Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
169 Cards in this Set
- Front
- Back

Label the Circle of Willis
|
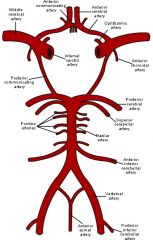
see above, also pg 170
|
|
Label the Circle of Willis, intracranial view
|
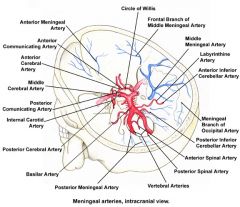
see above, also pg 170
|
|
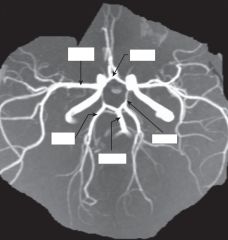
Magnetic resonance arteriography illustrating the circle of Willis and its branches
|
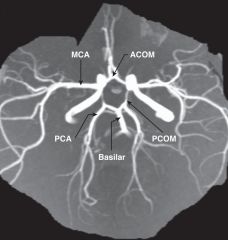
see labels above
|
|

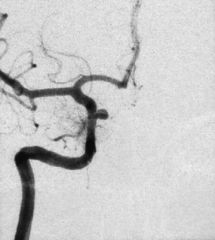
What do you see?
|
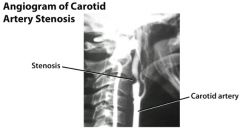
Lateral common carotid arteriogram in a patient with a neck bruit. Note the focal narrowing of the proximal internal carotid artery (arrow). In severe cases, the kink may require carotid artery reconstruction.
DIT says that you need to be able to recognize a stenosis vs aneurysm |
|
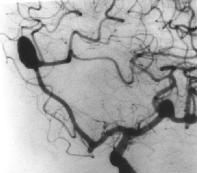
What do you see?
|
Left oblique cerebral angiogram in a patient with multiple intracranial aneurysms shows an anterior communicating aneurysm and a middle cerebral artery aneurysm. The patient underwent a frontotemporoparietal craniotomy, during which surgical clips were placed in both lesions in one setting.
DIT says that you need to be able to recognize the difference btw an aneurysm and arterial stenosis on an angiogram |
|
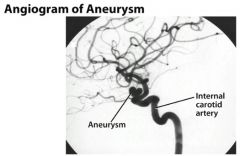
what do you see?
|
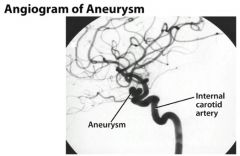
(from Medscape): Left oblique cerebral angiogram in a patient with a proximal intracranial internal carotid artery aneurysm. The surgical approach to this aneurysm requires a craniotomy with an orbitotomy and drilling of the anterior clinoid process; however, this aneurysm has a favorable neck-to-fundus ratio for endovascular coil placement.
DIT says that you need to be able to recognize the difference btw aneurysm & stenosis on angiogram imaging |
|

A 49yo, presents with sudden onset of vertigo, nausea, vomiting, dysphagia, hoarseness, and nystagmus in addition to ipsilateral Horner syndrome, limb ataxia, and impairment of all sensory modalities over the face. There is also impairment of pinprick and temperature appreciation in the contralateral limbs.
|

This case illustrates the development of the lateral medullary syndrome (Wallenberg's syndrome) as a result of occlusion of the posterior inferior cerebellar artery (PICA).
-Loss of pain & temp over contralateral body -Loss of pain & temp over ipsilateral face -Cerebellar defects - Involvement of the sympathetic pathways may lead to Horner's syndrome - Vertigo results from involvement of the vestibular nuclei and hemiataxia from involvement of the inferior cerebellar peduncle. |
|
|
What viruses preferentially infect the ventral horn of spinal cord, leading to a flaccid paralysis?
|
polio & west nile
|
|
|
Which spinal tract carries touch, vibration, and pressure sensation?
|
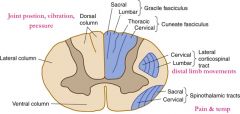
Dorsal columns:
Fasciculus gracilis & cuneatus |
|
|
Which spinal tract carries voluntary motor commands from motor cortex to body?
|

Lateral & ventral corticospinal tracts
|
|
|
Which spinal tract carries voluntary motor commands from motor cortex to head/neck?
|
Corticobulbar tract
|
|
|
Which spinal tract carries pain & temp sensation?
|
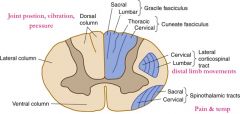
Lateral spinothalamic tract
|
|
|
Which spinal tract is important for postural adjustments & head mvmts?
|

Vestibulospinal tract
|
|
|
Which CN is responsible for Eyelid opening?
How do you differentiate between benign & serious cause of deficit of this nerve? |
CN 3 (oculomoter)
Benign cause (ie HTN or Diabetes) of CNIII palsy - the pupil will be normal in size & reactive - no treatment is needed Serious causes (ie aneurysm, tumor, or uncal herniation) - pupil will be dilated & nonreactive ("blown") - urgent CT/MRI is needed |
|
|
Which CN is responsible for
Taste from ant 2/3 of tongue? What other sxs would you look for to distinguish whether the damage to this nerve was UMN or LMN? |
CN 7 (Facial)
UMN lesion of Facial nerve = forehead is spared on the affected side, cause is usually stroke or tumor LMN lesion of Facial nerve = forehead is involved, and cause is usually Bell's palsy or tumor |
|
|
Which CN is responsible for
Head turning? How do you know which side the lesion is located? |
CN 11 (spinal accessory)
Patients with CN 11 lesions have trouble turning their head to the side OPPOSITE the lesion & have ipsilateral shoulder droop (due to loss of innervation to SCM & trapezius) |
|
|
Which CN is responsible for
Tongue movement? How do you know which side the lesion is located? |
CN 12 (hypoglossal)
protruded tongue will deviate to the SAME side of the lesion |
|
|
Which CN is responsible for
Muscles of Mastication? What pathological condition of this nerve is provoked by chewing? |
CN 5 (trigeminal) - also innervates facial sensation
Trigeminal Neuralgia ("Tic doulourex") = unilateral shooting pains in the face & often triggered by chewing, brushing the teeth - tx with Carbamazepine |
|
|
Which CN is responsible for balance?
Kids with balance probs - likely cause is? Adults with balance probs - likely cause? |
CN 8 (Vestibulocochlear) - needed for hearing & balance
Lesions of CN 8 can cause deafness, tinnitus, and/or vertigo - in kids, think of meningitis as a cause in adults - think of medications (aspirin, aminoglycosides, loop diuretics, cisplatin), infection (labyrinthitis, tumor, or stroke |
|
|
Which CN is responsible for monitoring carotid body & sinus chemoreceptors & baroreceptors?
|
CN 9 (glossopharyngeal)
|
|
|
What are the 2 most common locations of aneurysms in the Circle of Willis?
|
Anterior communicating artery
Posterior communicating artery |
|
|
Where is the brain lesion if pt presents with:
contralateral hemiballismus |

subthalamic nucleus
|
|
|
Where is the brain lesion if pt presents with:
eyes look toward the side of the lesion |
frontal eye fields (Prefrontal cortex)
|
|
|
Where is the brain lesion if pt presents with:
eyes looking away from the side of the lesion |
PPRF
|
|
|
Where is the brain lesion if pt presents with:
paralysis of upward gaze |
Superior colliculi (Parinaud syndrome)
Also known as dorsal midbrain syndrome, this is a distinct supranuclear vertical gaze disorder caused by damage to the posterior commissure. It is a classic sign of hydrocephalus from aqueductal stenosis. Pineal region tumors, cysticercosis, and stroke also cause Parinaud's syndrome. Features include loss of upgaze (and sometimes downgaze), convergence-retraction nystagmus on attempted upgaze, downward ocular deviation ("setting sun" sign), lid retraction (Collier's sign), skew deviation, pseudoabducens palsy, and light-near dissociation of the pupils. |
|
|
Where is the brain lesion if pt presents with:
hemispatial neglect syndrome |
non-dominant parietal lobe
|
|
|
Where is the brain lesion if pt presents with:
coma |
reticular activating system (RAS) - in the ventral pons
likely a/w Basilar Artery occlusion |
|
|
Where is the brain lesion if pt presents with:
poor repetition |
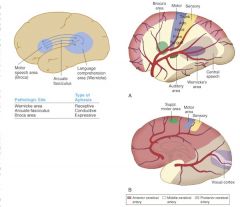
arcuate fasciculus
|
|
|
Where is the brain lesion if pt presents with:
poor comprehension |
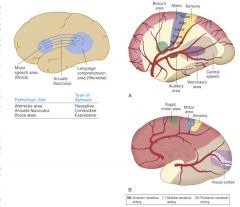
Wernicke's area
|
|
|
Where is the brain lesion if pt presents with:
poor vocal expression |
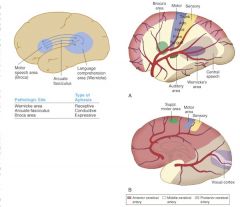
Broca's area
|
|
|
Where is the brain lesion if pt presents with:
resting tremor - think of the classic "pill rolling" tremor that disappears with movement or sleep What conditions cause a resting tremor? |

basal ganglia (↓ dopamine)- think Parkinson's Disease
Other conditions other than Parkinson's disease that can cause resting tremors: - hyperthyroidism, anxiety - tx with Beta blockers - Drug withdrawal or intoxication (MPTP found in designer drugs) Or Antipsychotics used to treat Schizophrenia - treat this side-effect with anticholinergics (benztropine, trihexyphenidyl) or antihistamines (diphenhydramine) - benign hereditary tremor - usually Aut Dom (look for fam hx) Also beware of: Wilson's disease (hepatolenticular degeneration) - causes chore-like movements Liver failure - causes asterixis (slow, involuntary flapping of outstretched hands |
|
|
Where is the brain lesion if pt presents with:
intention tremor |
cerebellar hemisphere
this is why alcoholics will have INTENTION tremors |
|
|
Where is the brain lesion if pt presents with:
hypororality, hypersexuality, disinhibited behavior |
bilateral amygdala (Kluver-Bucy)
|
|
|
Where is the brain lesion if pt presents with:
Personality changes - apathy, inattention, disinhibition, labile affect |
frontal lobe
|
|
|
Where is the brain lesion if pt presents with:
dysarthria (trouble articulating words - slurred speech) |
cerebellar vermis - this is why alcoholics have slurred speech
|
|
|
Where is the brain lesion if pt presents with:
agraphia & acalculia inability to read, write, name or do math |
dominant (left) parietal lobe
|
|
|
Where do the dorsal columns decussate?
|

medulla
recall the dorsal columns carry touch, vibration, pressure sensation |
|
|
where does the lateral corticospinal tract decussate?
|
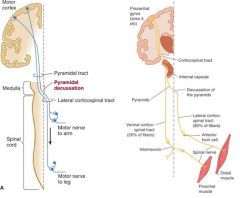
medullary pyramids
|
|
|
Where does the spinothalamic tract decussate (crossover)?
|
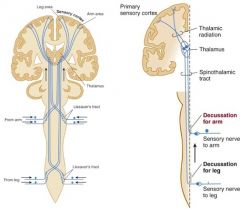
Anterior white commissure at the spinal cord level
spinothalamic carries pain & temperature sensation correlation: syringomyelia, in which there is central cavitation of the spinal cord (usually in cervical or upper thoracic region) presents with loss of pain & temp sensation in a "cape" distribution b/c damage to the lateral spinothalamic tracts MRI is best test to diagnose, tx with surgical creation of a shunt |
|
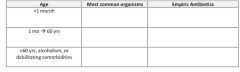
fill out this chart - 4star topic!!
what are the common organisms and empiric IV antibiotic choices for bacterial meningitis based on age of the patient? |

see above
|
|
|
What is the rational for dosing dexamethasone prior to or along with the first dose of antibiotics for empiric treatment of bacterial meningitis?
|
Dexamethasone when given with or prior to the first dose of antibiotic reduces the risk of neurologic sequelae (ie hearing loss) in children with meningitis, esp in the cases of H. influenza Type B or Tuberculosis (TB) meningitis
In adults with bacterial mengingitis, dexamethasone reduces both morbidity and mortality esp in the case of pneumococcal meningitis |
|
|
Do you always need to get a CT scan (prior to an LP) if you suspect meningitis?
|
No – you do not have to get a CT scan in a patient you suspect of having meningitis
|
|
|
In which situations do you need to get a CT scan prior to an LP?
|
Focal neurologic defects
Papilledema Pupil asymmetry Suspect hematoma Suspect brain tumor |
|
|
What is the treatment for viral meningitis?
|
Acetominophen for pain
IV fluids as needed Empiric antibiotics until bacterial meningitis can be excluded if younger than 3 yrs, severely ill, or immunocompromised, continue empiric antibiotics until bacterial culture results confirm nonbacterial etiology *** Give empiric Acyclovir if suspicion of HSV or signs of encephalitis such as focal neurologic findings d/c if HSV PCR and cultures are negative or alternative diagnosis is made |
|
|
An infant is brought to the ER. The parents say that over the last day the infant has developed a fever, refused to eat, vomited, and is lethargic. The PE reveals petechiae and confirms the fever. WBC is elevated, and CSF results show a ↓ glucose and ↑ neutrophils. On which medications should this patient be started?
|
Cover: E. coli, Listeria, Group B Strep (GBS)
Tx: Ampicillin + cefotaxime Ampicillin + gentamicin |
|
|
What other drug should be given just before or along with the first dose of antibiotics in a pt suspected of having bacterial meningitis?
|
Dexamethasone
|
|
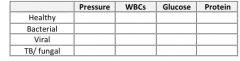
Fill in the table of CSF findings in cases of meningitis caused by different types of pathogens:
|
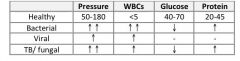
Think: Bacterial eat sugar, viruses increase protein a little but noting else, TB/fungis same as bacteria
|
|
|
When should a CT scan be performed as a next step instead of an LP in a pt suspected of having meningitis?
|
When there are signs of ↑ ICP or other comorbidity
Focal neurologic defect Papilledema Focal seizure Suspicion of mass effect Soft tissue infection at site of LP Bleeding diathesis Cardiopulmonary instability |
|
|
You suspect an AIDS pt may have meningitis. What specific CSF preparation should be ordered in addition to the usual CSF analysis, gram stain, and culture?
|
India Ink stain to look for Cryptococcus meningitis
|
|
|
When would you suspect West Nile Viral infection? How would you make the dx? what's the tx?
|
Birds are the resevoir, and mosquitoes are the vectors. Human, horses, and dogs are incidental hosts
S/S: usually only headache, malaise, back pain, myalgia, and anorexia for 3-6 days (“flu like”) Severe S/S in 1/150: meningitis +/- encephalitis including muscle weakness and flaccid paralysis (via anterior-horn involvement), alteration in consciousness, possibly death Dx: serology – check for IgM Abs against West Nile Virus Tx: supportive |
|
|
What is the treatment for Reye's syndrome?
|
d/c salicyclate (ie Aspirin)
Hospitalization (usually ICU) for cardiorespiratory monitoring (+/- mechanical ventilation), supportive care, fluid & electrolyte management Maintain euglycemia: accuchecks, IV dextrose or insulin as needed Maintain isovolemia: IVF or Lasix as needed, Foley catheter for strict I/Os Reduce brain swelling: avoid hypo-osmotic fluids, elevate head of bed, +/- corticosteroids, +/- ICP monitor If seizures: phenytoin |
|
|
How should you treat a pt that has been bitten by an animal suspected of having rabies, or an animal that cannot be observed for 10 days?
|
Clean the wound with iodine
Administer rabies immunoglobulin & rabies vaccine Tetanus prophylaxis |
|
|
A pt is brought into the ED with progressive muscle weakness, intact sensation, headache, vomiting, neck pain, and fever. CSF analysis shows ↑ lymphocytes and normal glucose and protein. What life-threatening complication can result in this disease process?
|
Dx: Polio (muscle weakness is key to dx)
Complication: respiratory muscle paralysis |
|
|
What other term should you remember when considering Reye’s syndrome?
|
Hepatoencephalitis
|
|
|
A pt is recovering in the ICU after suffering a subdural hematoma that occurred b/c of a MVC. The neurosurgery team performed a craniotomy and drain placement to evacuate the clot. For the past few days the drainage in the collection bulb was serous. Now however, the drainage is thick and yellow. Along with this, the pt’s neurological exam has deteriorated. What is the likely cause of this clinical picture?
|
Dx: abscess within subdural space
Likely etiology: Staph aureus Tx: cover for MRSA, gram (+) and Gram negs with Vancomycin and Ceftazidime |
|
|
What are the differences in the acute treatment of tension headaches, cluster headaches, and migraine headaches?
|
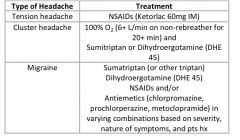
see above
|
|
|
What agents can be used for prophylaxis of migraine headaches?
|
Ca2+ channel blockers: verapamil (often first-line b/c safe and well tolerated)
β-blockers: propanolol, metoprolol (good choice if comorbid HTN) Tricyclic antidepressants (TCA): amitriptyline, nortriptyline (good choice if comorbid depression, incsomnia, pain syndrome) Note – nortriptyline has fewer side effects NSAIDs: naproxen (good choice if menstrual migraine or comorbid osteoarthritis or other pain that could benefit from NSAIDs) Anticonvulsants: valproic acid (good if h/o Bipolar disorder), topiramate, gabapentin |
|
|
What is the most likely cause of a pt's headache if:
Made worse by foods containing tyramine |
migraine
|
|
|
What is the most likely cause of a pt's headache if:
Obese female with papilledema |
pseudotumor cerebri
|
|
|
What is the most likely cause of a pt's headache if:
Jaw muscle pain when chewing |
Giant cell (temporal) arteritis
|
|

What is the most likely cause of a pt's headache if:
Periorbital pain with ptosis and miosis |
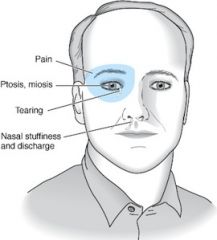
cluster headache
|
|
|
What is the most likely cause of a pt's headache if:
Photophobia, Phonophobia |
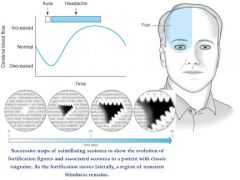
migraine
|
|
|
What is the most likely cause of a pt's headache if:
Bilateral frontal/ occipital pressure |
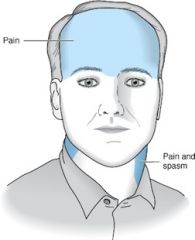
tension headache
|
|
|
What is the most likely cause of a pt's headache if:
Lacrimation and/or rhinorrhea |
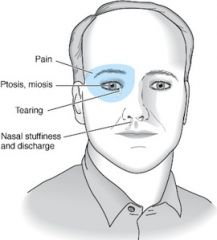
cluster headache
|
|
|
What is the most likely cause of a pt's headache if:
Elevated ESR |
Giant cell (temporal) arteritis
|
|
|
What is the most likely cause of a pt's headache if pt states:
“Worst headache of my life” |
Subarachnoid hemorrhage
|
|
|
What is the most likely cause of a pt's headache if:
Headache + extraocular muscle palsies |
Cavernous sinus thrombosis
|
|
|
What is the most likely cause of a pt's headache if:
Scintillating scotomas prior to headache |
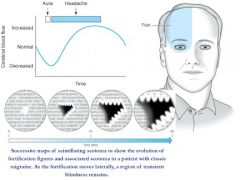
Migraine with aura
|
|
|
What is the most likely cause of a pt's headache if:
Headache occurring either before or after orgasm |
Post-coital cephalgia
|
|
|
What is the most likely cause of a pt's headache if:
Responsive to 100% Oxygen supplementation |
cluster headache
|
|
|
What is the most likely cause of a pt's headache if:
Trauma to the head → headache begins days after the event, persists for over a week and does not go away |
Subdural hematoma
|
|
|
What headache symptoms would lead you to suspect a brain tumor as a cause of a headache?
|
mild headache which progressively worsens over days to weeks
new onset after age 50 Papilledema: worsened by a bending, lifting, cough, or Valsalva maneuver (= ↑ in ICP) Associated seizures, confusion, altered mental status (AMS) Abnormal neurologic signs and symptoms (ie focal numbness or weakness) Disturbs sleep or present immediately upon awakening Vomiting precedes headache Known systemic illness (ie cancer, HIV, or collagen-vascular disorder) |
|
|
What are the characteristic features of pseudotumor cerebri?
|
Young, obese female
Headaches – daily (worse in the morning), pulsatile, possible nausea/vomiting, possible retroocular pain worsened by eye movement Papilledema Most worrisome sequela is vision loss CT Scan: (normal) no ventricular dilation, no mass CSF pressure elevated > 200 mmH2O in non-obese, >250 in obese pt) |
|
|
What treatment options are available for managing pseudotumor cerebri?
|
Confirm absence of other pathology with CT and MRI of the head (r/o central venous thrombosis)
d/c any inciting agents (ie Vit A excess, tetracyclines, withdrawal from corticosteroids) Weight loss in obese pts Acetozolamide – first line (start 250mg qid or 00mg bid → increase to 500mg qid to 1000mg qid) Invasive treament options: Serial lumbar punctures Optic nerve sheath decompression Lumboperitoneal shunting (CSF shunt) |
|
|
A 25 yo M is seen in the ER with a severe headache. He tells you that the headache always occurs at around the same time of day, and that the pain is localized around the right eye. On exam his pupils are unequal and his right eye is tearing. While he waits for a CT scan of the head, what treatment should he receive?
|
Dx: cluster headache
Tx: 100% O2, Sumitriptan or IV ergotamines |
|
|
30 yo F is in the office with a complaint of facial pain. She describes that whenever her face is lightly touches that she experiences incredible electricity-like pain. What is the 1st line therapy for this condition?
|
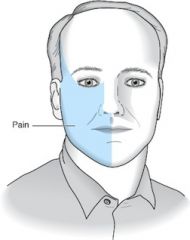
Dx: Trigeminal neuralgia
Tx: Carbamazepine or Baclofen |
|
|
27 yo M comes to the clinic b/c of progressively worsening headache. He denies a prior h/o headaches. He adds that this one was easy to ignore at first, but over the last few weeks has never let up and is increasing in severity. What should be next for this pt?
|
next step: MRI of brain (if it’s getting worse, be worried!)
|
|
|
What are the demographic characteristics of a typical pseudotumor cerebri patient?
|
obese female in 20's-30's
|
|
|
A pt with longstanding poorly-controlled diabetes has tension headaches. What should you check before recommending pharmacologic treatment?
|
Kidney function (Creatinine, BUN, GFR) – because NSAIDs are treatment for Tension Headaches
|
|
|
Which spinal cord lesion matches the following description?
Fasciculations but also spastic paralysis |
ALS
|
|
|
Which spinal cord lesion matches the following description?
Impaired proprioception + pupils do not react to light |
Syphilis (Tabes Dorsalis & Argyll Robinson pupils)
|
|
|
Which spinal cord lesion matches the following description?
Bilateral loss of pain and temp below lesion + hand weakness |

Syringomyelia
|
|
|
Which spinal cord lesion matches the following description?
Bilateral loss of vibration sense + spastic paralysis of legs then arms |
Vit B12 Deficiency
|
|
|
Which spinal cord lesion matches the following description?
Bilateral loss of pain/temp below lesion + bilateral spastic paralysis below lesion + bilateral flaccid paralysis at level of lesion |

Occlusion of Anterior Spinal Artery
|
|
|
What are the characteristic features of Brown-Sequard syndrome?
|
Ipsilateral vibration & discrimination below lesion
Ipsilateral spastic paralysis (below lesion) Ipsilateral flaccid paralysis (level of lesion) Contralateral pain & temp (below lesion) |
|
|
HYQ: most likely cause of headache in a 40yo woman with frontal headache that is made worse by bending over?
|
Sinus headache
|
|
|
HYQ: What would be the preferred antihypertensive in a pt with chronic hypertension and recurrent migraines?
|
β-blockers or Ca2+ channel blockers
|
|
|
HYQ: What medication should be given to close contacts of those with either meningococcal or HIB meningitis?
|
Rifampin or Ciprofloxacin
|
|
|
HYQ: What are the four most common sequelae of meningitis in children?
|
Hearing loss
Mental retardation Seizure disorder Spastic paralysis |
|
|
What is the treatment for fungal meningitis?
|
Amphotericin B
|
|
|
What medications are used in combination in the treatment of TB meningitis?
|
RIPE – Rifampin, Isoniazid, Pyrazinamide, Ethambutol
|
|
|
What cerebral artery infarct can cause aphasia?
|
MCA infarction
|
|
|
What organism is responsible for bacterial meningitis given the following findings on CSF examination?
Gram (+) diplococci |
Streptococcus pneumoniae
|
|
|
What organism is responsible for bacterial meningitis given the following findings on CSF examination?
Gram neg diplococci |
Neisseria meningitis
|
|
|
What organism is responsible for bacterial meningitis given the following findings on CSF examination?
Small pleomorphic gram neg coccobacilli |
Haemophilus influenza
|
|
|
What organism is responsible for bacterial meningitis given the following findings on CSF examination?
Gram (+) rods and coccobacilli |
Listeria
|
|
|
What is the anticoagulant of choice in a pt with a h/o stroke or TIA?
|
First TIA ➔ Aspirin
TIA/stroke due to Atrial Fibrillation ➔ Warfarin TIA/Stroke + coronary artery disease ➔ Clopidogrel (Plavix) Repeat TIA/stroke while on aspirin ➔ Clopidogrel (Plavix) |
|
|
What are the classic signs and symptoms of carotid artery stenosis?
|
Carotid bruit
Transient ischemic attacks (TIAs) Reversible ischemic neurologic deficits lasting up to 3 days Amaurosis fugax (transient unilateral blindness) Cerebrovascular accidents (CVAs) (Vertigo & Syncope are NOT caused by carotid artery stenosis) |
|
|
What are the surgical indications for carotid endarterectomy?
|
Symptomatic carotid stenosis 70-99%: strong benefit
Symptomatic carotid stenosis 50-69%: marginal benefit (more benefit in men and if performed w/in 2 wks of stroke/TIA) Asymptomatic pts with 80-99% stenosis who are expected to live longer than 5 yrs by a surgeon with a perioperative complication rate of less than 3% (some books will mention a blanket >60% and asymptomatic rule, but this varies by surgeon and patient) |
|
|
What are the important nonsurgical treatments for carotid artery stenosis?
|
HTN control to < 140/90
Dyslipidemia control to LDL < 100mg/dL, HDL >35, TGs <200 Lipid control with statin reduces stroke while other lipid lowering drugs do not Niacin reduces carotid artery intima thickness ADA diet DM control to fasting glucose <126 and HgA1c <7% Smoking avoidance, consider varenicline (Chantix) ↑ physical activity to at least 30-60 minutes 4x weekly alcohol consumption up to 2 drinks daily is beneficial. Avoidance of heavy drinking Evaluation for CAD and PAD Aspirin Anticoagulation if history of TIA/stroke while on aspirin → use Aggrenox or clopidogrel instead |
|
|
What are some major signs and symptoms of a TIA?
|
Amaurosis fugax (brief unilateral blindness)
Weakness Slurred speech Impaired coordination Impaired sensation/ paresthesias |
|
|
What anticoagulant would you give a pt who has just had their first TIA? What if the pt had another TIA while on ASA, what would you add?
|
First TIA: Aspirin
Second TIA, while on Aspirin: add Clopidogrel (Plavix) or combination of Aspirin + dipyridamole |
|
|
What is the maximum amt of time a TIA may last?
|
24 hrs or less
|
|
|
What medication should be taken by a pt with atherosclerotic disease and risk of stroke?
|
Statin & Aspirin
|
|
|
What are the indications for carotid endarterectomy?
|
Asymptomatic men with narrowing of 80-99%
Symptomatic men with narrowing of 50-69% Symptomatic women with narrowing of 70-99% |
|
|
What are the 5 main lacunar syndromes that may arise from a lacunar infarct?
|
1) Pure motor hemiparesis: (most common, about 50% of lacunar strokes) – weakness of the face, arm, and leg on one side of the body + absent sensory or cortical signs (aphasia, neglect, apraxia, hemianopsia)
2) Pure sensory: sensory defect (numbness) of the face, arm, and leg on one side of the body + absent motor or cortical signs 3) Ataxic hemiparesis: ipsilateral weakness and limb ataxia out of proportion to the motor defect, possible gait deviation to the affected side + absent cortical signs 4) Sensory motor stroke: weakness and numbness of the face, arm, and leg on one side of the body + absent cortical signs 5) Dysarthria – Clumsy Hand Syndrome: (least common) – facial weakness, dysarthria, dysphagia, and slight weakness and clumsiness of one hand + absent sensory or cortical signs |
|
|
A stroke, by definition, must last how long?
|
> 24 hrs
|
|
|
What thrombolytics are used in the treatment of an acute ischemic stroke?
|
tPA, streptokinase (streptase)
|
|
|
What long-term medications should be started within 2-3 days of ischemic stroke?
|
Antiplatelet (aspirin) + statin
|
|
|
What would be the most likely initial imaging for a pt suspected to have a stroke?
|
Noncontrast CT scan
then, If the above study did not yield useful information, then what study might you get? MRI of the head |
|
|
What is the next step in management of a pt with ischemic stroke symptoms after a hemorrhagic stroke has been ruled out by noncontrast CT?
|
Thrombolytic therapy
|
|
|
To maintain cerebral perfusion during the acute treatment of ischemic stroke, hypertension is generally not actively treated. At what blood pressure does treatment become necessary?
|
BP > 220/120
|
|
|
Hemorrhagic stroke requires the following treatment:
|
Reversal of any anticoagulation
Control of intracranial pressure (ICP) Control of blood pressure Surgical decompression may be needed |
|
|
What is the treatment for a subarachnoid hemorrhage?
|
d/c all anticoagulants and reverse and anticoagulation
systolic BP < 150 only if cognitive function is intact (adequate cerebral perfusion pressure) until the aneursm is clipped or coiled to prevent rebleeding. If the cerebral perfusion pressure is not adequate then lowering the BP will increase the risk of infarction Labetalol preferred Avoid Nitroprusside & Nitroglycerin which can ↑ ICP Nimodipine (a CCB) to prevent vasospasm Prevent physiologic derangements that may worsen brain injury Avoid hypoxia and hyperglycemia Maintain a normal pH, euvolemia, and normothermia (Phenytoin for seizure prophylaxis is controversial and generally avoided due to poorer outcomes) Ventriculostomy to monitor ICP in select patients Surgical clipping or metal coil into aneurysm |
|
|
Are patients with parenchymal hemorrhage at an increased risk of seizures?
|
yes
|
|
|
In which scenario is seizure prophylaxis with anticonvulsants recommended? Parenchymal hemorrhage or subarachnoid hemorrhage (SAH)?
|
Parenchymal → always start prophylaxis
SAH → only if seizures develop |
|
|
How can AVMs and/or aneurysms be treated?
|
Coil or clip
|
|
|
What diseases are associated with berry aneurysms?
|
Polycystic Kidney Disease
Marfan’s Syndrome |
|
|
What are 3 feared complications of parenchymal hemorrhage?
|
Uncal herniation
CSF flow obstruction Death |
|
|
How may a pt describe the symptom of a subarachnoid hemorrhage?
|
"worst headache of my life"
|
|
|
What 2 studies must be performed to rule out SAH?
|
Noncontrast CT scan of the head
Lumbar puncture |
|
|
How does one differentiate between SAH and a traumatic LP as a cause of bloody CSF?
|
collect several tubes of CSF, if blood decreases then more likely due to traumatic LP than SAH
|
|
|
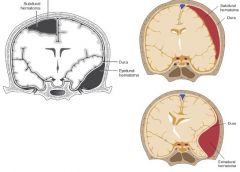
What are the most common causes of an epidural hematoma and subdural hematoma?
|
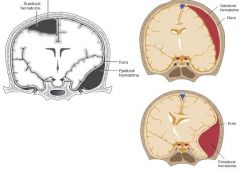
Epidural hematoma: rupture of middle meningeal artery
Subdural hematoma: rupture of bridging veins |
|
|
Commonly a pt with an epidural hematoma will have the typical three part history of:
|
(1) head trauma with brief LOC
(2) Lucid interval (3) Deterioration (expansion of epidural hematoma) |
|
|
What is the definitive treatment of an epidural hematoma?
|
Evacuation of hematoma
|
|
|
Where is the bleeding in a subdural hematoma? What shape would be expected on a head CT of a pt with subdural hematoma?
|
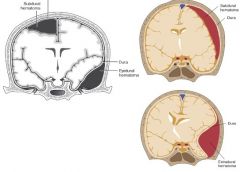
Bleeding is btw dura & arachnoid
Classic finding: crescent shape on CT scan |
|
|
If you suspect a pt has an epidural or subdural hematoma, should you perform a LP to confirm the diagnosis?
|
NO! can ↑ risk of brain herniation
|
|
|
Describe the differences between Broca’s aphasia and Wernicke’s aphasia?
|
Broca’s: expressive
Wernicke’s: receptive |
|
|
What are the three Ws that help diagnose normal pressure hydrocephalus?
|
Wacky – cognitive impairment
Wet – incontinence Wobbly – gait disturbance |
|
|
Which medications or medication withdrawal are known for causing seizures?
|
Medications that ↓ seizure threshold:
Buproprione Buspirone Enflurane Medication withdrawals that can cause seizures: Barbiturates Alcohol Anticonvulsants Benzodiazepines - choose the short acting (Alprazolam, Lorazepam) if given more than one to choose from |
|
|
What medications are used for prevention of grand mal (tonic-clonic) seizures?
|
Valproate, carbamazepine, phenytoin, lamotrigine, topiramate
|
|
|
What medications are used for prevention of partial seizures?
|
(same as prevention of grand mal seizures)
Carbamazepine, Phenytoin, Lamotrigine > Valproate, Topiramate |
|
|
What medications are used for prevention of absence seizures?
|
Ethosuximide
|
|
|
What seizure medications are used for prevention of myoclonic seizures?
|
Valproic Acid
|
|
|
Which seizure medication matches the following description?
Gingival hyperplasia |
phenytoin (Dilantin)
|
|
|
Which seizure medication matches the following description?
DOC for absence seizures |
Ethosuximide (Zarontin)
|
|
|
Which seizure medication matches the following description?
2nd choice for absence seizures |
Valproic Acid (Depakene)
|
|
|
Which seizure medication matches the following description?
DOC for Trigeminal Neuralgia |
carbamazepine
|
|
|
Which drugs are known for causing Stevens-Johnson syndrome?
|
“sulfa, -cillin & seizure”
most commonly lamotrigine (lamictal) |
|
|
Which drugs are known for inducing the cytochrome P450 system thereby speeding up the metabolism of other drugs such as OCPs and warfarin?
|
“BCG PQRS”
Barbiturates Carbamazepine Griseofulvin Phenytoin Quinidine Rifampin St John’s Wort |
|
|
what is Arnold-Chiari Malformation?
|
Downward displacement of the cerebellar tonsils and medulla thru the foramen magnum
Type I is the most common type and is often asymptomatic. Manifestations may include headaches and/or cerebellar symptoms Type II (of IV severity) is usually accompanied by other neurologic anomalies |
|
|
What other neurologic anomalies are associated with an Arnold-Chiari malformation?
|
Hydrocephalus
Syringomyelia Myelomeningocele |
|
|
What are some of the possible presenting features of cerebral palsy?
|
Spastic features: spastic paresis of any or all limbs, clonus present
Athetosis features: slow, writhing movements in distal muscles Chorea features: rapid, irregular, unpredictable contractions of muscles in face or extremities Dystonic features: uncontrollable jerking, writhing, or posturing Infants have persistence of primitive reflexes, involuntary grimacing, tendency to drool, and delayed psychomotor development Ataxia: difficulty coordinating purposeful movements Atonic features: severe hypotonia present at birth with no future ability to stand or walk Neonates: may show signs of encephalopathy including lethargy, ↓ spontaneous movement, hypotonia, and suppressed primitive reflexes Associated disorders: mental retardation, epilepsy, sensory impairment (speech, hearing, vision) |
|
|
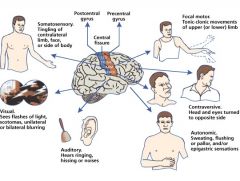
What type of seizure fits each description?
Focal sensory or motor deficit with no loss of consciousness |
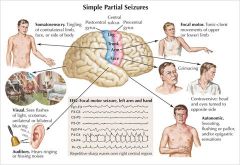
simple partial
|
|
|
What type of seizure fits each description?
Focal sensory or motor deficit, with impaired consciousness (commonly localized to temporal lobe on EEG) |
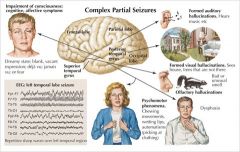
Complex partial
|
|
What type of seizure fits each description?
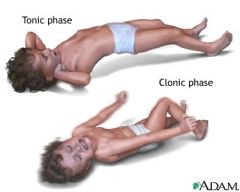
Involves both hemispheres of brain with a pattern of neuromuscular activation: tonic, clonic, toni-clonic, myoclonic, or atonic. Loss of consciousness present with postictal period |
Generalized
|
|
|
What type of seizure fits each description?
Characterized by a brief (few second) impairment of consciousness often with automatisms such as blinking or picking at shirt. No postictal period. Spike and wave pattern on EEG |
Absence
|
|
|
What is status epilepticus?
|
Uninterrupted seizure > 20min
|
|
|
What is the initial treatment for a pt in status epilepticus?
|
Monitor ABCs
|
|
|
Once ABCs are under control, what is the treatment for a pt in status epilepticus?
|
IV Benzos - Lorazepam
|
|
|
What is the DOC for absence seizures?
|
Ethosuximide
|
|
|
A 45yo M is brought to the ER for new-onset status epilepticus. What are some of the components of the workup to determine epilepsy?
|
Hx & PE (ask about trauma, drugs, illness)
CBC Fasting blood glucose BMP & LFTs Toxic drug screen CT head (if not actively seizing… ) LP for CSF infection (r/o meningitis) |
|
|
How long must a focal neurologic deficit last to qualify as a stroke?
|
> 24 hrs
|
|
|
In what timeframe must thrombolytic therapy be instituted in cases of ischemic stroke?
|
Within 3 hrs
|
|
|
HYQ: What is the treatment for an epidural hematoma or subdural hematoma?
|
Evacuation of the hematoma via surgical drainage
|
|
|
HYQ: Most common predisposing consition for an intracranial hemorrhage?
|
hypertension
|
|
|
HYQ: What is the principle cause of a lacunar infarct?
|
hypertension
|
|
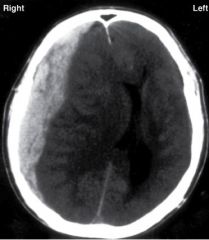
HYQ: CT Scan of the head shows a cresent shaped lesion. What event most likely caused this lesion?
|
Subdural hematoma → blunt head trauma, rupture of bridging veins
|
|
|
HYQ: What is the preferred treatment for febrile seizures?
|
Acetominophen or ibuprofen (No Aspirin)
Reassure parents |
|
|
HYQ: A patient with a DVT develops a stroke. What study would most would most likely identify the underlying etiology of the stroke?
|
Transesophageal echocardiogram (TEE)
|
|
|
What neurologic defects would be seen with an infarction of anterior cerebral artery
|
Contralateral loss of sensory and/or motor information
Legs, feet, trunk |
|
|
What neurologic defects would be seen with an infarction of middle cerebral artery (MCA)
|
Loss of sensory and/or motor info in hands, face, arms
Aphasia: Broca’s, Wernicke’s, Conduction, global |
|
|
What neurologic defects would be seen with an infarction of posterior cerebral artery
|
Visual defects: unilateral hemaniopia, macular sparing
|
|
|
What neurologic defects would be seen with an infarction of lacunar arteries?
|
one of the lacunar syndromes:
Pure motor hemiparesis Pure sensory stroke Ataxic hemiparesis Sensorimotor stroke Dysarthria – Clumsy hand syndrome |
|
|
What neurologic defects would be seen with an infarction of the basilar artery?
|
Cranial nerve abnormalities
|
|
|
What are the 5 main lacunar syndromes that may arise from a lacunar infarct?
|
Pure motor hemiparesis
Pure sensory stroke Ataxic hemiparesis Sensorimotor stroke Dysarthria – Clumsy hand syndrome |
|
|
An aphasic patient has great trouble producing words but understands everything you say. What type of aphasia does he most likely have?
|
Broca’s aphasia
|
|
|
Although benzodiazepines are used to end a seizure in status epilepticus, what is of more concern in the initial treatment?
|
Monitor ABCs
|
|
|
What is the treatment for subarachnoid hemorrhage?
|
Stop anticoagulants
BP < 150 (Labetalol) Avoid nitroprusside/ nitroglycerin etc |