Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
168 Cards in this Set
- Front
- Back
|
What are the deficits in dementia? |
Decreased cognitive ability, memory, or function, with intact consciousness
|
|
|
What are the top two most common cause of dementia in the elderly?
|
1. Alzheimer Disease
2. Multi-infarct |
|
|
What can increase your risk of getting Alzheimer Disease?
|
- Down syndrome (Amyloid Precursor Protein - APP is on chr 21)
- Familial forms (10% of cases) |
|
|
What are the types of familial Alzheimer Disease? What is affected?
|
Early onset:
- Amyloid Precursor Protein (APP) - chr 21 - Presenilin-1 - chr 14 - Presenilin-2 - chr 1 Late onset: - ApoE4 - chr 19 |
|
|
What can protect against Alzheimer Disease?
|
ApoE2 (chr 19)
|
|
|
What are the gross changes in Alzheimer Disease?
|
- Widespread cortical atrophy
- Narrowing of gyri - Widening of sulci |
|
|
What hormone changes occur in Alzheimer Disease?
|
↓ ACh
|
|
|
What are the histologic change associated with Alzheimer Disease?
|
- Senile Plaques
- Neurofibrillary tangles |
|
|
What are the contents and effect of a senile plaque?
|
- Extracellular β-amyloid core
- May cause amyloid angiopathy → intracranial hemorrhage - Aβ (Amyloid-β) synthesized by cleaving Amyloid Precursor Protein (APP) - Associated with Alzheimer Disease |
|
|
What are the contents and effect of a neurofibrillary tangle?
|
- Intracellular hyperphosphorylated tau protein = insoluble cytoskeletal elements
- Tangles correlate with degree of dementia - Associated with Alzheimer Disease |
|
|
What type of dementia is associated with aphasia, parkinsonian aspects, and a change in personality?
|
Pick Disease (Frontotemporal Dementia)
|
|
|
What are the gross changes in Pick Disease (Frontotemporal Dementia)?
|
- Frontotemporal atrophy
- Spares parietal lobe and posterior 2/3 of superior temporal gyrus |
|
|
What is the histologic finding in Pick Disease (Frontotemporal Dementia)?
|
Pick bodies = spherical tau protein aggregates
|
|
|
What type of dementia is associated with visual hallucinations followed by parkinsonian features?
|
Lewy Body Dementia
|
|
|
What defect is associated with Lewy Body Dementia?
|
α-Synuclein defect
|
|
|
What type of dementia is rapidly progressive (weeks to months) and causes myoclonus ("startle myoclonus")?
|
Creutzfeldt-Jakob disease
|
|
|
What is the cause and effect of Creutzfeldt-Jakob disease?
|
- Prions (PrP-c → PrP-sc sheet [β-pleated sheet resistant to proteases])
- Causes a spongiform cortex - Dementia is rapidly progressive (weeks to months) and associated with myoclonus |
|
|
What other diseases can cause dementia?
|
- Multi-infarct (2nd most common cause of dementia in elderly)
- Syphilis - HIV - Vitamins B1, B3, or B12 deficiency - Wilson disease - NPH |
|
|
What vitamin deficiencies can cause dementia?
|
Vitamins B1, B3, or B12
|
|
|
What causes Multiple Sclerosis?
|
Auto-immune inflammation and demyelination of the CNS (brain and spinal cord)
|
|
|
What are the common symptoms in a patient with Multiple Sclerosis?
|
- Optic neuritis (sudden loss of vision)
- Internuclear Ophthalmoplegia - Hemiparesis - Hemisensory symptoms - Bladder / bowel incontinence |
|
|
Who is most commonly affected by Multiple Sclerosis? Clinical course?
|
- Most often women in 20s and 30s
- More common in whites - Relapsing and remitting course |
|
|
What is the classic triad of symptoms in Multiple Sclerosis?
|
SIN:
- Scanning speech - Intention tremor (also Incontinence and Internuclear ophthalmoplegia) - Nystagmus |
|
|
What are the lab findings associated with Multiple Sclerosis?
|
Increased protein (IgG) in CSF
*Oligoclonal bands are diagnostic |
|
|
What is the best way to diagnose Multiple Sclerosis? What findings do you look for?
|
MRI is the gold standard
- Periventricular plaques (areas of oligodendrocyte loss and reactive gliosis) with destruction of axons - Multiple white matter lesions separated in space and time |
|
|
How do you treat Multiple Sclerosis?
|
- β-interferon
- Immunosuppression - Natalizumab - Symptomatic treatment for neurogenic bladder (catheter, muscarinic antagonists) - Symptomatic treatment for spasticity (baclofen, GABA receptor agonist) - Symptomatic treatment for pain (opioids) |
|
|
What drugs are given to patients with Multiple Sclerosis regardless of symptoms?
|
- β-interferon
- Immunosuppression - Natalizumab |
|
|
What drugs are given to patients with Multiple Sclerosis with neurogenic bladder problems?
|
- Catheterization
- Muscarinic antagonists |
|
|
What drugs are given to patients with Multiple Sclerosis with spasticity problems?
|
- Baclofen
- GABA receptor agonist |
|
|
What drugs are given to patients with Multiple Sclerosis with pain problems?
|
Opioids
|
|
|
What is the most common variant of Guillain-Barré Syndrome?
|
Acute Inflammatory Demyelinating Polyradiculopathy
|
|
|
What causes Acute Inflammatory Demyelinating Polyradiculopathy?
|
Auto-immune condition that destroys Schwann cells → inflammation and demyelination of peripheral nerves and motor fibers
|
|
|
What are the consequences of the demyelination of the peripheral nerves and motor fibers in Acute Inflammatory Demyelinating Polyradiculopathy?
|
- Symmetric ascending muscle weakness and paralysis beginning in lower extremities
- Facial paralysis in 50% of cases - Autonomic function may be severely affected (eg, cardiac irregularities, hypertension, or hypotension) - Almost all survive, majority recover after weeks to months |
|
|
What are the lab findings associated with Acute Inflammatory Demyelinating Polyradiculopathy?
|
- ↑ CSF protein
- Normal cell count (albuminocytologic dissociation) - ↑ Protein → Papilledema |
|
|
What is Acute Inflammatory Demyelinating Polyradiculopathy associated with / cause?
|
Infections:
- Campylobacter jejuni - CMV Leads to auto-immune attack of peripheral myelin due to molecular mimicry, inoculations, and stress, but no definitive link to pathogens |
|
|
How do you treat a patient with Acute Inflammatory Demyelinating Polyradiculopathy?
|
- Respiratory support is critical until recovery
- Additional: plasmapheresis, IV immune globulins |
|
|
What disease is associated with AIDS patients and destroys oligodendrocytes leading to demyelination of CNS? Cause?
|
Progressive Multifocal Leukoencephalopathy
- Associated with reactivation of latent JC virus infection |
|
|
How common is Progressive Multifocal Leukoencephalopathy in AIDS patients?
|
2-4%
|
|
|
What is the prognosis for Progressive Multifocal Leukoencephalopathy?
|
- Rapidly progressive
- Usually fatal |
|
|
What increases the risk of Progressive Multifocal Leukoencephalopathy?
|
- ↑ risk with Natalizumab
- More common in AIDS patients |
|
|
What disease causes multi-focal perivenular inflammation and demyelination after infection or vaccinations?
|
Acute Disseminated Encephalomyelitis
|
|
|
What is the cause of Acute Disseminated Encephalomyelitis?
|
- Occurs after infection: commonly measles or VZV
- Or occurs after vaccine: rabies or smallpox |
|
|
What are the consequences of Acute Disseminated Encephalomyelitis?
|
Multifocal perivenular inflammation and demyelination
|
|
|
What disease is due to an arylsulfatase A deficiency? What builds up?
|
Metachromatic Leukodystrophy
- Build up of sulfatides |
|
|
What causes build up of sulfatides in Metachromatic Leukodystrophy? What does this lead to?
|
- Autosomal recessive deficiency of Arylsulfatase A
- Leads to impaired production of myelin sheath |
|
|
What are the findings of a patient with Arylsulfatase A deficiency (Metachromatic Leukodystrophy)?
|
- Build up of sulfatides → impaired production of myelin sheath
- Central and peripheral demyelination - Ataxia and dementia |
|
|
What disease is related to defective production of proteins involved in the structure and function of peripheral nerves or myelin sheath?
|
Charcot-Marie-Tooth disease
|
|
|
What is wrong in Charcot-Marie-Tooth disease?
|
Hereditary motor and sensory neuropathy (HMSN)
- Progressive hereditary disorder related to defective production of proteins involved in structure and function of peripheral nerves or myelin sheath - Typically autosomal dominant |
|
|
What is Charcot-Marie-Tooth disease associated with?
|
- Scoliosis
- Foot deformities (high or flat arches) |
|
|
What disease is associated with a deficiency of galactocerebrosidase? What builds up?
|
Krabbe Disease
- Build up of galactocerebroside and psychosine which destroy the myelin sheath |
|
|
What are the clinical findings caused by a deficiency of galactocerebrosidase (Krabbe Disease)?
|
- Peripheral neuropathy
- Developmental delay - Optic atrophy - Globoid cells |
|
|
What disease disrupts metabolism of very-long-chain fatty acids? Cause?
|
Adrenoleukodystrophy
- X-linked (typically affects males) |
|
|
What are the clinical findings caused by a disruption of very-long-chain fatty acid metabolism / Adrenoleukodystrophy?
|
- Excessive build-up in nervous system, adrenal gland, ante testes
- Progressive disease that can lead to long-term coma/death and adrenal gland crisis |
|
|
What is characterized by synchronized, high-frequency neuronal firing?
|
Seizures
|
|
|
How can you categorize seizures?
|
- Partial / focal vs generalized
- Simple vs complex |
|
|
What is the difference between partial and generalized seizures?
|
- Partial / focal: affects 1 area of brain (but can generalize)
- Generalized: diffuse |
|
|
What is the most common location for a partial seizure?
|
Medial temporal lobe
|
|
|
What typically precedes a partial seizure?
|
Seizure aura
|
|
|
What are the types of partial seizures? How do they differ?
|
- Simple Partial (consciousness intact): motor, sensory, autonomic, psychic
- Complex Partial (impaired consciousness) |
|
|
What are the types of generalized seizures?
|
- Absence (petit mal)
- Myoclonic - Tonic-clonic (grand mal) - Tonic - Atonic |
|
|
What is epilepsy?
|
Disorder of recurrent seizures (febrile seizures are not epilepsy)
|
|
|
What is status epilepticus?
|
Continuous seizure for >30 minutes or recurrent seizures without regaining consciousness between seizures for >30 minutes
(Medical emergency) |
|
|
What kind of seizure is characterized by a blank stare and causes no postictal confusion?
|
Absence (petit mal) - 3 Hz
|
|
|
What kind of seizure is characterized by quick, repetitive jerks?
|
Myoclonic (generalized seizure)
|
|
|
What kind of seizure is characterized by alternating stiffening and movement?
|
Tonic-Clonic (grand mal) generalized seizure
|
|
|
What kind of seizure is characterized by stiffening only?
|
Tonic generalized seizure
|
|
|
What kind of seizure is characterized by "dropping" (falling to floor) and is commonly mistaken for fainting?
|
Atonic generalized seizure
|
|
|
What are the common causes of seizures in a child?
|
- Genetic
- Infection (febrile) - Trauma - Congenital - Metabolic |
|
|
What are the common causes of seizures in an adult?
|
- Tumors
- Trauma - Stroke - Infection |
|
|
What are the common causes of seizures in the elderly?
|
- Stroke
- Tumor - Trauma - Metabolic - Infection |
|
|
What causes a headache?
|
Irritation of structures such as the dura, cranial nerves, or extracranial structures
|
|
|
What are the types of headaches?
|
- Cluster
- Tension - Migraine |
|
|
How do the types of headaches differ in terms of localization?
|
Unilateral:
- Cluster - Migraine Bilateral: - Tension |
|
|
How do the types of headaches differ in terms of duration?
|
- Cluster: 15 min - 3 hours (repetitive)
- Tension: >30 min (typically 4-6 hours); constant - Migraine: 4-72 hours |
|
|
Which type of headache causes repetitive brief headaches with excruciating periorbital pain with lacrimation and rhinorrhea?
|
Cluster Headache
|
|
|
Which type of headache may induce Horner syndrome?
|
Cluster Headache
|
|
|
Which type of headache causes a steady pain without photophobia, phonophobia, or auras?
|
Tension Headache
|
|
|
Which type of headache causes a pulsating pain with nausea, photophobia, and/or phonophobia?
|
Migraine
|
|
|
Which type of headache is due to irritation on CN V, meninges, or blood vessels? What is released?
|
Migraine
- Release of substance P, CGRP, and vasoactive peptides |
|
|
What do Cluster Headaches cause? Treatment?
|
- Repetitive brief headaches
- Excruciating periorbital pain with lacrimation and rhinorrhea - May induce Horner syndrome - More common in males Treatment: - Inhaled O2 - Sumatriptan |
|
|
What do Tension Headaches cause? Treatment?
|
- Steady pain
- No photophobia, phonophobia, or auras Treatment: - Analgesics, NSAIDs, or acetaminophen - Amitriptyline for chronic pain |
|
|
What do Migraine Headaches cause? Treatment?
|
- Pulsating pain with nausea, photophobia, or phonophobia
- May have "aura" - Due to irritation of CN V, meninges, or blood vessels (release of substance P, CGRP, and vasoactive peptides) Treatment: - Abortive therapies (eg, triptans or NSAIDs) - Prophylactic therapies (eg, propranolol, topiramate, CCBs, or amitriptyline |
|
|
What mnemonic helps you remember characteristics of migraine headaches?
|
POUND
- Pulsatile - One day duration - Unilateral - Nausea - Disabling |
|
|
What are the abortive therapies used for migraine?
|
- Triptans (eg, Sumatriptan)
- NSAIDs |
|
|
What are the prophylactic therapies used for migraine?
|
- Propranolol
- Topiramate - Calcium channel blockers - Amitriptyline |
|
|
What are some other causes of head pain (not a headache)?
|
- Subarachnoid hemorrhage ("worst headache of my life")
- Meningitis - Hydrocephalus - Neoplasia - Arteritis |
|
|
How can you distinguish a cluster headache from trigeminal neuralgia?
|
Depends on duration:
- Cluster headache: 15 min - 3 hours (repetitive) - Trigeminal neuralgia: repetitive shooting pain in distribution of CN V that lasts typically for <1 minute |
|
|
What is the sensation of spinning while actually stationary?
|
Vertigo
- Subtype of "dizziness" but distinct from "lightheadedness" |
|
|
What are the types of vertigo? Which is more common?
|
- Peripheral vertigo (more common)
- Central vertigo |
|
|
What causes peripheral vertigo?
|
Inner ear etiology (eg, semicircular canal debris, vestibular nerve infection, Ménière disease
|
|
|
What causes central vertigo?
|
Brain stem or cerebellar lesion (eg, stroke affecting vestibular nuclei or posterior fossa tumor)
|
|
|
What are the findings in peripheral vertigo?
|
Positional testing → delayed horizontal nystagmus
|
|
|
What are the findings in central vertigo?
|
- Directional change of nystagmus
- Skew deviation - Diplopia - Dysmetria - Postional testing → immediate nystagmus in any direction; may change directions - Focal neurological findings |
|
|
What disease is characterized by a port-wine stain of the face, seizures/epilepsy, intellectual disability, and early-onset glaucoma?
|
Sturge-Weber Syndrome
STURGE: - Sporadic port-wine Stain - Tram track Ca2+ (opposing gyri) - Unilateral - Retardation - Glaucoma and GNAQ gene - Epilepsy |
|
|
What is the cause of Sturge-Weber Syndrome?
|
- Congenital, non-inherited (somatic), developmental anomaly of neural crest derivatives (mesoderm/ectoderm)
- Due to activating mutation of GNAQ gene |
|

What causes the port-wine stain seen in Sturge-Weber Syndrome?
|

Small (capillary-sized) blood vessels have developmental anomalies → port-wine stain of face (non-neoplastic "birthmark" in CN V1/V2 distribution)
|
|
|
What causes the seizures/epilepsy seen in Sturge-Weber Syndrome?
|
Ipsilateral leptomeningeal angioma → seizures / epilepsy
|
|
|
What causes the glaucoma in Sturge-Weber Syndrome?
|
Episcleral hemangioma → ↑ intraocular pressure → early onset glaucoma
|
|
|
What genetic change causes Sturge-Weber Syndrome?
|
Activating mutation of GNAQ gene
|
|
|
What disease causes hamartomas in the CNS and skin, angiofribromas, mitral regurgitation, ash-leaf spots, cardiac rhabdomyoma, mental retardation, renal angiomyolipoma, seizures, and Shagreen patches?
|
Tuberous Sclerosis
|
|
|
What mnemonic helps you remember the characteristics of Turberous Sclerosis?
|
HAMARTOMAS:
- Hamartomas in CNS and skin - Angiofibromas (C) - Mitral regurgitation - Ash-leaf spots - Rhabdomyoma (cardiac) - Tuberous sclerosis - autosomal dOminant - Mental retardation - Angiomyolipoma (renal) (D) - Seizures and Shagreen patches |
|
|
What is there increased incidence of in Turberous Sclerosis?
|
- Subependymal astrocytomas
- Ungual fibromas |
|
|
Which disease is associated with café-au-lait spots, Lisch nodules, neurofibromas in the skin, optic gliomas, and pheochromocytomas?
|
Neurofibromatosis Type 1 (von Recklinghausen disease)
|
|
|
What is the cause of Neurofibromatosis Type 1 (von Recklinghausen disease)?
|
- Mutated NF1 tumor suppressor gene (neurofibromin - a negative regulator of Ras)
- On chromosome 17 |
|
|
What does a mutated NF1 tumor suppressor gene (chr 17) cause? Clinical symptoms?
|
Neurofibromatosis Type 1 (von Recklinghausen disease)
- Café-au-lait spots (E) - Lisch nodules (pigmented iris hamartomas) (F) - Neurofibromas in skin - Optic gliomas - Pheochromocytoma |
|
|
What are skin tumors of NF-1 derived from?
|
Neural crest cells
|
|
|
What disease is associated with cavernous hemangiomas in skin, mucosa, and organs; bilateral renal cell carcinomas; hemangioblastoma in retina, brain stem, cerebellum; and pheochromocytoma?
|
von Hippel-Lindau Disease
|
|
|
What is the cause of von Hippel-Lindau Disease?
|
- Autosomal dominant mutation in VHL tumor suppressor gene on chr 3
- Results in constitutive expression of HIF (transcription factor) and activation of angiogenic growth factors |
|
|
What disease is caused by the autosomal dominant mutation in the VHL tumor suppressor gene on chr 3? What does this mutation cause?
|
von Hippel-Lindau Disease
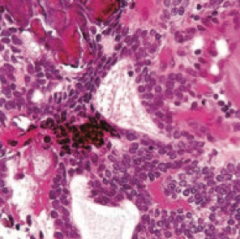
- Mutation results in constitutive expression of HIF (transcription factor) and activation of angiogenic growth factors - Cavernous hemangiomas in skin, mucosa, and organs - Bilateral renal cell carcinoma - Hemangioblastoma (high vascularity with hyperchromatic nuclei (G)) in retina, brainstem, and cerebellum (H) - Pheochromocytoma |
|
|
Where are there cavernous hemangiomas in von Hippel-Lindau Disease?
|
- Skin
- Mucosa - Organs |
|
|
Where are there hemangioblastomas in von Hippel-Lindau Disease?
|
- Retina
- Brainstem - Cerebellum |
|

What is wrong with this little girl? Associated with what disease?
|

Port-wine stain on face
- Caused by Sturge Weber Syndrome |
|
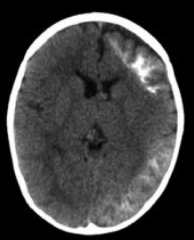
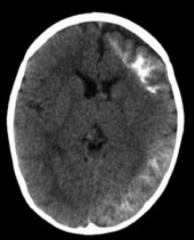
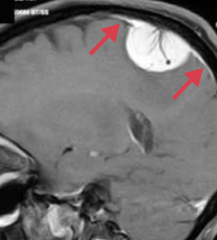
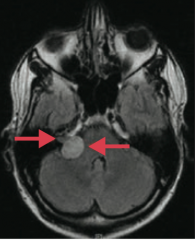
What is wrong with this brain? Associated with what disease?
|
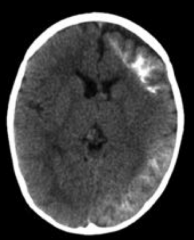
Ipsilateral leptomeningeal angioma → seizures / epilepsy
- Caused by Sturge Weber Syndrome |
|

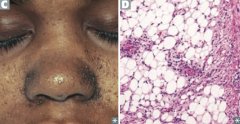
What is wrong with this little boy? Associated with what disease?
|

Angiofibromas of the face
- Caused by Tuberous Sclerosis |
|
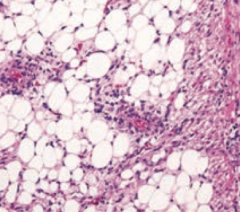
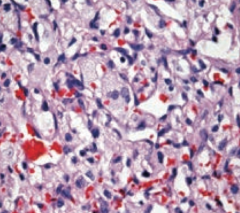
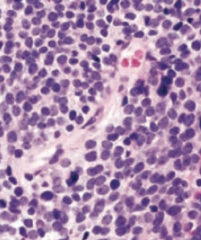
What aspect of Tuberous Sclerosis has this histology?
|
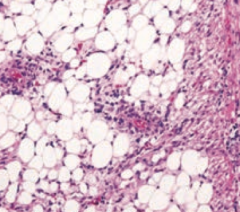
Renal Angiomyolipoma
|
|

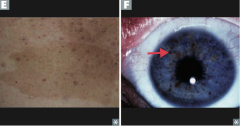
What is this skin finding? Associated with what disease?
|
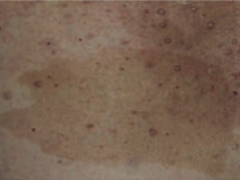
Café-au-lait spot
- Caused by Neurofibromatosis type I (von Recklinghausen disease) |
|
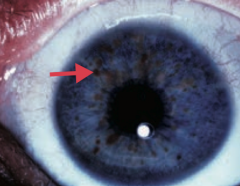
What is this eye finding? Associated with what disease?
|

Lisch nodule (pigmented iris hamartoma)
- Caused by Neurofibromatosis type I (von Recklinghausen disease) |
|
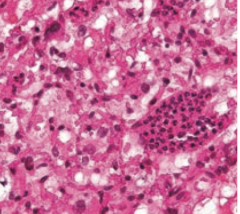
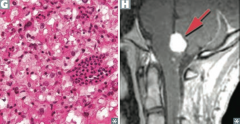
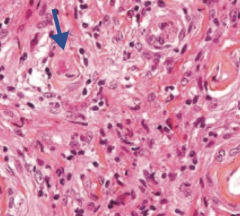
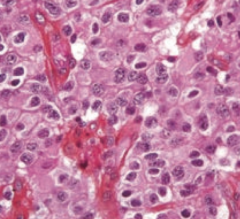
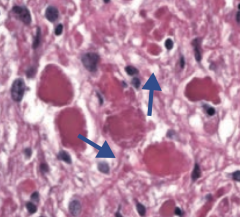
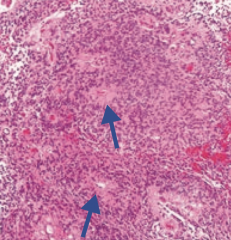
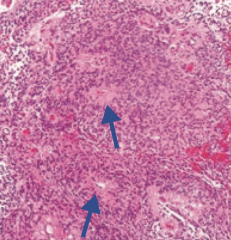
What aspect of von Hippel Lindau disease has this histology?
|
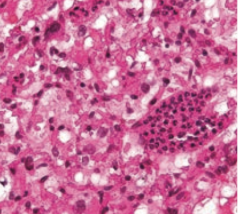
Hemangioblastomas (high vascularity with hyperchromatic nuclei)
|
|

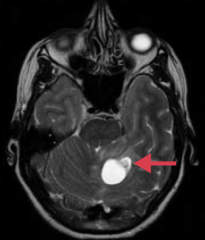
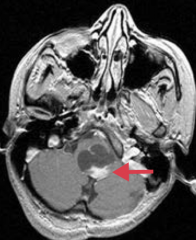
What is this brain finding? Associated with what disease?
|

Hemangioblastoma in cerebellum
- Caused by von Hippel Lindau disease |
|
|
What are the adult primary brain tumors?
|
- Glioblastoma multiforme (grade IV astrocytoma)
- Meningioma - Hemangioblastoma - Schwannoma - Oligodendroglioma - Pituitary adenoma |
|
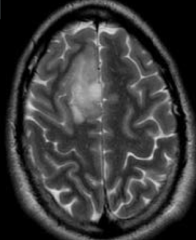
What tumor is found in the cerebral hemispheres and is known for crossing the corpus callosum?
|
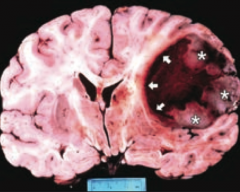
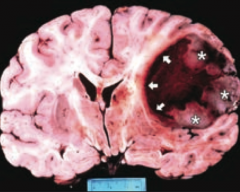
Glioblastoma Multiforme (grade IV astrocytoma)
|
|
|
What is the prognosis of Glioblastoma Multiforme (grade IV astrocytoma)? How common?
|
- Common, in adults
- Highly malignant with ~1 year median survival |
|
|
What is the appearance of a Glioblastoma Multiforme (grade IV astrocytoma)?
|
- Found in cerebral hemispheres
- Can cross corpus callosum ("butterfly glioma") |
|
|
What adult primary brain tumor will stain positively for GFAP? Why?
|
Glioblastoma Multiforme (grade IV astrocytoma) - astrocytes are stained with GFAP
|
|
|
What is the histologic appearance of Glioblastoma Multiforme (grade IV astrocytoma)?
|
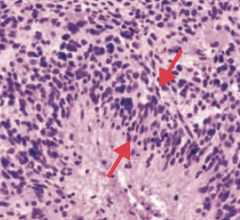
"Pseudopalisading" pleomorphic tumor cells - border central areas of necrosis and hemorrhage
|
|
|
Which type of adult brain tumor occurs in the convexities of hemispheres (near the surfaces of the brain) and parasagittal region?
|
Meningioma
|
|
|
What kind of cells are involved in a Meningioma? Significance for location of tumor?
|
- Arises from arachnoid cells
- Extra-axial (external to brain parenchyma) - May have dural attachment ("tail") |
|
|
What are the symptoms and prognosis for a Meningioma?
|
- Typically benign
- Often asymptomatic - May present with seizures or focal neurologic signs |
|
|
How do you treat Meningioma?
|
Resection and/or radiosurgery
|
|
|
What is the histologic appearance of a Meningioma?
|
- Spindle cells, concentrically arranged in a whorled pattern
- Psammoma bodies (laminated calcifications) |
|
|
What type of adult brain tumor is often cerebellar and is associated with von Hippel-Lindau syndrome when found with retinal angiomas?
|
Hemangioblastoma
|
|
|
What brain tumor can lead to polycythemia? How?
|
Hemangioblastoma - can produce erythropoietin → 2° polycythemia
|
|
|
What is the histologic appearance of a Hemangioblastoma?
|
Closely arranged, thin-walled capillaries with minimal interleaving parenchyma
|
|
|
Which type of adult brain tumor is often found at the cerebellopontine angle and can be localized to CN VIII? Origin of cells?
|
Schwannoma (if localized to CN VIII it is an acoustic schwannoma / acoustic neuroma)
- Schwann cell origin |
|
|
Which adult brain tumor is S-100 (+)?
|
Schwannoma
|
|
|
How do you treat a Schwannoma?
|
Resected or treated with stereotactic radiosurgery
|
|
|
What should you think of if you see bilateral acoustic Schwannomas?
|
NF-2
|
|
|
Which adult brain tumor is often found in the frontal lobes?
|
Oligodendroglioma
|
|
|
What is the histologic appearance of an Oligodendroglioma?
|
- Chicken-wire capillary pattern
- Oligodendrocytes = "fried egg" cells with round nuclei and clear cytoplasm - Often calcified |
|

What type of adult brain tumor can put pressure on the optic chiasm causing bitemporal hemianopia?
|

Pituitary Adenoma (most commonly a prolactinoma)
|
|
|
What are the possible sequelae of a pituitary adenoma?
|
Hyper or hypo-pituitarism
|
|
|
What is the location of the adult brain tumors?
|
- Glioblastoma Multiforme: cerebral hemispheres and corpus callosum
- Meningioma: external to brain parenchyma - Hemangioblastoma: cerebellar - Schwannoma: cerebellopontine angle, may localize to CN VIII - Oligodendroglia: frontal lobes - Pituitary adenoma: pituitary / optic chiasm |
|
|
What are the types of childhood primary brain tumors?
|
- Pilocytic (low-grade) astrocytoma
- Medulloblastoma - Ependymoma - Craniopharyngioma |
|
|
Which type of childhood brain tumor is GFAP (+)?
|
Pilocytic (low-grade) Astrocytoma
|
|
|
Where are Pilocytic (low-grade) Astrocytoma usually found? Prognosis?
|
- Most often in posterior fossa (eg, cerebellum), but can be supratentorial
- Benign with good prognosis |
|
|
Which type of childhood brain tumor is associated with Rosenthal fibers (eosinophilic, corkscrew fibers)?
|
Pilocytic (low-grade) Astrocytoma
|
|
|
What is the gross and histologic appearance of Pilocytic (low-grade) Astrocytoma?
|
- Usually well circumscribed
- Rosenthal fibers: eosinophilic, corkscrew fibers - Cystic + solid |
|
|
Which type of childhood brain tumor is a form of primitive neuroectodermal tumor?
|
Medulloblastoma
|
|
|
What can a Medulloblastoma cause?
|
- Can compress the 4th ventricle → hydrocephalus
- Can send "drop metastases" to spinal cord |
|
|
What type of childhood brain tumor is associated with Homer-Wright rosettes? Prognosis?
|
Medulloblastoma - highly malignant
|
|
|
What is the gross and histologic appearance of Medulloblastoma?
|
- Solid cerebellar tumor
- Homer-Wright rosettes - Small blue cells |
|
|
What type of childhood brain tumor is derived from ependymal cells? Prognosis?
|
Ependymoma - poor prognosis
|
|
|
What can an Ependymoma cause?
|
Most commonly found in 4th ventricle so it can cause hydrocephalus
|
|
|
What type of childhood brain tumor is associated with perivascular rosettes
|
Ependymoma
|
|
|
What is the gross and histologic appearance of an Ependymoma?
|
- Commonly in 4th ventricle
- Perivascular rosettes - Rod-shaped blepharoblasts (basal ciliary bodies) found near nucleus |
|
|
What type of childhood brain tumor may be confused with a pituitary adenoma? Source?
|
Craniopharyngioma - derived from remnants of Rathke pouch
|
|
|
What is the prognosis and clinical syndrome caused by Craniopharyngioma?
|
- Benign tumor
- May be confused with pituitary adenoma because they both cause bitemporal hemianopia |
|
|
What is the most common childhood supratentorial brain tumor?
|
Craniopharyngioma
|
|
|
What is the histologic appearance of a Craniopharyngioma?
|
Calcification is common (tooth-enamel like)
|
|
|
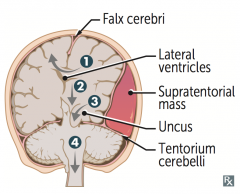
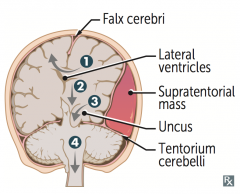
What are the types of herniation syndromes?
|
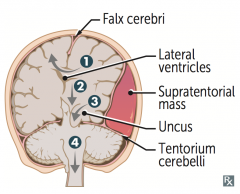
1. Cingulate (subfalcine) herniation under falx cerebri
2. Downward transtentorial (central) herniation 3. Uncal herniation 4. Cerebellar tonsillar herniation into foramen magnum |
|
|
What type of herniation can compress the anterior cerebral artery?
|
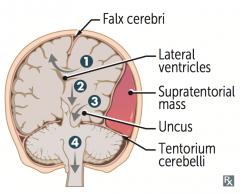
Cingulate (subfalcine) herniation under falx cerebri (#1)
|
|
|
What type of herniation can compress the ipsilateral CN III causing a blown pupil and down and out gaze?
|
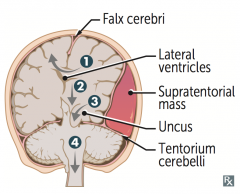
Uncal Herniation (#3) - medial temporal lobe
|
|
|
What type of herniation can compress the posterior cerebral artery causing contralateral homonymous hemianopsia)?
|
Uncal Herniation (#3) - medial temporal lobe
|
|
|
What type of herniation can compress the contralateral crus cerebri causing ipsilateral paralysis / false localization sign?
|
Uncal Herniation (#3) - medial temporal lobe
|
|
|
What type of herniation can compress the brainstem, inhibiting respiration, and possibly causing coma and death?
|
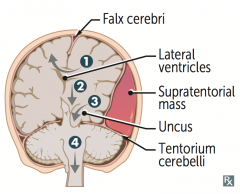
Cerebellar tonsillar herniation into the foramen magnum (#4)
|
|
|
What are the potential consequences of a cingulate (subfalcine) herniation under the falx cerebri?
|
Can compress anterior cerebral artery
|
|
|
What are the potential consequences of an uncal herniation?
|
Compresses:
- Ipsilateral CN III → blown pupil and down and out gaze - Ipsilateral PCA → contralateral homonymous hemianopsia - Contralateral crus cerebri → ipsilateral paralysis, "false localization sign" |
|
|
What are the potential consequences of a cerebellar tonsillar herniation into the foramen magnum?
|
Coma and death result when these herniations compress the brain stem (and inhibit respiration)
|