Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
62 Cards in this Set
- Front
- Back
|
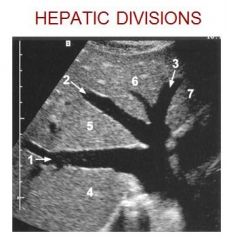
1. RHV
2. MHV 3. LHV 4. Posterior right lobe 5. Anterior right lobe 6. Medial left lobe 7. Lateral left lobe |
|

|
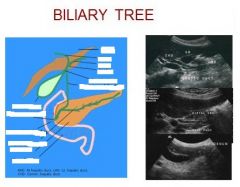
Is this a transverse or sagittal image? Transverse… note IVC
A = hepatic vein (believe middle) because it demonstrates “naked” walls and courses towards the IVC B = portal vein (lateral left) because it demonstrates echogenic walls |
|
|
|
|
|
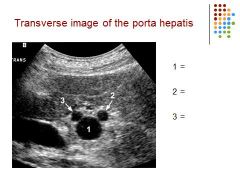
1 = main portal vein
2 = proper hepatic artery 3 = common hepatic duct |
|
|
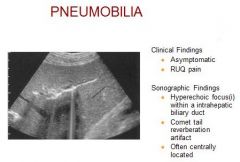
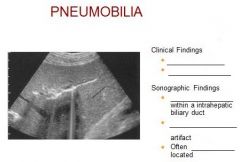
Etiology – surgical procedure, trauma, infection
Clinical – asymptomatic, RUQ pain Differential foreign body, biliary calculus, arterial calcification |
|
|
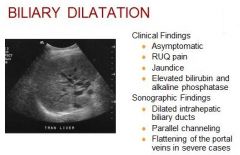
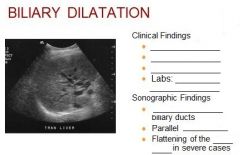
Etiology - Biliary obstruction
Differential Normal biliary tree Portal hypertension Portal vein thrombosis Portal hypertension |
|
|
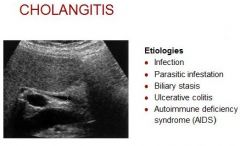
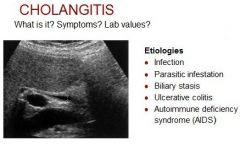
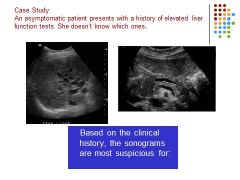
Cholangitis is an infection of the common bile duct, the tube that carries bile from the liver to the gallbladder and intestines.
Clinical – abd pain, fever, leukocytosis, jaundice, mild elevation AST, ALT Marked elevation in bilirubin and alk phos |
|
|
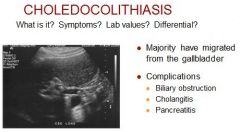
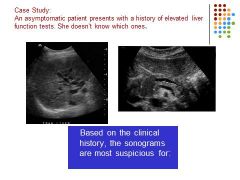
Choledocholithiasis is the presence of a gallstone in the common bile duct. The stone may consist of bile pigments or calcium and cholesterol salts. Symptoms usually do not occur unless the stone blocks the common bile duct
Clinical – RUQ colicky pain Elevated bilirubin and alk phos Mild elevation AST, ALT Differential: Surgical clip |
|
|
|
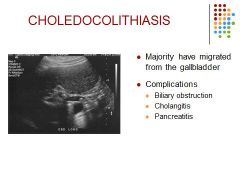
Choledocholithiasis is the presence of a gallstone in the common bile duct. The stone may consist of bile pigments or calcium and cholesterol salts. Symptoms usually do not occur unless the stone blocks the common bile duct
Clinical – RUQ colicky pain Elevated bilirubin and alk phos Mild elevation AST, ALT Differential: Surgical clip |
|
|
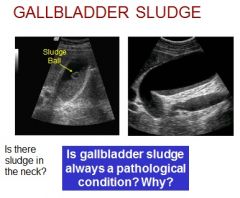
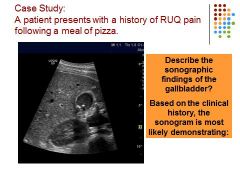
****** Is this sludge in the neck of the gallbladder? No, most likely reverberation artifact.
No sludge is not always pathological – i.e prolonged fasting |
|
What is it?
Clinical? Sonographic Appearance? Differential Diagnosis? |
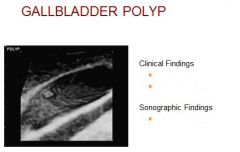
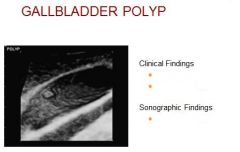
Benign epithelial tumor
Clinical – Asymptomatic Dull RUQ pain Intolerance to fatty foods Sonographic appearance: Non- mobile, non-shadowing intraluminal echogenic focus Differential diagnosis: Gallbladder fold, cholelithiasis, carcinoma |
|
What is it?
Clinical? Sonographic Findings? |
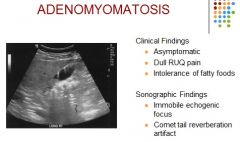
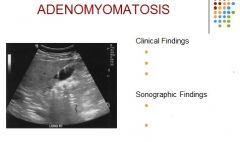
Hyperplasia of the epithelial and muscle layers of the gb wall
Clinical – asymptomatic, dull RUQ pain, intolerance to fatty foods Sonographic – non-mobile echogenic focus; comet tail reverberation artifact |
|

What is it?
Dilatation of? Bile duct? Labs? |

Increase in AST, ALT
Elevated bilirubin and alk phos |
|
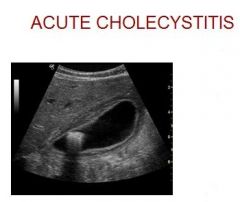
What is it?
Clinical Findings? Sonographic Findings? Differential? |
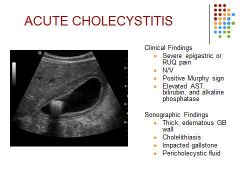
Acute cholecystitis is a sudden inflammation of the gallbladder that causes severe abdominal pain.
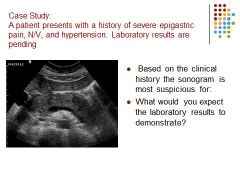
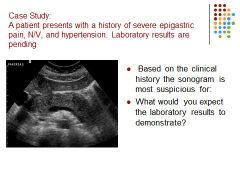
Etiology – Obstruction of the cystic duct, infection, idiopathic Clinical Findings: Severe epigastric or RUQ pain Nausea/Vomiting Positive Murphy’s sign Elevated AST, bilirubin and alkaline phosphatase Sonographic Findings: Thick, edematous GB wall Cholelithiasis (90%) Impacted gallstone Pericholecystic fluid Thick wall termed “halo sign” 10% cases acalculous cholecystitis Differential consideration – Liver abscess, ascites, non-fasting pt. |
|
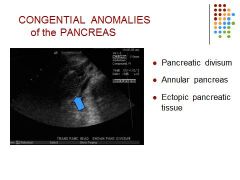
Explain each
|
Divisum - Failure of the normal fusion of the Wirsung and Santorini ducts; duct of santorini drains the majority of pancreas; associated with a higher incidence of pancreatitis
Annular- Rare anomaly where the head of the pancreas surrounds the duodenum resulting in obstruction of the biliary tree or duodenum Ectopic tissue - Located in the stomach, duodenum, small or large intestines. Look like polyp type masses |
|
Normal Serum amylase level?
Normal serum lipase? |
Serum amylase- normal 25 – 125 U/L
Serum lipase – normal 10 -140 U/L |
|
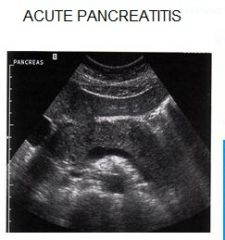
What are the clinical findings and sonographic findings? Causes?
|
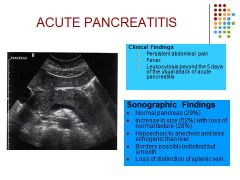
Biliary obstruction the most common etiology followed by alcohol abuse. Other causes include: trauma, peptic ulcer disease and idiopathic
|
|
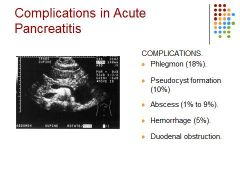
Explain each complication
|
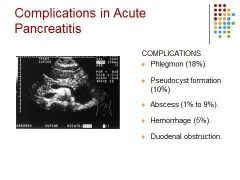
Phlegmon - extension of pancreatic inflammation into the peripancreatic tissues
Pseudocyst – focal collection of inflammatory necrotic tissue, blood, and pancreas secretions; Most often located in the lesser sac. Abscess develops due to infection of the necrotic pancreas Hemorrhage - rapid development of inflammation causing necrosis and hemorrhage Duodenal obstruction - high protein concentration in the pancreas enzymes can irritate the duodenum. |
|
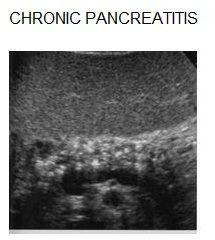
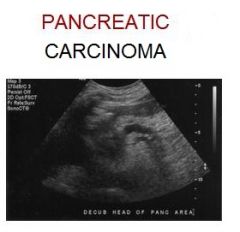
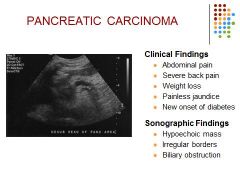
Causes? Clinical Findings? Sonographic Findings? Differentials?
|
Repeated, prolonged or persistent attacks of pancreatitis; hyperlipidemia
Differential considerations: fatty replacement |
|
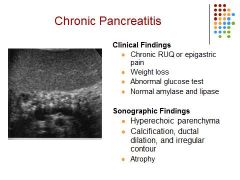
Clinical findings? Sonographic findings?
|
|
|
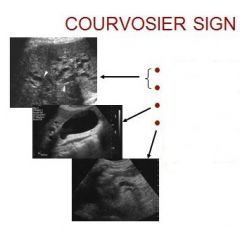
What is it? Explain the three causes pictured.
|
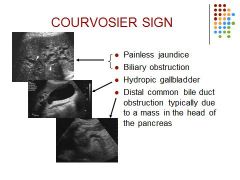
Courvoisier syndrome means that you have jaundice and a gallbladder that is enlarged but is not painful, and your doctor can feel it when he or she examines you.
Hydropic GB: accumulation of clear, watery fluid in the gallbladder as a result of long-standing cystic duct obstruction. |
|
|
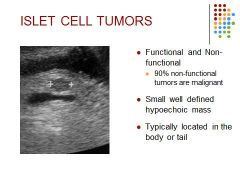
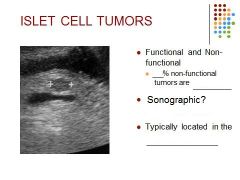
90% of non-functional tumors are malignant and compromise 1/3 of all islet cell tumors
In the normal pancreas, cells called islet cells produce hormones that regulate a variety of bodily functions, such as blood sugar level and the production of stomach acid. Tumors that arise from islet cells of the pancreas can also produce a variety of hormones, though some do not. Although islet cells produce many different hormones, most tumors release only one hormone that leads to specific symptoms. Pancreatic islet cell tumors can be noncancerous (benign) or cancerous (malignant). |
|
|
Need to add answer text!
|
|
|
Biliary obstruction secondary to mass in the pancreatic head.
COURVOSIER SIGN |
|
|
NEED TO ADD TEXT!
|
|
|
Fatty infiltration may be seen in all patients except those with:
A) diabetes mellitus B) chronic alcoholism C) hepatoportal fistula D) hepatitis |
C) hepatoportal fistula
|
|
|
Sonographic findings of acute hepatitis include:
A) accentuated brightness, more extensive demonstration of portal vein radicles, and overall decreased echogenicity of liver B) decreased brightness and echogenicity of liver C) increased brightness and echogenicity of liver; no demonstration of portal vein radicles D) ascites, decreased brightness, and echogenicity |
A) accentuated brightness, more extensive demonstration of portal vein radicles, and overall decreased echogenicity of liver
|
|
|
The most common benign tumor of the liver is:
A) mesenchyma hamartoma B) adenoma C) cavernous hemangioma D) infantile hemangioendothelioma |
C) cavernous hemangioma
|
|
|
Patients who have hepatocellular carcinoma are likely to have had:
A) hemochromatosis B) adenosis C) cirrhosis D) carcinosis |
C) cirrhosis
|
|
|
The most common form of neoplastic involvement of the liver is:
A) metastases B) hepatocellular carcinoma C) hepatoma D) hamartoma |
A) metastases
|
|
|
In severe hepatocellular destruction, the AST and ALT are:
A) high B) moderately high C) moderate D) mild |
A) high
|
|
|
Elevation of alkaline phosphatase is associated with:
A) biliary obstruction B) tumor lesion in the liver C) hepatocellular disease D) cystic disease of the liver |
A) biliary obstruction
|
|
|
Diminished vascular structures within the liver parenchyma most likely represent:
A) obstructive portal disease B) cirrhosis C) Budd-Chiari syndrome D) acute viral hepatitis |
B) cirrhosis
|
|
|
Elevation of serum bilirubin results in:
A) hepatocellular disease B) ascites C) jaundice D) hemolysis |
C) jaundice
|
|
|
Typical symptoms a patient may have with an abscess formation include all of the following EXCEPT:
A) fever B) decreased white blood count C) pain D) increased white blood count |
D) increased white blood count
|
|
|
The vascular tumor composed of blood vessel cells with nonspecific sonographic findings is:
A) adenoma B) hemangioma C) Ewing's angioma D) hamartoma |
B) hemangioma
|
|
|
The right and left hepatic ducts emerge from the right lobe of the liver in the porta hepatis and unite to form the:
A) common hepatic duct B) cystic duct C) common bile duct D) common pancreatic duct |
A) common hepatic duct
|
|
|
The hepatic duct is joined by the _____ to form the _____.
A) pancreatic duct; cystic duct B) cystic duct; common bile duct C) common bile duct; cystic duct D) right hepatic duct; common bile duct |
B) cystic duct; common bile duct
|
|
|
The cystic duct connects the _____ of the gallbladder with the common hepatic duct to form the _____.
A) fundus; common hepatic duct (CHD) B) fundus; common bile duct (CBD) C) neck; CBD D) body; CHD |
C) neck; CBD
|
|
|
A phrygian cap of the gallbladder is:
A) partial septation B) calcification of the gallbladder wall C) septations within the organ D) folding of the fundus |
D) folding of the fundus
|
|
|
The function of the gallbladder is:
A) storage for extra cholesterol B) storage for enzymes C) reservoir for bile D) reservoir for biliary salts |
C) reservoir for bile
|
|
|
Hartmann's pouch is formed:
A) when septations divide the neck from the cystic duct B) when the gallbladder folds back on itself at the neck C) when the gallbladder is partially septated D) when the fundus is folded |
B) when the gallbladder folds back on itself at the neck
|
|
|
Classic symptoms of gallbladder disease include all of the following EXCEPT:
A) hematuria B) right upper quadrant pain C) right shoulder pain D) nausea and vomiting |
A) hematuria
|
|
|
Inflammation of the gallbladder is:
A) cholecystitis B) choledocholithiasis C) cholesterosis D) adenomyomatosis |
A) cholecystitis
|
|
|
Gallstone appearance on ultrasound examination is:
A) dependent, mobile, echogenic B) dependent, immobile, echogenic C) dependent, float, immobile D) independent, mobile, hypoechoic |
A) dependent, mobile, echogenic
|
|
|
Cholelithiasis is characterized on ultrasound as:
A) fuzzy margins B) low-level echoes beyond the stone C) shaggy borders of the margin D) clean shadow with distinct margins |
D) clean shadow with distinct margins
|
|
|
Nonshadowing, low-amplitude echoes in a dependent gallbladder is most characteristic of:
A) stones B) porcelain gallbladder C) cholecystitis D) sludge |
D) sludge
|
|
|
The head of the pancreas lies in the:
A) lap of the liver B) lap of the gallbladder, common bile duct (CBD) C) lap of the duodenum D) lap of the lesser omentum |
C) lap of the duodenum
|
|
|
The head of the pancreas is inferior to the:
A) right lobe of liver B) caudate lobe of liver C) right lateral fissure of liver D) left lateral fissure of liver |
B) caudate lobe of liver
|
|
|
The _____ is the anterolateral border of the pancreas.
A) common bile duct B) gastroduodenal artery C) hepatic duct D) superior mesenteric vein |
B) gastroduodenal artery
|
|
|
The tail of the pancreas is found:
A) posterior to the left kidney, near the splenic hilum B) anterior to the left kidney, near the splenic hilum C) posterior to the right kidney, near the liver hilum D) anterior to the right kidney, near the liver hilum |
B) anterior to the left kidney, near the splenic hilum
|
|
|
The primary pancreatic duct is the:
A) duct of Santorini B) duct of Ampulla C) duct of Vater D) duct of Wirsung |
D) duct of Wirsung
|
|
|
The duct of Santorini is a/an:
A) small accessory duct to the gallbladder B) accessory duct to the cystic duct C) accessory duct to the pancreas D) small opening in the duodenum |
C) accessory duct to the pancreas
|
|
|
The normal size of the pancreatic duct is less than:
A) 1 mm B) 3 mm C) 5 mm D) 6 mm |
B) 3 mm
|
|
|
The enzyme that is the most sensitive over time in laboratory tests for the diagnosis of acute pancreatitis is:
A) aspartate amniotransferase (AST) B) alkaline phosphatase C) amylase D) lipase |
D) lipase
|
|
|
The splenic artery is considered to be the:
A) superior border of the pancreas B) lateral border of the pancreas C) anterior border of the pancreas D) inferior posterior border of the pancreas |
A) superior border of the pancreas
|
|
|
Clinical signs and symptoms in acute pancreatitis include all of the following EXCEPT:
A) severe abdominal pain radiating to the back B) severe abdominal pain radiating to the right shoulder C) elevated amylase D) nausea and vomiting |
B) severe abdominal pain radiating to the right shoulder
|
|
|
The pancreas is reflective in its sonographic appearance because of the multiple:
A) islets of Langerhans B) Cooper’s ligaments C) small glands or acini D) fat between the lobules |
D) fat between the lobules
|
|
|
Gallstones are present in 40% to 60% of patients with:
A) chronic pancreatitis B) annular pancreas C) cystic fibrosis D) acute pancreatitis |
D) acute pancreatitis
|
|
|
On ultrasound, acute pancreatitis may appear:
A) homogeneous B) echogenic C) calcified D) hypoechoic |
D) hypoechoic
|
|
|
The most common cause of acute pancreatitis in children is:
A) surgery B) drinking C) baseball D) trauma |
D) trauma
|
|
|
A patient who presents with jaundice, weight loss, and a palpable right upper quadrant (RUQ) mass should be evaluated for:
A) cholecystitis B) adenocarcinoma of the pancreas C) pancreatitis D) pancreatic pseudocyst |
B) adenocarcinoma of the pancreas
|