Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
189 Cards in this Set
- Front
- Back
|
Important genes of embryogenesis - Sonic hedgehog gene
|
Produced at base of limbs in zone of polarizing activity. Involved in patterning along anterior-posterior axis.
|
|
|
Important genes of embryogenesis - Wnt-7 gene
|
Produced at apical ectodermal ridge (thickened ectoderm at distal end of each developing limb). Necessary for proper organizing along dorsal-ventral axis.
|
|
|
Important genes of embryogenesis - FGF gene
|
Produced at apical ectodermal ridge. Stimulates mitosis of underlying mesoderm, profiding for lengthening of limbs.
|
|
|
Important genes of embryogenesis - Homeobox (Hox) genes
|
Involved in segmental organization of embryo in a craniocaudal direction. Hox mutations -> appendages in wrong locations.
|
|
|
Fetal landmarks - Day 0
|
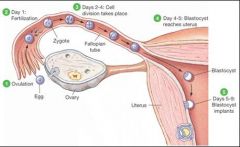
Fertilization by sperm forming zygote, initiating embryogenesis.
|
|
|
Fetal landmarks - Within week 1
|
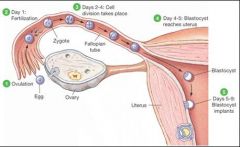
hCG secretion begins after implantation of blastocyst
|
|
|
Fetal landmarks - Within week 2
|

Bilaminar disk (epiblast, hypoblast)
|
|
|
Fetal landmarks - Within week 3
|

Trilaminar disc. Gastrulation.
Primitive streak, notochord, mesoderm and its organization, and neural plate begin to form. |
|
|
Fetal landmarks - Weeks 3-8
|
Embryonic period.
Neural tube formed by neuroectoderm and closes by week 4. Organogenesis. Extremely susceptible to teratogens. |
|
|
Fetal landmarks - Week 4
|
Heart begins to beat. Upper and lower limb buds begin to form.
|
|
|
Fetal Landmarks - Week 8
|
Fetal Period begins.
Fetal movement, fetus looks like a baby. |
|
|
Fetal Landmarks - Week 10
|
Genitalia have male/female characteristics.
|
|
|
Fetal landmarks - Alar Plate/ Basal plate
|
Alar plate (dorsal) - Sensory
Basal Plate (Ventral) - Motor Same orientation as spinal cord. |
|
|
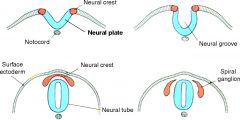
Neural Development - details?
|
Notochord induces overlying ectoderm to differentiate into neuroectoderm and form the neural plate.
Neural plate gives rise to the neural tube and neural crest cells. Notochord becomes nucleus pulposus of the intervertebral disk in adults. |
|
|
Rules of Early Development - Rule of 2's for 2nd week
|
2 germ layers (bilaminar disk): epiblast, hypoblast
2 cavities: amniotic cavity, yolk sac 2 components to placenta: cytotrophoblast, syncytiotrophoblast The epiblast (precursor to embryo) invaginates to form primitive streak. Cells from the primitive streak give rise to both intraembryonic mesoderm and part of the endoderm. |
|
|
Rules of Early Development - Rule of 3's for 3rd week
|
3 germ layers (gastrula): ectoderm, mesoderm, endoderm
|
|
|
Rules of Early Development - Rule of 4's for 4th week
|
4 heart chambers
4 limb buds grow |
|
|
Embryologic derivatives - Surface ectoderm
|
Adenohypophysis (from Rathke's pouch); lens of eye; epithelial linings of oral cavity, sensory organs of ear, and olfactory epithelium; epidermis; anal canal below the pectinate line; parotid, sweat, and mammary glands
Craniopharyngioma - benign Rathke's pouch tumor with cholesterol crystals, calcifications |
|
|
Embryologic derivatives - Neuroectoderm
|
Brain (neurohypophysis, CNS neurons, oligodendrocytes, astrocytes, ependymal cells, pineal gland), retina, spinal cord
Neuroectoderm - think CNS and brain |
|
|
Embryologic derivatives - Neural crest
|
PNS, dorsal root ganglia, cranial nerves, celiac ganglion, melanocytes, chromaffin cells of adrenal medulla, parafollicular (C) cells of thyroid, Schwann cells, pia and arachnoid, bones of the skull, odontoblasts, aorticopulmonary septum.
Neural crest - think PNS and non-neural structures nearby Odonto = teeth. Think Crest toothpaste. |
|
|
Embryologic derivatives - Endoderm
|
Gut tube epithelium (including anal canal above the pectinate line) and derivatives (e.g., lungs, liver, pancreas, thymus, parathyroid, gallbladder, eustachian tube, thyroid follicular cells).
|
|
|
Embryologic derivatives - Mesoderm
|
Muscle, bone, connective tissue, serous linings of body cavities (e.g., peritoneum), spleen (derived from foregut mesentery), cardiovascular structures, lymphatics, blood, wall of gut tube, wall of bladder, urethra, vagina, kidneys, adrenal cortex, skin dermis, testes, ovaries.
|
|
|
Embryologic derivatives - Notochord
|
Notochord induces ectoderm to form neuroectoderm (neural plate). Its postnatal derivative is the nucleus pulposus of the intervertebral disk.
|
|
|
Types of errors in organ morphogenesis - name 5 types
|
1. Malformation
2. Deformation 3. Agenesis 4. Hypoplasia 5. Aplasia |
|
|
Types of Errors in Organ Morphogenesis - Malformation
|
Intrinsic disruption; occurs during the embryonic period (weeks 3-8)
|
|
|
Types of Errors in Organ Morphogenesis - Deformation
|
Extrinsic disruption; occurs after the embryonic period.
|
|
|
Types of Errors in Organ Morphogenesis - Agenesis
|
Absent organ due to absent primordial tissue
|
|
|
Types of Errors in Organ Morphogenesis - Hypoplasia
|
Incomplete organ development; primordial tissue present.
|
|
|
Types of Errors in Organ Morphogenesis - Aplasia
|
Absent organ despite present primordial tissue.
|
|
|
What is the difference between agenesis and aplasia?
|
Both describe the absence of an organ. In aplasia, the absence occurs in spite of the presence of the primordial tissue. In agenesis, the absence occurs BECAUSE of the absence of the primordial tissue.
|
|
|
Teratogens - details?
|
Most susceptible in 3rd - 8th weeks (embryonic period - organogenesis) of pregnancy. Before week 3: all-or-none effects. After week 8: growth and function affected.
|
|
|
Teratogens - ACE inhibitors
|
Renal damage
|
|
|
Teratogens - Alkylating agents
|
Absence of digits, multiple anomalies
|
|
|
Teratogens - Aminoglycosides
|
CN VIII toxicity
|
|
|
Teratogens - Carbamazepine
|
Neural tube defects, craniofacial defects, fingernail hypoplasia, developmental delay, IUGR
|
|
|
Teratogens - Diethylstilbestrol (DES)
|
Vaginal clear cell adenocarcinoma
|
|
|
Teratogens - Folate antagonists
|
Neural tube defects
|
|
|
Teratogens - Lithium
|
Ebstein's anomaly (atrialized right ventricle)
|
|
|
Teratogens - Phenytoin
|
Fetal hydantoin syndrome: microcephaly, dysmorphic craniofacial features, hypoplastic nails and distal phalanges, cardiac defects, IUGR, mental retardation
hydanTOIN - phenyTOIN |
|
|
Teratogens - Tetracyclines
|
Discolored teeth
|
|
|
Teratogens - Thalidomide
|
Limb defects ("flipper" limbs)
|
|
|
Teratogens - Valproate
|
Inhibition of maternal folate absorption --> neural tube defects
|
|
|
Teratogens - Warfarin
|
Bone deformities, fetal hemorrhage, abortion, ophthalmalogic abnormalities
|
|
|
Teratogens - Alcohol
|
Leading cause of birth defects and mental retardation; fetal alcohol syndrome
|
|
|
Teratogens - Cocaine
|
Abnormal fetal development and fetal addiction; placental abruption
|
|
|
Teratogens - Smoking (nicotine, CO)
|
Preterm labor, placental problems, IUGR, ADHD
|
|
|
Teratogens - Iodide (lack or excess)
|
Congenital goiter or hypothyroidism
|
|
|
Teratogens - Maternal diabetes
|
Caudal regression syndrome (anal atresia to sirenomelia), congenital heart defects, neural tube defects
|
|
|
Teratogens - Vitamin A (excess)
|
Extremely high risk of spontaneous abortions and birth defects (cleft palate, cardiac abnormalities)
|
|
|
Teratogens - X-rays
|
Microcephaly, mental retardation
|
|
|
VACTERL
|
Mesodermal Defects:
Vertebral defects Anal Atresia Cardiac defects TracheoEsophageal fistula Renal defects Limb defects (bone and muscle) |
|
|
Fetal Alcohol Syndrome - Details?
|
Leading cause of congenital malformations in the US. Newborns of mothers who consumed significant amounts of alcohol during pregnancy have an increased incidence of congenital abnormalities, including pre- and postnatal developmental retardation, microcephaly, holoprosencephaly, facial abnormalities, limb dislocation, and heart and lung fistulas. Mechanism may include inhibition of cell migration.
|
|
|
What is thought to be the mechanism of Fetal Alcohol Syndrome?
|
Mechanism may involve inhibition of cell migration.
|
|
|
Twinning - details?
|
Dizygotic twins arise from 2 eggs that are separately fertilized by 2 different sperm (always 2 zygotes). Monozygotic twins arise from 1 fertilized egg (1 egg + 1 sperm) that splits into 2 zygotes in early pregnancy. The degree of separation between monozygotic twins depends on when the fertilized egg splits into 2 zygotes. The timing of this separation determines the number of chorions and the number of amnions. (See diagram on pp 128)
|
|
|
Number of Amnions and Chorions in monozygotic twinning when cleavage occurs at 0-4 days? 4-8 days? 8-12 days? >13 days?
|
0-4 days - Fused placenta or separate placenta. Dichorionic, diamniotic. (25%)
4-8 days - Monochorionic, diamniotic (75%) 8-12 days - monochorionic, monoamniotic (<1%) >13 days - monochorionic, monoamniotic, conjoined twins |
|
|
Placental development - Fetal component
|
Cytotrophoblast - inner layer of chorionic villi (Cyto makes Cells)
Syncytiotrophoblast - outer layer of chorionic villi; secretes hCG (structurally similar to LH; stimulates corpus luteum to secrete progesterone during first trimester) |
|
|
Placental development - Maternal component
|
Decidua basalis - derived from the endometrium. Maternal blood in lacunae.
|
|
|
Umbilical cord - details?
|
2 Umbilical Arteries - return deoxygenated blood from fetal internal iliac arteries to placenta (single umbilical artery is associated with congenital and chromosomal abnormalities)
1 Umbilical vein - supplies oxygenated blood from placenta to fetus; drains into IVC Umbilical arteries and vein are derived from allantois. |
|
|
Umbilical cord - Urachal duct abnormalities
|
3rd week - yolk sac forms allantois, which extends into urogenital sinus. Allantois becomes urachus, a duct between bladder and yolk sac.
Failure of urachus to obliterate: 1. Patent urachus - urine discharge from umbilicus 2. Vesicourachal diverticulum - outpouching of bladder |
|
|
Umbilical cord - Vitelline duct abnormalities
|
Vitelline duct (a.k.a. Yolk Sac)
7th week - obliteration of vitelline duct (omphalomesenteric duct), which connects yolk sac to midgut lumen Vitelline fistula - failure of duct to close --> meconium discharge from umbilicus Meckel's diverticulum -- partial closure, with patent portion attached to ileum. May have ectopic gastric mucosa --> melena and periumbilical pain. |
|
|
Truncus arteriosis (TA) - gives rise to?
|
Ascending aorta and pulmonary trunk
|
|
|
Bulbus cordis - gives rise to?
|
smooth parts (outflow tract) of left and right ventricle
|
|
|
Primitive ventricle - gives rise to?
|
Trabeculated left and right ventricles
|
|
|
Primitive atria - gives rise to?
|
Trabeculated left and right atrium
|
|
|
Left horn of sinus venosus (SV) - gives rise to?
|
Coronary sinus
|
|
|
Right horn of sinus venosus (SV) - gives rise to?
|
Smooth part of right atrium
|
|
|
Right common cardinal vein and right anterior cardinal vein - gives rise to?
|
SVC
|
|
|
Truncus Arteriosus - details?
|
Neural crest migration --> truncal and bulbar ridges that spiral and fuse to form the aorticopulmonary septum --> ascending aorta and pulmonary trunk
Pathology -- transposition of great vessels (failure to spiral), tetralogy of Fallot (skewed AP septum development), persistant TA (partial AP septum development) |
|
|
Interventricular septum development
|
1. Muscular ventricular septum forms. Opening is called interventricular foramen.
2. AP septum meets and fuses with muscular ventricular septum to form membranous interventricular septum, closing interventricular foramen 3. Growth of endocardial cushions separates atria from ventricles and contributes to both atrial separation and membranous portion of interventricular septum. Pathology - improper neural crest migration into the TA can result in transposition of the great arteries or a persistent TA. Membranous septal defect causes initial left-to-right shunting, which then becomes right-to-left shunting (Eisenmenger's syndrome). |
|
|
Interatrial septum development
|
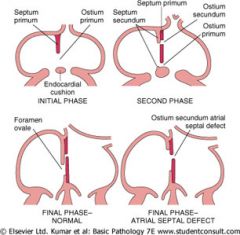
1. Foramen primum narrows as septum primum grows toward endocardial cushions.
2. Perforations in septum primum form foramen secundum (foramen primum disappears). 3. Foramen secundum maintains right-to-left shunt as septum secundum begins to grow. 4. Septum secundum contains a permanent opening (foramen ovale). 5. Foramen secundum enlarges and upper part of septum primum degenerates. 6. Remaining portion of septum primum forms valve of formaen ovale. 7. Septum secundum and septum primum fuse to form the atrial septum. 8. Foramen ovale usually closes soon after birth because of increased LA pressure. Pathology - patent foramen ovale, caused by excessive resorption of septum primum and/or secundum |
|
|
Fetal Erythropoiesis - 4 locations?
|
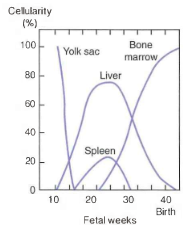
1. Yolk sac (3-10 wks)
2. Liver (6wks to birth) 3. Spleen (15-30 wks) 4. Bone marrow (22 wks to adult) "Young Liver Synthesizes Blood" |
|
|
Fetal circulation - details? 3 important shunts?
|
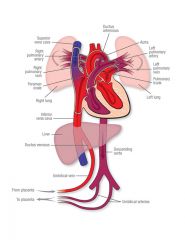
Blood in umbilical vein is 80% saturated with O2. Umbilical arteries have low O2 saturation.
3 important shunts: 1. Blood entering the fetus through the umbilical vein is conducted via the ductus venosus into the IVC to bypass the hepatic circulation. 2. Most oxygenated blood reaching the heart via the IVC is diverted through the foramen ovale and pumped out the aorta to the head and body. 3. Deoxygenated blood from the SVC is expelled into the pulmonary artery and ductus arteriosus to the lower body of the fetus. |
|
|
Fetal circulation - what happens shortly after birth
|
At birth, infant takes a breath; decreased resistance in the pulmonary vasculature causes increased left atrial pressure vs. right atrial pressure; foramen ovale closes (now called fossa ovalis).
Increased O2 leads to decrease in prostaglandins, causing closure of ductus arteriosus. Indomethacin helps close PDA. Prostaglandins keep PDA open. |
|
|
Fetal-postnatal derivatives - Umbilical vein becomes?
|
Ligamentum teres hepatis (contained in the falciform ligament)
|
|
|
Fetal-postnatal derivatives - Umbilical arteries become?
|
Medial umbilical ligaments
|
|
|
Fetal-postnatal derivatives - Ductus arteriosus becomes?
|
ligamentum arteriosum
|
|
|
Fetal-postnatal derivatives - Ductus venosus becomes?
|
ligamentum venosum
|
|
|
Fetal-postnatal derivatives - Foramen ovale becomes?
|
fossa ovalis
|
|
|
Fetal-postnatal derivatives - Allantois becomes?
|
Allantois (a.k.a. Urachus) becomes median umbilical ligament
The urachus is the part of the allantoic duct between the bladder and the umbilicus. Urachal cyst or sinus is a remnant. |
|
|
Fetal-postnatal derivatives - Notochord becomes?
|
nucleus pulposus of intervertebral disc
|
|
|
Regional specification of developing brain - Name three primary vesicles
|
Forebrain (prosencephalon), Midbrain (Mesencephalon), Hindbrain (rhombencephalon)
|
|
|
Regional specification of developing brain - Name five secondary vesicles (and their origin)
|
Telencephalon (from prosencephalon)
Diencephalon (from prosencephalon) Mesencephalon Metencephalon (from rhombencephalon) Myelencephalon (from rhombencephalon) |
|
|
Regional specification of developing brain - Telencephalon walls? cavities?
|
Walls - Cerebral hemispheres
Cavities - Lateral ventricles |
|
|
Regional specification of developing brain - Diencephalon walls? cavity?
|
Walls - Thalamus
Cavity - Third ventricle |
|
|
Regional specification of developing brain - Mesencephalon walls? Cavity?
|
Walls - Midbrain
Cavity - Aqueduct |
|
|
Regional specification of developing brain - Metencephalon walls? cavity?
|
Walls - Pons and Cerebellum
Cavity - Upper part of fourth ventricle |
|
|
Regional specification of developing brain - Myelencephalon walls? cavity?
|
Walls - Medulla
Cavity - Lower part of fourth ventricle |
|
|
Neural Tube Defects - details?
|
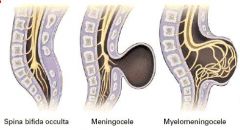
Neuropores fail to fuse (4th week) --> persistent connection between amniotic cavity and spinal canal. Associated with low folic acid intake during pregnancy.
Elevated alpha-fetoprotein (AFP) in amniotic fluid and maternal serum. Increased AFP + acetylcholinesterase in amniotic fluid. |
|
|
Neural Tube Defects - Spina bifida occulta?
|
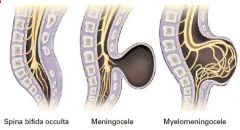
failure of bony spinal canal to close, but no structural herniation. Usually seen at lower vertebral levels. Dura is intact.
See tuft of hair. |
|
|
Neural Tube Defects - Meningocele
|
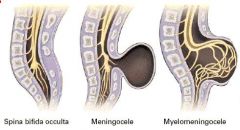
Meninges herniate through spinal canal defect. Dura broken.
|
|
|
Neural Tube Defects - Meningomyelocele
|
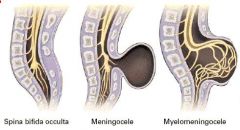
Meninges and spinal cord herniate through spinal canal defect. Dura broken.
|
|
|
What structures develop from the 1st pharyngeal pouch? Groove? Membrane?
|
1st pouch - epithelium of middle ear and auditory tube
1st Membrane - Tympanic membrane 1st groove - Epithelium of external ear canal |
|
|
What structures develop from the 2nd pharyngeal pouch? Groove? Membrane?
|
2nd pouch - Epithelium of palatine tonsil crypts
2nd membrane - obliterated 2nd groove - obliterated |
|
|
What structures develop from the 3rd pharyngeal pouch? Groove? Membrane?
|
3rd pouch - Thymus, inferior parathyroid glands
3rd membrane - obliterated 3rd groove - obliterated |
|
|
What structures develop from the 4th pharyngeal pouch? Groove? Membrane?
|
4th pouch - Superior parathyroid glands, ultimobranchial body
4th groove - obliterated 4th membrane - obliterated |
|
|
Aortic arch derivatives - 1st arch
|
Develops into part of the maxillary artery (branch of external carotid).
1st arch is MAXimal. |
|
|
Aortic arch derivatives - 2nd arch
|
Develops into the stapedial artery and hyoid artery.
Second = Stapedial |
|
|
Aortic arch derivatives - 3rd arch
|
Develops into the common Carotid artery and proximal part of the internal carotid artery.
C is the 3rd letter of the alphabet. |
|
|
Aortic arch derivatives - 4th arch
|
On the left, develops into the aortic arch.
On the right, develops into the proximal part of the right subclavian artery. 4th arch (4 limbs) = systemic. |
|
|
Aortic arch derivatives - 6th arch
|
Develosp into the proximal part of pulmonary arteries and (on left only) ductus arteriosus.
6th arch = pulmonary and the pulmonary-to-systemic shunt (ductus arteriosus) |
|
|
Branchial apparatus - What layer of gastrula for Clefts? Arches? Pouches?
|
Also called pharyngeal apparatus. Composed of branchial clefts, arches, and pouches.
Branchial clefts - derived from ectoderm. Also called branchial grooves. Branchial arches - derived from mesoderm (muscles, arteries) and neural crest (bones, cartilage). Branchial pouches - derived from endoderm |
|
|
How to remember the layers of the gastrula that lead to the various parts of the branchial apparatus?
|
CAP covers outside from inside:
Clefts = ectoderm Arches = mesoderm Pouches = endoderm |
|
|
Branchial cleft derivatives - 1st? 2nd - 4th? Persistent cervical sinus?
|
1st - develops into external auditory meatus
2nd - 4th - form temporary cervical sinuses, which are obliterated by proliferation of the second arch mesenchyme. Persistent cervical sinus --> branchial cleft cyst within lateral neck |
|
|
Branchial arch derivatives - 1st arch (Cartilage? Muscles? Nerves? Abnormalities?)
|
Cartilage - Meckel's cartilage: Mandible, Malleus, incus, spheno-Mandibular ligament
Muscles - Muscles of Mastication (temporalis, Masseter, lateral and Medial pterygoids), Mylohyoid, anterior belly of digastric, tensor tympani, tensor veli palatini Nerves - CN V2 and V3 chew Abnormalities: Treacher Collins syndrome - 1st arch neural crest fails to migrate --> mandibular hypoplasia, facial abnormalities |
|
|
What is Treacher Collins syndrome?
|

1st branchial arch neural crest fails to migrate --> mandibular hypoplasia, facial abnormalities
|
|
|
Branchial arch derivatives - 2nd arch (Cartilage? Muscles? Nerves?)
|
Cartilage: Reichert's cartilage - Stapes, Styloid process, lesser horn of hyoid, Stylohyoid ligament
Muscles: muscles of facial expression, Stapedius, Stylohyoid, posterior belly of digastric Nerves: CN VII (facial expression), smile |
|
|
Branchial arch derivatives - 3rd arch (Cartilage? Muscles? Nerves? Abnormalities?)
|
Cartilage - greater horn of hyoid
Muscles: Stylopharyngeus (think of stylo-pharyngeus innervated by glossopharyngeal nerve) Nerves: CN IX (innervates stylopharyngeus) - swallow stylishly Abnormalities: Congenital pharyngocutaneous fistula - persistence of cleft and pouch --> fistula between tonsillar area, cleft in lateral neck |
|
|
Branchial arch derivatives - 4-6 arches (Cartilage? Muscles? Nerves? Comments?)
|
Cartilages: thyroid, cricoid, arytenoids, cornicuate, cuneiform
Muscles: 4th arch - most pharyngeal constrictors, cricothyroid, levator veli palatini 6th arch - all intrinsic muscles of larynx EXCEPT cricothyroid Nerves: 4th arch - CN X (superior laryngeal branch) simply swallow 6th arch - CN X (recurrent laryngeal branch) speak Comments: Arches 3 and 4 form posterior 1/3 of tongue; arch 5 makes no major developmental contributions |
|
|
How to remember the major functions of the branchial arches?
|
When at the restaurant of the golden arches, children tend to first chew (1), then smile (2), then stylishly swallow (3), or simply swallow (4) and then speak (6).
|
|
|
Branchial pouch derivatives - 1st pouch
|
develops into middle ear cavity, eustachian tube, mastoid air cells.
1st pouch contributes to endoderm-lined structures of the ear. |
|
|
Branchial pouch derivatives - 2nd pouch
|
develops into epithelial lining of palatine tonsil
|
|
|
Branchial pouch derivatives - 3rd pouch (dorsal wings)
|
develops into inferior parathyroids
|
|
|
Branchial pouch derivatives - 3rd pouch (ventral wings)
|
develops into thymus
|
|
|
Branchial pouch derivatives - 4th pouch (dorsal wings)
|
develops into superior parathyroids
3rd pouch structures end up BELOW 4th pouch structures |
|
|
what 3 major structures does the 3rd pharyngeal pouch contribute to?
|
right and left Inferior parathyroids, thymus
|
|
|
Branchial pouch derivatives - Aberrant development of 3rd and 4th pouches
|
DiGeorge syndrome --> T cell deficiency (thymic aplasia) and hypocalcemia (failure of parathyroid development)
|
|
|
How to remember the derivatives of the 4 pharyngeal pouches?
|
Ear, tonsils, bottom-to-top:
1 (ear), 2 (tonsils), 3 dorsal (bottom for inferior parathyroid), 3 ventral (to = thymus), 4 (top = superior parathyroids) |
|
|
Branchial pouch derivatives - MEN 2A
|
mutation of germline RET (neural crest cells)
-Adrenal medulla (pheochromocytoma) -Parathyroid (tumor): 3rd/4th pharyngeal pouch - Parafollicular cells (medullary thyroid cancer): derived from neural crest cells; associated with the 4th/5th pharyngeal pouches |
|
|
Tongue Development
|
1st branchial arch forms anterior 2/3 (thus sensation via CN V3 and taste via CN VII)
3rd and 4th arches form posterior 1/3 (thus sensation and taste mainly via CN IX, extreme posterior via CN X) Motor innervation is via CN XII. Muscles of the tongue are derived from occipital myotomes. |
|
|
What nerves are involved in taste sensation of the tongue? Pain? Motor?
|
Taste - CN VII, IX, X (solitary nucleus)
Pain - CN V3, IX, X Motor - CN XII |
|
|
Thyroid Development - details? Thyroglossal duct cyst?
|
Thyroid diverticulum arises from floor of primitive pharynx, descends into neck. Connected to tongue by thyroglossal duct, which normally disappears but may persist as pyramidal lobe of thyroid. Foramen cecum is normal remnant of thyroglossal duct. Most common ectopic thyroid tissue site is the tongue.
Thyroglossal duct cyst in midline neck and will move with swallowing (vs. persistent cervical sinus leading to branchial cleft cyst in lateral neck). |
|
|
What is the most common ectopic thyroid tissue site?
|
Base of the tongue
|
|
|
Cleft lip and cleft palate
|
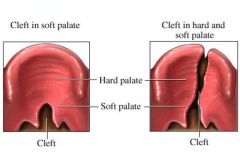
Cleft lip - failure of fusion of the maxillary and medial nasal processes (formation of primary palate)
Cleft palate - failure of fusion of the lateral palatine processes, the nasal septum, and/or the median palatine process (formation of secondary palate) Cleft lip and cleft palate have two distinct etiologies, but often occur together. |
|
|
GI embryology - Foregut? Midgut? Hindgut?
|
Foregut - pharynx to duodenum
Midgut - duodenum to transverse colon Hindgut - distal transverse colon to rectum |
|
|
GI embryology - Developmental defects of anterior abdominal wall due to failure of: Rostral fold closure? Lateral fold closure? Caudal fold closure?
|
Rostal fold closure: Sternal defects
Lateral fold closure: omphalocele, gastroschisis Caudal fold closure: bladder exstrophy |
|
|
GI embryology - Duodenal atresia
|
failure to recanalize (trisomy 21)
|
|
|
GI embryology - Jejunal, ileal, colonic atresia
|
Due to vascular accident (apple peel atresia)
|
|
|
GI embryology - Midgut development - 6th week? 10th week? Pathology?
|
6th week - midgut herniates through umbilical ring
10th week - returns to abdominal cavity + rotates around SMA Pathology - malrotation of midgut, omphalocele, intestinal atresia or stenosis, volvulus |
|
|
GI embryology - Gastroschisis vs. Omphalocele
|
Gastroschisis - extrusion of abdominal contents through abdominal folds; not covered by peritoneum
Omphalocele - persistence of herniation of abdominal contents into umbilical cord, covered by peritoneum |
|
|
Tracheoesophageal fistula
|
Abnormal connection between esophagus and trachea.
Most common subtype is blind upper esophagus with lower esophagus connected to trachea (type C). Results in cyanosis, choking and vomiting with feeding, air bubble in stomach on CXR, polyhydramnios, failure to pass NG tube into stomach, and pneumonitis. |
|
|
Describe the anatomy of the most common TE fistula. What letter designation?
|
Type C - Blind upper esophagus with lower esophagus connected to trachea
|
|
|
Congenital pyloric stenosis
|
Hypertrophy of the pylorus causes obstruction. Palpable "olive" mass in epigastric region and nonbilious projectile vomiting at ~ 2 weeks of age. Treatment is surgical incision. Occurs in 1/600 live births, often in 1st born males.
|
|
|
Pancreas and spleen embryology - Pancreas
|
derived from foregut. Ventral pancreatic buds contribute to the pancreatic head and main pancreatic duct. The uncinate process is formed by the ventral bud alone. The dorsal pancreatic bud becomes everything else (body, tail, isthmus, and accessory pancreatic duct).
|
|
|
Pancreas and spleen embryology - Annular pancreas
|
ventral pancreatic bud abnormally encircles 2nd part of duodenum; forms a ring of pancreatic tissue that may cause duodenal narrowing
|
|
|
Pancreas and spleen embryology - Pancreas divisum
|
ventral and dorsal parts fail to fuse at 8 weeks
|
|
|
Pancreas and spleen embryology - Spleen
|
arises from dorsal mesentery (hence is mesodermal) but is supplied by artery of foregut (celiac artery)
|
|
|
Kidney embryology - Pronephros
|
week 4; then degenerates
|
|
|
Kidney embryology - Mesonephros
|
functions as interim kidney for 1st trimester; later contributes to male genital system
|
|
|
Kidney embryology - Metanephros
|
permanent; beginnings first appear during 5th week of gestation; nephrogenesis continues through 32-36 weeks of gestation
|
|
|
Kidney embryology - Ureteric bud
|
Derived from caudal end of mesonephros; gives rise to ureter, pelvises, and, through branching, calyces and collecting ducts; fully canalized by 10th week
|
|
|
Kidney embryology - Metanephric mesenchyme
|
Ureteric bud interacts with this tissue; interaction induces differentiation and formation of glomerulus and renal tubules to distal convoluted tubule
- aberrant interaction between these 2 tissues may result in several congenital malformations of the kidney |
|
|
Kidney embryology - Ureteropelvic junction with kidney
|
Last to canalize --> most common site of obstruction (hydronephrosis) in fetus
|
|
|
Potter's syndrome
|
Bilateral renal agenesis --> oligohydramnios --> limb deformities, facial deformities, pulmonary hypoplasia. Caused by malformation of ureteric bud
|
|
|
Horseshoe kidney
|
Inferior poles of both kidneys fuse. As they ascend from pelvis during fetal development, horseshoe kidneys get trapped under inferior mesenteric artery and remain low in the abdomen. Kidney functions normally. Associated with Turner syndrome.
|
|
|
Genital embryology - Female
|

Default development. Mesonephric duct degenerates and paramesonephric duct develops.
Mesonephric duct must be induced to remain; default program for embryo development is for paramesonephric duct to develop into female. |
|
|
Genital embryology - Male
|
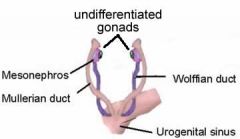
SRY gene on Y chromosome -- produces testis-determining factor (testes development).
Mullerian inhibitory factor from Sertoli cells --> suppresses development of paramesonephric ducts. Increased androgens from Leydig cells --> stimulates development of mesonephric ducts. |
|
|
Genital embryology - Mesonephric (wolffian) duct
|
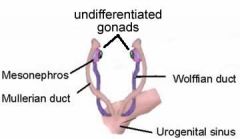
Develops into male internal structures (except prostate) -- Seminal vesicles, epididymis, Ejaculatory duct, and Ductus deferens (SEED)
|
|
|
Genital embryology - Paramesonephric (mullerian) duct
|
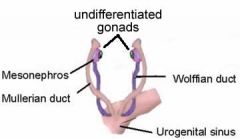
Develops into female internal structures -- fallopian tube, uterus, and upper portion of vagina (lower portion from urogenital sinus). Mullerian duct abnormalities result in anatomical defects that may present as primary amenorrhea in females with fully developed secondary sexual characteristics (indicator of functional ovaries).
|
|
|
Bicornuate uterus
|
Results from incomplete fusion of the paramesonephric ducts. Associated with urinary tract problems and infertility.
|
|
|
Explain the actions of the SRY gene
|
SRY gene on Y chromosome --> Testis-determining factor production
Testis-determining factor --> activation of Sertoli cells to secrete Antimullerian hormone --> degeneration of paramesonephric (mullerian) duct (female internal genitalia) Testis-determining factor --> Leydig cell --> secretes testosterone --> Wolffian duct develops into Male internal genitalia (except prostate) Testosterone is converted to DHT by 5alpha-reductase leading to genital tubercle and urogenital sinus development into male external genitalia, and prostate gland, respectively |
|
|
Male embryology - no Sertoli cell or lack of anti-mullerian hormone
|
Develop both male and female internal genitalia and male external genitalia
|
|
|
Male embryology - 5alpha reductase deficiency
|
Male internal genitalia, ambiguous external genitalia until puberty
|
|
|
Male/female genital homologues - Genital tubercle (Estrogen? DHT?)
|
Estrogen - Glans clitoris, vestibular bulbs
DHT - Glans penis, corpus cavernosum and spongiosum |
|
|
Male/female genital homologues - Urogenital sinus (Estrogen? DHT?)
|
Estrogen - Greater vestibular glands (of Bartholin), urethral and paraurethral glands (of Skene)
DHT - Bulbourethral glands (of Cowper), Prostate gland |
|
|
Male/female genital homologues - Urogenital folds (Estrogen? DHT?)
|
Estrogen - Labia minora
DHT - Ventral shaft of penis (penile urethra) |
|
|
Male/female genital homologues - Labioscrotal swelling (Estrogen? DHT?)
|
Estrogen - Labia majora
DHT - Scrotum |
|
|
Congenital penile abnormalities - Hypospadias
|
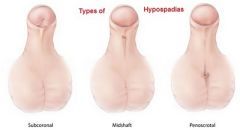
abnormal opening of penile urethra on inferior (ventral) side of penis due to failure of urethral folds to close
Hypospadias is more common than epispadias. Fix hypospadias to prevent UTIs. |
|
|
Congenital penile abnormalities - Epispadias
|
Abnormal opening of penile urethra on superior (dorsal) side of penis due to faulty positioning of genital tubercle.
Exstrophy of the bladder is associated with Epispadias. |
|
|
Descent of testes and ovaries - Gubernaculum (band of fibrous tissue) - Female remnant? Male remnant?
|
Female remnant: Ovarian ligament + round ligament of uterus
Male remnant: Anchors testes within scrotum |
|
|
Descent of testes and ovaries - Processus vaginalis (evagination of peritoneum) - Female remnant? Male remnant?
|
Female remnant: obliterated
Male remnant: Forms tunica vaginalis |
|
|
how does valproate induce teratogenicity?
|
inhibits intestinal folic acid absorption
|
|
|
If there is a twin question and there is a male and female on ultrasound what should you be thinking?
|
Dizygotic twins - they have to be the same sex in order to be monozygotic!!!
|
|
|
21 day old baby cocks head to one side and has pain when the neck is cocked the other way - waht is it?
|
Congenital torticollis - SCM fibrosis from fetal malposition or birth trauma, can be associated with cervical spine abnormalities and you should always get radiographs to check
|
|
|
What is the most common cause of FETAL hydronephrosis?
|
obstruction of the ureteropelvic junction - NOT the vesicoureteral junction (that type does not develop until antenatally)
|
|
|
What is the rule of 2's with Meckel's diverticulum?
|
2% of the population
2 feet from the ileocecal valve 2 inches in length 2% are symptomatic 2x more likely in males |
|
|
What are the fourth pathologies associated with failure of full degeneration of the vitelline duct?
|
1. Persistent vitelline duct - connection between ileum and externally through the umbilicus
2. Vitelline duct cyst - ends of the vitelline duct are closed but the middle remains fluid filled. Asymptomatic. 3. Meckel diverticulum - umbilicus portion closes but ileum portion stays open, usually asymptomatic but may present with rectal bleeding or SBO 4. Vitelline sinus - ileum side closed but umbilicus side open |
|
|
What are the main causes of polyhydramnios?
|
GI obstruction (duodenal, esophageal or intestinal atresia)
Hydrocephalus |
|
|
What direction do neural crest cells migrate during gestation in terms of segments of the intestines that become innervated?
|
Cranial --> caudal
Rectum is last. |
|
|
If you see a baby with cyanosis and a PDA, what should you immediately think?
|
Cyanotic lesion (first one i think of is Transposition of the Great Arteries)
|
|
|
Hydrocele can be associated with what type of hernia?
|
Indirect inguinal
|
|
|
What is the cause of ileal atresia? and jejunal/colic atresias?
|
Vascular accident - NOT a congenital abnormality but an ischemic event in utero - leads to "apple peel atresia" where the ileum winds around the ischemic SMA
|
|
|
Although the blastocyst starts secreting hCG around day 5.5, it can not be detected in the blood until after implantation. Why?
|
It does not spill into the mother's blood stream until then.
|
|
|
What is different between false diverticulum and true diverticulum?
|
Meckel's is a true, it has mucosa, submucosa, and muscular layers.
False diverticula only have mucosa and submucosa. |
|
|
What objects fuse to form the lip? The palate?
|
Lip - Fusion of the two medial nasal prominences creates the midline intermaxillary segment. This then fuses with the left and right maxillary prominences.
Palate - The intermaxillary segment (primary palate) is connected by medial growth of the two maxillary prominences (secondary palate). |
|
|
Why are craniopharyngiomas associated with the pituitary gland?
|
They come from remnants of Rathke's pouch, an evagination of the ectoderm that lines the fecal-oral cavity. This protrusion of the roof of the mouth forms the anterior portion of the pituitary (adenohypophysis). The posterior lobe of the pituitary (neurohypophysis) develops from the neuroectoderm.
|
|
|
What is the most common other defect associated with anal atresia?
|
Urinary tract defects - hindgut derivatives, much more common than VACTERL syndrome
|
|
|
What are the three major venous systems in the developing embryo?
|
Cardinal - turn into systemic veins
Vitelline - form the portal veins Umbilical - degenerate |
|
|
What is the most common tissue present in ectopic cells from Meckel's diverticulum?
|
gastric mucosa - secretes acid
(can also develop pancreatic, and other types) |
|
|
What two proteins are elevated and detected to diagnose neural tube defects in utero?
|
Alpha-fetoprotein (AFP) and acetylcholinesterase
|
|
|
What are the heart defects in tetralogy of fallot?
|
Overriding aorta, pulmonary stenosis, ventricular septal defect, RVH
|
|
|
Explain Tet spells?
|
In tetralogy of fallot, right-to-left shunting of blood occurs across the VSD due to pulmonary stenosis. When a child squats they increase systemic blood pressure which forces blood across the pulmonary valve (thus less blood bypasses the lungs).
|
|
|
What cells come from the neural crest?
|
Think PNS and non-neural structures nearby!
ANS, dorsal root ganglia, cranial nerves, celiac ganglion, melanocytes, chromaffin cells of adrenal medulla, parafollicular (C) cells of thyroid, Scwann cells, pia and arachnoid, bones of the skull, odontoblasts, aorticopulmonary septum |
|
|
Is epispadias or hypospadias the result of a failure of two structures to fuse?
|
Hypospadias - failure of urethral folds to fuse
Epispadias is due to improper positioning of the genital tubercle. |
|
|
What are the two most common causes of eugonadotropic amenorrhea?
|
Incomplete canalization of the vaginal plate and mullerian duct anomalies
|
|
|
Posterior fossa malformations - Arnold-Chiari II
|
Cerebellar tonsillar and vermal herniation through foramen magnum with aqeuductal stenosis and hydrocephaly. Often presents with thoraco-lumbar myelomeningocele and paralysis below the lesion.
|
|
|
Posterior Fossa malformations - Dandy-walker
|
Large posterior fossa; absent cerebellar vermis with cystic enlargement of 4th ventricle. Can lead to hydrocephalus and spina bifida.
|
|
|
Syringomyelia
|
Enlargement of the central canal of spinal cord. Crossing fibers of spinothalamic tract are typically damaged first. "Cape-like" bilateral loss of pain and temperature sensation in upper extremities with preservation of touch sensation.
Associated with Chiari I malformation. Most common at C8-T1. |
|
|
A child presents with microcephaly, microphthalmia, and omphalocele, what genetic disease may she have?
|
Trisomy 13 (Patau syndrome)
|
|
|
A child with an underdeveloped mandible may also have underdevelopment of what ossicle?
|
Malleus
|