![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
58 Cards in this Set
- Front
- Back
|
Macule |

Small, flat, circumscribed lesion of a different color than the normal skin |
|
|
Papule |

Small, firm, elevated lesion |
|
|
Nodule |

Palpable, elevated lesion, varies in size |
|
|
Pustule |

Elevated, erythematous lesion, usually containing purulent exudate |
|
|
Vesicle |

Elevated, thin-walled lesion containing clear fluid (blister) |
|
|
Plaque |

Large, slightly elevated lesion with flat surface, often topped by scale |
|
|
Crust |

Dry, rough surface or dried exudate or blood |
|
|
Lichenification |

Thick, dry, rough surface (leather-like) |
|
|
Keloid |

Raised, irregular, and increasing mass of collagen resulting from excessive scar tissue formation |
|
|
Fissure |

Small, deep, linear crack or tear in skin |
|
|
Ulcer |

Cavity with loss of tissue from the epidermis and dermis, often weeping or bleeding |
|
|
Erosion |

Shallow, moist cavity in epidermis |
|
|
Comedo |

Mass of sebum, keratin, and debris blocking the opening of a hair follicle (blackheads) |
|

Seborrheic Dermatitis (1) |
- One of the most common skin disorders--inflammation of the sebaceous/oil glands - Gradual increase in amount/change in quality of sebum - Skin is reddened and covered by yellowish greasy looking scales |
|

Seborrheic Dermatitis (2) (Pictured: Cradle Cap) |
- Most common during infancy called cradle cap - Higher rate in adults with CNS disorders such as Parkinson's - Condition is idiopathic - Treatment, use of low-strength cortisone cream applied topically to the area - Massage cradle cap/ warm cloth/ possible lotions |
|

Contact Dermatitis |
- Acute inflammation triggered by exogenous chemical/substance - Erythema, edema, and small vesicles that ooze/itch/burn - Poison ivy/oak, sumac, dyes, latex, furs, etc. - Can come from irritation or sensitization - Could come from a photo-allergy, certain substances could sensitize skin to sunlight |
|

Atopic Dermatitis (Eczema) |
- Chronic inflammation of skin - Rash, vesicular and exudative eruptions in children, and dry, leathery vesicles in adults - Idiopathic, inherited allergic reaction is assumed - Changes in temp can aggravate - Skin moisturizers, sun therapy, vitamin D, no meds can completely eliminate it |
|

Urticaria (hives) |
- Severe itching, redness and swelling - Can occur in airway causing asphyxiation - When swelling deeper in tissues, called angiodema, more serious - Common and often acute - Acute hypersensitivity/release of histamine - Remove antigenic factor/ antihistamines, epinephrine injection if serious |
|

Psoriasis |
- Chronic--thick flaky red patches, white silvery scales--scales develop into plaques--sometimes into pustules - Possibly slightly itchy or sore--most common between 10-30 years - Cause unknown possibly genetic--may be autoimmune - Reduce inflammation/slow growth of cells--keep lubricated, may be lifetime |
|

Rosacea |
- Chronic inflammation face--redness - Starts out mild, gets more severe/noticeable - May be dry/pimples - Ocular rosacea--eyelids swollen, eyelashes fall out - No cure - Change of lifestyle, some creams |
|

Acne Vulgaris |
- Inflammatory disease of sebaceous glands/hair follicles--papules, pustules, and comedones--deeper, boil-like nodules sometimes - Can form scars - More common in adolescents - Hormonal changes, hereditary, too much oil - Topical antibiotics, keratolyic agents, acutane if severe |
|

Herpes Zoster (Shingles) |
- Acute inflammatory dermatomal--painful vesicles - Burning/tingling begins 2-3 days before appearance of lesions/sometimes fever - Incubation 7-12 days--duration 10 days to 5 weeks - Caused by Herpes varicella-zoster virus (VZV) chickenpox - Vaccine available--not contagious but someone could get chickenpox |
|

Impetigo (1) |
- Common/contagious, superficial skin infection--vesicular/pustular lesions, rupture form thick yellow crusts - Small vesicles surrounded by circle of reddened skin - Very contagious among children - Caused by either streptococcus or staphylococcus aureus
|
|

Impetigo (2) |
- Insect bites/scabies, poor hygiene, anemia, malnutrition - Systemic use of antibiotics/ proper lesion cleaning - Good hygiene to prevent/ hand-washing |
|

Furuncles and Carbuncles |
- Furuncle/boil--pus-containing abscess--hair follicle - Carbuncle either large furuncle or multiple furuncles - inflamed hair follicle infected and infection extends beyond follicle - Bacterial infection - Hot compresses |
|

Cellulitis |
- Acute, diffuse bacterial infection of skin/subcutaneous tissue often low extremities - skin tender/hot--red lines/streaks to nearby lymph glands--prompt immediate evaluation - bacteria enzymes break down skin cells - Limb immobilized/elevated + antibiotics |
|

Dermatophytoses (general) |
- Chronic superficial fungal infection of the skin - Active border and are marked by scaling with central clearing - Dermatophytoses on scalp called tinea capitis |
|

Dermatophytoses: Tinea Capitis |
- Round/gray scaly lesions on the scalp - Contagious/epidemic among children - Rarely seen in adults |
|

Dermatophytoses: Tinea Corporis (Ringworm) |
- Lesions round, ringed and scaled with vesicles - Skin contact with infected domestic animals, especially cats |
|

Dermatophytoses: Tinea Unguium |
- Typically begins at the tip of toenails, affecting one or more nails at a time--can also affect fingernails - Affected nail looks hypertrophic or thickened, brittle, and lustreless |
|

Dermatophytoses: Tinea Pedis (Athlete's Foot) |
- Intense burning, stinging pruritus between the toes and on the soles of feet - Skin can become inflamed, dry and peeling, fissures may develop - Rare in children |
|

Dermatophytoses: Tinea Cruris (Jock Itch) |
- Raised, red, pruritic vesicular patches, well defined borders, in the groin area - More often in adult men - More in summer and aggravated by physical activity - Anti-fungals and stay dry, loose clothing, limit exercise to prevent sweating |
|

Decubitus Ulcers (Pressure Ulcers/Bed Sores) |
- Localized area of dead skin, can affect all layers - Early sign shiny reddened skin--prolonged immobilization, eventually blisters, erosions, necrosis, and ulceration - Lack of blood supply to area from constant pressure on skin - Must be treated vigorously or could become very serious |
|

Scabies and Pediculosis |
- Itch mites (scabies) and lice (pediculosis) two most common parasitic insects to infest humans - Highly contagious--intense pruritus and crawling on skin feeling, rash itching worse at night - Head lice--special shampoo, combing with special comb - Scabies special shampoos/creams/topical steroids |
|
|
Benign and Premalignant Tumors (general) |
- Benign usually just cosmetic - Premalignant tumors include: Seborrheic keratoses, dermatofibromas, keratoacanthomas, keloids, and hypertrophic scars, epidermal (sebaceous) cysts, acrochordons (skin tags), actinic keratoses, and nevi |
|

Seborrheic Keratosis |
- Benign growths originating in epidermis--tan/brown, greasy papules or plaques - Rough, wart-like texture - Cause unknown - Should be differentiated from other possibly malignant tumors |
|

Dermatofibroma |
- Benign/asymptomatic - Particularly on front of lower leg - Most often young adults, more in women - Thought to be caused by fibrous reactions to viral infections - Scaly, hard, slightly raised, pinkish-brown |
|

Keratoacanthoma |
- Benign epithelial growth--may be caused by virus--generally seen in people in their 60s - Smooth, red, dome-shaped papule with a central crust - Can disappear spontaneously but scarring is common - Must be differentiated from squamous cell carcinoma |
|

Keloids and Hypertrophic Scars |
- Occur secondary to trauma or surgery - Scar tissue out of hand, larger and thicker - More common in black-skinned people - Keloids extend beyond the wound do not regress spontaneously - Hypertrophic scars do not extend past the wound site and generally regress over time |
|

Epidermal (Sebaceous) Cyst |
- Sebaceous gland slowly fills with a thick fluid - Some cysts have a blackhead--larger cysts usually closed - Palpable and movable - Cyst may eventually burst, releasing a foul-smelling pus |
|

Acrochordon (Skin Tag) |
- Common benign skin growths/tags - Painless/usually caused by friction, found mainly on the axilla, neck and on inguinal areas of the body |
|
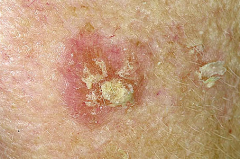
Actinic Keratosis |
- Common premalignant lesions seen on su-exposed areas - Long-term exposure to ultra-violet sunlight - Increases with age - Lighter skin--higher risk---avoid sunlight - Initially appears as an area of rough, vascular skin, which later forms a yellowish brown, adherent crust - Surgery/cryosurgery |
|
|
Skin Carcinomas (general) |
- Collectively, the skin cancers, basal cell carcinoma (BCC), squamous cell carcinoma (SCC), and malignant melanoma are the most common |
|
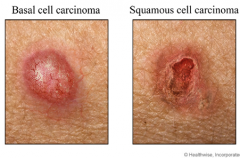
Non-melanoma Skin Cancers (Basal Cell Carcinoma and Squamous Cell Carcinoma) |
- BCC and SCC affect more than 1 million Americans each year - BCC in basal layer of epidermis--SCC in epithelial layer - Can appear anywhere-sun exposure - Can appear in several ways - Some forms of SCC more aggressive and may spread. Both need to be treated - Surgery--minimize sun exposure |
|

Malignant Melanoma |
- Most serious of the three types - Most are solitary lesions - Newly pigmented area or a change in a mole - Change in size, color, shape, elevation, surface appearance, surrounding skin, or consistency - Sun-sensitive. lighter skin--higher risk. - Surgery/removal--metastizised chemotherapy/radiation |
|
|
Abnormal Skin Pigmentation (general) |
- Skin has melanocytes that produce melanin a black pigment - Sometimes fewer in number=pale. Sometimes more numerous = darker area - Conditions include albinism, vitiligo, melasma (chloasma), nevi (moles), seborrheic warts, pityriasis, and abnormal suntan |
|

Albinism |
- Rare inherited condition, melanocytes do not produce melanin--pale/white hair, pink or blue eyes--occurs in all races. - Often accompanied by eye problems - Must avoid sun to prevent eyes and skin from burning--no cure--eye problems can sometimes be treated |
|

Vitiligo |
- Possibly autoimmune--irregular pale patches of skin--may enlarge, shrink, or stay the same size - Affects all races - No cure, cosmetics may be used - Encouraged to use sunscreen |
|

Melasma (Chloasma) |
- Occurs in woman during hormonal changes such as pregnancy or with oral contraceptive use - Patches of darker skin on the face especially cheeks - Disappears after childbirth or when oral contraceptive use is discontinued |
|

Hemangiomas |
- Benign lesions of proliferating blood vessels n the dermis - Nervus flammeus (port-wine stain) usually on face--strawberry hemangioma (pictured)--cherry hemangioma small little dot |
|
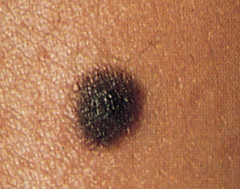
Nevi (Moles) |
- Small dark areas of the skin--dense collection of melanocytes, some may contain hair - May occasionally become malignant |
|

Pityriasis |
- Fungal infection causes patches of flaky, light or dark skin to develop on the trunk of the body - Uncommon |
|

Alopecia (Baldness) |
- Loss or absence of hair especially on the scalp - Temporary or permanent--could be underlying health problem - Aging/hereditary--could be from illness |
|

Folliculitis |
- Inflammation of hair follicles - Thighs/buttocks, beard area, scalp - Relatively common in young adults - Cleanser |
|

Corns and Calluses |
- Extremely common, localized hyperplastic areas of the stratum corneum layer of the epidermis - Corns may have glassy core, are small, and more painful - Calluses larger and commonly on ball of foot, and palms of hands - Remove pressure/friction |
|

Verrucae (Warts) |
- Elevated growths of epidermis that result from hyperplasia - Cutaneous manifestation of the HPV virus |
|

Deformed or Discoloured Nails |
- Any thickening, color change, or shape change of fingernails/toenails could be symptoms of underlying diseases/disorders |
|

Paronychia |
- Infection of skin around a nail - Caused by bacteria or fungi - Culture of the exudate taken - Antibiotics or anti-fungals |