Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
119 Cards in this Set
- Front
- Back
|
Cell Body
|

Single nucleus
Protein synthesis |
|
|
Dendrites
|

Short, highly branching extensions
input summation this is where the other nerve cells contact this nerve cell and form a synapse The more dendrites = the more synapses made (multiple contact points) |
|
|
Axons
|

Often long cell process
Conduct Action potentials sends signals long distances, it's a wire for transmitting action potentials |
|
|
Neuron Variations
|
Multi-Polar Neuron
Bipolar Neuron Pseudo-Unipolar Neuron |
|
|
Major Functions of the nervous System
|
Major functions:
Sensory input Integration = Processing Motor output Homeostasis Mental activity |
|
|
Major divisions of Nervous System
|
Major divisions
CNS: brain and spinal cord PNS: nerves and ganglia outside of CNS |
|
|
Glial Cells
|

Glial cells are the nonneuronal cells of the nervous system: Found in the brain (brain cells)
Characteristics More numerous than neurons (nerve cells) Can divide myelin sheaths wrap around axons of neural cells Cell types CNS: oligodendrocytes PNS: Schwann cells |
|
|
Astrocytes
|
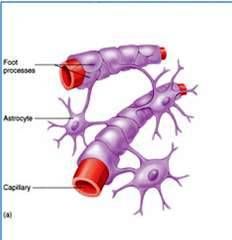
Major support cell in CNS
Limit damage to neurons Help form blood-brain barrier Astrocytes care for the nerve cells a lot. Most Numerous |
|
|
Ependymal cells
|
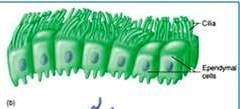
Ciliated; line cavities
Produce and move CSF |
|
|
Microglia
|
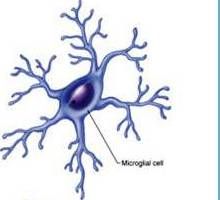
Immune Cells
Derived from macrophages Remove bacteria and cell debris Found in Brain and Spine |
|
|
oligodendrocytes
|
CNS
|
|
|
Schwann cells
|
PNS
|
|
|
Myelin
|
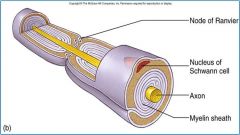
Lipid insulator
Blocks ionic currents |
|
|
Nodes of Ranvier
|
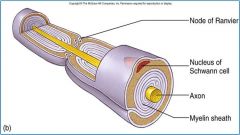
Breaks in myelin; action potential generation
What would be expected in great abundance in these nodes? |
|
|
Central Nervous System
|
The central nervous system consists of the brain and spinal cord.
|
|
|
Peripheral Nervous System
|
The peripheral nervous system consists of all the nervous tissue outside the CNS (nerves and ganglial)
|
|
|
Sensory Division (Peripheral Nervous System
|
The sensory division, or afferent division, conducts action potentials from sensory receptors to the CNS. The neurons that transmit action potentials from the periphery to the CNS are called sensory neurons.
The motor division, efferent division, conducts action potentials from the CNS to effector organs, such as muscles and glands. The neurons that transmit action potentials from CNS toward the periphery are called motor neurons. |
|
|
Somatic Nervous (Peripheral Nervous System)
|
The motor division can be further subdivided into the somatic nervous system, which transmits action potentials from the CNS to skeletal muscles.
|
|
|
Autonomic Nervous System
|
ANS transmits action potentials from the CNS to cardiac muscle, smooth muscle, and glands. The autonomic nervous system, in turn, is divided into sympathetic and parasympathetic divisions.
|
|
|
Enteric Nervous System
|
ENS is a unique subdivision of the PNS. The ENS has both sensory and motor neurons contained wholly within the digestive tract. The ENS can function without input from the CNS or other parts of the PNS, although it is normally integrated with the CNS by sensory neurons and ANS motor neurons.
|
|
|
Neurons
|
nerve cells receive stimuli, conduct action potentials, and transmit signals to other neurons or effector organs. There are three parts to a neuron: a cell body and two types of processes, called dendrites and axons.
Nerve cells don't divide after they have reached their stopping point. (the only exception is in the nose) |
|
|
Describe the respective roles of the major divisions of the nervous system under the circumstance of encountering a bear.
|
Involuntary (Autonomic) = sweat, heart rate increases, smooth muscles and blood vessels could change diameter so you have more blood flow.
Voluntary (Somatic) = scream, run |
|
|
Afferent vs. Efferent
|
Afferent = information from PNS into the CNS; Sensory Information
Efferent = information from CNS into muscles; Muscle control |
|
|
What is Electrochemical Equilibrium?
Would net diffusion continue until the intracellular and extracellular concentrations of the ion were equal? |
Potential (charge difference) across cell membrane when no longer any net movement of ion
1) Greater concentration of chloride in the extracellular fluid compared to the intracellular (Thus making a diffusion gradient pushing chloride in). 2) The inside of the cell must have a net negative charge (thus forming the electrical field pushing chloride out). Diffusion would not continue. Diffusion would stop because ions are electrically charged (there will always be a bit on one side or the other) |
|
|
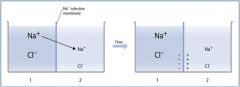
Describe how diffusion of an ion across a membrane (through a channel) results in the generation of a potential.
|
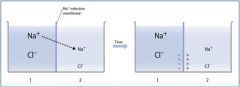
Membrane permeable only to Na+
Since [Na+ ] is higher in Box 1, it diffuses (chemical force) to Box 2 Diffusion continues until positive charge accumulating in Box 2 begins to push back (electrical force) and prevent any further net Na+ diffusion |
|
|
How is the resting membrane potential established?
What is a typical value for the resting membrane potential? |
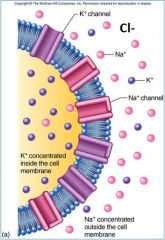
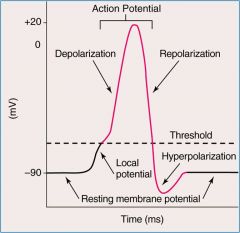
Interior of cell membrane slightly more negative than exterior
Leaky channels (more for K+ and Cl-). K leaks OUT of cell (this causes equilibrium) making the interior more negatively charged. Cl (higher concentration outside) leaks into cell making the interior more negative, again. Potential at equilibrium around -70 mV (negative) to -80 mV |
|
|
Describe the phases of the action potential. Explain the underlying basis of these phases in terms of the activity of voltage-gated ion channels.
|
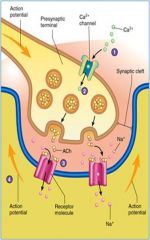
1. NT binds its receptors
2. Ion channels open (by ACh) 3. Ion flow across cell membrane (Sodium flows in) 4. Membrane potential changes (Na+ makes cell positive) 5. Local ion currents flow along the interior of the membrane until they dissipate (MAY or MAY NOT cause signal to flow) |
|
|
Leak Channels
|
Leaky ion channels are ALWAYS open. Allows ions to leak across membrane down their concentration gradients.
|
|
|
Synapse
|
A synapse is a junction where the axon of one neuron interacts with another neuron or with an effector organ, such as a muscle or gland.
|
|
|
Local Current
|
When an ion flows directly across the chemical gated channels (controlled by ACh) and causes a change in charge making a potential.
Like in neuromuscular junction with Sodium. |
|
|
Describe how action potentials move across the membrane (in excitable cells).
|
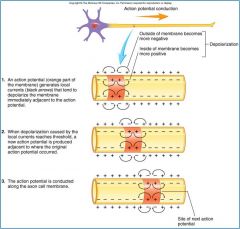
Controlled by ion channels. Specifically VOLTAGE gated channels. Local currents start process at synapse (chemically gated), sodium flows in, Voltage gated Na channels sense the charge and open. TONS MORE Na flows in.
Depolarization Potential becomes more positive Often Na+ influx Repolarization Potential returns to resting potential Often K+ efflux Hyperpolarization Potential becomes more negative than resting potential |
|
|
What is a Threshold Potential?
What is a Strong Depolarization? |

Threshold potential
Voltage-gated Na+ channels (NaVs) open only if local current makes the interior of cell membrane positive enough “All or none” Strong depolarization NaVs open and even greater amount of Na+ rushes in the cell Potential becomes much more positive |
|
|
What happens in the cell immediately after strong depolarization?
|

NaVs do not stay open long as inactivation gates quickly close
Unidirectional movement of action potentials Repolarization Interior of the cell membrane begin to return to resting potential as Na+ flow stops and K+ rushes out |
|
|
Why doesn't the charge flow in both directions down and up the axon?
|
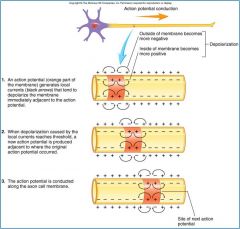
After gated channels close they have to "recover" basically and are inactive for a time. So if (which it does) a positive current flows in the opposite direction (than down the axon) the gates will not respond.
|
|
|
Why are action potentials said to be “non-decremental”?
|
This refers to the strength of the action potential (depolarization/repolarization) down the axon getting weaker.
It stays strong because there's a ton of sodium rushing in. Der... |
|
|
How does myelin increase the conduction velocity of action potentials? What other property of axons allows very rapid conduction of action potentials?
|

Myelin is a lipid insulator for these excitable cells.
Nodes of Ranvier are the breaks in between each Schwann Cell (Myelin wrapped). The action potential jump the node of ranvier and travel through the myelin conduction making it go much FASTER. This is also called Saltatory Conduction. When it travels through the schwann cell it's incredibly positive causing Na channels to open and more Na rushes in making it more positive, then it's more positive causing more Na to rush in (and on and on and on) |
|
|
Presynaptic Cell? Postsynaptic Cell? Synaptic Cleft?
How would the postsynaptic membrane potential change if neurotransmitter binding resulted in the opening of chloride channels? |
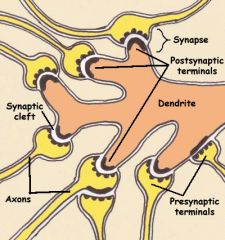
Presynaptic = the end of the axon
Postsynaptic = membrane of the dendrite or effector cell Synaptic Cleft = the space separating the pre- and post- Cl- would cause hyperpolarization, making it less likely to fire an action potential, makes it more negative making it harder to become positive.. |
|
|
Excitatory Synapse? Inhibitory Synapse?
|
Excitatory = tries to increase the chance that the site will generate an action potential
(Na+) Inhibitory = decrease the chance for action potential (Cl-) |
|
|
What determines whether a neuron will generate an action potential?
|
Basically... It's the summation of all the action potential inputs
and whether they pass the threshold |
|
|
Spinal Cord Anatomy
|
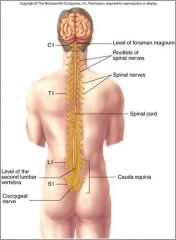
Extends from foramen magnum to 2nd lumbar vertebra
Major divisions: cervical, thoracic, lumbar and sacral 31 pairs of spinal nerves (sensory=afferent and motor=efferent) |
|
|
Cross Section of Spinal Cord Anatomy
|
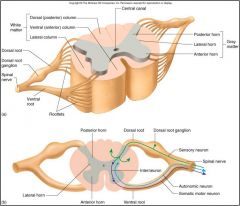
White matter: myelinated axons
Axons run in ascending and descending tracts Gray matter : neuron cell bodies; found in dorsal and ventral horns Spinal nerves arise from rootlets along dorsal and ventral surfaces Sensory info contacts Dorsal Horns. Motor Neurons are found in Ventral Horns. Central canal contains CSF |
|
|
Provide an example of a spinal reflex. Include a brief description the circuitry required.
|

Rapid, involuntary reactions; important for protection, basically when your body doesn't have time to run through a full neural process
Patellar reflex = knee moves Withdrawal reflex = hot stove There are nerve cells just below the surface of the skin. When tissue is damaged ion channels are opened. The sensation travels and connects to dorsal horn, which then sends it out. It also contacts neurons in the gray matter which then sends it to ventral horn which creates a quick motor function. {inhibitory neural cells would cause relaxation of other muscles, while excitable contract others} |
|
|
Basic Brain Structure
|
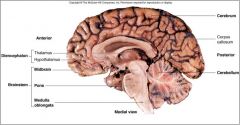
Brainstem
Diencephalon Cerebellum Cerebrum |
|
|
Brainstem Structure
|
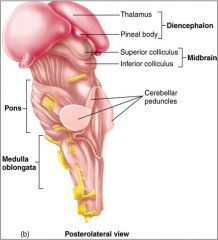
Controls Autonomic Voluntary Functions (has nerves ALL over)
Medulla oblongata = Autonomic functions - Cardiovascular and breathing Reflexes - Swallowing, vomiting, coughing and sneezing Motor tracts - Pyramids on anterior surface Pons = Autonomic functions - Breathing Connects cerebellum and cerebrum Midbrain = Visual reflexes (superior colliculus) Auditory relay Balance and regulation of body movement |
|
|
Cerebellum Structure
|
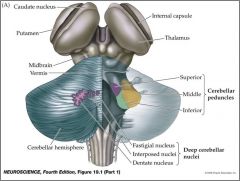
Attached to brainstem (by cerebellar peduncles)
Numerous gyri (the folds) and sulci (the indention between the folds); cortex larger than half of cerebral cortex (contains most of the grey matter, lots of nerves) white matter contains axons {nuclei hear means = clusters of nerve cells} Involved in motor function, motor balance, posture, motor learning |
|
|
Diencephalon Structure
|
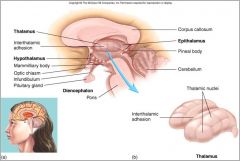
Found in between the brain.
Thalmus has lots of relay cells (nuclei) that contact the cerebrum (its a stopping place for information either efferent or afferent) Hypothalmus Maintains Homeostasis - Body Temperature - Water Balances (thirst) - fuel levels (hunger) Endocrine Functions - (decides) hormone releases |
|
|
Basic Cerebrum Structure
|
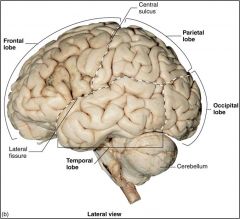
Gyri = the actual coral reef part
Sulci = the fissures or cracks in the coral reef Thin cortex contains gray matter Sulci and Gyri help to really compact the large number of connection points for the cortex White matter has lots of myelinated axons. More white than gray matter. Right and Left hemispheres 4 Lobes Each - Frontal - Parietal - Temporal - Occipital |
|
|
The Meninges
|
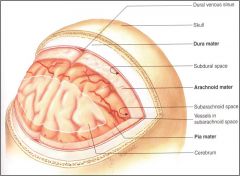
Connective tissue membranes surround and protect CNS structures
Dura mater (tough mother): most superficial, thickest; folds form venous sinuses Arachnoid mater (thinner, looks like spider web): underneath dura mater Pia mater (affectionate mother, hugs brain): tightly adheres to brain and spinal cord What are the consequences of a subdural hematoma over the right frontal lobe? |
|
|
Meninges around Spine
|
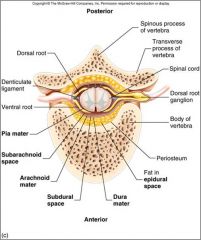
Dura Mater
Arachnoid Mater Pia Mater Epidural space - Space between bone and dura mater - injection site for anesthesia during labor Subarachnoid space - between arachnoid and pia - spinal block (also for anesthesia) or spinal tap to sample CSF - insertion in space below inferior spine, to avoid damaging the spine, if you do it below it will travel upward through the space |
|
|
Describe the production, circulation and drainage of Cerebrospinal Fluid (CSF)
|
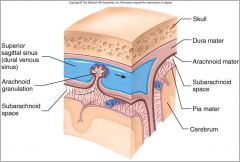
Ventricles = CSF-filled cavities in the brain and spinal cord (like ventricles in heart are filled with blood)
CSF Functions - bathes the brain and spinal cord & provides a protective cushion - CSF is produced by the ependymal cells in the choroid plexuses. - CSF drains through arachnoid granulations into the dural venous sinus. CSF Production - Produced by ependymal cells lining ventricles - Flows from lateral ventricles to 4th ventricle where enters spine central canal and subarachnoid space (covers all of brain) CSF Drainage into blood - Passes through arachnoid granulations - Drains into superior sagittal sinus What is hydrocephalus? What causes it? |
|
|
Sensory Receptors
|
Sensory Receptors in PNS send signals (afferent) to CNS.
Specialized neurons or epithelial cells in periphery that detect stimuli (undergo the transduction) Sensory transduction = regardless the type of stimulus, energy converted to electrochemical energy (potentials and action potentials) by transduction Must have ions moving no matter what the stimuli may be |
|
|
How do sensory receptors encode the intensity of a stimulus? The duration?
|
the more intense a signal the more quickly action potentials follow one after another, back to back signaling.
Duration is how long the action potentials keep flowing. |
|
|
Dorsal Column Pathway
|

One of the pathways for somatosensation. It is an Ascending tract.
Functions= Proprioception, Touch, Deep Pressure, Vibration Cell body is located just outside the spinal cord. There are groups of cells, ganglia, just outside of the CNS. They repeat over and over on dorsal side of the spine, in the White Matter. This is where the somatosensory neurons are located, they ultimately join with the spine. Sensory comes into the dorsal roots of the spine, but it doesn't synapse so it keeps moving all the way up the spine (ascending tract). When it ascends it stays on the same side of the spine, so if right stays on right side (this is called ipsilateral). Travels to Medulla and there it synapses, there the action potential stops and nerotransmitter releases. They get excited and move on. So once it gets to the Medulla it crosses to the contralateral side (it decussates). And then the action potentials go up, up, up (through pons, midbrain) and stops at the Thalamus. The Thalmus sends it on to the cerebral cortex (on the opposite side of where it was sent from). It synapses to cortical cells. THIS is where Perception occurs. Left side of body is perceived on right side of cerebrum. |
|
|
What side of the brain perceives somatosensory information from the left side of the body?
|
It would be perceived on the right side of the cerebrum (cortex).
|
|
|
What are the major sensory pathways to the brain? (different)?
|
Spinothalamic =
- goes into spine and then up to the thalamus, to the cerebrum cortex - pain and temperature information Spinocerebellar = - goes into the spine and then up to the thalamus, to the cerebellum - proprioception (information about how your body is positioned in space) information Dorsal Column = - goes into the spine and then up to the thalamus, to the cerebrum cortex - touch, vibration information |
|
|
Be able to describe the deficits in sensation that would occur with a hemisection of the spinal cord.
|
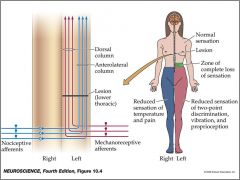
|
|
|
Where in the brain do sensory pathways ultimately terminate? What major functions are associated with these points of termination?
|

Brainstem = particularly sensory information from inside the body (Ex: blood pressure, autonomic functions)
Hypothalamus = homeostasis (Ex: body temperature) Cerebral Cortex = Perception of senses, Recognition of a sense |
|
|
What are the functional distinctions between primary sensory areas and association areas?
|
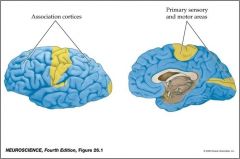
Primary Sensory Areas = Perception, devoted to only one sense at a time (visual, auditory, somatosensory, motor)
Association Sensory Areas = recognition, comprehension, analyzing more than one sense at once If you had damage to a primary area, you wouldn't be able to feel that sense. |
|
|
How is the somatosensory cortex organized with regard to how it represents the body? Is more somatosensory cortex devoted to certain areas of the surface of the body, why?
|
Somatosensory cortex =
Huge chunk devoted to: Fingers Mouth & Lips |
|
|
Somatic Nervous System
|
All about Muscle control
Upper Motor Neurons (in the brain) contact Lower Motor Neurons (in the spine and brainstem) and then those contact muscles Upper Motor Neurons are found in the (cerebral) motor cortex & brainstem Cerebellum = modulates the activity of the UMN Basal Ganglia = (found DEEP in cerebrum) modulates UMN |
|
|
The Motor Cortex
|

Motor Cortex is in charge of muscle movement
Prefrontal area = anterior frontal lobe; motivation (to do or start a motor activity), foresight and emotion (well-developed in primates) Premotor area = most of frontal cortex; planning motor activity Primary motor cortex = posterior frontal lobe anterior to central sulcus; initiation voluntary movements, upper motor neurons (UMNs) corresponding to specific body areas |
|
|
Lateral Corticospinal Pathway
|

Overall Purpose = muscle tone and skilled movements, especially of hands
Primary Motor Cortex (has motor neurons that initiate function) projects down through cerebrum enters brainstem passes through brainstem and enters medulla. In the medullary pyramids the neuron decussates (crosses), and enters the ventral horn of the spine. It indirectly contacts the LMN in ventral horn of spine and goes to periphery and enervates and branches to many muscle fibers (motor units). |
|
|
The left primary motor cortex controls fine motor functions on which side of the body?
|
The right side of the body.
|
|
|
Contrast the direct and indirect motor pathways in terms of where they originate and their respective, major function.
|
Direct
UMN originate in cortex voluntary functions (hands) Indirect UMN originate in brainstem involuntary functions (posture) |
|
|
Organization of LMN
|
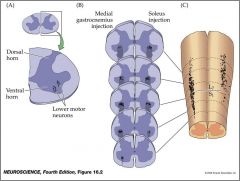
In the spine, in the ventral horns
Motor pool = all the motor units innervating a given muscle Motor Pools are distributed in columns (of the spine) |
|
|
From which brain areas do the basal nuclei receive input? Where is the ultimate target of the basal nuclei? What is the function of this motor subsystem?
|

Controls UMNs
Found DEEP in the Cerebrum The 2 primary nuclei are the corpus striatum , deep in the cerebrum, and the substantia nigra in the midbrain. The basal nuclei are the integral links in complex stimulatory and inhibitory feedback loops between the cerebral cortex, the basal nuclei, the thalamus and the frontal cortex. The basal nuclei = important for initiating movements and inhibiting unwanted movements |
|
|
What is the cause of Parkinson’s disease? How does this affect motor function?
|
Parkinson’s disease is a hypokinetic (lack of motion) disorder of the basal nuclei
Pathophysiology = - Progressive degeneration of dopamine-releasing neurons in the substantia nigra (dark substance), they die off slowly Signs and symptoms = - Muscular rigidity - Resting tremor - Shuffling gait - General lack of movement - have trouble starting a movement, and once begun have trouble stopping that movement Therapies = - L-dopa (dopamine precursor) and other drugs - Electrical pulse generator - Stem cells |
|
|
What are the major functions of the cerebellum? Describe how the comparator function of the cerebellum works.
|
Cerebellum = Muscle coordination (atoxia = lack of coordination), Maintenance of balance and muscle tone, coordinating fine movements, modulating ongoing movement (comparator), motor learning; and sensory discrimination
Receives information on proprioception (important for motor learning) Cerebellum modifies UMN (motor cortex activity) = so that movements may be smooth |
|
|
sympathetic vs. parasympathetic
|
sympathet = fight or flight, prepares the body for physical activity
Parasympathetic = stimulates involuntary activities of the body at rest. |
|
|
somatic vs. autonomic
|
somatic = voluntary
autonomic = involuntary |
|
|
Describe the lateralization of language function.
|
Language tends to be lateralized in the left cerebral cortex
|
|
|
Describe the areas of the brain involved in language. What are the respective functions of these areas?
|
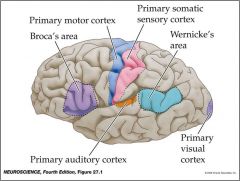
sensory speech area (comprehension) = wernicke area (parietal lobe)
motor speech area = broca area (fronal lobe) |
|
|
What is the difference between Broca’s and Wernicke’s aphasia? Which would you rather have and why?
|
Inability to produce or comprehend language
Caused by strokes, tumors or trauma Tissues die. Broca’s = inability to speek Wernicke’s = inability to understand |
|
|
Why do humans need sleep? Is sleep necessary for survival? Explain.
|
Energy expenditure =
restore brain glycogen; conserve heat loss at night Predation avoidance = relies on vision Memory consolidation = increased strength of synaptic connections; replenish neurotransmitters Deeper stages are necessary; REM sleep is not The longest documented period of voluntary sleeplessness in humans is about 19 days. |
|
|
Describe EEG waves during wakefulness, sleep stages I – IV and REM sleep.
|
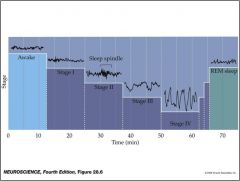
EEG waves patterns = activity of millions of cortical neurons in the cerebrum
Stage I - IV = each cortical waves gets larger and larger due to synchronicity. Stage IV is the deep sleep that is what is actually needed for survival REM is similar to wakeful hours in the cortical waves. REM is dream state that repeats. |
|
|
Hippocampus?
Describe the case of patient H.M. and what is demonstrated with regard to the hippocampus and its role in memory. |
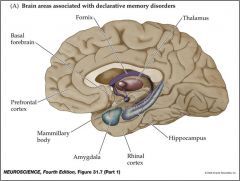
Hippocampus = Located in medial temporal lobe; Site of memory consolidation
H.M. = Following his surgery to treat major seizures, H.M. developed anterograde amnesia, or an inability to form new memories. They removed the hippocampi from the brain, this is what caused his inability to form new memories. |
|
|
Where are long-term memories stored in the brain?
|
Increased strength of synapses
Stored in the cerebral cortex Different categories of memories in different cortical areas |
|
|
Name 2 brain structures involved in emotional processing. What are their respective roles?
|
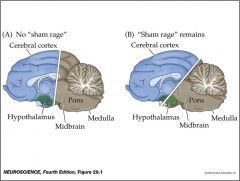
Subjective feelings and associated physiological states
Visceral motor activity: heart rate, cutaneous blood flow, piloerection and sweating Somatic motor changes: facial muscles Hypothalamus = modulates expression of emotion, controls visceral motor activity |
|
|
How is motor activity related to emotional states?
|
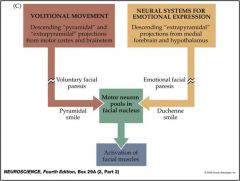
fake facial smiles = primary motor cortex
real smile = frontal cortex, not entirely voluntary |
|
|
Amygdala
|
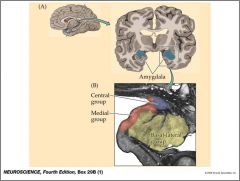
Temporal Lobe, medial. = Important role in fear and aggression (also involved in visceral, like pains in tummy when scared)
When the amygdala was transected in monkeys on one side, they would lose normal fearful and aggressive responses to stimuli when the stimulus was presented in the visual field on the same side. |
|
|
How do anti-depressant drugs improve mood?
|
Improve neurotransmitter synapses
|
|
|
What are sensory receptors?
|
Can be specialized epithelial cells or neurons
Receptors = usually proteins Sensory receptors = refers to the WHOLE cell that detects the stimulus What is the common way they transduce and send signals to the CNS? = Involves ions moving through ion channels; It has to fire an action potential This is transduction = change from stimulus energy to electrochemical energy Mechanoreceptors = skin, mechanical things like pressure Chemoreceptors = detect chemicals, odors and taste Photoreceptors = light and vision Thermoreceptors = heat and cold Nocicepors = pain |
|
|
How is the anatomy and location of the various touch receptors related to their respective functions?
|
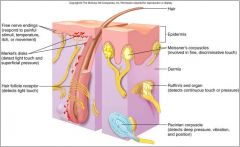
Receptors found in dermal layer
Some have capsular structures on end, that helps for their specific detection purpose (vibrations) Free nerve endings = temperature or pain detections |
|
|
How is the anatomy and location of the various touch receptors related to their respective functions?
|
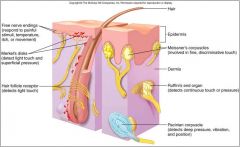
Receptors found in dermal layer
Some have capsular structures on end, that helps for their specific detection purpose (vibrations) Free nerve endings = temperature or pain detections |
|
|
Describe the nerve endings of cold and warm receptors. How do these sensory receptors detect temperature? How is temperature perceived outside the sensitivity ranges of these receptors?
|
Free nerve endings express temperature-sensitive ion channels
Cold receptors respond to cool temperatures but not below 54º F Warm receptors respond to warm temperatures but not above 117º F Must have express ion channels that are sensitive to temperature When it gets cold, those receptors release ion channels that are receptive to cold Same with warm If it’s above 117 or below 54, then it reads it as pain |
|
|
Describe the nerve endings of nociceptors. What causes painful stimuli?
|
Free nerve endings; respond to noxious stimuli
Nociceptor = perception of a noxious substance, something that could potentially cause damage Pain = affective, or emotional issues in brain (negative thoughts, feelings) Nociceptors = free nerve endings Release substances after stimuli, inflammatory substances that bind to receptors on nerve endings, this causes ions flowing through ion channels Some cause dialated blood vessels, this causes redness and warmth (a leakage) This also causes swelling, cause of leakage of blood vessels Local or topical Anesthetic to stop pain can Block voltage gated Sodium-Potassium channels (If its local that’s fine) |
|
|
Hyperalgesia
|
is an increased sensitivity to pain, which may be caused by damage to nociceptors or peripheral nerves.
|
|
|
How do anesthetics work? Describe the gate control theory?
|
Local or topical Anesthetic to stop pain can Block voltage gated Sodium-Potassium channels (If its local that’s fine)
gate control theory = action potentials "close the gate" and inhibit action potentials carried to the brain by the lateral spinothalamic tract. The gate control theory may explain reduced pain intensity when focusing on something else. |
|
|
Hyperalgesia
|
is an increased sensitivity to pain, which may be caused by damage to nociceptors or peripheral nerves.
|
|
|
Hyperalgesia
|
is an increased sensitivity to pain, which may be caused by damage to nociceptors or peripheral nerves.
|
|
|
How do anesthetics work? Describe the gate control theory?
|
Local or topical Anesthetic to stop pain can Block voltage gated Sodium-Potassium channels (If its local that’s fine)
gate control theory = action potentials "close the gate" and inhibit action potentials carried to the brain by the lateral spinothalamic tract. The gate control theory may explain reduced pain intensity when focusing on something else. |
|
|
How do anesthetics work? Describe the gate control theory?
|
Local or topical Anesthetic to stop pain can Block voltage gated Sodium-Potassium channels (If its local that’s fine)
gate control theory = action potentials "close the gate" and inhibit action potentials carried to the brain by the lateral spinothalamic tract. The gate control theory may explain reduced pain intensity when focusing on something else. |
|
|
Referral pain
|
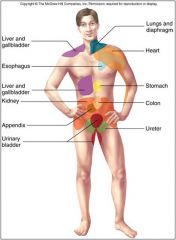
Referral Pain = feeling of pain on the surface, when it is really a problem for organs underneath
Ischemia = decreased blood flow How does this work? Common convergence points at neruons, Nerves are shared……. |
|
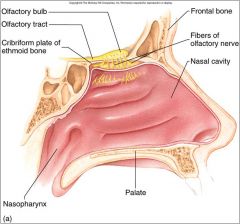
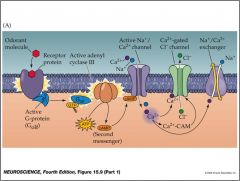
Where are olfactory neurons located? Describe how odorants are trapped and an olfactory signal is transduced.
|
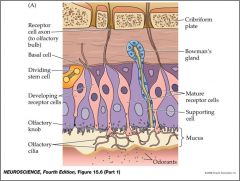
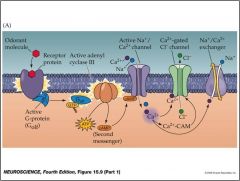
Olfaction = smell
Chemicals have to bind receptors, triggers ion channels to flow, and action potentials Olfactory Neurons (olfactory nerves) = found inside mucous, stimuli binds to neuron receptors which creates change in potential Cribriform plate (has tons of holes so all the axons can go through the ethmoid) Mucous = helps to trap oderants Pink = olfactory neurons Nerve endings are called olfactory cilia = these detect oderants and bind them Nerve cells are regenerative because they die from exposure to environment (in general nerves do NOT grow back or regenerate) Stem cells help it regenerate the tissue Axons form a synapse with a second order neruon Specialized cilia project into nasal cavity Olfactory receptors expressed on cilia Easily damaged; regenerate from stem cells Send axons to olfactory bulb |
|
|
Why are humans able to perceive as many as 10,000 smells while they only express around 400 different types of odorant receptor?
|
About 400 different olfactory receptors in humans
Each can bind more than one odorant Humans can perceive around 10,000 different smells Low activation threshold; quickly adapt Only about 400 receptor proteins Combination of receptor activation We can detect around 10,000 kinds of smells These adapt quickly |
|
|
Describe the neural circuitry by which olfactory neurons synapse with mitral cells in the olfactory bulb. To what part of the brain do mitral cells relay olfactory information? Does this information pass through the thalamus?
|
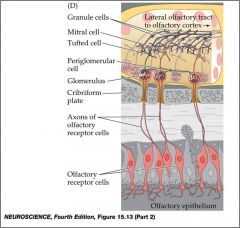
Olfactory neurons Send axons through cribriform plate, ultimately synapse with second order neuron (mitral cells)
mitral = cells in olfactory bulb, send axons out to the olfactory cortex Glomerulus = looks like sphere found in olfactory bulb, distinct smells contact distinct glomerulus Projections from olfactory neurons converge on glomeruli in olfactory bulb As many as 25,000 axons converge in 1 glomerulus; all from neurons with same olfactory receptor type! Each glomerulus contains dendrites of about 25 mitral cells which project to olfactory cortex |
|
|
Olfactory Cortex
|
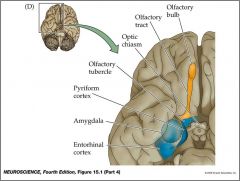
Olfaction: only major sense NOT relayed through thalamus
Olfactory cortex: more primitive cortex (fewer cell layers) in temporal and frontal lobe Emotional responses to smells; note proximity to amygdala Blue is temperal lobe Olfactory lobe is yellow This is the only major sense NOT relayed through thalamus Amygdala = close to smell which processes emotion. |
|
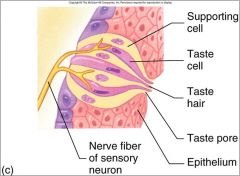
Where are taste cells located? How do they trap and transduce taste stimuli?
|
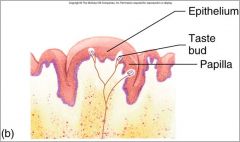
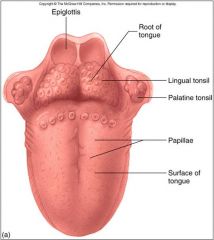
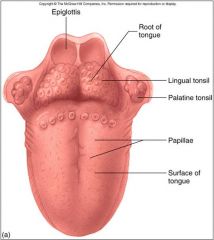
Taste bud cells are located within the papillae.
Taste buds also found in other parts of mouth and throat Each contains supporting cells and about 40 taste cells Taste hairs trap tastes |
|
|
What are the 5 basic tastes? How are many more tastes perceived by humans?
|
salt, sour, bitter, sweet and umami
Super tasting = being able to taste certain bitter things that most people can not, its thought they have more papillae A lot of flavor experience is the smell at the same time, smell is critically important to experience of flavor As well as combination |
|
|
Where is taste sensation perceived in the cerebral cortex? Is taste information relayed from the thalamus?
|
Taste information (on receptors) relayed to thalamus via cranial nerves (arise out of brain stem or brain), up the brain stem and then ultimately to the thalamus which projects to the parietal cortex (somatosensation, and taste)
Taste information relayed to thalamus via 3 different cranial nerves; thalamic cells project to parietal cortex |
|
|
Structures of the eye?
Glaucoma? |
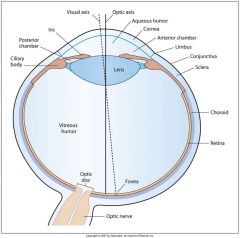
Drainage through venous ring blocked; pressure on retina can cause blindness
Cornea = transparent Sclera = whites of eye Choroid = pigmented, prevents light scatter Cilliary body & iris (colors for eye) = a lot of what composes this is smooth muscle Retina = neural tissue (nerve cells), this is where visual transduction occurs Lens = also transparent Aqueous humor = in the chambers, provides pressure to keep cornea inflated. This is produced by cilliary body, drains through venous system. If drainage is blocked its called glaucoma, increases pressure and may lead to blindness from pressure on retina; nutrients Vitreous humor = more jelly like, also transparent Multiple layers, or tunics: fibrous, vascular and neural |
|
|
Pupil Control? Pupillary light reflex?
|
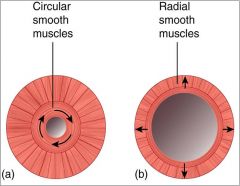
This is the Iris
Smooth muscle = involuntary Pupil = a hole through which light passes, used to adjust to different levels of light Circular muscle = used to constrict pupil radial muscle = used to dilate pupil Light signals go to midbrain and tells the muscles via parasympathetic response whether to dilate or constrict (damage to midbrain can be seen if pupil does not change in light) Circular and radial smooth muscles in the iris Pupillary light reflex: controlled by parasympathetic fibers |
|
|
How are images focused on the retina? Which eye structures participate in light refraction? How does accommodation work?
|
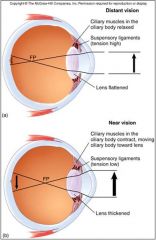
Ciliary body = involuntary muscle
Attached by suspensory ligaments Image light bends or refracts (from air medium to solid medium), moves to acqueous humor bends some more, hits cornea and bends even more, image is inverted on retina (cortex is in charge of making everything right side up) Lens is the fine tuning of refraction. If we’re looking in the distance the lens becomes flattened, shorter distance lens rounds. This is called accommodation Near vision causes cilliary muscles to contract, reduces tension in ligaments, this causes lens to round up (these signals were sent to midbrain, motor response follows). This causes the rays to refract even more (trying to make the blurry clearer) Eyeball can change shape over time (near sighted and far sighted) making the different place the light hits the retina is actually out of focus Light refracted by eye structures; lens “fine tunes” Accommodation: blurred retinal images cause lens to “round up” parasympathetic fibers cause ciliary body to contract for near vision Images on retina are inverted |
|
|
What is the role of pigmented cells?
|
Pigmented cells in the eye prevent light scatter.
|
|
|
Describe the arrangement of neural cell layers in the retina. How do visual signals move through and out of the retina?
|
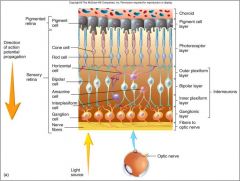
Rods and Cones
- detect light - in back of cell layers VISUAL SIGNAL STRUCTURE - Signal travels backward where Rods and cones detect light - then signals come forward from rods and cones and leaves through axons of the ganglion cells (output cells basically) - ganglion axons make up what is known as the optic nerve - so signals leave the optic nerve. - The connections with the different cells do not actually involve action potentials, their just changes in potentials (because it’s a short distance, rather than long distance which is what need axons and action potentials use); chemical synapses |
|
|
Compare the photo-receptors; rods and cones.
|

Rods:
Numerous discs (full of rhodopsin) High sensitivity Night vision (Do not function in bright light) Numerous in Peripheral retina Cones: Membrane enfoldings Low sensitivity High acuity Numerous in fovea (FULL, very few Rods) Day vision Color vision |
|
|
Briefly describe how rhodopsin responds to light. Why does it take a moment for one’s vision to adjust to dark conditions?
|
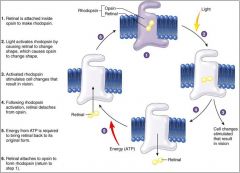
Opsin protein receptor and retinal ligand
When light hits a rod cell, the retinal changes shape, making opsin detach from retinal - the change in rhodopsin shape triggers vision from the rod cells so that you can see. But it takes a moment. Vitamin A required for retinal recycling in rod cells - lack of Vitamin A may cause night blindness, rods use retinal for night vision (without, rods die away) |
|
|
Phototransduction?
How are visual signals transmitted through the retina? |
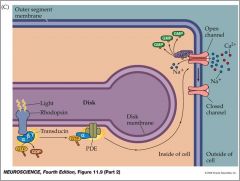
Light causes hyperpolarization of photoreceptors and less neurotransmitter release
Dark causes depolarization and more neurotransmitter release |
|
|
Describe the neural pathways by visual information travels to the primary visual cortex.
Which side of the brain perceives visual information from the right visual field? Why does this occur? |
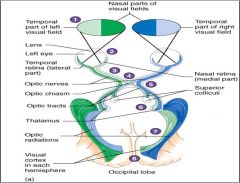
Optic nerve - formed by the final output cells, ganglion cells (blind spot where nerves come together is referred to as optic disc)
Optic chiasm - nerves come from nasal retina cross, called chiasm Nerves from Temporal Retina do NOT cross Axons terminate in the Thalamus hypothalamus receive information about the light that influence sleep patterns (produced by melatonin) Superior Colliculus in Brainstem controls pupillary light reflex, bright flash reflex (motor neuron controls) Occipital Lobe - Primary visual cortex Right occipital cortex would see the left, visa versa Left side of both retinas, they see the right visual field Right side of both retinas, see the left visual field |
|
|
Describe the role of the middle ear structures in the transmission of sound to the inner ear.
|
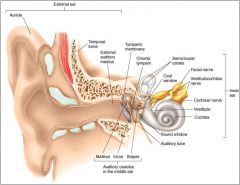
Outer ear: auricle (elastic cartilage), auditory meatus (canal)
Functions: Focus sound waves into ear Middle ear: tympanic membrane and auditory ossicles (bones) Functions: Connected through lever system, amplifies energy of sound waves, converts air medium to fluid Inner ear: cochlea (oval window), semicircular canals and vestibule Functions: maze type structure, fluid filled, auditory transduction occurs here |
|
Describe auditory transduction in the inner ear.
What is the role of the basilar membrane and the auditory hair cells? How do these events ultimately lead to the transduction of action potentials to the CNS? |
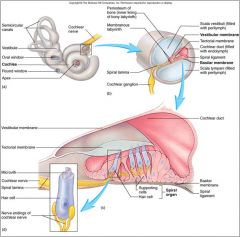
Chochlea = Spiral shaped
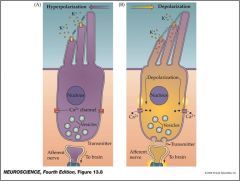
- transduces sound waves - 3 fluid-filled ducts: Perilymph fluid: ECF-like (found outside duct), Endolymph fluid: ICF-like (found inside duct (Organ of corti:) Rows of auditory hair cells (specialized epithelial cells) embedded in Basilar membrane and touch with their tops the Tectorial membrane Sounds cause basilar membrane to vibrate Bends stereocilia on hair cells back and forth - this causes ion channels to open and close (mechanically gated) Much stiffer tectorial membrane moves less HAIR CELLS Bending toward largest stereocilium opens mechanically-gated K+ channels and causes depolarization Bending away from largest stereocilium closes mechanically-gated K+ channels and causes hyperpolarization Intermittent release of neurotransmitter |
|
|
Describe 2 mechanisms by which sound frequency, or pitch, is encoded in the inner ear.
How is sound intensity, or loudness, encoded? |
1. Frequency can be encoded by the firing rate of auditory nerves, up to a point! (everything moves to the same frequency) - if too high then the cells just remain depolarized
2. Different points along the basilar membrane resonate with specific frequencies. (different pitches vibrate different parts better than others) - this helps perceive different pitches, some at higher frequencies |
|
|
Describe the auditory neural pathway to the brain.
Why do central unilateral lesions often NOT lead to deafness? |

1. Vestibulocochlear nerve
2. Cochlear nuclei (medulla) 3. Inferior colliculus (midbrain) - responsible for auditory refelxes 4. Thalamus 5. Primary auditory cortex (temporal lobe) As it ascends up the brain stem, nerve signals deccasate to opposite side AND stay on same side. So no matter which side is damaged (as long as its above the mid-pons) you will not be deaf. |
|

What types of head movements are detected by the semicircular canals and vestibular organs, respectively? How does the body use these types of sensory information?
|
Utricle and saccule detect pitch and roll of the head
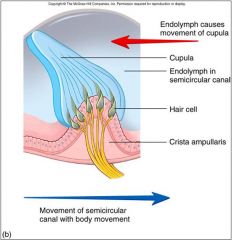
Macula: patches of epithelium with vestibular hair cells Stereocilia embedded in gelatinous matrix containing otoliths HEAD JERKING REFLEX - Macula displaced forward - Stereocilia bend - Depolarization SEMICIRCULAR CANALS - 3 in each ear; oriented at along perpendicular axes - Detect head turns - Crista ampularis epithelium containing vestibular hair cells - Stereocilia embedded in gelatinous cupula - push endolymph and causes ion channel flow - Displaces cupula which bends stereocilia Nystagmus Visual Reflex May occur |
|
|
Vestibular Pathways?
|
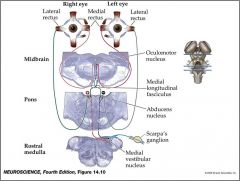
Control of visual reflexes
1. Vestibulocochlear nerve 2. Vestibular nuclei (medulla) 3. Oculomotor nucleus (midbrain) 4. Rectus muscles of the eyes |
|
|
What is the overall purpose of the endocrine system?
What are some examples of specific endocrine functions? |
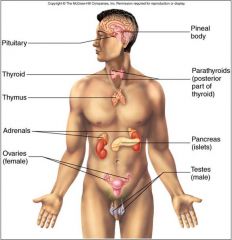
Overall purpose of the endocrine system is hormones that are vital to maintaining homeostasis
- Growth and metabolism - Blood glucose - Body fluid ions - Water balance - Cardiovascular functions - Immunity - Reproduction Glands are located throughout the body(Brain, neck, abdomen, ect.) Intercellular communication is often done by chemicals. See table 10.1 for examples Hormones in general are released from a gland, enter circulation and act in specific parts of the body |
|
|
Quick Quiz over Chemical Signals in Endocrine System
|

|
|
|
How are hormones able to target specific tissues in the body?
|
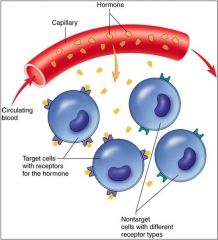
Water vs. lipid-soluble
Water sol.: proteins, peptides and amino acid derivatives Lipid-sol.: Steroid hormones and thyroid hormones Intercellular communication is often done by chemicals. See table 10.1 for examples Hormones in general are released from a gland, enter circulation and act in specific parts of the body Tissues must have certain hormone receptors for hormones to act upon a cell. Drugs work in a similar fashion-need receptors |
|
|
What are the 2 chemical classes of hormones? Provide examples for each
How do these hormone classes differ in the types of receptors they act upon?. |

There are two big classes of hormones
Hydrophillic hormones(generally peptides-example:insulin) Receptors are generally on the membrane Lipophillic- Steroid hormones such as sex Receptors are generally inside a cell Water vs. lipid-soluble Water sol.: proteins, peptides and amino acid derivatives Lipid-sol.: Steroid hormones and thyroid hormones |