Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
44 Cards in this Set
- Front
- Back
|
superior thoracic aperture is also called _____
inferior thoracic aperture is also called _______ |
thoracic inlet
thoracic outlet |
|
|
Thoracic cavity consists of R and L pleural cavities, each surrounding a lung, and the mediastinum, which separates ___________
|
separates the R and L pleural cavities
|
|
|
Penetrating wounds to the neck or poor technique in attempting to access the subclavian vein can lead to what?
|
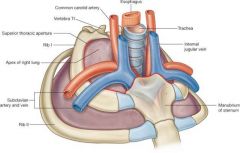
collapsed lung
(copula of lung extends into root of neck) |
|
|
The pleurae are closed sacs of serous membrane that enclose each lung. What are the two parts?
|
parietal & visceral pleura
|
|
|
The Visceral pleura surrounds the lung and the parietal pluera surrounds ........
|
everything else!
encloses entire pleural area & separates it from the other regions of the thorax |
|
|
The Parietal pleura is divided into regions based on the structures that they contact. What are the 4 regions?
|
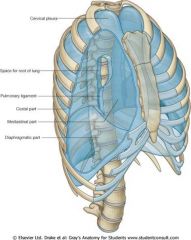
costal
diaphragmatic mediastinal cervical (cupola) |
|
|
The ___________ is the potential space between the parietal and visceral pleura.
|
pleural cavity
|
|
|
T/F
Normally the two pleural layers are separated by a thin layer of serous fluid, not an actual space or cavity. |
TRUE
|
|
|
What does the serous fluid allow?
|
the parietal and visceral pleura to slide across each other easily
|
|
|
Where do some actual spaces btwn the parietal and visceral plueras' exist?
why do these spaces exist? |
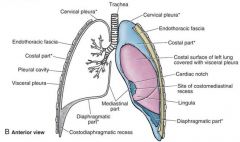
costomediastinal recess & costodiaphragmatic recess
the lungs typically do not expand into these spaces |
|
|
Where does the costodiaphragmatic recess occur?
|
btwn the costal & diaphragmatic parts of the parietal plueral
|
|
|
where does the costomediastinal recess occur?
|
anteriorly btwn the costal & mediastinal parts
*larger on left side due to cardiac notch |
|
|
Fluids may collect in these spaces, know as ?
What fluids may accumulate? |
pleural effusion
serous fluid = hydrothorax blood = hemothorax chyle = chylothorax (can be seen on X-ray bc space is white instead of black) |
|
|
Clinical significance of the pleurae
|
-each cavity is separate compartment--> isolation of infection
-fluid accumulation can occur -inflammation = pleuritis |
|
|
The trachea descends into the thorax and splits into left and right __(a)____.
_(a)___ divide into __(b)___, which divide into __(c)__ |
(a) main (primary) bronchi
(b) lobar (secondary) bronchi (c) segmental (tertiary) bronchi |
|
|
Each segmental (tertiary) bronchi supplies a ______________, the functional unit of the lung
|
bronco-pulmonary segment
|
|
|
The right inferior (lower) lobar bronchus is in line with the _________, and foreign objects often lodge here
|
right main bronchus
|
|
|
O2 & nutrients are provided to lungs via __________
|
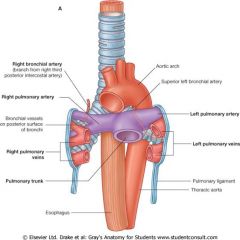
bronchial arteries
|
|
|
The left side has a superior & inferior left bronchial artery that arise directly from what?
|
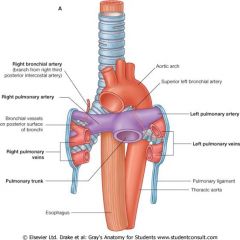
the anterior surface of the thoracic aorta
|
|
|
The right side has a SINGLE right bronchial artery which typically arises from _____________________
or from ________________________ |
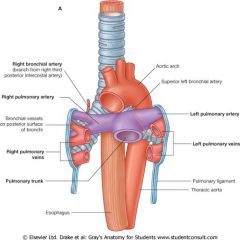
the proximal part of one of the posterior intercostal arteries (usually the 3rd)
or from a common trunk w/ the left superior bronchial artery |
|
|
Air enter/leaves the lung via _______
Deoxygenated blood enters via ______ Oxygenetated blood leave via _______ |
(air) primary bronchi
(deoxygenated blood) pulmonary artery (oxygenated blood) pulmonary veins |
|
|
The collection of tubular structures connecting the lung to structures in the mediastinum is referred to as what?
|
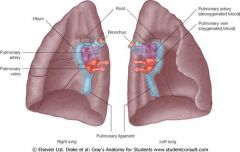
the root of the lung
|
|
|
The root of the lung contains what?
|
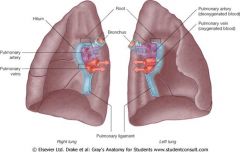
primary bronchus
pulmonary artery & vein bronchial vessels nerves lymphatics |
|
|
The _______ nerve runs anterior to the root of the lung & the _____ nerve runs posterior to it
|
anterior - phrenic nerve
posterior- vagus nerve |
|
|
The region on the medial surface of the lung outlined by plueral reflection, where the structures that make up the root of the lung enter, is the what?
|
hilum of lung
(hilum & root are NOT the same, hilum = where structures enter, root = structures) |
|
|
What is the pulmonary ligament?
|
a thin reflection of pleura connecting the lung hilum to the mediastinum
|
|
|
The right lung has (2/3) lobes and (1/2) fissures
What runs along the sulcus? |
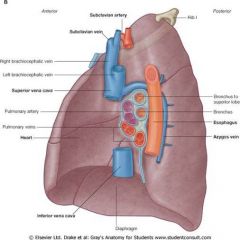
3 lobes - superior, middle, inferior
2 fissures- horizontal, oblique sulcus- Azygos v, esophagus, R Subclavian a, vena cava, 1st rib |
|
|
The left lung has (2/3) lobes and (1/2) fissures
What runs along the sulcus? What 2 other features are unique to the left lung? |
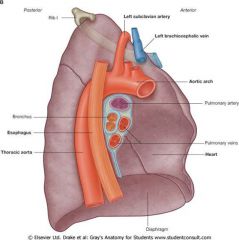
2 lobes- superior, inferior
1 fissure- oblique sulcus- aorta, esophagus, L Subclavian a, L brachiocephalic v, 1st rib unique features- lingula & cardiac impression |
|
|
What are 3 signs that would indicate lung disease?
|
enlarged air spaces (emphysema)
carbon deposits (black) enlarged/blackened lymph nodes |
|
|
What is significant about bronchopulmonary segments?
|
Each segment has its own artery and can function independently, allows individual segments to be removed if diseased, leaves rest of lung intact & function remains
|
|
|
During normal inhalation, what muscle is responsible?
during forced? |
normal- mainly diaphram (phrenic n) & some intercostal muscles
forced- anything attached to rib is involved |
|
|
During normal exhalation, what muscle is responsible?
during forced? |
normal- none
forced- anterior abdominal wall muscles |
|
|
The _______ is the main muscle involved in breathing. It also separates the thoracic and abdominal cavitites
|
diaphram
|
|
|
What arteries supply the diaphram?
|
-paricardiacophrenic (from internal thoracic)
-musculophrenic (terminal branch of internal thoracic along w/ superior epigastric) -superior phrenic (from thoracic aorta) -inferior phrenic arteries (often from abdominal aorta) |
|
|
What are the 3 openings in the diaphragm?
what spinal level are they at, and what passes through? |
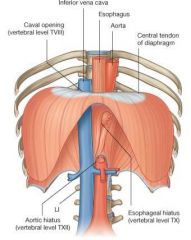
Caval opening: T8, inferior vena cava
Esophageal hiatus: T10, esophagus & vagal trunks Aortic hiatus: T12, aorta & thoracic duct |
|
|
Increaseing intrathoracic voume requires what movements?
|
-descent of the diaphram (piston)
-anterior movement of the sternum (pump handle movement) -elevation of the lateral aspect of the ribs (widening region of ribs)(bucket handle movement) |
|
|
Normal breathing diaphram & abdominal movement, pressure change:
Inspiration- Exhalation- |
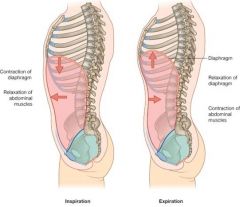
Inhalation-
contraction of diaphram relaxation of abdominal muscles decrease intrathoracic pressure (increase vertical dimension) Exhalation- relaxation of diaphram NO abdominal movement increases intrathoracic pressure (decrease vertical dimension) |
|
|
Lung examination involves what?
|
observation
palpation ausculation *need to know surface anatomy* (also percussion & fremitus) |
|
|
Where is the superior border of the lung?
|
pleura and lung project above 1st rib
|
|
|
Where is the anterior border ?
|

pleura approaches midline on R but not as far on L
costomediastinal recess |
|
|
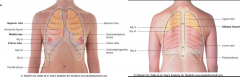
Where is the inferior & posterior border?
|
lower border of lung high anteriorly
6th Rib level at mi-clavicular line, 8th rib level at mid-axillary line, and 10th rib level at scapular level (pleural border is at 2 ribs lower at each point) costodiaphragmatic recess |
|
|
What lung points do you check with a stethoscope?
|
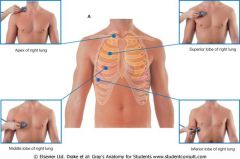
Apex
middle lobe (right lung only) superior lobe inferior lobe |
|
|
What can be found using lung palpation?
|
-thoracic expansion during respiration
-pleural friction rub -crepitus due to trapped air |
|
|
Thoracocentesis (chest tube placement) is done at the ______________ recess.
Procedurally start at inferior rib and go up slightly, making sure to avoid the intercostal___________, which is unprotected directly below the superior rib. |
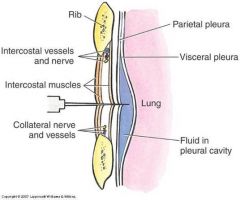
costodiaphragmatic recess
intercostal nerve |