscular tissue
|

schatski's ring
|
|
|
pt presents w/ dysphagia only with solids
|
strictures
|
|
|
most common esophageal motor disorder
|
achalasia
|
|
|
bird's beak on barium swallow
|
achalasia
|
|
|
pt presents w/ dysphagia w/ solids and liquids of sudden onset and weight loss. what's the dx tests of choice?
|
Barium swallow and esophageal manometry
|
|
|
tx for achalasia
|
nifedipine before meals
botox injection pneumatic dilation |
|
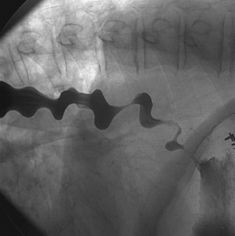
corkscrew appearance in the barium swallow
|
diffuse esophageal spasm
|
|
|
test of choice to dx mallory-weiss tears
|
endoscopy
|
|
|
thermal coagulation can be used to treat mallory-weiss tears. in which pt would this be contraindicated?
|
esophageal varices and portal htn
|
|
|
pt presents with chest pain, anorexia, weight loss, odynophagia w/ solids that developed to liquids later
|
esophageal ca: adeno or squamous
|
|
|
which esophageal ca is not sensitive to rxt
|
adenocarcinoma
|
|
|
female pt w/ iron def anemia presents w/ solid dysphagia. most likely dx?
|
cervical esophageal webs
|
|
|
tx for esophageal varices
|
adh iv
nitro iv ocreotide iv balloon tamponade endoscopic hemostasis (toc) variceal band ligation |
|
|
xrt and achalasia are risk factors for what type of esophageal ca?
|
squamous cell ca
|
|
|
gold standard test to dx gerd
|
ph monitoring
|
|
|
test that establishes gerd as cause of reflux sx
|
Bernstein's test
|
|
|
life style modifications for pts w/ gerd
|
1. no eating at bed time
2. no fatty, spicy foods, coffee, orange juice, sodas and tea 3. eat smaller meals 4. elevated bed 6 inches 5. stop etoh and smoking |
|
|
mechanism of action of antiacids w/ some drugs names
|
hcl buffering and increase in les pressure
ie. mylanta, maalox, tums... |
|
|
this drug group increases les pressure and gastric emptying. give some names
|
prokinetics
ie. bethanechol (urecholine)(muscarinic agonist) metoclopramide (reglan) |
|
|
name some ppis
|
omeprazole (prilosec)
lansoprazole (prevacid) pantoprazole (protonix) rabeprazole (aciphex) |
|
|
complication of autoimmune gastritis
|
pernicious anemia
|
|
|
tx for h.pylori gastritis
|
ppi + clarithromycin (resistant gets levaquin) + amoxicillin( pen allergic gets flagyl)
can add pepto or kaopectate |
|
|
blood group at risk for stomach ca
|
group A
|
|
|
pt feels bloated, dysphagia, early satiety think...
|
stomach ca
|
|
|
lymph nodes involved in metastatic ca of the stomach
|
left supraclavicular (virchow's node)
periumbilical (sister marie-joseph node) |
|
|
medical tx for stomach ca
|
chemo and radiation
rxt alone is ineffective |
|
|
peptic ulcer dz caused by a gastrinoma
|
zollinger-ellison syndrome
|
|
|
pt presents with diarrhea, gastrin releasing tumors in pancreas and duodenum
|
zollinger-ellison syndrome
|
|
|
which type of ulcer presents w/ n/v, weight loss, and doesnt relieve w/ food
|
gastric ulcer
|
|
|
which ulcer presents w/ nocturnal epigastric pain, episodic pain that gets better w/ food
|
duodenal ulcer
|
|
|
which type of ulcer requires bx due to risk of malignancy
|
gastric ulcers
|
|
|
most common cause of upper gi bleeding
|
pud
|
|
|
us finding highly specific for acute cholecystitis
|
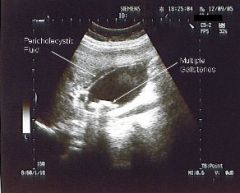
pericholecystic fluid
|
|
|
nonsurgical tx for cholelithiasis
|
Ursodeoxycholic acid (ursodiol)
|
|
|
nonsurgical tx for cholelithiasis is ineffective in which type of stones
|
pigmented or bigger than 1.5 cm
|
|
|
test to assess gallbladder fnx
|

oral cholecystography
|
|
|
types of gallbladder stones
|
cholesterol
pigmented |
|
|
in this phase the hepatitis virus can be detected but the labs are normal and there are no sx
|
incubation period
|
|
|
in which phase of hepatitis infection pt presents w/ nausea, anorexia, vague abdominal pain and labs show specific antibodies and elevated liver enzymes
|
pre-icteric phase
|
|
|
in this phase of hepatitis infection liver enzymes peak at ten times the normal levels, there's light colored stools and dark urine
|
icteric phase
|
|
|
type of hepatitis seen only in the presence of hepatitis B
|
hepatitis D
|
|
|
tx for hep C
|
pegylated interferon-alpha
ribavirin |
|
|
test to screen chronic hepatitis due to wilson's dz
|
ceruloplasmin (most important copper carrier enzyme)
|
|
|
nucleoside analogues for the tx of hep B
|
lamivudine (zeffix,epivir)
adefovir dipivoxil (hepsera) |
|
|
most common malignant tumors of the liver
|
gi, lung and breast metastatic tumors
|
|
|
most common primary malignancy of the liver
|
hepatocellular ca
|
|
|
causes of hepatocellular ca (3)
|
etoh
hep C hemochromatosis |
|
|
marker elevated in hepatocellular ca
|
alpha-feto protein
|
|
|
autosomal recessive disorder presents w/ copd and cirrhosis
|
alpha-1-antitrypsin deficiency
|
|
|
tx for wilson's dz
|
copper chelation with
penicillamine |
|
|
labs in hemochromatosis
|
high ferritin
high hepatic iron index |
|
|
tx for hemochromatosis
|
iron chelation w/ deferoxamine
phlebotomy |
|
|
bilirubin metabolism disorder that responds to phenobarbital
|
crigler-najjar syndrome type 2
|
|
|
what differentiates rotor syndrome from dubin-johnson syndrome
|
there's no liver pigmentation
gallbladder can be visualized |
|
|
ramson's criteria for pancreatitis on admission
|
1. a pt older than 55 yo with
wbc count over 16,000 2. ast over 250 3. ldh over 350 4. glucose over 200 |
|
|
what's the use of the ramson's criteria?
|
determine the severity and clinical complications of the pancreatitis
3 or more criteria met predicts a complicated course of illness |
|
|
in which type of pt care must be taken when administering Mg OH as tx for constipation?
|
renal failure pt. can lead to hypermagnesemia
|
|
|
lactulose and sorbitol are...?
|
nonabsorbable sugar laxatives
|
|
|
what pts taking nonabsorbable sugar laxatives should be warned of?
|
1. it'll take 3 h for med to cause an effect
2. cramping and bloating can be noted |
|
|
possible complication when taking mineral oil
|
aspiration pneumonitis
|
|
|
name two emollient laxatives
|
docusate (colace)
mineral oil (petrollatum) |
|
|
name two stimulant laxatives and their use
|
senna
bisacodyl (Dulcolax, Alophen) - use to tx acute constipation |
|
|
time of stimulant laxative effect w/ oral administration vs rectal
|
oral takes 12 h
rectal takes 1 h |
|
|
condition caused by the vasa recta penetrating the circular muscle layers between the taenia coli
|
diverticulosis
|
|
|
sawtooth pattern seen on barium enema
|
diverticulitis w/ spasms
|
|
|
brigth red painless bleeding per rectum
|
diverticular hemorrhage (50% of lower GI bleeds)
|
|
|
condition affecting pts in the 15-25 and 55-65 age groups, it presents w/ fecal incontinence or urgency and bloody diarrhea
|
ulcerative colitis
|
|
|
extraperitoneal manifestations of ulcerative colitis (5)
|
1. ankylosing spondylitis
2. sclerosing cholangitis 3. pyoderma gangrenosum 4. erythema nodosum 5. liver dz |
|
|
loss of haustra markings, narrowing of the lumen and straightening of the colon. dx?
|
ulcerative colitis
|
|
|
name the most common aminosalicylates
|
sulfasalazine (Azulfidine)
olsalazine (Dipentum) mesalamine (Asacol) balsalazide (Colazal) |
|
|
pts in 15-25 or 55-65 age groups presenting w/ abdominal pain, weight loss, nonbloody diarrhea and aphtous ulcers in the mucosa suspect...
|
chron's dz
|
|
|
immunosupressant drugs shown to be effective in chron's dz
|
azathioprine (Imuran)
6-mercaptoprine (Purinethol) |
|
|
tx for chron's dz for pts who have failed immunomodulators like Imuran and Purinethol
|
tnf antagonists: Infliximab
|
|
|
criteria for the dx of IBS
|
3 months of:
1. abdominal pain relieved by defecation 2. changes in frequency and consistency 3. bloating or distension of the abdomen |
|
|
structures supplied by the celiac trunk
|
1. liver and biliary tract
2. spleen 3. stomach 4. duodenum 5. pancreas |
|
|
structures supplied by the SMA
|
1. lower part of duodenum, ileum and jejunum
2. head of the pancreas 3. ascending colon 4. part of transverse colon |
|
|
structures supplied by the IMA
|
the rest of the colon from transverse and rectum
|
|

pt w/ hx of CAD presents w/ abdominal pain. labs show leukocytosis, metabolic acidosis and high amylase and cxr show thumbprinting pattern. dx?
|
arterial mesenteric ischemia
|
|
|
most common ischemic injury of the GI tract
|
ischemic colitis
|
|
|
test for carbohydrate malabsorption
|
d-Xylose test. suggests mucosal dysfunction
|
|
|
malabsorption disorder where there's antigliadin and antiendomysial antibodies
|
celiac sprue
|
|
|
most prevalent cancer of the large intestine
|
adenocarcinoma
|
|
|
syndrome which predisposes to colon ca w/ mucocutaneous pigmentation and hamartomas
|
Peutz-Jeghers syndrome
|
|
|
syndrome that predisposes to colon ca w/ the following characteristics: supernumerary teeth, cotton-wool appearance of the jaws from osteomas, and numerous colon polyps
|
gardner's syndrome
|
|
|
explain colorectal ca screening
|
1. fobt every year
2. flexible sigmoidoscy every 5 years 3. colonoscopy every 10 years (5 for high risk pts) |
|
|
condition caused by a split in the anoderm
|
anal fissure
|
|
|
pt presents w/ pain with defecation and has seen blood on the toilet paper. on pe there's a linear tear w/ an white ulcerated base. dx?
|

|
|
|
tx for an anal fissure that doesnt improve w/ medical tx?
|
internal anal sphincterotomy
|
|
|
tender mass palpable externally on the perianal area caused by infected anal glands
|
anal fistula
|
|
|
hollow tract lined with granulation tissue connecting a primary opening inside the anal canal to a secondary opening in the perianal skin
|

fistula-in-ano
|
|
|
hemorrhoids arising above dentate line
|
internal
|
|
|
hemorrhoids arising below dentate line
|
external
|
|
|
degrees of internal hemorrhoids
|
1- only bleeding
2- bleeding and prolapse that reduces by itself 3- bleeding and prolapse that requires manual reduction 4- bleeding with incarceration that cannot be reduced |
|
|
anal mucous discharge, rectal fullness and no pain
|
internal hemorrhoids
|
|
|
severe rectal pain with perianal mass
|
external hemorrhoids
|
|
|
risk factors for anal neoplasms
|
1. smoking
2. pelvic ca 3. warts |
|
|
anal ca located at the anal canal
|
epidermoid ca
|
|
|
rectal mass, bleeding, pain, discharge, itching, and tenesmus
|
anal ca
|
|
|
when polyps are noted in the colon, follow up should be...
|
colonoscopy q 3 y or less
|
|
|
type of esophageal hernia where pt is usually asx
|
paraesophageal hernia
|
|
|
most effective surgery to tx hiatal hernia
|

nissen fundoplication
|
|
|
inguinal hernias that present in the first year of life
|
indirect
|
|
|
pathophysiology of direct inguinal hernia
|
weakness of transversalis fascia in hesselback's triangle
|
|
|
boundaries of the hesselbach's triangle
|
medially: rectus abdominis
superior and laterally: epigastric vessels inferiorly: inguinal ligament |
|
|
other name for inguinal ligament
|
poupart's ligament
|
|
|
hernia that usually descends to the scrotum and is hard to reduce
|
indirect
|
|
|
hernia that usually bulges when standing and reduces when supine
|
direct
|
|
|
hernias that tend to incarcerate or strangulate more
|
indirect
|
|
|
small volume bloody diarrhea, fecal urgency and lower abdominal pain
|
inflammatory diarrhea
|
|
|
large volume watery diarrhea, n/v and upper abdominal pain
|
non-inflammatory diarrhea
|
|
|
pt develops nausea, vomiting, abdominal pain and diarrhea within six hours of eating eggs with mayonnaise. what's the culprit?
|
staph aureus
|
|
|
pt eats fried rice stored in the fridge for 2 days and develops vomit and diarrhea. what's the culprit?
|
bacillus cereus
|
|
|
pt eats canned meat and develops diarrhea and epigastric pain. what's the culprit?
|
clostridium botulinum
|
|
|
rice water stools diarrhea
|
vibrio cholerae
|
|
|
drug of choice for cholera
|
tetracyclines
|
|
|
4 y/o pt has small volume bloody diarrhea after eating chicken at the day care. what's the culprit?
|
shigella species
|
|
|
tx for diarrhea due to shigella species
|
ceftriaxone
quinolones x 5 days for hiv + |
|
|
diarrhea caused from eating poultry, eggs and reptiles
|
salmonella
|
|
|
three bugs associated with diarrhea after eating chicken
|
shigella
salmonella campylobacter |
|
|
tx for salmonella
|
3rd gen cephs
quinolones |
|
|
tx for severe cases of campylobacter infection
|
erythromycin
|
|
|
pt ate undercooked beef and develops diarrhea, pain and vomiting. what's the culprit and what precautions should be taken regarding tx?
|
entero-hemorrhagic E. Coli 0157:H7
antibiotics can lead to HUS |
|
|
watery diarrhea in an HIV pt. what's the culprit?
|
Cryptosporidium parvum
|
|
|
when should antimotilic agents should be avoided?
|
fever and bloody diarrhea
|
|
|
mention two common antimotilic agents
|
diphenoxylate (lomotil)
loperamide (imodium) |
|
|
most common cause of nosocomial diarrhea
|
c. difficile
|
|
|
diarrhea after course of antibiotics
|
c. diffile pseudomembranous colitis
|
|
|
niacin B3 deficiency causes...
|
pellagra
|
|
|
3 D's of pellagra
|
diarrhea
dermatitis dementia |
|
|
condition caused by B1/ thiamine deficiency
|
beriberi
|
|
|
irregular heart rate, pain in the limbs, wernicke's encephalopathy due to vitamin deficiency
|
beriberi from vit B1 deficiency
|
|
|
vitamin that's teratogenic in early pregnancy
|
vit A
|
|
|
vit A toxicity results in...
|
hepatocellular necrosis
increased ICP |
|
|
B2/riboflavin deficiency causes...
|
cheilosis
glossitis stomatitis |
|
|
mention 4 common h2 blockers
|
1. cimetidine (tagamet)
2. ranitidine (zantac) 3. famotidine (pepcid) 4. nizatidine (axid) |
|
|
prostaglandin e1 analog used in the tx of nsaids ulcers and contraindicated in pregnancy
|
misoprostol (cytotec)
|
|
|
drug contraindicated to use with sucralfate
|
h2 blocker
|
|
|
ramsom's criteria after 48 h (5)
|
1. > 10% hematocrit drop
2. > 5 bun increase 3.Pao2 drop of more than 60 mmhg 4. more than 4 base deficit 5. more than 6 l of sequestrated fluid |
|
|
Nonprogressive, episodic dysphagia to only solids, coined "steakhouse syndrome",
|
SCHAZTKI RING
|
|
|
Keratin deposits in the eye due to vit A def
|
BITOT'S SPOTS
|
|
|
Which vitamin deficiency causes xerophthalmia, night blindness and acne
|
VIT A DEF.
|
|
|
Which vitamin def. causes fragile RBCS along with peripheral neuropathy
|
VIT E
|
|
|
Which def. causes decreased smell and taste senses
|
ZINC DEF.
|
|
|
Most common cause of infectious diarrhea
|
CAMPYLOBACTER JEJUNI
|
|
|
Most common cause of viral diarrhea in adults
|
NOROVIRUS
|
|
|
Most common cause of viral diarrhea in childs
|
ROTAVIRUS
|
|
|
Inverted U on xrays of the abdomen
|
VOLVULUS
|
|
|
Meckel's diverticulum inside a hernia
|
LITTRE'S HERNIA
|
|
|
EEEK bugs of cholecystitis
|
E.COLI
ENTEROBACTER ENTEROCOCCUS KLEBSIELLA |
|
|
Most common site of volvulus
|
SIGMOID COLON
|
|
|
Weight loss, post-prandial abdominal pain and abdominal bruit
|
MESENTERIC ISCHEMIA
|
|
|
Almond scented breath
|
CYANIDE POISONING
|
|
|
Medication that would alter a h. pylori breath test
|
PPI FALSE NEG
|
|
|
Medical term for gas in the bowel wall
|
PNEUMATOSIS INTESTINALIS
|
|
|
Most common cause of esophageal rupture
|
ESOPHAGOSCOPY
|
|
|
Retrosternal pain w/ evidence of air in the mediastanum
|
ESOPHAGEAL RUPTURE
|
|
|
Diagnostic test to reveal an esophageal tear
|
CONTRAST ESOPHAGOGRAM W/ GASTROGRAFIN
|
|
|
This contrast agent is used in pts allergic to barium or when it's contraindicated, contains iodine and kills tapeworms
|
GASTROGRAFIN
|
|
|
Xray reveal air in the retroperitoneal space after blunt trauma to the abdomen. Dx?
|
RUPTURE OF THE SECOND PART OF THE DUODENUM
|
|
|
RLQ pain elicited by voluntary coughing suggestive of peritoneal inflammation in appendicitis
|
DUNPHY'S SIGN
|
|
|
RLQ pain elicited by landing on heels from standing position 74% sensitive for appendicitis
|
MARKLE SIGN
|
|
|
Histologic findings pathognomonic for Whipple's disease
|
ACID-SCHIFF POSITIVE MACROPHAGES W/ EVIDENCE OF ACID FAST NEGATIVE GRAM NEGATIVE BACILLI
|
|
|
Tx for Whipple's disease
|
CEFTRIAXONE IV FOR TWO WEEKS, THEN BACTRIM BID FOR A YEAR THEN REPEAT BX. SULFA ALLERGIC PTS GET DOXY
|
|
|
In an ICU pt, which could be the first sign of a GI bleed?
|
ELEVATED BUN (BLOOD ABSORBED BY THE INTESTINES IS METABOLIZED TO UREA NITROGEN)
|
|
|
Pt presents with paresthesias in the form of pins and needles in the extremities mainly hands, ataxic gait, proximal muscle weakness and stiffness and hyperactive dtr's..what's the dx and tx
|
SUBACUTE COMBINED DEGENERATION OF THE SPINAL CORD
TX- VIT B12 |
|
|
Pt presents w/ steatorrhea, macrocytic anemia and malnutrition s/p gi tract operation..dx?
|
BLIND LOOP SYNDROME 2/2 BACTERIAL OVERGROWTH
|
|
|
Why should Sucralfate not be used along with H2B or antacids?
|
H2B AND ANTACIDS DECREASE THE PH IN THE STOMACH AND INHIBIT THE ACCION OF SUCRALFATE WHICH NEEDS AN ACID ENVIROMENT TO WORK
|
|
|
Pt presents with hematemesis 2/2 esophageal varices however there's no portal hypertension. What test should be ordered and what's the tx for this condition?
|
A CT TO RULE OUT SPLENIC VEIN THROMBOSIS WHICH CAUSES THIS AND THE TX IS SPLENECTOMY
|
|
|
Pt complains of regurgitation of undigested food which woke him from sleep as well as trouble swallowing both solids and liquids in a non proressive fashion. Dx?
|
ACHALASIA
|
|
|
Pt complains of regurgitation of undigested food, grugling sounds in his neck and bad breath. Dx?
|
ZENKER'S DIVERTICULUM
|
|
|
Name of the area where a Zenker's Diverticulum is likely to appear?
|
KILLIAN TRIANGLE
|
|
|
Pt c/o trouble swallowing and hoarseness. He has lost weight and there's wheezing unilaterally. Dx?
|
ESOPHAGEAL CA
|
|
|
Most sensitive test to determine esophageal tumor invasion?
|
ENDOSCOPIC US
|
|
|
Pt c/o chest pain with diffuse radiation and trouble swallowing both solids and liquids in a episodic manner. EKG is neg and barium swallow shows a "corkscrew" pattern. What's the MLDx?
|
DIFFUSE ESOPHAGEAL SPASM
|
|
|
Pt c/o of food stuck in his esophagus when he eats too fast. He has a pmhx of hiatal hernia but doesn't complain of heartburn. This happens ocasionally and improves in a few minutes. MLDx?
|
SCHATZKI RING
|
|
|
60+ yo pt presents with painless GI bleeding that comes and goes. Pt has h/o VWF deficiency and Aortic Stenosis. MLDx? Which test confirms it?
|
DX: ANGIODYSPLASIA
TEST: ANGIOGRAPHY SHOWS DELAYED VENOUS EMPTYING |
|
|
Pt is on cisapride for poor gastric motility and GERD. He complains his reflux is still bothering him. Why is Cimetidine a bad idea?
|
CIMETIDINE INHIBITS CYP-450 AND IT WILL CAUSE AN ELEVATION OF CISAPRIDE CONTENT CAUSING PROLONGED QT SYNDROME AND TORSAD DE POINTES
|