Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
150 Cards in this Set
- Front
- Back
|
Name the types of vessels that lack medial layer. (3)
|
- capillaries
- post-capillary venules - lymphatics |
|
|
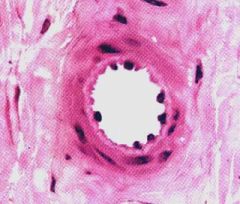
Which type of vessel is this?
- thick medial layer - rich in elastic fibers separated by alternating smooth muscle cells |
large elastic arteries
|
|
|
Which type of vessel is this?
- elastin in internal and external elastic lamina - circulatory or spirally arranged smooth muscle cells |
medium sized muscular arteries
|
|
|
Which type of vessel is this?
- no medial layer - one cell layer endothelium - no valves |
capillaries
|
|
|
Which type of vessel is this?
- no medial layer - one cell layer endothelium - one way valves |
lymphatic vessel
|
|
|
Which type of vessel is this?
- 1-2 layers of smooth muscle cells - resistance vessels - internal elastic lamina |
arterioles
|
|
|
Which type of vessel is this?
- thin medial layer - no internal elastic lamina - one way valves - large capacitance |
veins
|
|
|
Which type of vessel is this?
- no medial layer - site of vascular leakage and leukocyte emigration |
post-capillary venules
|
|
|
Atherosclerosis usually takes place in which type of vessels?
What about HTN? |
Atheroclerosis
- large elastic arteries - medium sized muscular arteries HTN - small size muscular arteries - arterioles |
|
|
Which type of capillaries are in these organs?
- endocrine glands, renal glomeruli, some digestive tract capillaries |

fenestrated
|
|
|
Which type of capillaries are in these organs?
- heart, lung, skin, muscle, CNS |

continuous
|
|
|
Which type of capillaries are in these organs?
- liver, spleen, marrow |

sinusoids
|
|
|
What are some antigens expressed on endothelial cells under normal condition?
|
- CD31(PECAM1) at inter-endothelial junction: leukocyte transmigration
- CD34 on endothelial cells in lymph nodes: bind to naive T cell - vWF |
|

Ultrastructure near endothelial cell membrane.
|
pinocytic vesicles
|
|

Ultrastructure of endothelial cells with neighbouring cells.
|
junctional complexes: eg tight junctions, etc.
|
|

Intracellular ultrastructure of endothelial cells. (hint: storage site for vWF)
|
Weibel-Palade bodies
|
|
|
Endothelial cell functions. (6)
|
- transfer of molecules
- produce ECM - regulate blood flow - regulate stasis - regulate cell growth - regulate inflammation, immuniry. |
|
|
How does endothelial cells regulate blood flow?
|
- synthesis of vasoconstrictors: endothelin, ACE
- synthesis of vasodilators: NO, prostacyclin |
|
|
How does endothelial cells regulate stasis?
|
- synthesis of pro-thrombotic factors: vWF, TF, plasminogen activator inhobitor
- synthesis of anti-thrombotic factors: prostacyclin, thrombomodulin, plasminogen activator, heparin like molecules |
|
|
How does endothelial cells regulate cell growth?
|
- synthesis of growth stimulators: PDGF, FGF, CSF
- synthesis of growth inhibitors: TGF-beta, heparin |
|
|
How does endothelial cells regulate inflammation and immunity?
|
- make cytokines: IL1,6,8
- make surface molecules: VCAM1, ICAM, E-selectin, P-selectin, CD31, HLA antigens. |
|
|
Which of the following is faster?
- endothelial stimulation - endothelial activation |
- endothelial stimulation: seconds to minutes
|
|
|
Endothelial stimulation or activation?
- rapid, reversible - induced by histamine to increase permeability, inhibit NO synthesis - redistribute P-selectin from Weibel-Palade bodies to cell surface |

endothelial stimulation:
histamine, thrombin, PAF, cytokines by activated macrophages |
|
|
Endothelial stimulation or activation?
- slow, hours to days - express newly acquired properties: altered gene expression and synthesis of new proteins |
endothelial activation:
- activators: cytokines, lipid products, hemodynamic forces, viruses, complement products, hypoxia, advanced glycosylation end products. - induced genes: adhesion molecules, cytokines, GF, vasoactive mediators, coagulation proteins, MHC molecules. |
|
|
What are some normal functions of smooth muscle cells in blood vessels? (3)
|
- vasoconstriction, vasodilation
- synthesize collagen, elastin, proteoglycans - synthesize GF, cytokines |
|
|
Minor or major vascular injury?
- proliferation of endothelial cells to repair the injury - smooth muscle minimally stinulated and stay in the medial layer |
minor vascular injury
|
|
|
Minor or major vascular injury?
- stimulation of smooth muscle cells: migrate to intimal layer and increase in proliferation and synthesis of ECM, lost ability to contract. |
Major/chronic vascular injury
- results in intimal thickening -> stenosis, thrombotic occlusion |
|
|
Causes of intimal thickening. (3)
|
- progressive atherosclerosis (most common)
- post-angioplasty: restenosis - post-organ transplant: stenosis |
|
|
What is the cause of the largest morbidity of all US diseases?
|
atherosclerosis
|
|
|
What is the age onset of atheroscleosis?
|
teens, usually becomes symptomatic in middle age.
|
|
|
Describe the progression of atherosclerosis from normal artery to clinical evident diseases.
|
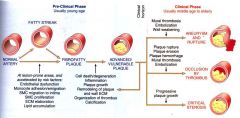
- normal artery
- fatty streak - fibrofatty plaque - vulnerable plaque - aneurysm, rupture, thrombosis, stenosis. |
|
|
What is this disease?
- hardening of large arteries |
atherosclerosis
|
|
|
What is this disease?
- hardening of small arteries and arterioles |
ateriolosclerosis
|
|
|
What is this disease?
- thickened arterial walls - calcium deposits in medial layer of medium muscular arteries - do not cause stenosis alone |
Monckeberg medial calcific sclerosis
|
|
|
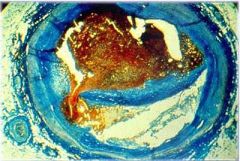
What is the "foot print" of atherosclerosis?
|
atheromatous plaque: yellowish-gray,slightly elevated.
|
|
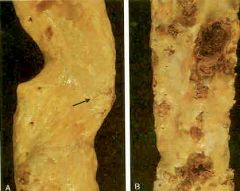
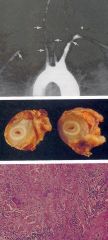
What are these called? Compare these 2 pictures.
|
left: atheromatous plaque, class IV or V lesion
right: ulcerated athreroatous plaque, class VI lesion. |
|
|
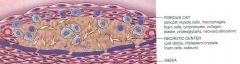
What are the components of atheromatous plaque?
|
|
|

What is this disease?
|
coronary artery plaque
- fibrosis in intima: fibrous cap - weak,thin media - lipid core of cholesterol clefts - 65% stenosis of lumen |
|
|
Which class of atherosclerosis is this?
- isolated macrophage foam cells with lipid |
class I
|
|
|
Which class of atherosclerosis is this?
- fatty streak |
class II
|
|
|
Which class of atherosclerosis is this?
- fatty streak - small extracellular lipid pool |
class III
|
|
|
Which class of atherosclerosis is this?
- atheroma: core of extracellular lipid |
class IV
|
|
|
Which class of atherosclerosis is this?
- fibroatheroma: lipid core and fibrotic layer |
class V
|
|
|
Which class of atherosclerosis is this?
- lesion with surface defect (ulceration) - hematoma or thrombosis - accompanied by dystrophic calcification |
class VI
|
|
|
Which classes of atherosclerosis are clinically significant?
|
class V and VI
|
|
|
Class VI atherosclerotic lesion:
What is the cause of hemorrhage? |
- rupture of neovascular vessels or fibrous cap
|
|
|
Class VI atherosclerotic lesion:
What is the cause of thrombosis (most serious complicaiton)? |
- exposure of thrombogenic substance -> secondary acute occlusion of lumen -> acute ischemic infarction
|
|
|
What are the top 5 manifestations of atherosclerosis in the US?
|
- coronary arteries: angina, MI
- cerebral arteries: TIA, infarction, multi-infarct dementia - aorta: aneurysm, embolism - lower extremity arteries: ischemia (claudication), stasis ulcers, gangrenous necrosis - mesenteric arteries: ischemic enteritis, acute infarction. |
|
|
What happens to the medial layer of medium/large arteries in atherosclerosis?
|

aneurysm
- variable atrophy - loss of elastic fibers - dystrophic calcification |
|
|
What are the components of fatty streak?
|
- lipid filled foam cells (macrophages)
- small amounts of T cells - extracellular lipids - not raised |
|
|
Phases of atherosclerosis:
- chronic endothelial injury |
Phase I
- hyperlipidemia - HTN - smoking - homocysteine - hemodynamic factors - toxins - viruses - immune reactions |
|
|
How does hyperlipidemia cause chronic endothelial injury?
|
- LDL-cholesterol oxidized at sites of fatty streak -> chemotactic for monocytes, toxic to endothelial cells
- ingested by macrophages |
|
|
Phases of atherosclerosis:
- increased endothelial permeability - leukocyte adhesion via VCAM1 - monocyte adhesion via VCAM1 and emigration |
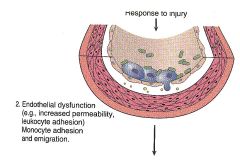
Phase II: endothelial dysfunction
|
|
|
Phases of atherosclerosis:
- smooth muscle emigrate into intimal layer: change from contractile phenotype to sythetic phenotype - macrophage activation: secrete IL1,TNF, monocyte chemoattractant protein-1, smooth muscle cell growth factor (PDGF, FGF, TGF-alpha) |
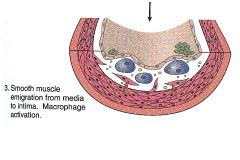
Phase III: smooth muscle cell emograion
|
|
|
Phases of atherosclerosis:
- macrophages and smooth muscle cells engulf lipid: oxidzed LDL-cholesterol - T cells augment inflammation and secrete cytokines |
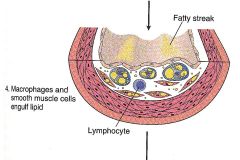
Phase IV: lipid phagocytosis
|
|
|
Phases of atherosclerosis:
- smooth muscle cell proliferation - collagen, ECM deposition - extracellular lipid |
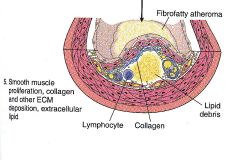
Phase V: collagen and extracellular lipid deposition and smooth muscle cell proliferation
|
|
|
T/F: Risk factors for atherosclerosis are more than additive.
|
T.
|
|
|
Non-modefiable risks for atherosclerosis.
|
- aging
- male - family history - genetic abnormality |
|
|
Modefiable risks for atherosclerosis.
|
- hyperlipidemia
- HTN - smoking - diabetes - lack of exercise |
|
|
Which genetic lipoprotein disorder is this?
- defeciency of LDL receptor |
heterozygous familial hypercholesterolemia
|
|
|
Which genetic lipoprotein disorder is this?
- apo B-100 problem |
- familial defective apoprotein B
- hypobetalipoproteinemia |
|
|
Give four common lipoprotein disorders that put people at risk for atherosclerosis
|
- familial combined hyperlipidemia: 1:200
- heterozygous familial hypercholesterolemia and familial hypertriglyceridemia: 1:500 - familial defective apoprotein B: 1:700 - hypobetalipoproteinemia: 1:1000 |
|
|
Name the three biochemical risk factors for atherosclerosis.
|
- CRP: reflect chronic component of atherosclerosis
- homocycteine: risk for ischemic heart disease - Lp(a): apoB-100 of LDL linked to apoA, particularly for men. |
|
|
Two congenital vascular anomalies.
|
- berry (saccular) aneurysms of cerebral arteries
- arteriovenous fistula |
|
|
Where is a common location of berry aneurysms?
|
ACA and MCA near branch points
|
|
|
What increases the risk for berry aneurysm to rupture?
|
- inherited disease: marfan, Ehlers-Danlos, NF-1
- smoking - HTN |
|
|
What is consequence when berry aneurysms rupture?
|
subarachnoid hemorrhage
|
|
|
What are some causes of AV fistula?
|
- trauma
- inflammation - surgery created fistula for vascular access during hemodialysis |
|
|
What are AVM or AV fistula at risks for?
|
- high output heart failure: more blood on venous side
- inadequate exchange of O2, CO2, and nutrients: bypass capillaries - rupture with hemorrhage |
|

What is this disease?
|
cerebral AVM
- gross: soft, spongy, red-brown mass - histo: haphazard arrangement of variably-sized vessels, most larger than capillaries. |
|
|
What are the two most likely cause of essential HTN?
|
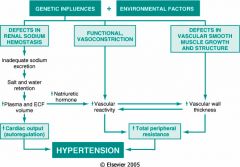
- retention of excess Na
- vasoconstriction and vascular hypertrophy |
|
|
What are hypertensive people most likely at risk for? (6)
|
- heart failure: cardiac hypertrophy
- atherosclerosis - renal failure: renal vascular arteriolosclerosis - cerebral hemorrhage and infarction - aortic dissection - ruptured berry and atherosclerotic aneurysms |
|
|
Which of the following seconday cause of HTN is most common?
- renal - cardiovascular - endocrine - neurologic |
- renal
|
|
|
What are hypertensive people most likely at risk for? (6)
|
- heart failure: cardiac hypertrophy
- atherosclerosis - renal failure: renal vascular arteriolosclerosis - cerebral hemorrhage and infarction - aortic dissection (CMD) - ruptured berry and atherosclerotic aneurysms |
|
|
Which of the following seconday cause of HTN is most common?
- renal - cardiovascular - endocrine - neurologic |
- renal
|
|
|
What is the most common lesion associated with HTN?
|
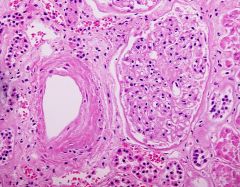
Hyaline arterioloscleosis
- thickening of media by pink hyaline material |
|
|
What is the pathogenesis of hyaline arteriolosclerosis?
|
HTN -> endothelial damage -> leakage of plasma to media -> stimulation of smooth muscle to synthesize ECM
|
|
|
Sequelae of hyaline arteriolosclerosis (HTN)
|
Progressive arteriolar stenosis:
- diffuse renal ischemia -> atrophy of glomeruli -> nephrosclerosis -> renal insufficiency -> worsen HTN (increased TPR) |
|
|
What lesion is associated with malignant HTN?
|
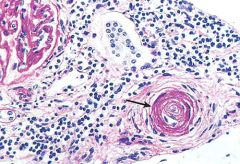
Hyperplastic arteriolosclerosis
- "onion-skin" thickening of arteriolar media and intima |
|
|
What type of HTN is this?
- diastolic pressure > 110-120 |
malignant HTN
|
|
|
True or False aneurysm?
- vascular wall contains all components of arterial wall - blood ramains within normal circulation |
- true
|
|
|
True or False aneurysm?
- extravascular hematoma communicating with vascular space |
- false
|
|
|
What are the two causes of true aneurysm?
|
- atherosclerosis
- cystic medial degeneration |
|
|
What are some causes of false aneurysm?
|
- trauma
- surgery |
|
|
What are some causes of mycotic aneurysm?
|
- infection induced
- any infectious agent |
|
|
What is the most common site to find atherosclerotic aortic aneurysm?
|
- abdominal aorta > common iliac > aortic arch > descending thoracic aorta
- most develop between renal arteries ans aortic bifurcation |
|
|
Pathogenesis of atherosclerotic aortic aneurysm (AAA). (4)
|
- media layer gradually thinned and weakened by intimal plaques.
- connective tissue defects - HTN and atherosclerosis - complicated grade VI atherosclerosis |
|
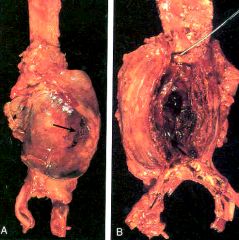
What is this?
|
AAA of abdominal aorta
- layered fibrin - unorganized thrombus in lumen |
|
|
These are associated with which disease?
- pulsatile mass (palpable in thin people) - impingement on ureter - atherosmbolism - ischemia due to occlusion od ostium of major aortic branch - |
AAA
|
|

What is this disease?
|
syphilic aneurysm
- obliterative endarteritis of vasa vasorum -> ischemic injury to media -> aneurysm -> aortic valvular insufficiency (regurgitation) with left ventricular hypertrophy |
|
|
What do you think of when a patient presents with sudden onset or acutely worsening chest or back pain?
|
aortic dissection (an emergency)
|
|
|
What people are at risk for aortic dissection?
|
- HTN patients
- Marfan syndrome - pregnant women - patients undergoing invasive vascular procedures |
|
|
Where in the media does aortic dissection happen?
|
between middle and outer 1/3 of media
|
|
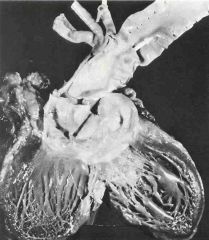
What is the cause of death of this person?
|
aortic dissection
- proximal spread -> weakened aortic valve annulus -> ruptured aortic root with resulting massive hemopericardium |
|
|
Name some complications of aortic dissection.
|
- compression/occlusion of aotic branches -> ischemia of areas supplied by these branches
|
|

What disease is this?
|
aortic dissection
- double shadow sign: column of blood on medial layer creates the sedcond line peripheral to the aortic lumen |
|

What is this?
|
Type A aortic dissection
- hemopericardium |
|

What is this?
|
Type A aortic disseciton
- extending around coronary arteries into peridcardial sac |
|

What is this? and what can this cause?
|
Cystic medial degeneration (always present in Marfan syndrome)
- aneurysm - aortic dissection |
|
|
Raynaud disease or phenomenon?
- younger women - proxysmal and reversibe - due to exaggerated vasomotor response to cold or emotion - no underlying disease |
Raynaud disease
|
|
|
Raynaud disease or phenomenon?
- older adults - intermittent and chronic cyanosis and coldness of same area - due to persistent arterial ischemia - cause arterial stenosis - due to exaggerated vasomotor response to cold or emotion - associated with atherosclerosis, SLE, Buerger disease. |
Raynaud phenomenon
|
|
|
What are the two pathogenic mechanisms of vasculitis?
|
- immune-mediated
- direct invasion by infectious agent |
|
|
What is the most common vasculitis in the US?
|
giant cell arteritis (temporal arteritis)
|
|
|
Two patterns of active giant cell arteritis.
|
- granulomatous inflammation od inner media with giant cells
- nonspecific panarteritis without giant cells |
|
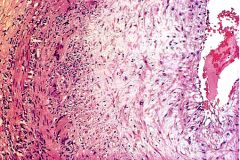
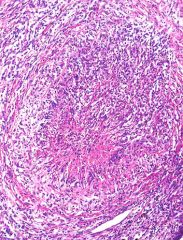
What is this disease?
|
giant cell arteritis
- intimal fibrosis - scattered giant cells - patchy, transmural infiltrate of lymphocytes, plasma cells and macrophages |
|
|
Where are the major arteries affected by giant cell arteritis?
|
- temporal
- vertebral - ophthalmic |
|
|
What is this disease?
- younger women, under age 40 - weaker pulses and lower pressure in arms than legs - see giant cell miscroscopically |
Takayasu arteritis (pulseless disease)
- intimal thickening -> narrowed arotic orifice of major arteries to upper body |
|
What is this disease?
|
Takayasu arteritis (puseless disease)
- multiple stenosis of aortic arch vessels - severe fibrosis with stenosis - lymphocytic infiltrate with multinucleated giant cells |
|
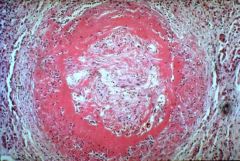
What is this disease?
|
PAN
- destruction of medial smooth muscle cell - fibrinoid necrosis of intima and media - obliteration/stenosis of lumen - transmural neutrophils (necrotizing inflammation) |
|
|
Name a segmental disease.
|
PAN
|
|
|
What is this disease?
- systemic vasculitis with transmural necrotizing inflammation if medium/small arteries in any organ except lungs. |
PAN
|
|
|
What is the most frequently affect artery in PAN?
|
Kiney
- heart - liver - GI tract - pancreas - testes - skeletal muscle - nervous system - skin |
|
|
The following are sequelae of what disease?
- microaneurysms - obstruction - ischemia with ulceration - hemorrhage - necrosis - infarction |
PAN
|
|
|
What is this disease?
- vasculitis in medium sized vessels in young children - cardiac sequelae |
Kawasaki syndrome
|
|
|
What is this disease?
- sinusitis by necrotizing granulomatous inflammation - necrotizing capillaritis in lungs - acute focal glomerulitis |
Wegener granulomatosis
- upper respiratory tract lesion - lung - kidney |
|
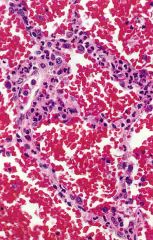
What is this?
|
necrotizing capullaritis of lung
- neutrophils infiltrating alveolar septae - wegener granulomatosis |
|
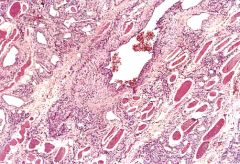
What is this?
|
transmural necrosis and obliteratio of lumen in medium sized artery
- wegener granuloamtosis |
|
|
What type of arteritis is this?
- pneumonitis -> secondary pulmonary vasculitis |
infectious arteritis
|
|
|
What type of arteritis is this?
- meningitis -> vasculitis in adjacent superficial cerebral arteries |
infectious arteritis
|
|
|
What type of arteritis is this?
- endicarditis -> embolization to arteries |
infectious arteritis
|
|
|
Pathogenesis of varicose veins in the leg.
|
venous stasis -> incompetent venous valves -> congestion, thrombosis -> edema/dermatitis/ulcers
|
|
|
T/F: Pulmonary emboli are often from superficial venous varices.
|
F.
|
|
|
Pathogenesis of esophageal varices.
|
cirrhosis -> portal hypertension -> progressively enlarging varices
|
|
|
Pathogenesis of hemorrhoids.
|
prolonged pelvic venous congestion caused by pregnancy, chronic constipation, straining at stool, pants too tight.
|
|
|
Thrombosis in veins is called ___.
|
thrombophlebitis / phlebothrombosis
|
|
|
Where does phlebothrombosis most likely originate from?
|
deep leg veins
|
|
|
What are some risk factors for phlebothrombosis?
|
- prolonged bed rest
- cardiac failure - neoplasia - pregnancy - post operative state - obesity - genetic hypercoagulable state |
|
|
What is this disease?
- leg edema, redness, swelling - + homan sign |
phlebothrombosis
|
|
|
What is usually the first manefestation of phlebothrombosis?
|
embolic event
|
|
|
What is the #1 cause of sudden death in post-op patients?
|
pulmonary thrmobiembolism (saddle)
|
|
|
Which patients are at risk for pulmonary thromboembolism?
|
- cancer
- post-operative - cardiac failure |
|
|
What are some sequelae of pulmonary thromboembolism?
|
- acute ischemia of lung
- impaired filling of left atrium and ventricle, may lead to cardiovascular collapse |
|
|
What is this disease?
- dusky cyanosis - dilated veins of head, neck, arms - respiratory disress |
Superior vena cacal syndrome
- obstruction of SVC by neoplasm (lung cancer mostly) |
|
|
What ist his disease?
- leg edema - distension of superficial abdominal collateral veins - massive proteinuria |
inferior vena caval syndrome
- neoplasm compress or envade vein - mostly hepatocellular carcinoma, renal cell carcinoma |
|
|
What is this disease?
- dilated lymphatics up to the point of obstruction - big body parts - secondary induration and ulaceration of skin |
primary lymphedemas (rare)
|
|
|
Name a hereditary familial lymphedema syndrome
|
Milroy disease
|
|
|
What is this disease?
- female, 10-25 age - edema in feet, progress upward |
lymphedema praecox
|
|
|
What is this disease?
- painful red subcutaneous streaks - regional llymphadenopathy |
lymphangitis
- bacterial infection: group A strep most common |
|

What is this disease?
|
hemangioma (begnine)
- red-purple spongy mass - +/- thrombosis |
|
What is this disease?
|
hemangioma (benign)
- proliferating blood vessels - irregular vessels lined by uniform endothelial cells |
|

What is this disease?
|
vascular ectasia (benign)
- dilation of preformed vessels - telangiectasia - nevus flammeus - spider telangiectasia of skin: cirrhosis, pregnancy |
|

What is this disease?
|
osler-weber-rendu disease
- spontaneous epistaxis - diffuse telangiectasia - death from intestinal bleeding |
|

What is the cause of this?
|
bacillary angiomatosis
- bartonella henselae (cat-scratch) - bartonella quintana tumor like growth capillary growth with cellular atypia and mitoses |
|
|
Name 2 malignant vascular tumors.
|
- angiosarcoma
- hemagiopericytoma |
|
|
Which type of kaposi sarcoma do europeans have?
|
chronic
|
|
|
Which type of kaposi sarcoma do Africans have?
|
lymphadenopathic
|
|
|
Which type of kaposi sarcoma do transplant patients have?
|
immunosuppression associated
|
|
|
Which virus is associated with kaposi sarcoma?
|
HHV8
|
|
|
Describe the stages of skin lesions in kaposi sarcoma.
|
- patch
- plaque - nodule |
|
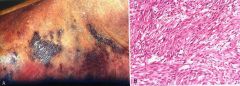
What is this disease?
|
kaposi sarcoma
- patches and plaque |