![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
60 Cards in this Set
- Front
- Back
|
What is the normal flora in the female genital tract responsible for creating an acidic environment? |
Lactobacillus sp.
(acidic environment helps protect against many pathogens) |
|
|
what are the five etiologic microorganisms that cause STDS? |
Neisseria Gonorrhoeae |
|
|
how is Neisseria G distinguished in a culture (morphology)? What culture does it grow on?
what cells can Neisseria G be found on and w/n? |
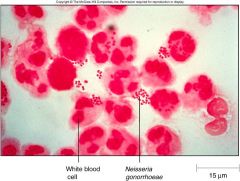
as a gram (-) diplococcus
chocolate agar |
|
|
how is Neisseria G transmitted?
how is it gaining resistance to antibiotics? |
Transmitted by direct contact (since it does not survive well outside of the host)
|
|
|
How does Neisseria G attach to host cells? |
via their pilli (fimbriae)
|
|
|
what allows for N. Gonorrhoeae to attach to many different types of cells? |
antigenic variation of pilli -different types of pilli can attach to different tissues types throughout boy |
|
|
how does N. Gonorrhoeae escape the immune system? |
antigenic variation- immune system cannot form antibodies (no future defense either)
It also produces an enzyme that breaks down IgA antibody. |
|
|
what is the main fxn of OPA proteins on the outer membrane of N. Gonorrhoea?
how do the OPA proteins prevent activation & proliferation of lymphocytes? |
fxn: increase adherence btwn gonococci & a variety of eukaryotic cells. |
|
|
what sxs are caused by gonorrhea in men? in women? What might be some end results for both sexes? |
men: uretheritis (pus) end result: sterility & prostatic abscesses
women: painful urination & vaginal discharge. (Spread in the cervix and fallopian tubes) |
|
|
How do you tx Gonorrhea? |
Ceftriaxone |
|
|
what other infection mimics gonorrhea (same symptoms)?
What does this organism attach to? (gonorrhea also does this) |
Chlamydia Trachomatis
attaches to sperm (^ this leads to PID & sterility)
|
|
|
what is lymphogranuloma venerem? |
Rare STD caused by 3 types of C. Trachomatis.
Lymph nodes in the groin swell & drain pus leading to gross swelling of the genitalia. |
|
|
4 types of C. Trachomatis can cause a chronic eye disease ___________ what does this lead to? |
Trachoma
can cause blindness! |
|
|
Main differentiation of Chlamydia from Gonorhea. |
Chlamydia is a spherical obligate intracellular bacterium
(relies on host cell for ATP, etc) |
|
|
what are the different phases of C. trachomatis?
|
1) elementary body-> non replicating, infectious
|
|
|
what form attaches to the receptor cells of the epithelium, is taken in via endocytosis, & releases cytokines (causing cell-mediated immune response)? |
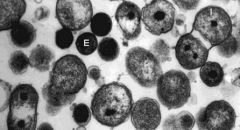
elementary body (dispersal form)
Once inside it germinates into a vegetative reticulate form. |
|
|
what form is contained w/i the endocytic vacole, replicates via binary fission, & expands/grows eventually leading to cell lysis (exocytosis)? |

reticulate body
Reverts back to elementary body before being released from cell via exocytosis
|
|
|
how do you diagnose C. trachomatis?
how do you tx it? |
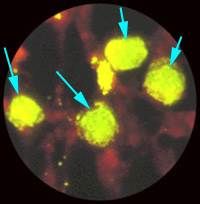
Immunofluorescence (antibody stain) *green apple bodies w/i cell |
|
|
What complication can arise if a mother w/ chlamydia has a vaginal birth? |
newborn may be infected--> conjunctivitis & pneumonia
tx: erythromycin |
|
|
what characterizes primary syphilis? |
painless, red ulcer w/ a hard rim called a hard chancre (heals after 3-6 wks).
10-90 days from exposure to appearance of 1st sxs. (usually at site of organism entry) |
|
|
Pt presents to your office with a runny nose, watery eyes, a sore throat w/ mucus patches inside mouth & a distinctive rash on palms and soles. Dx and tx |
dx: secondary syphilis (2-10 wk incubation)--> d/t immune complex formation
|
|
|
pt presents to your office complaining of difficulty coordinating muscle movements, paralysis, gradual blindness and a propensity for forgetting things (mental illness, stroke likely also). Pt also presented with a gumma on the roof of their mouth. Dx and tx |
dx: tertiary syphilis (Gumma- granulomatous necrotizing mass) |
|
|
Tertiary syphillis results from a hypersensitivity reaction to________________ & may result in DEATH |
Treponema pallidum |
|
|
how is syphilis transmitted? |
primary- chancre contact w partners body
secondary- rash sores (hands/feet) or mucus patches contain active bacteria
|
|
|
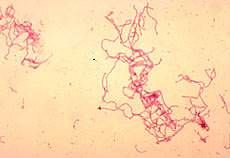
what causes syphilis?
how do you identify this pathogen? |
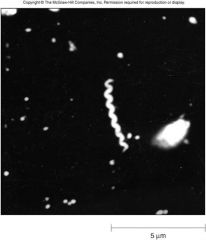
Treponema pallidum- motile spirochete |
|
|
what are the 2 non-specific serologic tests for syphilis? (ALWAYS do this if no chancre present)
what three conditions will give you a false positive? (false + are common, but if - can rule out) |
RPR (rapid plasma reagin) |
|
|
T/F RPR & VDRL are used to identify the presence of syphillis organism in a serologic culture |
FALSE
do not detect the actual organism, only detect tissue damage |
|
|
what is the purpose of quantitative, nonspecific tests for syphilis? |
monitor efficacy of tx... ab titers decreased w/ successive txs
(check Ab levels) |
|
|
Once you have a (+) RPR of VDRL, you MUST do a confimatory test for syphillis.
What are the 2 specific treponemal antibody confirmatory tests? why can't u use these tests to follow therapy? |
FTA-ABS (fluorescent treponemal antibody absorption) |
|
|
what pathogen causes chancroid (genital ulcer disease, GUD)? |
Haemophilus ducreyi
--> gram (-) bacillus, produces cytolethal, distending toxin
|
|
|
Pt presents to your office with a soft chancre that is painful, but not indurated.
Dx? what is this dx associated with? |
dx: chancroid
assoc w/ unilateral, inguinal, lymphadenitis--> untxed buboes can form), chancres rupture & form ulcer but do NOT heal |
|
|
(males/females) w/ chancroid are usually asymptomatic.
If symptomatic, how do pts present? |
females- usually asymptomatic, but can present w/ sxs such as dysuria, vaginal discharge, painful defecation, rectal bleeding.
males- symptomatic painful lesions & inguinal tenderness |
|
|
What 3 factors are used to make a probable diagnosis of Chancroid (H. ducreyi)? |
-1 or more painful, genital ulcers - no evidence of T. pallidum (rule out syphillis chancre) - HSV are negative (rule out herpes sores) |
|
|
T/F |
FALSE |
|
|
what genital ulcer disease is the major co-factor in transmission of HIV (esp in Africa)? |
Chancroid
|
|
|
who common gets granuloma inguinale (Donovanosis)?
what pathogen causes it? |
commonly found in the tropics and subtropics (poor-- blacks 6x more than caucasians) |
|
|
what is the morphology of calymmatobacterium granulomatis?
where is it normally found?
what happens when it comes in contact w skin (genital)? |
gram neg, non motile capsular rod |
|
|
what is the key diagnostic feature of calymmatobacterium granulomatis? |
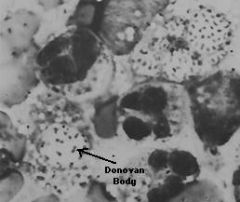
intracellular inclusions called donovan bodies
(w/i macriphageo |
|
|
What type of lesions are characteristic of calymmatobacterium granulomatis? |
lesions on the genitals & perianal regions
- start as raised nodules (look similar to chancroids) which erode into beefy-red ulcers |
|
|
what does the herpes virus encode that is an excellent target for antiviral drugs? |
DNA polymerase (promotes viral DNA replication)
(HSV is a dsDNA virus) |
|
|
what are the three immune escape proteins of the HSV genome?
What portion of the complement system and antibody are they bound to? |
gC, gE, gI |
|
|
pt presents to your office complaining of genital itching, burning and severe pain. On PE you notice small, red bumps on genitalia (some of which that have already turned into blisters). Dx and tx |
HSV |
|
|
T/F |
true
|
|
|
what happens when the herpes blisters/ulcers heal? |
the virus becomes latent in neurons, may reoccur (usually same location) due to stress, etc at any time
*blisters are extremely contagious (full of virions) |
|
|
what is the most common STD in the world?
what is it responsible for? |
HPV non-warty lesions of mucosal surfaces (uterine & cervical cancer) |
|
|
what is the pathogenesis of papillomavirus STDS? |
believed to enter and infect the deep layers of epithelial cells through abrasions. (result--> latent infections or immune system elimination)
(different strains cause different types^, many diff strains, not all STD (30 are, 15 assoc cancer) |
|
|
what can happen to newborn infants that are infected (not common) w/ HPV at birth ? |
warts can obstruct respiratory tract |
|
|
How is papillomavirus diagnosed & treated? |
Dx: usually abnormal pap- abnormal squamous epithelial cells
Tx: warts- removed w liquid nitrgoen virus- imiquimod |
|
|
what virus is associated w/ cervical cancer? |
HPV
(also assoc w/ anal & penile cancer)
(vaccine is only for some of the strains*) |
|
|
Pt presents to your office complaining of an itching vulva and vagina w/ yellowish-green, frothy vaginal discharge.
dx and what else might you see on PE? tx? |
trichomonas vaginalis- trichomaniasis |
|
|
T/F |
true |
|
|
What should you be concerned w/ if you find trichomonas vaginalis in a child? |
suspect for child abuse |
|
|
How can a trichomonas vaginalis be diagnostically confirmed? |
microscopically -large protozoan w/ characteristic jerky motility
(not automatically checked for or seen in vaginal sample- only seen under microscope, ASK) |
|
|
what are the three etiologic microorganisms that cause vaginitis? |
trichomonas vaginalis
candida albicans gardnerella vaginalis |
|
|
T/F Bacterial vaginitis is an STD |
FALSE
* can be infected non-sexually |
|
|
how can you cause bacterial vaginosis non-sexually? what accounts for 60% of vulvovaginal infections? |
- use of broad-spectrum antibiotics---60% (kills lactobacillus- normal flora, allows pathogens to live) |
|
|
what 4 signs characterize bacterial vaginosis? |
- clue cells- sloughed off epithelial cells covered w/ bacteria - strong fishy odor - itching, irritation |
|
|
how do you diagnose bacterial vaginosis?
|
observation and smell |
|
|
what would you expect to see on a microscopic stain of gardnerella vaginalis? |
clue cells |
|
|
what are the complications of bacterial vaginosis? |
PID
*recommend full STD screening if pt has this* |