Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
30 Cards in this Set
- Front
- Back
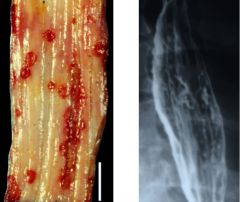
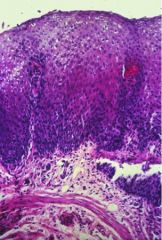
Identify.
A. Candida esophagitits B. Cytomegalovirus esophagitis C. Herpes esophagitis |
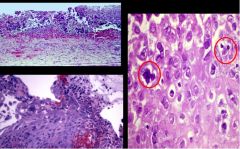
C. Herpes esophagitis
punched out erosions that are linear- classic for herpes! When you take a section thru one of the ulcers the squamous epithelium is jumbled up and at the edges of the epithelial cells you see the circled cells that are the herpes inclusions. The inclusions are only in the squamous epithelium. So look at the EDGE of the ulcer. (Unlike herpes, CMV is found at the BASE of the ulcer, not on the edges. ) |
|
|
True or False:
Unlike herpes in herpes esophagitis, CMV in CMV esophagitis is found at the BASE of the ulcer, not on the edges. |
TRUE
|
|

Identify.
|
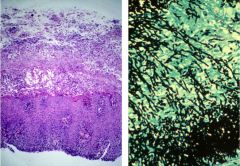
Candida esophagitis.
This is it histologically. The cheesy yellow material is the exudate (sloughed epithelium).. The hyphae are highlighted wiith a silver stain. |
|
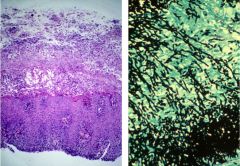
What is this?
A. Candida esophagitits B. Cytomegalovirus esophagitis C. Herpes esophagitis |
A. Candida esophagitits
The cheesy yellow material is the exudate (sloughed epithelium).. The hyphae are highlighted wiith a silver stain. |
|
This is reflux esophagitis. There is nothing really specific for reflux, anything that causes injury will have this effect. So irritation from medication injury can also make this. So really, the patient’s history of reflux is important. What three changes are seen histologically?
|
- Expansion of the basal zone
- Vascular dilation - Intra-epithelial inflammatory cells (lymphocytes, eosinophils, neurtophils) |
|
|
What complications are seen in reflux esophagitis? (4)
|
Peptic ulcers, strictures, Barrett's metaplasia, adenocarcinoma
The reason people get biopsies of this is because of the risk of Barrett’s metaplasia, or also known as intestinal metaplasia which can lead to adenocarcinoma. |
|
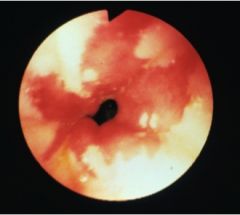
What is this?
A. Barrett's Esophagus B. Candida esophagitits C. Cytomegalovirus esophagitis D. Herpes esophagitis |
A. Barrett's Esophagus
|
|
|
True or False:
Mesenchymal tumors are usually malignant; epithelial tumors are usually benign |
FALSE
Mesenchymal tumors are usually BENIGN; epithelial tumors are usually MALIGNANT |
|
|
_____________ is a benign tumor composed solely of mature smooth muscle that preferentially arises in the esophagus and rectum.
|
Leiomyoma
Is the most common tumor of the esophagus. Is normally small, solitary, round intramural mass of distal esophagus. Usually asymptomatic and is an incidental diagnosis at endoscopy or autopsy. 60% of symptomatic patients have pain or dysphagia of 2 years duration. 50 carcinomas for each clinically significant leiomyoma. |
|
|
True or False:
Leiomyoma is the most common tumor of the esophagus. |
TRUE. Leiomyoma is a benign tumor composed solely of mature smooth muscle that preferentially arises in the esophagus and rectum.
|
|
|
True or False:
Alcohol and smoking are the main risk factors for squamous cell carcinoma of the esophagus. |
TRUE
|
|
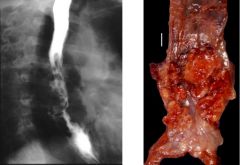
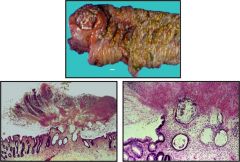
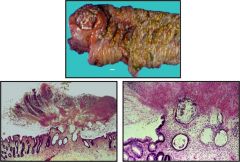
Identify.
|
Squamous cell carcinoma of esophagus.
Mass in upper third of esophagus is more likely to be squamous cell carcinoma; a lower mass is where the adenocarcinomas are usually. The resection of the tumor would be very broad because these tumors actually have the propensity to go underneath the surrounding normal mucosa (see arrows of the nests of malignant areas). Keratin pearls might be present too. |
|
|
Of the causes of chronic gastritis, which is more common and where is it usually centered - distal or proximal stomach - Autoimmune gastrities, Helicobacter pylori gastritis?
|
H. pylori in dystal stomach is much more common.
Remember, gastritis is just destruction of the mucosa by back-diffusion of acid. |
|
|
What is the difference between an erosion and ulcer?
|
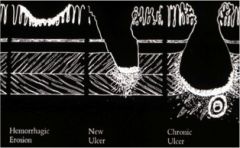
Erosion is injury to the epithelium that is superficial to the muscularis mucosa.
Ulcer is damage deeper into the muscularis mucosa, or stomach wall. This has implications because the mucosa can heal without sequelae, but ulcer heals by fibrosis so you get weakened wall when healed. Acute looks very punched out and chronic would have a lot of fibrotic tissue emanating around and away from it. For acute gastritis, a cross section of the erosion there is |
|
|
What condition is described?
20% of chronic gastritis. Antibodies to parietal cells and intrinsic factor result in destruction of acid-secreting mucosa --> Increased pH --> Pernicious anemia |
Autoimmune gastritis
Looks like chronic gastritis. Only difference is that it would be in proximal stomach with some sparing of the distal stomach. Nests in silver stain are highlighting the increase in neuroendocrine cells. |
|
|
Helicobacter pylori has many mechanisms of cell injury. What do each do?
A. urease B. LPS endotoxin C. ammonia D. protease and lipase |
A. urease - recruits and activates inflammatory cells
B. LPS endotoxin - activates immune response C. ammonia - direct tissue damage D. protease and lipase - impedes mucosal barrier |
|
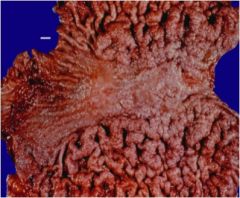
What condition is this? What are the three etiologies for this?
|
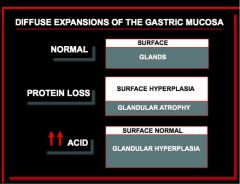
This is hypertorphic gastropathy.
H. pylori gastritis Ménétrier's disease - protein loss thus expansion of the surface Zollinger-Ellison syndrome - glandular hyperplasia so you get expansion of glandular area with normal surface |
|
|
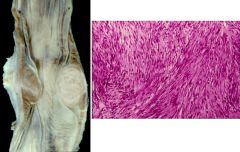
What is described?
75-80% of these have mutations of tyrosine kinase (c-kit); 8-10% have mutation to platelet derived growth factor alpha A. Adenocarcinoma of the stomach B. Gastrointestinal stromal tumor C. Menetrier's dz D. Zollinger-Ellison Syndrome |
B. Gastrointestinal stromal tumor GIST
These tumors are shelled out. The surface is totally different than a leiomyoma. This is more fleshy and has areas of hemorrhage. |
|
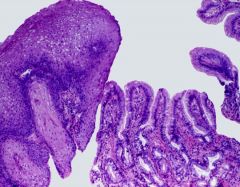
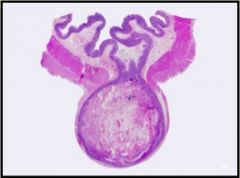
This is a picture of a "normal" what?
A. Crohn's dz B. Hirschsprung's dz C. Meckel's diverticulum D. Pseudomembranous colitis |
C. Meckel's diverticulum - failure of involution of vitelin duct during development. Most common is having a sac in the terminal ileum. Rule of 2s: 2 feet from terminus of ileum that is 2 inches in length and about 2% of the population has em. Can be asymptomatic but occasionally can have ulcers, twist and strangulate, have a carcinoma in em, etc.
|
|
|
What is Hirschsprung's dz?
|
Enteric aganglionosis.
Failure of migration of the neural crest cells down into the plexus of the rectum. It is enteric aganglionosis. The portion that doesn’t have ganglia do NOT relax so you end up with obstruction of bowel! To diagnose does a deep biopsy of the neural plexus in between the two muscle layers. Look to see if nerve in specimen has ganglion cells. To treat basically need surgery where they take out the aganglionic part and pull down ganglionic parts and then form an anastamoses. |
|
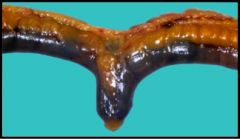
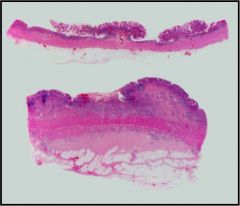
What condition is shown?
|
Diverticular dz of the colon!
Why are there weakened gaps in the muscle? That’s where the arterioles perforate to supply the muscle. That’s where the diverticula normally occur. |
|
What condition is shown?
|
Diverticular dz of the colon!
|
|
|
Vibrio cholera infection of the gut causes [ inflammatory dysentery / non-inflammatory osmotic diarrhea / non-inflammatory secretory diarrhea ].
|
non-inflammatory secretory diarrhea
remember, that is enterotoxin induced secretion of water. In cholera, the bacteria does not invade the mucosa. Instead what causes the symptoms is that the toxins that the bacteria secrete cause massive secretion of bicarbonate and fluid. So in cholera, you have diarrhea because of the TOXIN not the bacteria itself! |
|
|
What condition is described?
- Appears 4 - 10 days after administration of broad spectrum antibiotics - Overgrowth of resistant Clostridium difficile - Bacteria produce toxins that destroy mucosa - Sloughed mucosa and mucopurulent exudate form a "pseudomembrane" - High mortality (28%) |
Clostridium difficile colitis
|
|
Identify.
|
Clostridium difficile pesudomembranous colitis
|
|
|
What condition is described?
Systemic infection by Gram positive bacillus, Tropheryma whippellii Bacteria accumulate within macrophages in the lamina propria of the small bowel Bacterial-laden macrophages obstruct mucosal lacteals causing impaired transport |
Whipple's Disease
|
|
Describe the differences histologically.
|
UC: Bowel wall normal in thickness
Chrons’ dz: very thickened, fibrotic bowel , lymphoid aggregates in subserosal and submucosa. |
|
|
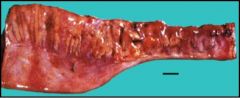
What condition is described?
Over time, you get knife-like fissures through the wall. In the R picture, the fissure goes THROUGH the wall, causing the serosa to become sticky! Then you end up with fistulas among the loops of the bowel. A. Ulcerative colitis B. Crohn's dz C. Celiac's Dz D. Whipple's Dz |
B. Crohn's dz
|
|

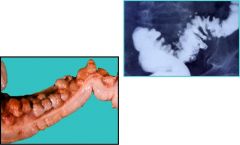
This is a picture of familial adenomatous polyposis. What is there an increased risk of?
|
Increased risk of colon cancer b/c pt has thousands of polyps in their colon and other places of their GI tract. If you don’t remove the colon, will develop a carcinoma before the age of 40.
|
|
|
What is the staging for colorectal cancer? (TNM specifics)
|
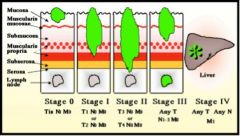
|