Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
21 Cards in this Set
- Front
- Back
What are the two sources of hepatic blood flow?
Which is oxygen-rich, nutrient poor? Which is o2-poor, nutrient rich? Which is the main source of blood for the liver? |
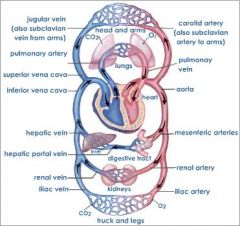
Hepatic artery (main)
Portal Vein |
|
Gallstones: Goroll page 549
Pathophysiology Risk factors Biliary sludge |

• Super-saturation of bile with cholesterol
• Family history, female gender, obesity, more estrogen= stones • Rapid weight loss • Regular exercise is protective in women • Similar pathophysiology as stones, • Risk for sludge: rapid weight loss, pregnancy, transplant, ceftriaxone, octreotide |
|
Statistically speaking, what is the most common cause of jandice in young adults? The Elderly?
|
Viral Hepatitis
Malignancy |
|
|
What are the two things bile is used for in the body?
|
- Promoting digestion and absorption of dietary lipids
- Allowing excretion of lipid organic metabolites and drugs not readily eliminated through the kidneys |
|
|
If necessary, liver can increase synthesis of bile acids up to __ times normal.
__% of bile acids are reabsorbed in the terminal ileum, then extracted from the portal circulation by hepatocytes. |
10
95% |
|
|
Do most gallstones cause sx?
What are the two types of gallstones, and what is the breakdown of one of those types? Of which type are 80% of stones? What are the 4F's, and what do they put you at risk for? |
No. 80% don't.
Cholesterol & Pigmented (Black and Brown) Cholesterol Fat, Fertile, Female, Forty - cholesterol stones! |
|
|
On which three factors do gallstone formation depend?
|
supersaturation of bile
a nidus for cholesterol crystal formation gallbladder dysmotility/bile stasis |
|
|
What differentiates the composition of black vs brown stones?
Which is more important in infections? |
Black: calcium bilirubinate
Brown: Ca-bilirubinate + FFA from breakdown of lecithin by bacteria Brown |
|
|
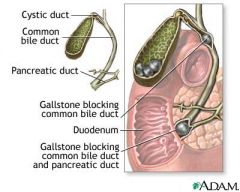
Define the following terms:
Cholelithiasis Biliary colic Cholecystitis Choledocholithiasis Cholangitis |
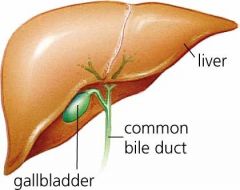
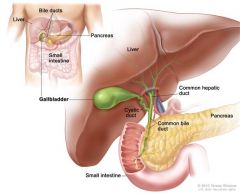
Cholelithiasis – stones in the gallbladder
Biliary colic – intermittant RUQ pain, can be a sign of obstruction Cholecystitis - infec of gallbladder Choledocholithiasis – stone in common bile duct Cholangitis – infection of bile duct |
|
|
Why might pain caused by gallstones selectively show up after eating? What is this pain called?
|
gallbladder contracts after eating --> temporary obstruction / pain of contraction on the stone --> biliary colic
|
|
|
In Cholecystitis, what type of LFTs would you expect to see? WBC count?
Would you see Jaundice? Tx of choice? |
LFTs = normal
Elevated WBC No; if you see jaundice, then something else is going on instead/with. Cholecystectomy, antiB |
|
|
Fever & Murphy's sign, in a pt with normal LFTs, elevated WBC, and no jaundice... what should we think of?
|
Cholecystitis
|
|
|
If the pt's stool is acholic ("clay-colored"), and their urine is dark, "tea-colored", what pathophysiology might we think of?
|
obstruction of the bile duct.
|
|
|
What is Charcot's triad? What is it the classical presentation of?
Is it an emergent condition? |
fever
right upper quadrant pain jaundice obstruction of the flow of bile Yes. |
|
|
List the status of the following parameters for these four dz (Cholelithiasis, Cholecystitis, Choledocholithiasis, Cholangitis):
- Sx - Fever + elevated WBC - LFTs - Biliary dilation on ultrasound - Tx? |
Cholelithiasis:
- biliary colic, No, normal, no, surgery if sx exist Cholecystitis: - biliary colic / RUQ pain, Yes, Normal, No, Surgery + antiBs Choledocholithiasis: - billiary colic / RUQ pain, Either, Elevated (AP, GGT, Bili), yes, ERCP Cholangitis: - RUQ pain, yes, all elevated, either, ERCP + AntiB |
|
|
Ultrasound is _____ and ____ for detecting cholelithiasis.
Can U/S dx cholecystitis? |
sensitive and specific
No, but it can suggest it. |
|
|
IV radio-nucleotides concentrate in the bile and collect in the GB
If GB doesn’t appear, what does that mean? As a corollary, what acute issue is this scan great for dx'ing? |
cystic duct must be obstructed
Great way to dx acute cholecystitis |
|
|
Think about what ERCP and MRCP are, and what there differences are.
|
ERCP = Endoscopic retrograde cholangiopancreatography
MRCP = non-invasive, almost as good |
|
|
Clinical presentation: Goroll page 552
Biliary Colic…. |
• Biliary colic: RUQ pain, sudden onset over about 1 hour, last 2-4 hours
• N/V, fever, jaundice ; all or only some of the symptoms • Intolerance to fatty food, belching, bloating, has been reported but cause and effect is in question • Presentation is highly variable and may be asymptomatic for a long time |
|
Clinical course for symptomatic patients
|
• At least one episode of pain, requiring hospitalization
• Jaundice , cholangitis, pancreatitis Ascending cholangitis or acute cholangitis (or sometimes cholangitis without a modifier - is an infection of the bile duct (cholangitis), usually caused by bacteria ascending from its junction with the duodenum (first part of the small intestine). It tends to occur if the bile duct is already partially obstructed by gallstones.[1][2] Cholangitis can be life-threatening, and is regarded as a medical emergency.[1] Characteristic symptoms include jaundice, fever, abdominal pain, and in severe cases, low blood pressure and confusion. Initial treatment is with intravenous fluids and antibiotics, but there is often an underlying problem (such as gallstones or narrowing in the bile duct) for which further tests and treatments may be necessary, usually in the form of endoscopy to relieve obstruction of the bile duct.[1][3] |
|
Goroll: therapeutic recommendations: page 553
|

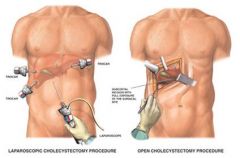
• No symptoms: watch and wait
• If one episode of biliary colic: same as above • If + stones and symptoms Do Laproscopic cholecystectomy • Symptomatic non-surgical patients get Ursodiol 12-24 months: only for small stones < 2 cm and fewer than 3 in count. Calcification rules out bile acid therapy • Estrogen preparations such as clomid can precipitate these stone……..so watch out or reduce dose • Diet: really does not effect outcome much • Obesity and calorie excess are big risk factors: as is rapid weight loss, so slow weight loss is better. • Dyspeptic symptoms are NOT grounds for medical or surgical interventions due to poor correlation with GB DZ |