Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
123 Cards in this Set
- Front
- Back
|
The EKG (electrocardiogram) is a graph that records....
|
the electrical activity of the heart
|
|
|
The ECG records the _____________________ in potential between the electrodes
|
differences
|
|
|
the signal for cardiac electrical stimulation starts in the...
|
sinus node, aka SA node
automaticity functions as normal pacemaker of the heart |
|
|
The AV junction serves to....
|
primarily shuttle electrical stimulus into ventricles
can also act as an independent pacemaker of the heart (if SA node fails to function properly, the AV junction can act as an escape pacemaker) |
|
|
Conduction is slow at the AV node because....
|
it allows ventricles time to fill with blood before signal for cardiac contraction arrives
|
|
|
Sick Sinus Syndrome
|
severe depression of SA node function
Patients experience light-headedness or even syncope d/t excessive bradycardia |
|
|
The outside of a resting cell is _________________, and the inside is ____________.
|
positive
negative (90 mV) |
|
|
When a heart muscle cell is stimulated (depolarizes), the outside of the cell becomes _______________, and the inside of the cell becomes ___________________.
|
negative
positive |
|
|
For the entire myocardium, depolarization proceeds from the ___________ layer to the ______________ layer.
Repolarization proceeds in the _______________ direction |
innermost (endocardium)
outermost (epicardium) opposite |
|
|
P wave: ____________________
PR interval: _____________________ QRS complex: ________________ ST segment, T wave, and U wave: _____________________ |
Atrial depolarization
Time from initial stimulation of atria to initial stimulation of ventricles; time for stimulus to spread through atria and pass through AV junction Ventricular depolarization Ventricular repolarization |
|
|
on a standardized ECG, 1 mV is ______ mm tall
|
10
|
|
|
The PR interval is measured from.....
|
the beginning of the P wave to the beginning of the QRS complex
|
|
|
normal PR interval is between
|
0.12 - 0.20 seconds
(~ 3-5 small boxes) |
|
|
Prolongation of the PR interval above 0.2 seconds is called....
|
1st degree heart block
(when conduction through AV junction is impaired, the PR interval maybe become prolonged) |
|
|
QRS Complexes
|
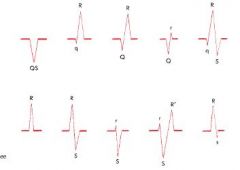
initial negative deflection is Q wave
the first positive deflection is R wave a negative deflection following is S wave If the entire complex is positive = R wave, if entire complex is negative = QS wave Extra waves are R' if positive, S' if negative |
|
|
QRS interval is normally....
|
0.1 seconds or less
A wide or prolonged QRS could indicate a block in one of the bundle branches |
|
|
ST segment is usually...
|
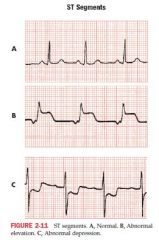
isoelectric
some pathological conditions such as MI can produce elevated or depressed ST segment |
|
|
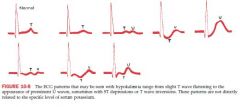
T wave normally ...
|
has a asymmetric shape with its peak closer to the end of the wave than the beginning
can become symmetrical in certain conditions such as MI and hyperkalemia |
|
|
The QT interval is measured from...
|
the beginning of the QRS complex to the end of the T wave
As the HR increases and RR interval shortens = QT interval shortens As HR decreases and RR interval lengthens = QT interval lengthens |
|
|
Rate-corrected QT (QTc)
|

Normally the QTc is less than or equal to 0.44 seconds
|
|
|
The QT interval can be prolonged by
|
certain drugs used to treat cardiac arrhythmias (amiodarone, quinidine, procainamide)
as well as other agents such as tricyclic antidepressants, phenothiazides, pentamidine, etc Electrolyte imbalances such as hypokalemia, hypomagnesemia, hypocalemia can cause prolongation Hypothermia, MI and infarction, subarachnoid hemorrage |
|
|
A prolonged QT prolongation may predispose patients to
|
potential lethal ventricular arrhythmias such as torsades de pointes
|
|
|
A shortened QT interval can be due to....
|
digitalis in therapeutic doses
hypercalcemia |
|
|
U wave is a
|
small rounded defleection sometimes seen after T wave
prominent U waves are characteristic of hypokalemia (very prominent U waves may also be seen in patients taking sotalol, phenothiazines or after CVA) Normally seen in the same direction as a T wave BUT if negative u wave follows a positive T wave, it could indicate LVH and MI |
|
|
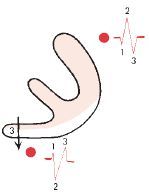
When the stimulus spreads downward and left, you will get...
|
Positive P wave in Lead II
Negative P wave in aVR = normal sinus rhythym |
|
|
When AV junction or ectopic pacemaker is pacing the heart....
|
atrial depolarization spreads up the atria in a retrograde direction (upward and right);
= positive P wave in aVR and negative P wave in lead II |
|
|
Mean QRS Axis
|
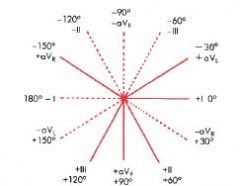
points midway between any two leads that show tall R waves of equal height
or directed 90 degrees from the lead that shows a biphasic complex, and + or - based on the lead showing the taller R wave |
|
|
In ECG of normal healthy individuals, the axis lies between...
|
-30 and +100
|
|
|
RAD exists if...
|
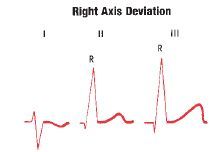
Axis of 100 or more positive (vertical) to +180
When leads II and III show tall R waves of equal height, QRS axis must be +90 If leads II and III show tall R waves and RIII > RII, then RAD is present (also lead I shows rS pattern with S wave deeper than R wave is tall) Another option: negative in Lead I, positive in Lead aVF |
|
|
LAD exists if...
|
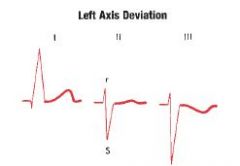
Axis of -30 or more negative ( horizontal) to -90
Lead II shows an rS complex with S wave deeper than R wave is tall Lead I shows a tall R wave Lead III shows a deep S wave aVL shows Rs Another option: positive in Lead I, negative in Lead aVF |
|
|
Causes if RAD
|
RVH is an important cause
lateral MI Left posterior hemiblock (rarer cause) COPD Acute PE |
|
|
Causes of LAD
|
LVH
Left anterior hemiblock is a common cause of marked deviation (more negative than -45) May be seen with LBBB* |
|
|
Right Atrial Abnormality
|
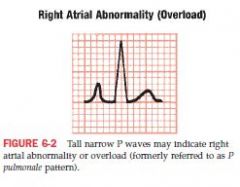
may cause increase in voltage of P wave
Normally the P wave is less than or equal to 2.5mm in amplitude; less than 0.12 seconds in width With RAA, the width of P wave is normal ( <0.12) but the height exceeds 2.5mm* = tall P waves Tall narrow P waves can be seen based in leads IIl, III, aVF, and sometimes V1 |
|
|
P Pulmonale
|
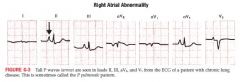
Dx can be made by finding an abnormally tall P wave in leads II, III, aVF or V1
RAD poor R wave progression Causes of pulmonary HTN: Chronic lung disease [cor pulmonale] Tricuspid stenosis Congenital heart disease (pulmonic stenosis, Fallot) Primary pulmonary HTN Renal Vascular Occlusion |
|
|
Clinical significance of RAA
|
usually associated with RVH** (volume overload)
MC causes of RAA are pulmonary disease and congenital heart disease The pulmonary disease can be asthma, PE, or COPD Congestive heart disease can include pulmonic valve stenosis, atrial septal defects, Ebstein's anomaly and tetralogy of Fallot |
|
|
Left Atrial Abnormality
|
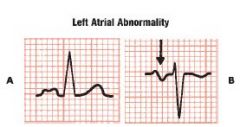
LAA should prolong the duration of atrial depolarization = abnormally wide P wave ( >0.12)*
Amplitude may be normal or increased the P waves can sometimes have a humped or notched appearance in I and II Lead V1 sometimes shows a biphasic P wave |
|
|
Clinical significance of LAA
|
Valvular heart disease (aortic stenosis, aortic regurgitation, mitral regurgitation and mitral stenosis) - listen for clicks and murmurs
Hypertensive heart disease which causes L ventricular enlargement and eventually LAA Cardiomyopathies Coronary artery disease |
|
|
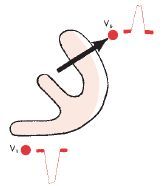
Normally the ______ ventricle is electrically predominant because of its greater mass
|

Left
as a reuslt, V1 which is placed on the right side of the chest records rS complexes indicating the spread of depolarization away from the right and towards the L side |
|
|
Right ventricular hypertrophy
|

Right chest leads (V1) show tall positive R waves
Along with tall R waves, RVH also produces RAD* and T wave inversions in right to mid-chest leads V1-V3 (right ventricular "strain" pattern)* |
|
|
RVH cause and associations
|
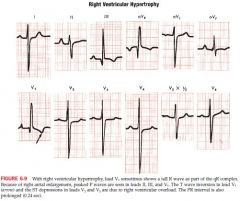
congential heart disease (pulmonic stenosis, atrial septal defect, tetralogy of Fallot) or lung disease (COPD, pulm HTN) that often causes RAA* also causes RVH; so signs of RVH are sometimes accompanied by tall P waves
The presence of RBBB by itself does not indicate RVH but a complete or incomplete RBBB with RAD should raise strong suspicion COPD may only show strain |
|
|
Left Ventricular Hypertrophy
|
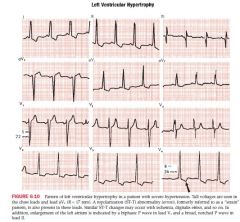
abnormally tall positive R waves seen in Left chest leads, and abnormally deep negative S waves seen in Right chest leads
If the sum of depth of the S wave in V1 and the height of the R wave in V5 or V6 exceeds 35mm, LVH should be considered Sometimes LVH produces tall waves in aVL (11-13mm +) ST-T changes are often seen in LVH (slight depression and broadly inverted T wave best seen in leads with tall R waves) Axis usually horizontal or LAD May eventually develop an incomplete of complete LBBB Signs of LAA (broad p waves in limb leads or wide biphasic p waves in V1) often seen |
|
|
LVH cause and associations
|
often with LAA
due to the presence of pressure or volume overload state such as systemic HTN and aortic stenosis, aortic regurgitation, mitral regurgitation and dilated cardiomyopathy at increased risk for CHF and arrhythmias |
|
|
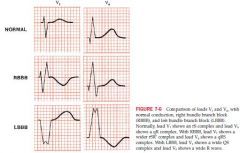
Right Bundle Branch Block
|
QRS complex will be widened - delays right ventricular depolarization creating a R' in V1 and wide negative S wave in lead V6
V1 = rSR' with broad R' wave (S wave does not necessarily make its way below the baseline and gets a notched appearance instead) V6 = qRS with broad S wave (S waves in I may occur) T waves can also be inverted in V1-V3 (secondary changes) and II, II and aVF; in leads with rSR' complex **(primary T wave changes would be from ischemia, hypokalemia or digitalis; in other leads like V4 and V5) |
|
|
Complete and Incomplete RBBB
|
Complete: QRS is 0.12 seconds or greater in duration, with an rSR' in lead V1 and a qRS in lead V6
Incomplete: QRS is 0.1-0.12 in duration with rSR' in lead V1 and qRS in lead V6 |
|
|
Clinical significance of RBBB
|
not necessarily abnormal but can be associated with heart disease
atrial septal defect COPD with pulmonary HTN pulmonic stenosis chronic coronary artery disease PE |
|
|
Left Bundle Branch Block
|
Wide QRS complex; LBBB affects early phase of ventricular depolarization
With LBBB, septum depolarizes from R to L so ECG losses normal septal r wave in lead V1 and normal septal q wave in V6 Lead V6 will show a wide entirely positive tall R wave with no q wave +\- notching at its peak (M shape) Lead V1 will record a wide negative QS complex +\- a small notching at its point (W shape)' (may show a broad R notched wave in I and aVL) Secondary T wave inversions also occur here with the tall R waves |
|
|
Complete and Incomplete LBBB
|
Complete: QRS is 0.12 sec or wider with tall wide R waves in V6 and wide QS in V1
Incomplete: QRS is 0.1-0.12 wide with tall wide R waves in V6 and wide QS in V1 |
|
|
Clinical Significance of LBBB
|
usually a sign of heart disease
long standing HTN or valvular disease coronary artery disease** and impaired L ventricular function Underlying LVH |
|
|
RBBB vs LBBB
|
|
|
|
Hemiblock/fascicular block
|
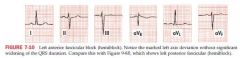
A block in either fascicle of the LBB system; partial block
does not widen the QRS complex; affects axis instead Left anterior hemiblock results in marked LAD (-45 or more negative); S wave in aVF equals or exceeds R in lead I; aVL shows a qR complex with rS complexes in II, III, and avF Left posterior hemiblock produces marked RAD (+120 or more positive); rS complex in I, qR complex in II, III, and aVF Dx made primarily from the limb leads; anterior more common |
|
|
LAFB vs LPFB summary
|
anterior: negative in II and avF and positive in I and aVL
posterior: negative in I and positive in II and III and aVF usually with RBBB; can mimic or mask AMI |
|
|
Cardiac blood supply
|
Right coronary artery - both inferior portion of heart and right ventricle
Left anterior descending coronary artery - ventricular septum and large part of L ventricular free wall Left circumflex coronary artery - lateral wall of L ventricle |
|
|
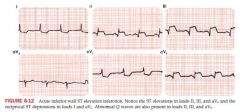
ECG changes with acute transmural infarction
|
acute phase: ST elevations +\- hyperacute T waves in certain leads
evolving phase: occurs hours or days later with deep T wave inversions in leads that previously shows ST elevations (ST returns to baseline) |
|
|
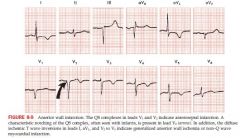
Location of infarct
|

Anterior wall: ST elevations and hyperacute T waves appear in one or more of V1-V6 and I, aVL; ST depressions in II, II and AVF
Inferior wall: ST elevations and hyperacute T waves are seen in II, II and aVF; ST depressions in V1 to V3, I and AVL Lateral: I, aVL, V5-6 Septal: V1, V2 Anterior: V3, and V4 Posterior: V1 |
|
|
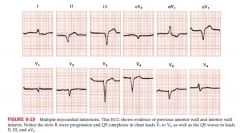
QRS changes with infarction
|
New Q Waves (can persist for months and even years after an acute infarction)
with transmural infarction, necrosis of heart muscle causes some voltages to disappear and instead of positive R waves over infarcted area, Q waves are often recorded Generally appear within 1st day or so of the infarct With anterior wall infarction, Q waves are seen in one or more of leads V1 to V6, I and aVL With inferior wall infarction, new Q waves seen in II, III, and aVF |
|
|
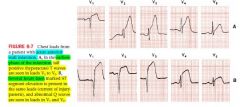
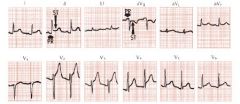
Anterior wall Q wave infarction
|
Characteristic feature of anterior wall is loss of normal R wave progression with pathological Q waves in the chest leads, I and aVL with inverted T waves
caused by occlusion of left anterior descending coronary artery or left circumflex coronary artery |
|
|
Inferior Wall infarctions
|
abnormal Q waves in leads II, III, aVF
generally caused by occlusion of Right coronary artery and less commonly by left circumflex coronary obstruction |
|
|
Posterior wall infarction
|
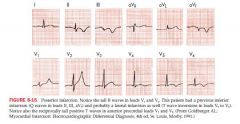
Tall R waves and ST depressions may occur in V1 and V2
can extend to lateral wall producing changes in V6, or to inferior wall producing changes in II, III, and aVF |
|
|
Determining an abnormal Q wave
|
normal septal q waves are narrow and low amplitude - less than 0.04 seconds
Abnormal Q wave is longer than 0.04 seconds in lead I, II, III, aVF, or V3 to V6 If large Q waves are seen in V1, normal If seen in V1 and V2, may be evidence of anterior septal MI |
|
|
Old vs new Q waves
|
Old MIs have Q waves but no ST elevation or depression
New Mis have Q waves with associated elevation or depression |
|
|
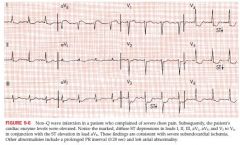
Subendo Ischemia (not infarct)
|

subendo is most vulnerable bc it is the most distant form the coronary blood supply
ST depression mostly seen in I, aVL, V1 to V6 or II, III and aVF; with elevation seen in aVR It has a characteristic squared off shape seen when experiencing angina |
|
|
Non-Q wave with Subendo infarction
|
|
|
|
Diverse changes if MI
|

early stage: Tall T wave, some ST depression
Stage I: ST elevation and R waves, no Q waves, T still positive Intermediate: ST elevation, Q waves, inverted T waves NonQ wave MI shows T wave inversion with no elevations or Q waves |
|
|
Cardiac Drugs
|
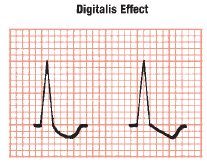
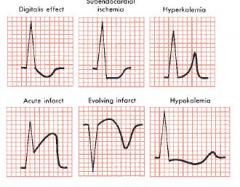
Digitalis shortens repolarization time in ventricles = shortens QT interval and associated with scooping of the ST interval
Quinidine, procainamide, and disopyramide are antiarrhythmic drugs but prolong ventricular repolarization due to blocking of K channel = prolong QT interval and flatten the T waves (toxic doses widen QRS) - can produce prominent U waves Prolongation of QT + u waves with risk of torsades de pointes can occur with ibutilide, sotalol, amiodarone, |
|
|
Other Drugs
|
psychotropic drugs such as antidepressants and phenothiazines can induce syncope or cardiac arrest in toxic doses due to Vtach or asystole
May also prolong QRS interval, causing BBB like pattern or lengthen repolarization (long QT interval) predisposing pts to torsades de pointes |
|
|
quinidine effects
|
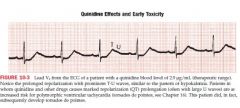
T-U waves
|
|
|
amiodarone effects
|
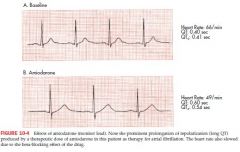
prolong QT
|
|
|
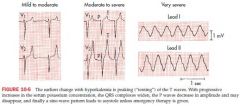
Hyperkalemia
|
normal serum conc is 3.5-5
narrowing and peaking of T waves (tented or pinched shape) and can become quite tall* with further elevation of serum levels, PR intervals become prolonged and p waves are smaller and may disappear continued elevations produce widening of QRS Seen most commonly with kidney failure |
|
|
Hypokalemia
|
ST depressions with prominent U waves* and prolonged repolarization
Flattened T waves |
|
|
Hypercalcemia and Hypocalcemia
|
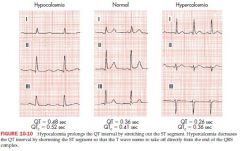
ventricular repolarization is shortened by hypercalcemia
ventricular repolarization is lengthened by hypocalcemia Hyper: Short QT* and short ST, and T wave appeasr to take off right from end of QRS; may lead to coma or death; AMS Hypo: long QT*, stretched out ST |
|
|
Specific ST changes
|
|
|
|
Pericarditis
|
early phase: ST elevations seen in both anterior and inferior leads with PR depression (V5, V6)
elevation of PR in aVF and depression of ST T wave inversions may follow ST elevations No Q waves |
|
|
Pericardial Effusions
|
low voltage (5 mm or less) QRS complexes
|
|
|
Pulmonary embolisms
|
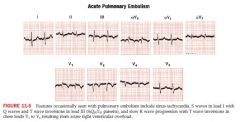
sinus tachy
strain pattern of inverted T waves in V1-V4 S wave lead I, new Q wave in lead III with T wave inversion in III RAD RBBB pattern |
|
|
Wolff Parkinson White
|
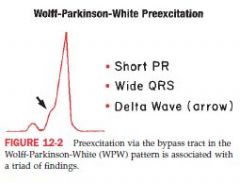
QRS widened d/t early stimulation
PR is shortened upstroke of QRS = delta wave tat is also slurred or notched - can be mistaken for BBB or MI Pts are prone to arrhythmias, esp paroxysmal supraventricular tachy, can develop afib |
|
|
Causes of sinus tachycardia
|
anxiety, excitement, pain
epi, dopamine, antidepressant, cocaine atropine, anticholinergic fever, infection, septic shock CHF, PE, acute MI, hypoxia Hyperthyroidism, volume loss from bleeding, V, D, dehydration intoxication or withdrawal |
|
|
Causes of sinus bradycardia
|
trained athletes
digitalis, beta blockers, ccb hypothyroidism hyperkalemia sick sinus syndrome, sleep apnea, vasovagal reactions |
|
|
Sinus pause or Sinus arrest
|
SA node fails to stimulate atria or prolonged period
Leads to syncope or even cardiac arrest with asystole unless some other escape pacemaker takes over Escape beats can come from atria, AV node or ventricles *SA block or arrest can be caused by hypoxemia, MI, hyperkalemia, digitalis toxicity or toxic responses to BB and CCB |
|
|
Atrial/Nodal Premature Beats (APBs)
|
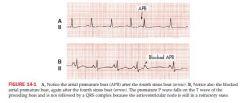
Results from ectopic stimuli; somewhere in the R or L atrium but not SA node
QRS complex is not affected by APBs or JPBs Atrial depolarization is premature, occurring before the next normal P wave The P wave of the QRS complex that follows the APB is different from the other P waves; the Pr interval is also shorter or longer then the other PR intervals (the P wave may be buried in the T wave of the preceding beat After the APB, a slight pause occurs before normal sinus beat resumes QRS complex of the APB is identical to the other QRS Occasionaly APBs result in aberrant ventricular conduction so QRS is wider than normal A blocked APB shows a premature P wave not followed by a QRS complex |
|
|
Atrial Bigeminy
|
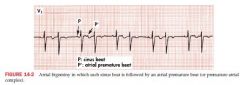
a sinus beat followed by an APB
|
|
|
Clinical Significance of APBs
|
very common
may be seen with emotional stress, excessive intake of caffeine, o admin of epi or theophylline May also occur with hyperthyroidism, caffeine May produce palpiations May lead to aFib* |
|
|
Paroxysmal Supraventricular Tachycardias (PSVTs)
|
a sudden run of three or more premature supraventricular beats
Episodes may be brief and nonsustained, or can last up to minutes or hours The three major types are atria tachy, atrio-ventricular nodal reentrant tachy, and AV reentrant tachy |
|
|
Atrial Tachycardia
|
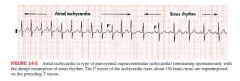
defined as three or more consecutive APBs
Most episodes involve an ectopic non sinus pacemaker located in either L or R atrium that fires automatically in a rapid way Atrial rate may be as high as 200 bpm or faster some p waves are neg in II, III, and aVF |
|
|
AV Nodal Reentrant Tachycardia (AVNRT)
|
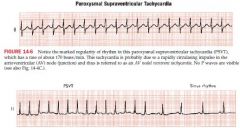
caused by a rapidly circulating impulse in AV node area
produces a very rapid and regular SV rhythm 140-250 bpm and are initiated by an APB P waves are hidden in narrow QRS complex May cease spontaenously A type of junctional rhythm |
|
|
Atrioventricular Reentrant Tachycardia
|
WPW syndrome associated (bypass tract)
may show p waves occurring visibly after QRS complexes in the ST segment |
|
|
AV Junctional rhythyms
|

AV junction functions as ectopic pacemaker
This retrograde stimulation of atria produces a postiive p wave in aVR and negative P wave in lead II Narrow QRS complexes P wave can occur before,or after the QRS complex, or simultaneously which shows no P wave |
|
|
AV Junctional escape rhythms
|
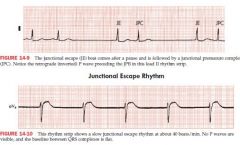
a beat that comes after a pause when normal sinus pacemaker fails to function
"a safety beat" HR is usually slow 30-50 bpm Seen in sick sinus syndrome, digitalis toxicity, excessive effects of BB or CCB, acute MI, hypoxemia, and hyperkalemia |
|
|
Atrial Flutter
|
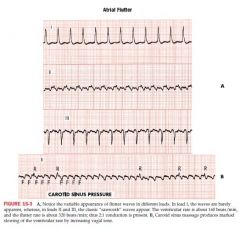
atrial rate is 250-350 bpm
example of reentrant arrhythmia originates in the RA traveling top to bottom to top atrial rate is 300/min and ventricular rate is about 150. 100, or 75/min sawtooth pattern occurs in pts with mitral disease, chronic ischemic heart disease, cardiomyopathy, HTN, acute MI, COPD,a nd PE May also occur after cardiac surgery May c/o of palpitations, light-headedness, or syncope |
|
|
Atrial Fibrillation
|
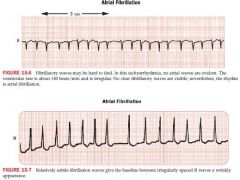
atria depolarization rate is between 350-600 cycles/min
irregular wavy baseline pattern in place of normal P waves ventricular rate is irregular, no p waves |
|
|
Ventricular premature beats (VPB)
|
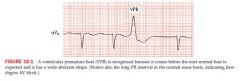
QRS complexes are wide
occur before the next normal beat is expected; precede a sinus P wave but before a normal QRS complex aberrant in appearance T wave and QRS complex point in opposite direction VPB may be followed by a nonsinus P wave (negative in lead II) |
|
|
Ventricular Tachycardia
|
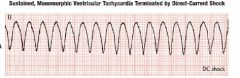
A run of three or more consecutive VPBs
may degenerate into VF causing immediate cardiac arrest |
|
|
Torsades De Pointes
|
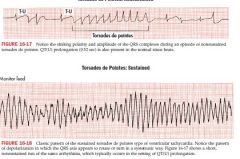
polymorphic Vtach
prolong QT, prominent U waves often initiated by a VPB caused by quinidine and other drugs |
|
|
Ventricular Fibrillation
|
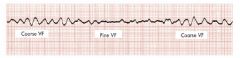
associ with cardiac arrest
|
|
|
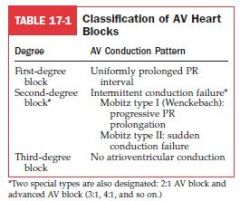
Heart Blocks
|
|
|
|
First degree AV block
|
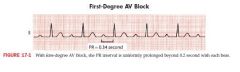
PR interval uniformly prolonged beyond 0.2 seconds with each beat
Causes: inferior MI, vagal stim, digitalis, amiodarone, BB, CCB, hyperkalemia |
|
|
Mobitz Type I Wenckbach 2nd degree AV block
|
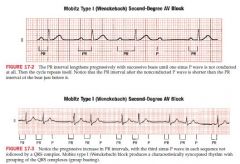
PR interval lengthens progressively with successive beats until one sinus p wave is not conducted
PR interval after non conducted p wave is shorter* than the one just before Cause: high AV node dysfunction (MI, digitalis, BB, CCB) |
|
|
Mobitz Type II 2nd degree AV block
|
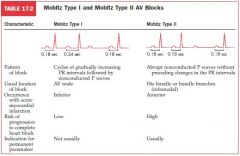
abrupt nonconducted P waves without preceding changes in PR intervals with sudden dropped QRS
deteriorates to 3rd degree quick;y |
|
|
Third degree Heart Block (complete)
|
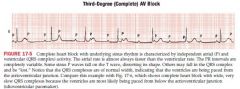
PR intervals completely variable with p waves bearing no relation to the QRS
atrial rate faster than ventricular rate |
|
|
Wandering Pacemaker
|
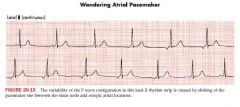
multiple p waves varying configuration with normal or slow HR
|
|
|
Wide QRS Complex Differentials
|
LBBB
RBBB Hyperkalemia Tricyclic antidepressants and phenothiazines Premature, escape ventricular beats WPW |
|
|
RAD Differentials
|
normal variant
acute PE or severe asthma COPD RVH lateral wall MI LPFB |
|
|
QT prolongation Differentials
|
Hypocalcemia****, Hypokalemia, Hypomagnesemia
Amiodarone, quinidine, sotalol phenothiazines, tricyclic antidepressants MI, CVA |
|
|
Q Waves Differentials
|
L pneumothorax
MI Hyperkalemia LVH RVH LBBB WPW COPD PE, PNA |
|
|
Tall R wave in V1
|
Posterior MI or lateral MI
RVH with RAD WPW |
|
|
ST Segment Elevations
|
transmural ischemia
Acute MI pericarditis LVH/LBBB Hyperkalemia |
|
|
ST depressions
|
acute subendo ischemia**
L or RVH LBBB, RBBB, WPW Digitalis**** Hypokalemia*** Strain |
|
|
Tall positive T waves
|
Hyperkalemia
CVA LVH LBBB pericarditis hyperacute phase of MI |
|
|
Prominent T wave Inversions
|
MI
CVA strain pattern secondary BBB and WPW pattern hypertrophy Digitalis, Epi electrolyte imbalnce pericarditis with PR interval depression Normal in kids, and V1 and V2 in adults |
|
|
Horizontal Axis 0
|

qR in I and aVL
rS in III and aVF |
|
|
Vertical Axis +90
|

qR in II, III, aVF
rS in I and aVL |
|
|
abnormal R wave progression
|
infarcts, hypertrophy, conduction disturbances
|
|
|
Strain
|
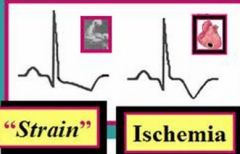
difference of >60 degrees of T waves from QRS
|
|
|
Ejection Fraction may decrease if
|
bulky d/t uncontrolled HTN
weak, d/t dilated cardiomyopathy scarred, secondary to MI valve failure |
|
|
Which of the following physical findings would you mist likely expect to be associated with the ECG dx of LAA or atrial fibrillation
|
Opening snap of mitral stenosis******
Carotid bruit Wheezing Renal Bruit Holosystolic murmur of PDA |
|
|
RVH + RBBB -->
|
often causes RAD and peaked p waves
|
|
|
LBBB suggestive of....
LBB + p mitrale = |
LVH
= dx of LVH |
|
|
RSR' variants in V1 and V2
|
occurs in 5% normal
pectus ASD RVH acute cor pulmonale WPW Duchenne dystrophy |
|
|
Dominant R in V1 and V2
|
true posterior or lateral MI
occasionally normal RVH WPW LV diastolic overload muscular subaortic stenosis Duchenne dystrophy |
|
|
Ischemia
Injury Infarction (NEW) Infarction (OLD) |
usually causes ST depression
usually causes ST-segment changes (elevation), hyperacute Ts and flipped T-waves ST-segment changes (elevation) and flipped T-waves followed by significant Q-waves usually has persistent Q-waves, ST-segment changes resolve (unless secondary MI) and flipped T-waves often resolve |
|
|
Troponin I and T, CPK-MB
|
Positive troponin T & I / CPK-MB) trump absent Q-waves and ambiguous ECG changes
•Must be interpreted according to the number of hours from the onset of chest pain. •Typically (+) after 3-4 hours. •When +, remains so for 1-2 weeks. •Typically rules-out AMI (-) after 8-10 hours after the onset of chest pain. •Normal <0.04 ng / mL at VAMC •Indeterminate 0.04 – 0.49 ng / mL at VAMC •Abnormal >0.49 ng / mL at VAMC. •In contrast, CPK-MB peaks 12-24h, resolves after 36-48h |
|
|
Inferior
Anteroseptal Anteroapical Anterolateral Posterior |
Right coronary
Left anterior descending Left anterior descending (distal) Circumflex Right coronary artery (distal) |
|
|
Electrical dysfunctions that commonly cause mortality in the first 72 hours include:
|
tachycardia that reduces CO and lowers BP
2nd degree mobitz II block complete 3rd degree block Vtach VFib |
|
|
five clinical characteristics predict 90% of mortality in pts who present with STEMI
|
older age
lower systolic BP Killip Class > 1 (LV failure, pulm edema, shock) Tachyarrhythmias anterior location |