Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
135 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
headaches and visual changes, calcified mass detected on MRI
|
craniopharyngoma
derivative of rathke's pouch suprasellar region cystic spaces lined by stratified squamous epithlium filled with thick yellow-brown, cholesterol rich fluid |
|
|
|
craniopharyngoma
|
headaches and visual changes, calcified mass detected on MRI
derivative of rathke's pouch suprasellar region cystic spaces lined by stratified squamous epithlium filled with thick yellow-brown, cholesterol rich fluid |
|
|
|
Alpha feto-protein in Adults
|
>500 indicative of
hepatocellular carcinoma germ cell tumors metastatic dz in liver ataxia telangiectasia |
|
|
|
Differentiating Polycythemias
|
Polycythemia: HCT >48 in woman, >52 in men
Normal RBC Mass: Relative Polycythemia 2° to dehydration/diuresis True ↑ in RBC mass: absolute polycythemia --All 3 cell lines increase, low [EPO] = polycythemia vera --Only RBC's increase: 2° polycythemia -------Saturation O2 <92% = hypoxia -------Sat >92% EPO producing tumor |
|
|
|
Chediak Higashi Sro
|
AR sro caused by defect lysosomal trafficking
Results in: --PMN failure to fuse phagolysosome w/ recurrent pyogenic infx (esp staph & strep) --albinism --neurologic abnormalities esp nystagmus & neuropathies |
|
|
|
Albino with recurrent pyogenic infections and nystagmus
|
Chediak Higashi Sro
AR defect lysosomal trafficking Results in: --PMN failure to fuse phagolysosome w/ recurrent pyogenic infx (esp staph & strep) --albinism --neurologic abnormalities esp nystagmus & neuropathies |
|
|
|
How can you prevent infection with an intravenous catheter
|
the best way to prevent infection is to wash your hands with antibacterial soap prior to catheter insetion
|
|
|
|
MODY2
|
glucokinase mutation
glucokinase catalyzes the irreversible conversion of glucose to glucose-6-phosphate, only found in hepatocytes and pancreatic β cells kinetics: high Km & high Vmax: will not phosphorylate gluocse during fasting conditions, but allows post-prandial trapping in liver Regulated by Glucokinase Regulatory Protein (GKRP); Fructose-1-phosphate (in equilibrium with glucose-6-phosphate) activates GKRP to bind glucokinase and translocate it to the nucleus where it is non-functional NB: mutations in glucokinase = MODY2 |
|
|
|
Neonate with lethargy, vomiting, hypotonia;
Metabolic acidosis with alrge anion gap, ketosis and hypoglycemia Prioprioc Acidemia |
Deficiency of Propionyl CoA carboxylase
Branched Chain Amino Acids (Isoleucine, Valine, Thronine, methionine), Cholesterol and Odd-chain fatty acid catabolism leads to proprionic acid production propionic acid (ie proprionyl CoA) is converted to Methylmalonyl CoA by Proprionyl CoA carboxylase with a biotin cofactor Methylmalonyl CoA is isomerized to Succinyl CoA which may enter the TCA cycle |
|
|
|
What is the most common cause of aortic rupture?
What is the most common site? |
Cause: motor vehicle accidents
site: aortic isthmus, connection between ascending and descending aorta distal to left subclanian artery |
|
|
|
What is the differentiating point between direct and indirect hernias
|
Indirect hernias occur through the deep inguinal ring; Their lateral border is the inferior epigastric vessels ascending off the femoral vasculature. They proceed through the processus vaginalis.
Direct hernias push the transversalis fascia ahead of them. They enter the inguinal ring below the inferior epigastric vessels and continue downwards outside of the spermatic cord. Indirect hernias are far more common. |
|
|
|
Ulcerative mass in the anal canal of AIDS pt
|
Squamous Cell Carcinoma 2° to HPV
|
|
|
|
Coronary Sinus Dilation: what is the primary pathology?
|
Pulmonary Hypertension
|
|
|
|
thalessemia intermedia
|
all mRNA begins with the Kozak consensus sequence gccgccRccAUGG
where R is a purine and AUG codes for methionine point mutation of R to pyrimidine prevents initiation this is the basis of thalessemia intermedia (β thal) |
|
|
|
Type I Glycogenosis
|
Glucose-6 phosphatase deficiency
Type I Glycogenosis, Von Gierke Dz Hepatic/renal enlargement PAS+ glucogen storage vacuoles in many cells Severe Hypoglycemia: failure to thrive, stunted growth, convulsions Hyperuricemia (gout) Xanthomas Bleeding (platelet dysfnx) |
|
|
|
Pompe's Dz
|
lysosomal α-1,4--glucosidase deficiency
(aka acid maltase); Type II Glycogen Storage Dz, technically also a lysosomal storage dz Glycogen in lever, heart, SkM w/ Muscle Hypotonia Micro: clear glycogen deposits in muscle Pediatric form: Massive cardiomegaly → early death Mn: -P-ompe's trashes the -P-ump Adult form: only SkM involved |
|
|
|
McArdle’s Syndrome
|
aka Type V Glycogenosis
deficiency of muscle phosphorylase produces myopathic glycogenolysis adult onset: muscle cramps & weakness w/ exercise: myocytolysis & rhabdomyolysis → ↑ [ammonia]serum, myoglobinuria, abnormal lack of ↑ [lactate]serum Px: normal longevity p155; Mn: McArdle-McVardle, the M stands for Muscle |
|
|
|
Philadelphia Chromosome
|
t(9:22)
creates BRC/ABL tyrosine kinase induces CML Imatinib inhibits BRC/ABL w/o apoptosis |
|
|
|
t(9:22)
|
Philadelphia Chromosome
creates BRC/ABL tyrosine kinase induces CML Imatinib inhibits BRC/ABL w/o apoptosis |
|
|
|
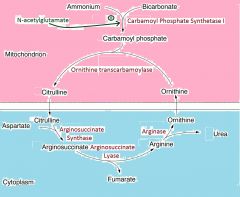
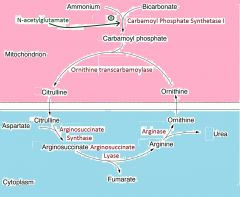
urinary orotic acid excretion
|
|
indicative of ornithine transcarbamoylase deficiency
the backup of carbamoyl phosphate is converted to orotic acid CPS1(CO2 + NH4+ + 2ATP → arbamoyl phosphate) = rate limiting step |
|
|
the urea cycle
most common disorder? |
|
CPS1(CO2 + NH4+ + 2ATP → arbamoyl phosphate) = rate limiting step
most common dysfnx = OTC (ornithine transcarbamoylase) → ↑ NH4+ & ↑ Carbamoyl phosphate → conversion of CP to orotic acid c orotic aciduria |
|
|
Achalasia
|
↓ peristalsis & ∅ LES relaxn
Barium Swallow = Bird's Beak Deformity |
|
|
|
What are the features of X-linked dominant Inheritance. Describe the features of the X-linked dominant example disease.
|
Infrequent
Males cannot transmit to sons Vitamin D resistant Rickets aka X-linked hypophasphatemia: point mutation of vitamin D receptor PHEX → ↑ renal tubular excretn of phosphate → hypophosphatemia → childhood osteomalacia w/ genu varum [also Rett Syndrome] |
|
|
|
Bird's Beak Deformity on Barium Swallow
|
Achalasia
↓ peristalsis & ∅ LES relaxn |
|
|
|
Cori's Dz
|
Type III Glycogen Storage Dz
debranching enzyme [ α-1,6-glucosidase ] deficiency accumulation of glycogen in liver, heart, muscle A milder version of Von Gierke Type I GSDz, as GNG remains intact Similar Sx: hepatomegaly hypoglycemia: stunted growth, failure to thrive, convulsions |
|
|
|
What are the genetic defect and clinical features of Prader-Willi syndrome? Of Angelman syndrome?
|
Epigeneitc process: selective inactivation of either maternal or paternal allele
Prader-Willi: MR, short stature, hypogonadism, obesity due to decreased satiety peptide YY, paternal interstitial delection chrom 15: 46XY del (15)(q11q13) + Universially Maternally imprinted (inactivated) Prader-Willi (Syndrome preventing) genes Angelman Syndrome "Happy Puppet Syndrome" MR, seizures, ataxia, inappropriate laughing maternal interstitial deletion chrom15 + + univerally paternally imprinted (inactivated) (Angelman Syndrome preventing) UBE3A gene |
|
|
|
male pseudohermaphroditism. What is the most common cause and what are the features of this cause? List additional causes and features where given.
|
Phen: female w/ normal breasts, bind pouch vagina, no uterus, amenorrhea
Y chrom & testes present but w/ ambiguous-to-female external genitalia or genital ducts Multiple causes, usually X-linked defective androgen receptor → Testicular feminization aka complete androgen insensitivity sro Else: WT gene (chrom 11): Transcriptl Activator for Gonadal & Renal Differentiation → defective testicular differentiation → Denys Drash: nephropathy, genital ambiguity, Wilm's Pediatric Kidney Tumor → WAGR: Wilm's Tumor, genital ambituity risk for gonadoblastoma, aniridia, MR Defective testicular hormone synth: 17-ketosteroid reductase, 5 alpha reductase |
p167
|
|
|
Define female pseudohermaphroditism. What is the most common cause and what are the features of this cause?
|
XX female w/ AR 21 hydroxylase deficiency → congential adrenal hyperplasia → excess androgen during embryogenesis
→ normal ovaries & internal genitalia, male external genitalia |
|
|
|
What defines a true hermaphrodite? What are some causes?
|
Both ovaries and testes present: either one testis + contralateral ovary or "ovotestis"
Chimera: individuals of 2+ zygotes (us. in vitro fertilization) Cryptic Chimera: 46XX w/ translocation of Y to autosome Mosaic: 46XX + 46XY |
|
|
|
XYY sro
|
Excessively Tall Male w/ Severe Acne
[Normal Intelligence, Normal Fertility] |
|
|
|
What are the clinical features of Klinefelter syndrome? What is the most common karyotype?
What complications are associated with this Syndrome? |
Y + ≥2X, mostly 47XXY's
2° to parental non-disjunction; maternal Ndj 2° to age Androgen Receptor (located X) contains CAG trinucleotide repeat polymorphism; shorter CAG both more active & preferentially silenced (physiologic in normal XX to use least active androgen receptor) → Sx hypogonadism w/ severe oligospermia to aspermia, common cause of male infertility Phen: Long Legs, ↓ IQ (≠MR) & Eunuch-like (gynecomastia, small penis, no virilization) ↑ # X's = ↓ IQ ↑ FSH, ↑ E ± ↓ T Risks: ↑ 20x extragonadal germ cell tumors & breast CA |
|
|
|
Acute Pancreatitis
|
2 levels:
Acute Interstitial Pancreatitis: Secretory Stasis → Digestion of Adiopse by lipase → fatty acids bind Ca2+ and precipitate into calcium salts. Inflammation and Edema. Lesions are visible on light microscapy. Acute Necrotic Pancreatitis: abnormal activation of trypsin → cascade of protease activation → autolysis of pancreas & vasculature → white chalky fat + black hemorrhage both grossly visible Causes: Gallsones, Ethanol, Trauma, Steroids, Mumps, Autoimmunitym Scorpion stings, HyperCalcemia, HyperTAGermia (>1000), ERCP (Endoscopic Retrograde Colangiopancreatography), sulfa Drugs Mn: GET SMASHED |
|
|
|
Trisomy 13
|
Patau syndrome
uniformly fatal w/in first year, vast majority <1mo ultimate cause: maternal age Phen: Cleft Palate, Cleft Lip, Polydacyly, Microcephalus w/ Narrow forehead, closely spaced eyes ± cyclopia, MR, umbilical hernia, rocker bottom feet, IUGR, Inside: Congenitla heart disease, renal defects Mn: Think P's: cleft Palate, cleft liP, Polydactyly, holoProsencephaly (forebrain dvlpt failure) Prenatal Screen: low PAPPA, low hCG [Pregnancy Assoc. Plasma Protein A] |
|
|
|
Trisomy 18
|
Edwards Syndrome usually nondisjunction or mosaic
IUGR small face to head ratio w/ micrognathia prominent occiput, low set ears, flat helices enlarged first finger: overlapping fingers congenital heart disease horseshoe kidney rocker bottom feet mental retardation mean survival 2 mo, overwelming majority die in infancy |
|
|
|
Unmineralized osteoid matrix
|
hallmark of ricketts
|
|
|
|
Alport Sro
|
X linked Mutation in Type IV Collagen production
Affects: Kidney, Ears, Eyes (Hear No Evil, See No Evil, Pee No Evil) Nephritic Sro → Chronic Renal Failure [Nephritic Sro: Inflammation → RBC Cast Hematuria, Azotemia, Oliguria, Na+ retaining Htn, & proteinuria <3.5g/d] Nerve Deafness Lens Problems (Cataracts, Lens Dislocation, Corneal Dystrophy) Interestingly: Pts lack the antigen which Goodpasture Sro Antibodies attack |
|
|
|
Mutation in Type IV Collagen Production
|
Alport Sro: X linked Mutation in Type IV Collagen production
Affects: Kidney, Ears, Eyes (Hear No Evil, See No Evil, Pee No Evil) Nephritic Sro → Chronic Renal Failure [Nephritic Sro: Inflammation → RBC Cast Hematuria, Azotemia, Oliguria, Na+ retaining Htn, & proteinuria <3.5g/d] Nerve Deafness Lens Problems (Cataracts, Lens Dislocation, Corneal Dystrophy) Interestingly: Pts lack the antigen which Goodpasture Sro Antibodies attack |
|
|
|
Hematuria w/ RBC Casts
Deafness & Cataracts |
Alport Sro: X linked Mutation in Type IV Collagen production
Affects: Kidney, Ears, Eyes (Hear No Evil, See No Evil, Pee No Evil) Nephritic Sro → Chronic Renal Failure [Nephritic Sro: Inflammation → RBC Cast Hematuria, Azotemia, Oliguria, Na+ retaining Htn, & proteinuria <3.5g/d] Nerve Deafness Lens Problems (Cataracts, Lens Dislocation, Corneal Dystrophy) Interestingly: Pts lack the antigen which Goodpasture Sro Antibodies attack |
|
|
|
Berger's Dz
|
IgA nephropathy, Berger's Dz
Respiratory/GI environmental antigen → abnormal ↑ IgA prodxn → overwhelm's hepatobiliary clearence → glomerular IgA deposition → complement activation → Nephritic Sro [Nephritic Sro: Inflammation → RBC Cast Hematuria, Azotemia, Oliguria, Na+ retaining Htn, & proteinuria <3.5g/d] LM: mesngeial proliferation EM- IC deposits in mesangium IF: IgA IC deposits in mesangium 2° IgA nephropathy may be due to celiac dz (Ab overprodxn) or liver dz (↓ IgA Clearance) NB: Henoch-Schonlein Purpura is a systemic manifestation of the same process: purpuric lesions & arthralgia + some type of renal manifestation |
|
|
|
IgA nephropathy
|
IgA nephropathy, Berger's Dz
Respiratory/GI environmental antigen → abnormal ↑ IgA prodxn → overwhelm's hepatobiliary clearence → glomerular IgA deposition → complement activation → Nephritic Sro [Nephritic Sro: Inflammation → RBC Cast Hematuria, Azotemia, Oliguria, Na+ retaining Htn, & proteinuria <3.5g/d] LM: mesngeial proliferation EM- IC deposits in mesangium IF: IgA IC deposits in mesangium 2° IgA nephropathy may be due to celiac dz (Ab overprodxn) or liver dz (↓ IgA Clearance) NB: Henoch-Schonlein Purpura is a systemic manifestation of the same process: purpuric lesions & arthralgia + some type of renal manifestation |
|
|
|
Most Common Cause of Death in SLE
|
Diffuse Proliferative Glomerulonephritis
LM: Wire Looping of capillaries EM: subendothelial/intramembranaous IgG based IC's , esp C3 IF: Granular May present as Nephritic or Nephrotic 2° to SLE or Membranoproliferative Glomerulonephritis Most common cause of death in SLE [Nephritic Sro: Inflammation → RBC Cast Hematuria, Azotemia, Oliguria, Na+ retaining Htn] [Nephrotic Sro: Massive proteinuria >3.5g/d, hyperlipidemia, fatty casts. Edema from protein loss, Thromoemboli from AT3 loss, infection from Ig loss] |
|
|
|
Diffuse Proliferative Glomerulonephritis
|
Diffuse Proliferative Glomerulonephritis
LM: Wire Looping of capillaries EM: subendothelial/intramembranaous IgG based IC's , esp C3 IF: Granular May present as Nephritic or Nephrotic 2° to SLE or Membranoproliferative Glomerulonephritis Most common cause of death in SLE [Nephritic Sro: Inflammation → RBC Cast Hematuria, Azotemia, Oliguria, Na+ retaining Htn] [Nephrotic Sro: Massive proteinuria >3.5g/d, hyperlipidemia, fatty casts. Edema from protein loss, Thromoemboli from AT3 loss, infection from Ig loss] |
|
|
|
Renal Problems
LM: Wire looping of capillaries |
Diffuse Proliferative Glomerulonephritis
LM: Wire Looping of capillaries EM: subendothelial/intramembranaous IgG based IC's , esp C3 IF: Granular May present as Nephritic or Nephrotic 2° to SLE or Membranoproliferative Glomerulonephritis Most common cause of death in SLE [Nephritic Sro: Inflammation → RBC Cast Hematuria, Azotemia, Oliguria, Na+ retaining Htn] [Nephrotic Sro: Massive proteinuria >3.5g/d, hyperlipidemia, fatty casts. Edema from protein loss, Thromoemboli from AT3 loss, infection from Ig loss] |
|
|
|
Acute Post-Streptococcal Glomerulonephritis
|
Nephritic/Nephrotic Sro Combo
LM: enlarged & hypercellular glomeruli EM: subepithelial IC hums IF: granular deposition of Antibodies and C3 Spontaneous resolution [Nephritic Sro: Inflammation → RBC Cast Hematuria, Azotemia, Oliguria, Na+ retaining Htn, & proteinuria <3.5g/d] [Nephrotic Sro: Massive proteinuria >3.5g/d, hyperlipidemia, fatty casts. Edema from protein loss, Thromoemboli from AT3 loss, infection from Ig loss] |
|
|
|
Rapidly Progressive Glomerulonephritis
|
Rapidly Progressive (Crescenteric) Glomerulonephritis
Nephritic Sro c Poor Px LM & IF: Crescent moon shape deposits of fibrin and plasma protein with cellularity of Monocytes & M∅ Goodpasture Sro: antibodies to GBM & Alveolar BM → linear IF, hematuria + hemoptysis Wegener's Granulomatosis: c-ANCA Microscopic polyangitis: p-ANCA [Nephritic Sro: Inflammation → RBC Cast Hematuria, Azotemia, Oliguria, Na+ retaining Htn, & proteinuria <3.5g/d] |
|
|
|
By what metabolic process do some drugs induce SLE-like effects
|
Slow Phase II N-acetylation
genetically determined |
|
|
|
Laron dwarfism
|
defective growth hormone receptors (JAK-STAT)
|
|
|
|
What is the fundamental defect of β thalassemias
|
mRNA processing
hypochromia & target cells |
|
|
|
Scotoma
|
area of visual loss surrounded by unimpaired vision
a neurologic result not an anatomic/physiologic finding |
|
|
|
Aseptic Hemorrhagic Cystitis in Children
|
Adenovirus
|
|
|
|
Ischemic Damage to Kidney:
which area of nephron is damaged |
proximal tubule s and thick ascending limb in the outer medulla
apparently the outer medulla has the lowest blood supply normally also these areas are actively exporting stuff, and so using up ATP and needing O2 NB: Muddy Brown casts are pathognomonic for ATN (which may be ischemic or toxic) |
|
|
|
Muddy Brown Casts
|
pathognomonic for Aute Tubular Necrosis
May be ischemic or toxic |
|
|
|
Ankylosing Spondylitis
|
HLA-B27 assoc chronic inflammatory condition
presents as morning stiffness, esp LBP ∅ ↓ lifespan Musculoskeletal: enthesitis (tendon insertion inflammation) Respiratory: limited chest expansion 2° to costal muscle enthesites Cardiovascular: Ascending aortitis → aortic dilation & insufficiency Eye: anterior uveities → blurred vision/photophobia |
|
|
|
morning stiffness/LBP
HLA-B27 |
Ankylosing Spondylitis
HLA-B27 assoc chronic inflammatory condition presents as morning stiffness, esp LBP ∅ ↓ lifespan Musculoskeletal: enthesitis (tendon insertion inflammation) Respiratory: limited chest expansion 2° to costal muscle enthesites Cardiovascular: Ascending aortitis → aortic dilation & insufficiency Eye: anterior uveities → blurred vision/photophobia |
|
|
|
Lipid Laden Macrophages in the skin of the eyelid
|
Xanthelasma, a form of xanthoma
assoc w/ hyperlipidemia |
|
|
|
Xanthelasma
|
lipid laden macrophages in the skin of the eyelid 2° to systemic hyperlipidemia
|
|
|
|
Pathogenesis of Marfan Sro
|
Defect in Fibrillin-1 "elastin assoc. glycoprotein"
most noted in; 1. habitus 2. zona fibers of lens (lens dislocation) 3. large arteries (aortic dissection) |
|
|
|
MR, eczema and mousy odor
|
PKU
AR |
|
|
|
Humoral Hypercalcemia of Malignancy
|
PTHrP
Parathyroid Hromone Related Peptide: closely resembles PTH at bioactive amino temrinal |
|
|
|
Dystonia
|
sustained involuntary contractions 2° to impaired fnx of basal ganglia, eg:
Torticollis Blepharospasm: uncontrollable blinking/forced closure Writer's Cramp |
|
|
|
Fibrous intimal thickening with endocardial plaques limited to the right heart
|
characteristic of carcinoid heart dz 2° to carcinoid sro
Canerous production of 5-HT, histamine, Bradykinin, Prostaglandins &/or tachykinins → pulmonary stenosis and/or restrictive cardiomyopathy degree of cardiac involvement ≈ 5-HT & prodxn 5-HT & bradykining inactivated by pulmonary vascular endothelial monoamine oxidase → no left sided effects Lab test: 5-hydroxyindoleacetic acid = urinary excretory metabolite of 5-HT |
|
|
|
5-hydroxyindoleacetic acid
|
Fibrous intimal thickening with endocardial plaques limited to the right heart → pulmonary stenosis and/or restrictive cardiomyopathy
characteristic of carcinoid heart dz 2° to carcinoid sro Canerous production of 5-HT, histamine, Bradykinin, Prostaglandins &/or tachykinins degree of cardiac involvement ≈ 5-HT & prodxn 5-HT & bradykining inactivated by pulmonary vascular endothelial monoamine oxidase → no left sided effects Lab test: 5-hydroxyindoleacetic acid = urinary excretory metabolite of 5-HT |
|
|
|
cardcinoid heart dz
|
Fibrous intimal thickening with endocardial plaques limited to the right heart → pulmonary stenosis and/or restrictive cardiomyopathy
2° to carcinoid sro Canerous production of 5-HT, histamine, Bradykinin, Prostaglandins &/or tachykinins degree of cardiac involvement ≈ 5-HT & prodxn 5-HT & bradykining inactivated by pulmonary vascular endothelial monoamine oxidase → no left sided effects Lab test: 5-hydroxyindoleacetic acid = urinary excretory metabolite of 5-HT |
|
|
|
Chronic Granulomatous Dz
|
Chronic Granulomatous Dz
X-linked defict of NADPH Oxidase → inability to kill organism in phagolysosomes → recurrent infx ↑↑↑ Susceptibility to certain catalase positive organism: --Staph aureus --Pseudomanas cepacia (burkholderia cepacia) --Serratia marcescens --Nocardia --Aspergillus PMN's cannot oxidize Nitroblue Tetrazolium: do not stain |
|
|
|
Defect of NADPH Oxidase
|
Chronic Granulomatous Dz
X-linked defict of NADPH Oxidase → inability to kill organism in phagolysosomes → recurrent infx ↑↑↑ Susceptibility to certain catalase positive organism: --Staph aureus --Pseudomanas cepacia (burkholderia cepacia) --Serratia marcescens --Nocardia --Aspergillus PMN's cannot oxidize Nitroblue Tetrazolium: do not stain |
|
|
|
PMN's do not stain with Nitroblue Tetrazolium
|
Chronic Granulomatous Dz
X-linked defict of NADPH Oxidase → inability to kill organism in phagolysosomes → recurrent infx ↑↑↑ Susceptibility to certain catalase positive organism: --Staph aureus --Pseudomanas cepacia (burkholderia cepacia) --Serratia marcescens --Nocardia --Aspergillus PMN's cannot oxidize Nitroblue Tetrazolium: do not stain |
|
|
|
liver biopsy sample: extensive lymphocyte infiltration with granulomatous destruction of bile ducts
|
primary biliary cirrhosis
classically: middle aged cuacasian female with hx pruritis and fatigue who now dvlps pale stool and xanthelasma |
|
|
|
middle aged cuacasian female with hx pruritis and fatigue who now dvlps pale stool and xanthelasma
|
classic picture of primary biliary cirrhosis
liver biopsy sample: extensive lymphocyte infiltration with granulomatous destruction of bile ducts |
|
|
|
male with long hx ulcerative colitis presents with fatigue and high alkaline phosphatase
|
primary sclerosing cholangitis
|
|
|
|
elderly female with weight loss, abdominal discomfort, jaundice and epigastric mass
|
pancreatic cancer
|
|
|
|
homeless malewith fever, abdominal pain and jaundice
|
acute cholangitis
|
|
|
|
What signals induce atherosclerotic plaque formatino
|
Platelet signals:
PDGF: chemotactic and mitogenic for VSMC's TGF-β: chemotactic for VSMC's |
|
|
|
Inheritance of Glaucoma
|
Polygenic
|
|
|
|
Inheritance of Epilepsy
|
Polygenic
|
|
|
|
Inheritance of Androgenic Baldness
|
Polygenic
|
|
|
|
MPO Deficiency
|
Myeloperoxidase Deficiency
cannot convert H2O2 → ROS's for killing Similar to Chronic Granulomatous Dz (NADPH deficiency) most organisms produce H2O2 on their own CGD catalase positive organisms will survive because H2O2 before MPO can convert it to SOD In MPO KO all organisms can survive within the phagocytes |
|
|
|
Late separation of the umbilical cord,
Recurrent non-puritic skin infx Gingivitis |
Classic Triad of Leukocyte Adhesion Deficiency
AR absence of CD18 necessary to form integrins Leukocyte migration: 1. Rolling adhesion via E & P Selectins expressed on Endothelium (ligand on WBC) 2. Firm attachment via Integrins expressed on WBC (ligand on Endothelium) 3. Transmigration via PECAM-1 (CD31) expressed on both |
|
|
|
CD18 deficiency
|
Leukocyte Adhesion Deficiency
AR absence of CD18 necessary to form integrins Classic Triad of Late separation of the umbilical cord, Recurrent non-puritic skin infx Gingivitis Leukocyte migration: 1. Rolling adhesion via E & P Selectins expressed on Endothelium (ligand on WBC) 2. Firm attachment via Integrins expressed on WBC (ligand on Endothelium) 3. Transmigration via PECAM-1 (CD31) expressed on both |
|
|
|
Deficiency of late complement components
|
C5b - C9
no MAC → esp vulnerable to Neisseria |
|
|
|
genetic defect: ↑ vunlnerability to Neisseria
|
Deficiency of late complement componentsC5b - C9
no MAC → esp vulnerable to Neisseria |
|
|
|
Hypersegmented PMNs
|
Indicative of B12 (transcobalamin) deficiency
|
|
|
|
Primary amenorrhea with fully developed 2° sexual characteristics
|
Anatomic Defect:
Imperforate Hymen or Mullerian duct abnormalities |
|
|
|
Heart Murmur + Bounding Pulses
|
Aortic Regurgitation
Abnormally high LVSV followed by rapid regurgitant flow into left ventricle → wide pulse pressure Signs: "water-hammer" pulses & de Musset's head bob |
|
|
|
Heart Murmur + Head Bob
|
Aortic Regurgitation
Abnormally high LVSV followed by rapid regurgitant flow into left ventricle → wide pulse pressure Signs: "water-hammer" pulses & de Musset's head bob |
|
|
|
Aortic Regurgitation
|
Abnormally high LVSV followed by rapid regurgitant flow into left ventricle → Diastolic murmur + wide pulse pressure
Signs: "water-hammer" pulses & de Musset's head bob |
|
|
|
Why don't all lungers with cor pulmonale have edema
|
passive ↑ in lymphatic flow
no edema until lymphatic flow overwhelmed |
|
|
|
Gilbert Sro
|
Reduced functionality of UDG glucuronyl transferase
AR episodic unconjugated bilirubinemia following stress w/o ↑ LFT's |
|
|
|
episodic jaundice following stress, ∅↑ LFT
|
Gilbert Sro
AR Reduced functionality of UDG glucuronyl transferase |
|
|
|
Reduced functionality of UDG glucuronyl transferase
|
Gilbert Sro
AR episodic unconjugated bilirubinemia following stress w/o ↑ LFT's |
|
|
|
Young adult with chronically elevated LFTs
|
most probable scenario for Wilson's Dz
↓ ceruloplasmin ↑ urinary copper Kayser-Fleisher rings |
|
|
|
Folate Deficiency
|
THF required for synthesis of
All purines dTMP (Thymidine) megaloblastic anemia phenytoin, sulfas, Methotrexate reverse with folate alleviate with thymidine NB: purines 90% recycled, thymidine synthesis most impaired |
|
|
|
ADA KO
|
Adenosine deaminase (Adenosine → Inosine)
an important step in Purine degradation Inosine will be degraded to Hypoxanthine Hypoxanthine may be recycled by HGPRT to IMP or degraded by Xanthine Oxidase (Hypoxanthine → Xanthine → Uric Acid) [same enzyme, 2 steps] ADA KO results in a mass-action ↑ dATP dATP inhibits Ribonucleotide Reductase, which is converts NDPs → dNDPs necessary for DNA synthesis [specifically ADP, UDP, CDP and GDP → dADP, dUDP, dCDP, dGDP] worst hit cells: rapidly proliferating lymphocytes → 2nd most common form of SCID (AR) (most common form: X linked deficiency of γ chain necessary for T lymphoblast response to IL7 survival signal in thymus) |
|
|
|
Exertional Dyspnea
PAS+ Cytoplasmic inclusions on Liver Biopsy |
globules of unsecreted α1 antitrypsin in periportal hepatocytes
→ cirrhosis & hepatocellular carcinoma → para-acinar emphysema emphysema |
|
|
|
Intranasal ulceration, Sudden Onset Oliguria
|
Wegener's Granulomatosis
antineutrophil cytoplasmic antibodies c-ANCA's → rapidly progressive (crescenteric) glomerulonephritis Nephritic Sro w/ poor px NB: hemoptysis indicative of Goodpasture Sro |
|
|
|
anti-neutrophil antibodies
|
Wegener's Granulomatosis
antineutrophil cytoplasmic antibodies c-ANCA's → rapidly progressive (crescenteric) glomerulonephritis Nephritic Sro w/ poor px NB: hemoptysis indicative of Goodpasture Sro |
|
|
|
hematuria + hemoptysis
|
Goodpasture Sro
hematuria + hemoptysis antibodies to GBM and alveolar basement membrane → rapidly progressive (crescenteric) glomerulonephritis Nephritic Sro w/ poor px linear Immunofluorescence NB: mucosal uceration typical of Wegener's w/ antineutrophil cANCA's |
|
|
|
Goodpasture Sro
|
hematuria + hemoptysis
|
|
|
|
Myotonic Dystrophy
|
CTG trinucleotide expansion within myotponia protein kinase
AD inheritance Cataracts & Myotonia Myotonia: unwanted sustained muscle contractions --cannot release doorhandles Type 1 fibers more affected Also: frontal balding & gonadal atrophy differentiate from Duchenne: Myotonic Dystrophy does not have necrosis of muscle fiber sand fibrofatty replacement |
|
|
|
Pre-schooler comes to stand by spreading legs and walking his hands backwards
|
Gower's Sign of Duchenne Muscular Dystrophy
X linked frameshift → nonsense mutation within dystrophin gene dystrophin anchors skeletal and muscle fibers → accelerated muscle breakdown starts in pelvic girdle → progresses superiorly Onset <5yo pseudohypertrophy of calves 2° fibro-fatty replacement Dx: ↑CPK and muscle biopsy: necrosis and fibrofatty replacement |
|
|
|
Dystrophin Gene Mutation
|
dystrophin anchors skeletal and muscle fibers → accelerated muscle breakdown
X linked frameshift → nonsense mutation → Duchenne's Muscular Dystrophy starts in pelvic girdle → progresses superiorly Onset <5yo pseudohypertrophy of calves 2° fibro-fatty replacement Gower's sign: coming to a stand via spreading legs apart and "walking" backwards on their hands so as not to need lower extremities Dx: ↑CPK and muscle biopsy: necrosis and fibrofatty replacement |
|
|
|
↑ CPK
muscle biopsy with fibrofatty replacement |
Duchenne's Muscular Dystrophy
X linked frameshift → nonsense mutation within dystrophin gene dystrophin anchors skeletal and muscle fibers → accelerated muscle breakdown starts in pelvic girdle → progresses superiorly Onset <5yo pseudohypertrophy of calves 2° fibro-fatty replacement Gower's sign: coming to a stand via spreading legs apart and "walking" backwards on their hands so as not to need lower extremities Dx: ↑CPK and muscle biopsy: necrosis and fibrofatty replacement |
|
|
|
What is the mechanism by which Systemic Hypertension produces Pulmonary Hypertension
|
systemic hypertension → Left Ventricular Failure → Pulmonary Congestion ie ↑ Hydrostatic pressure → Edema → reactive vasoconstriction
reactive vasoconstrxn normally physiologic to direct blood towards more oxygenated areas. With whole lung edema creates pulmonary htn |
|
|
|
Giant Cell Arteritis
|
aka Temporal Arterities
>50 yo with headaches and jaw claudication late stages visual impairment Pathogenesis: granulomatous inflam of large arteries, esp Tempral NB: looks just like Takayasu's Pulseless Arterities, except that one affects the aorta and great vessels <50yo |
|
|
|
Takayasu's Dz
|
aka Pulseless Dz
<50 yo with extremely weak Carotid/UE pulses (palpable LE pulses) Granulomatous obliteration of aorta & great vessels NB: same histology as Giant Cell temproal arteritis, except that dz affects medium sized vessels >50 yo |
|
|
|
Pt has extremely weak Carotid, UE pulses
|
Takayasu's Arteritis, aka Pulseless Dz
<50 yo with extremely weak Carotid/UE pulses (palpable LE pulses) Granulomatous obliteration of aorta & great vessels NB: same histology as Giant Cell temproal arteritis, except that dz affects medium sized vessels >50 yo |
|
|
|
Polyarteritis Nodosum
|
Chronically ongoing inflammation of medium & small arteries
Segmentally distinct acute inflam → Mixed WBC infiltrate → Fibrinoid necrosis (Contrast Mixed WBC Infitlrate to eosinophil dominated Churgg-Strauss, and PMN dominanted -ie leukocytoclastic- Microscopic polyangitis) Histology: thick hyalinosis in adventitia All stages concurrent around the body (Contrast to Kawasaki's lock-step progression) Not assoc with ANCA's (Contrast to Wegener's and Microscopic Polyangitis) Fatal if UnTx Rx: immunosuppressents |
|
|
|
Arterial Biopsies from different locations in different stages of acute inflammation and healed fibrinoid necrosis
|
Polyarteritis Nodosum; Chronically ongoing inflammation of medium & small arteries
Segmentally distinct acute inflam → Mixed WBC infiltrate → Fibrinoid necrosis (Contrast Mixed WBC Infitlrate to eosinophil dominated Churgg-Strauss, and PMN dominanted -ie leukocytoclastic- Microscopic polyangitis) Histology: thick hyalinosis in adventitia All stages concurrent around the body (Contrast to Kawasaki's lock-step progression) Not assoc with ANCA's (Contrast to Wegener's and Microscopic Polyangitis) Fatal if UnTx Rx: immunosuppressents |
|
|
|
Wegener's Dz
|
Wegener's Granulomatosis
c-ANCA assoc (PR3 ANCA) Classic triad: Acute, Cavitating, Necrotizing Granulomas of RespiratoryTract Necrotizing Vasculitis of Small and Medium Vessels with Ulceration of Pharynx Rapidly Progressive (Crescenteric) Glomerulonephritis (hypercellularity of parietal cell layer) [Nephritic Sro: Inflammation → RBC Cast Hematuria, Azotemia, Oliguria, Na+ retaining Htn, & proteinuria <3.5g/d] Poor Px |
|
|
|
c-ANCA
|
Wegener's Granulomatosis
c-ANCA assoc (PR3 ANCA) Classic triad: Acute, Cavitating, Necrotizing Granulomas of RespiratoryTract Necrotizing Vasculitis of Small and Medium Vessels with Ulceration of Pharynx Rapidly Progressive (Crescenteric) Glomerulonephritis (hypercellularity of parietal cell layer) [Nephritic Sro: Inflammation → RBC Cast Hematuria, Azotemia, Oliguria, Na+ retaining Htn, & proteinuria <3.5g/d] Poor Px |
|
|
|
Ulceration of Pharyngeal Mucosa
Acute Onset Oliguria |
Wegener's Granulomatosis
c-ANCA assoc (PR3 ANCA) Classic triad: Acute, Cavitating, Necrotizing Granulomas of RespiratoryTract Necrotizing Vasculitis of Small and Medium Vessels with Ulceration of Pharynx Rapidly Progressive (Crescenteric) Glomerulonephritis (hypercellularity of parietal cell layer) [Nephritic Sro: Inflammation → RBC Cast Hematuria, Azotemia, Oliguria, Na+ retaining Htn, & proteinuria <3.5g/d] Poor Px |
|
|
|
Buerger's Dz
|
Buerger's Thromboangitis Obliterans
Cigarette Smoking <35 yo Sharply segmental vasculitis of medium & small arteries Toxicity of Tobacco or Immune Response to Contents Severly painful episodes of ischemia |
|
|
|
Young Adult Smoker with Sharp Pain in Hands
|
Buerger's Thromboangitis Obliterans
Cigarette Smoking <35 yo Sharply segmental vasculitis of medium & small arteries Toxicity of Tobacco or Immune Response to Contents Severly painful episodes of ischemia |
|
|
|
Kawasaki's Dz
|
Young Children <4yo produce autoantibodies to endthlium
presents as acute febrile illness acute inflammation and fibrinoid necrosis unlike Polyarteritis nodosum: occurs all around body in lock step (no simultaneous presentation of different phases) Fibrinoid necrosis w/ predilicition for coronary arteries → aneurysm → death Rx: IVIg's & Aspirin |
|
|
|
Microscopic Polyangitis
|
Microscopic Polyangitis aka leukocytoclastic vasculitis
mostly ANCA assoc. Arterioles, Capillaries, Venules usually only PMN's seen (thus leukocytoclastic vasculitis) |
|
|
|
Churg Strauss Dz
|
Hyperallergic Response Vasculitis (to unknown antigen)
Classic Quartet Eosinophilia Asthma Necrotizing Vasculitis of Small Vessels Granulomas Extravascular Precipitated by Leukotriene Receptor Antagonists in Asthmatics |
|
|
|
leukocytoclastic vasculitis
|
Microscopic Polyangitis aka leukocytoclastic vasculitis
mostly ANCA assoc. Arterioles, Capillaries, Venules usually only PMN's seen (thus leukocytoclastic vasculitis) |
|
|
|
Vasculitis of Arterioles, Capillaries, and Venules
|
Microscopic Polyangitis aka leukocytoclastic vasculitis
mostly ANCA assoc. Arterioles, Capillaries, Venules usually only PMN's seen (thus leukocytoclastic vasculitis) |
|
|
|
Vasculities with only PMNs visible on biopsy
|
Microscopic Polyangitis aka leukocytoclastic vasculitis
mostly ANCA assoc. Arterioles, Capillaries, Venules usually only PMN's seen (thus leukocytoclastic vasculitis) |
|
|
|
Vasculitis with Eosinophilia
|
Churg Strauss Dz, aka Hyperallergic Response Vasculitis (to unknown antigen)
Classic Quartet Eosinophilia Asthma Necrotizing Vasculitis of Small Vessels Granulomas Extravascular Precipitated by Leukotriene Receptor Antagonists in Asthmatics |
|
|
|
Vasculitis following Leukast Administration
|
Churg Strauss Dz, aka Hyperallergic Response Vasculitis (to unknown antigen)
Classic Quartet Eosinophilia Asthma Necrotizing Vasculitis of Small Vessels Granulomas Extravascular Precipitated by Leukotriene Receptor Antagonists in Asthmatics |
|
|
|
Febrile Illness in Preschooler leads to Coronary Aneurism
|
Kawasaki's Dz
Young Children <4yo produce autoantibodies to endthlium presents as acute febrile illness acute inflammation and fibrinoid necrosis unlike Polyarteritis nodosum: occurs all around body in lock step (no simultaneous presentation of different phases) Fibrinoid necrosis w/ predilicition for coronary arteries → aneurysm → death Rx: IVIg's & Aspirin |
|
|
|
Abnormally High HbA2
|
α2δ2
indicative of β thalassemia trait |
|
|
|
The most sure sign of irreversible cell linjury
|
mitochondrial vacuolization
|
|
|
|
Mitochondrial Vacuolization
|
the most sure sign of irreversible cell injury
|
|
|
|
Wilsons's Dz
|
Wilson's Dz: Mutation of ATPB7 on chrom 13
ATPB7: ATP dependent copper transporter responsible for getting copper into the right place where it can be bound with ceruloplasmin or excreted in bile excess copper builds up in liver → liver toxicity long latent period until copper overwhelms liver → Systemic Manifetations Asterixis Damage to Basal Ganglia: dysarthria, parkinsonian like rigidity Kayser-Fleischer Rings around the iris Hemolysis Dx: Slit lamp examination demonstrates kayser fleischer rings Tx: penicillamine Cure: Liver transplant |
|
|
|
ATPB7
|
Wilson's Dz: Mutation of ATPB7 on chrom 13
ATPB7: ATP dependent copper transporter responsible for getting copper into the right place where it can be bound with ceruloplasmin or excreted in bile excess copper builds up in liver → liver toxicity long latent period until copper overwhelms liver → Systemic Manifetations Asterixis Damage to Basal Ganglia: dysarthria, parkinsonian like rigidity Kayser-Fleischer Rings around the iris Hemolysis Dx: Slit lamp examination demonstrates kayser fleischer rings Tx: penicillamine Cure: Liver transplant |
|
|
|
Young Adult with New Onset Bradykinesia, Dysarthria
|
Wilson's Dz: Mutation of ATPB7 on chrom 13
ATPB7: ATP dependent copper transporter responsible for getting copper into the right place where it can be bound with ceruloplasmin or excreted in bile excess copper builds up in liver → liver toxicity long latent period until copper overwhelms liver → Systemic Manifetations Asterixis Damage to Basal Ganglia: dysarthria, parkinsonian like rigidity Kayser-Fleischer Rings around the iris Hemolysis Dx: Slit lamp examination demonstrates kayser fleischer rings Tx: penicillamine Cure: Liver transplant |
|
|
|
Keyser-Fleischer
|
Wilson's Dz: Mutation of ATPB7 on chrom 13
ATPB7: ATP dependent copper transporter responsible for getting copper into the right place where it can be bound with ceruloplasmin or excreted in bile excess copper builds up in liver → liver toxicity long latent period until copper overwhelms liver → Systemic Manifetations Asterixis Damage to Basal Ganglia: dysarthria, parkinsonian like rigidity Kayser-Fleischer Rings around the iris Hemolysis Dx: Slit lamp examination demonstrates kayser fleischer rings Tx: penicillamine Cure: Liver transplant |
|
|
|
Homocysteinuria
|
Cystathionine synthase deficiency
Marfanoid Habitus and Thromboemboli --Homocysteine produced as end product of SAM usage --Methionine Synthase aka Homocysteine methyltransferase[B12] (Homocysteine + N5-methyl-THF → Methionine) --Methionine + ATP → SAM --Methyltransferase(SAM → S-adensoyl homocysteine + methyl group on other subtrate) --Unimportant enzyme (SAH → Homocysteine & Adenosine) --at this point Homocysteine may be recycled or Cystathione synthetase[B6](Homocysteine + Serine → Cystathione Csystathionase[B6](Cystathione → Cysteine) 1/2 of pts respond positively to B6 supplementation (↑ functionality of poorly functioning cystathione synthetase) |
|
|
|
Young Child with Thromboembolitic Infarcts in Various stages of healing
|
Homocysteinuria: Cystathionine synthase deficiency
Marfanoid Habitus and Thromboemboli --Homocysteine produced as end product of SAM usage --Methionine Synthase aka Homocysteine methyltransferase[B12] (Homocysteine + N5-methyl-THF → Methionine) --Methionine + ATP → SAM --Methyltransferase(SAM → S-adensoyl homocysteine + methyl group on other subtrate) --Unimportant enzyme (SAH → Homocysteine & Adenosine) --at this point Homocysteine may be recycled or Cystathione synthetase[B6](Homocysteine + Serine → Cystathione Csystathionase[B6](Cystathione → Cysteine) 1/2 of pts respond positively to B6 supplementation (↑ functionality of poorly functioning cystathione synthetase) |
|
|
|
polymicrogyria
|
small gyri → MR
assoc. w/ arnold chiari |
|
|
|
Arnold Chiari Malformation
|
Posterior fossa is too small: not enough space for the cerebellum
Components: Type 2: hydrocephalus and spina bifida you must correct clinically --malformed midline cerebellum: vermis extends thru foramen magnum; --aquaductal stenosis, hydrocephalus, hydromyelia (enlarge central canal) --kinked medulla oblongata --herniated cerebellar tonsils --broken qudrigeminal plate --spina bifida c lumbar myelomenigocele --displaced brain c pressure atrophy --assoc: polymicroyria, aqueductal stenosis, cerebral heterotopias, hydromyelia Type 1: sphingomyelia, loss of heat and pain cerebellar tonsils hang into vertebral canal → adult onset HA & Ataxia |
|
|
|
HNPCC
|
AD defect in DNA proofreading and mismatch repair
Colon, endometrial & ovarian cancers |
|
|
|
Defective enzyme in DNA proofreading and mismatch repair
|
HNPCC
AD Colon, endometrial & ovarian cancers |
|
|
|
Prolactinomas
|
prolactin suppresses GnRH prodxn → hypogonadism
risk for osteoporosis in women indolent tumor, mostly present in women <10mm as amenorrhea, in men as >10mm (micro vs macro) but still indolent |
|