Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
69 Cards in this Set
- Front
- Back
|
What are the cells in the adenohypophysis that produce growth hormone (GH)?
|
Somatotrophs
|
|
|
What are the cells in the adenohypophysis that produce prolactin (PRL)?
|
Lactotrophs
|
|
|
What are the cells in the adenohypophysis that produce ACTH, POMC, MSH, endorphins and lipotropin?
|
Corticotrophs
|
|
|
What are the cells in the adenohypophysis that produce TSH?
|
Thyrotrophs
|
|
|
What are the cells in the adenohypophysis that produce FSH and LH?
|
Gonadotrophs
|
|
|
What are the two peptide hormones that are produced by pituicytes and axonal processes extending from nerve cell bodies in supraoptic and paraventricular nuclei of the hypothalamus?
|
ADH/vasopressin
Oxytocin |
|
|
What types of neoplasms are more likely to produce excess secretion of trophic hormones?
|
Forms of Hyperpituitarism, specifically Benign tumors (adenomas)
|
|
|
What is the most common cause of hyperpituitarism?
|
Adenoma
|
|
|
T/F
Pituitary adenomas are classified on the basis of the hormones produced. |
True
i.e. TSH adenoma, PRL adenoma, etc. |
|
|
What is the most frquent type of hyperfunctioning pituitary adenoma?
|
Prolactinomas (PRL adenoma)
|
|
|
What two adenomas result in complications for dentistry?
|
Excess production of ACTH
Persistent hypersecretion of GH |
|
|
What leads to the development of hypercortisolism known as Cushing syndrome?
|
Excess production of ACTH by corticotroph adenoma
|
|
|
What causes hepatic secretion of isulin-like growth factor (IGF-I or somatomedin C), which causes many clinical manifestations?
|
Persistent hypersecretion of GH
|
|
|
What happens if a somatotrophic adenoma develops in children Before the epiphyses have closed?
|
The elevated levels of GH result in gigantism
|
|
|
T/F
Acromegaly and gigantism can occur together or separately, depending on when the tumor develops. |
True
|
|
|
What does the prefix Acro mean?
|
Acro = the most distal point
|
|
|
What develops if increased levels are present After closure of the epiphyses?
|
Acromegally
|
|
|
Which GH disorder results in hyperostosis (increases bone density)?
|
Acromegally
|
|
|
What GH associated disorder has growth most conspicuous in skin and soft tissues, increased bone density, prognathic jaw, frontal bossing, large ears, big nose, macroglossia, hands and feet are enlarged with broad, plump fingers, diabetes mellitus?
|
Acromegally
|
|
|
What causes a Diabetes insipidus and is characterized by excessive urination (polyuria) owing to an inability of the kidney to reabsorb water properly from the urin?
|
ADH deficiency
|
|
|
What do these lesions cause?
idiopathic sporadic mutations, familial (30%) Tumors (25%) Trauma (16%) Post-hypophysectomy (20%) |
ADH deficiency resulting in Diabetes Insipidus
|
|
|
What causes a deficiency in water resorption in the collecting duct?
|
ADH deficiency causing Diabetes Insipidus
|
|
|
What is a hypermetabolic state (increased BMR) caused by and elevation of free T3 and T4?
|
Thyrotoxicosis
|
|
|
What is an interchangeable term for Hyperthyroidism?
|
Thyrotoxicosis
|
|
|
What are the following conditions associated with?
Graves Disease (diffuse toxic hyperplasia) Hyperfunctioning multinodular goiter Hyperfunctioning adenoma Iodine-induced hyperthyroidism TSH secreting pituitary adenoma (rare) |
Hyperthyroidism
|
|
|
What are the most common causes of thyrotoxicosis?
|
Diffuse hyperplasia
Hyperfunctional Multinodular Goiter Hyperfunctional Adenoma of the thyroid |
|
|
What is the term for a tumor that is producing too much of the hormone that is normally produced by healythy tissue from that area?
|
Toxic tumor
|
|
|
What are the clinical manifestations of hyperthyroidism and are generally referable to the hypermetabolic state and the overactivity of the sympathetic nervous system?
|
1. Increased BMR (skin is soft, warm, and flushed; heat intolerance with sweating; weight loss & increased appetite)
2. Cadiac manifestations (increased CO; tachycardia; palpitations; cardiomegaly; arhythmias; CHF) 3. Neuromuscular manifestations are related to overactivity of the sympathetic nervous system. (tremor, hyperactivity, emotional liability, anxiety, inability to concentrate, insomnia, muscle weakness) 4. Occular changes (wide staring gaze like someone just said boo; lid lag; thyroid ophthalmopathy associated with exiphthalmos (only in graves disease)) 5. GI Manifestations (sympathetic hyperstimulation results in hypermotility, malabsorbtion, diarhea) 6. Skeletal manifestations (Thyroid hormone stimulates bone resorption leading to osteoporosis and an increased risk of fractures |
|
|
*What is a condition associated with Graves disease, but NOT other forms of hyperthyroidism?
|
Thyroid Opthalmopathy associated with exophthalmos
|
|
|
*What is an abrupt/acute onset of severe hyperthyroidism and is a medical emergency as some untreated patients die of cardiac arrhythmias?
|
Thyroid Storm
Patient can progress on coma and death. |
|
|
*What is important regarding dental management of the hyperthyroid patient?
|
1. No elective dental care should be given to a patient with hyperthyroidism until the patient has been rendered euthyroid (the condition of having normal thyroid function, as opposed to hyperthyroidism and hypothyroidism)
2. Epinephrine-containing local anesthetics and retraction cords should be avoided because of epinephrine's cardiostimulating and hypertensive action 3. Thyroid storm is a medical emergency |
|
|
*What is the most common cause of endogenous hyperthyroidism?
|
Grave's Disease
|
|
|
*What is the triad of clinical findings for Grave's disease?
|
1. Hyperthyroidism
2. Infiltrative ophthalmopathy with exophthalmos (from the loose connective tissue pushing the eye out, not found in other forms of hyperthyroidism) 3. Localized infiltrative dermopathy (pretibial mixedema) (deposits of tissue on the skin of the leg over the tibia and down to the ankle, Not found in other types of hyperthyroidisms) |
|
|
*What makes Primary hypothyroidism primary?
|
Because of an intrinsic abnormality within the thyroid gland itself.
|
|
|
*What are the most common causes of Primary Hypothyroidism?
|
1. Surgical or radiation induced ablation as well as thyroid agenesis or hypoplasia
2. Autoimmune hypothyroidism with the majority of cases associated with Hashimoto Thyroiditis (hashimoto's is a prototype autoimmune disease) |
|
|
What is the name for hypothyroidism developing in infants or in early childhood?
|
Cretinism
|
|
|
*What is hypothyoidism that develops in an older child or adult?
|
Myxedema
|
|
|
*What is the most important clinical feature of cretinism?
|
Severe mental retardation particularly if maternal thyroid deficiency develops before development of the fetal thyroid
|
|
|
*What is the most common cause of hypothyroidism in areas of the world where iodine levels are sufficient?
|
Hashimoto Thyroiditis
|
|
|
*How does Hashimotothyroiditis occur?
|
Progressive autoimmune destruction of the thyroid gland
(immune system reacts against a variety of thyroid antigens; thyroid tissue is destroyed and it kind of looks like it is being replaced with lymphocytes) |
|
|
*What is the most common type of thyroid cancer?
|
Papillary Carcinoma - this is the least aggressive 95% 10-year survival rate for papillary carcinomas of the thyroid
|
|
|
*What is MEN-2A & MEN-2B associated with in Medullay carcinomas?
|
MEN-2A = Sipple Syndrome
MEN-2B = Williams Syndrome (MEN = Multiple Endocrine Neoplasia Syndromes) |
|
|
*What are neuroendocrine neoplasms derived from the Parafollicular (C) cells of the Thyroid?
|
Medullary Carcinoma
(the other three types of thyroid carcinomas all arise from follicular epithelial cells) |
|
|
*What are the three types of neoplasms associated with the Thyroid?
|
Papillary Carcinoma
Medullary Carcinoma MEN-2A Sipple Syndrome Medullary Carcinoma MEN-2B Williams Syndrome* |
|
|
What are chromaffin cell tumors that produce catecholamines, particularly epinephrine?
|
Pheochromocytomas (this will increase BP; these patients will often have a problem with hypertension)
|
|
|
What are the manifestations of MEN-2B syndrome?
|
Agressive Medullary Carcinomas and Pheochromocytomas
Neuromas or ganglioneuromas of the skin, oral mucosa, tongue, eyes and respiratory and GI tracts Marfanoid habitus (tall, slender, long fingers) A single AA change in the RET gene locus gives rise to the disorder tumors have ill defined margins |
|
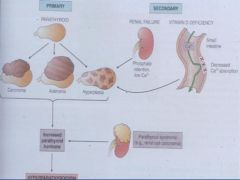
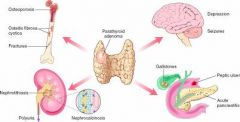
*What are the properties of Primary Hyperparathyroidism?
|
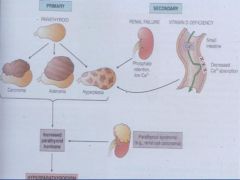
Disease is within the gland
Represents an autonomous, spontaneous overproduction of PTH. |
|
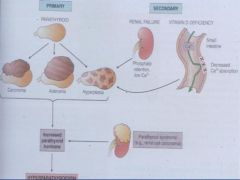
*What are the characteristics of Secondary Hyperparathyroidism?
|
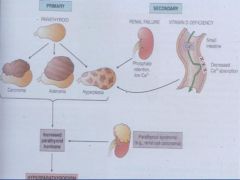
Occurs as secondary phenomena most commonly associated with renal insufficiency
|
|
What is the most common cause of Primary Hyperparathyroidism?
|
Adenoma (75-80% of cases)
[Hyperplasia (10-15%), Carcinoma <5%] |
|
|
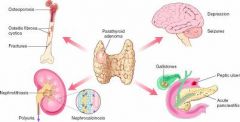
What are the Classic Clinical Presentations of Primary Hyperparathyroidism?
|
Reflect the combined effects of increased PTH and hypercalcemia
The constellation of symptoms can be summarized by the statement: Painful bones, Renal stones, Abdominal groans, Psychic moans with Fatigue overtones |
|
|
What are the dental manifestations of Hyperparathyroidism?
|
1. Loss of lamina dura
2. Ground glass appearance (Little radiolucencies and radiopacities right next to each other; looks foggy or stippled) 3. Osteoporosis 4. Brown tumor (brown appearance from osteoclasts RBCs and Hemosiderin from the breakdown of RBCs, cellular fibrous CT) 5. Osteitis Fibrosa Cystica |
|
What is the Most common cause of the secondary form of Secondary Hyperparathyroidism?
|
Renal Failure
(causes retention in phosphate, which means we have low serum levels; This causes hyperplasia of the gland and more PTH is produced in an attempt to increase serum calcium) |
|
What is the most likely cause of Cushing Syndrome?
|
Administration of Exogenous Glucocorticoids
|
|
|
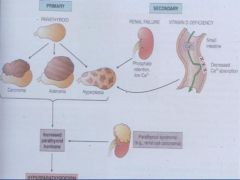
What are the four different ways that one can develop Cushing Syndrome?
|
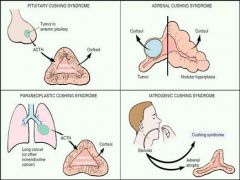
1. Pituitary Cushing Syndrome
2. Adrenal Cushing Syndrome 3. Latrogenic Cushing Syndrome 4. Paraneoplastic Cushing Syndrome |
|
|
Which Cushing Syndrome is caused by ACTH causes hyperplasia of adrenal cortex and excess cortisol levels?
|
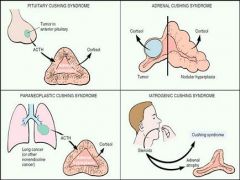
Pituitary Cushing syndrome
|
|
|
Which Cushing Syndrome occurs when the disease process is in the adrenal cortex?
|
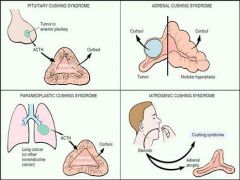
Adrenal Cushing Syndrome
|
|
|
Which Cushing Syndrome is caused by the physician? When you are taking steroids your adrenal gland undergoes atrophy.
|
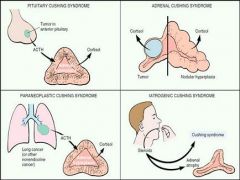
Laterogenic Cushing Syndrome
|
|
|
Which Cushing Syndrome occurs when there is small cell carcinoma of the lung that can produce ACTH or ACTH-like cmpds, leading to hypercortisolism?
|
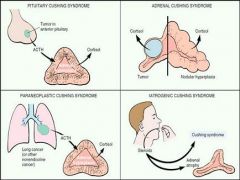
Paraneoplastic Cushing Syndrome
|
|
|
What is the biggest negative effect can glucocorticoids have on the body?
|
Glucocorticoids suppress the immune response so these patients are prone to infection.
|
|
|
What are the clinical features of Cushings Syndrome?
|
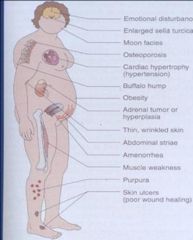
Emotional Disturbance
Enlarged Sella Turcica Moon Faced Osteoporosis Cardiac Hypertrophy (hypertension) Buffalo Hump Obesity Adrenal Tumor or Hyperplasia Thin wrinkled skin Abdominal Striae Amenorrhea Muscle Weakness Purpura Skin Ulcers (poor wound healing) |
|
|
What are the two types of Primary Adrenal Insufficiency?
|
Primary Acute Adrenal Insufficiency (Waterhouse-Friderichsen Syndrome)
Primary Chronic Adrenal Insufficiency (Addison Disease) |
|
|
What are the two causes of Primary Acute Adrenal Insufficiency?
|
1) Chronic AI that can undergo an acute exacerbation that can lead to an adrenal crisis
2) Waterhouse-Friedrich Syndrome (bacterial infection where you get hemorrhage into the adrenal gland, which destroys the gland. May turn into a sack of blood) |
|
|
What is the cause of primary Chronic Adrenal Insufficiency?
|
Addison Disease - Described by the constellation of symptoms of the disease as including general languor and dibility, remarkable feebleness of the heart's action and a peculiar change in color of the skin associated with a disease of the adrenal glands
|
|
|
What are the dental considerations of Primary Chronic AI?
|
1)Low Coping under stress
2)Hypotension 3)Hypoglycemic syncope 4)Most diagnosed pts are taking steroids and under control 5)Non-diagnosed pts should be referred for a steroid therapy consult |
|
|
What are the four disorders that cause 90% of adrenal cortex damage cases?
|
1)Autoimmune Adrenalitis (mostly)
2)Tuberculosis 3)AIDS 4)Metastatic cancers |
|

What are the clinical manifestations of Grave's Disease?
|
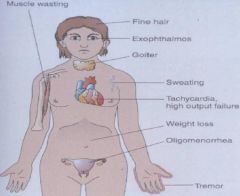
1) Muscle Wasting
2) Fine Hair 3) Exophthalmos 4) Goiter 5) Sweating 6) Tachycardia (high output failure) 7) Weight loss 8) Oligomenorrhea 9) Tremor |
|
What are the clinical features of Mixedema aka Gull Disease?
|
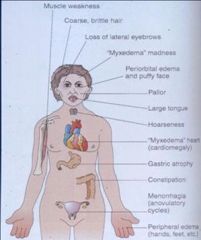
1) Muscle Weakness
2) Course Brittle Hair 3) Loss of Lateral Eyebrows 4) Myxedema Madness 5) Periorbital Edema and puffy face 6) Pallor 7) Large Tongue 8) Hoarseness 9) Mixedema Heart (cardiomegally) 10) Gastric Atrophy 11) Constipation 12)Menorrhagia (anovulatory cycles) 13) Peripheral Edema (hands, feet) |
|
|
What are the Clinical Features of Primary Chronic Adrenal Insufficiency?
|
1) Doesn't present clinically until 90% of the cortex is destroyed
2) Progressive weakness and patient is easily fatigued 3) GI disturbances including anorexia, nausea, vomiting, weight loss and diarrhea 4) Hyperpigmentation of the skin and oral mucosa particularly on sun exposed areas, pressure points. 5) Decreased mineralcorticoid activity results in electrolyte disturbaces which manifest as hyperkalemia, hyponatremia, volume depletion and hypertension 6) Stresses such as infections trauma and surgery may precipitate an acute crisis manifest by vomiting, abdominal pain, hypotension, coma and vascular collapse; death may occur unless corticosteroid therapy begins at once. |
|
|
What is a neoplasm of the Adrenal Medulla?
|
Pheochromocytoma
|