![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
135 Cards in this Set
- Front
- Back
|
30.TMP11B30 New- Post delivery neonate did not breath post stimulation by midwife, not vigorous, heart rate drop from 140 to 90bpm. Next step of action |
ANSWER B
PPV aids in circulation transition |
|
|
84
TMP-Jul10-038 Chronic alcohol use. Which is not an associated complication ? A. Pancreatitis B. Atrial fibrillation C. Macrocytosis D. Nephrotic syndrome E. Hypertriglyceridaemia |
ANSWER D
|
|
|
55. New- 75yo patient seen for femoral bypass surgery, no significant cardiac risk factor. He will be admitted 3 days prior to operation. You decided NOT to start on beta blocker and you are justified because:
A. There is increase mortality and morbidity B. There is not enough time to safely start beta blocker C. The beta blocker may make the patient claudication worst D. ? |
ANSWER A
POISE TRIAL |
|
|
120. New- Pre eclamptic patient post LSCS continue on Mg infusion in ICU. Found to be in respiratory depressed. Next management is:
A. Calcium gluconate B. IV fluid C. Frusemide |
ANSWER A
From RWH Request magnesium level and review management if: * respiratory rate < 12 breaths/minute * urine output < 100mLs in 4 hours * loss of patellar reflexes * further seizures occur. Response to magnesium toxicity The following clinical signs of magnesium toxicity must be reviewed by a consultant obstetrician/anaesthetist: * urine output <100mL in 4 hours * absent patellar reflexes * respiratory depression. The antidote for magnesium toxicity is: calcium gluconate (10mL of 10% solution over 10 minutes) by slow intravenous injection. The patient requires ECG monitoring during and after administration because of the potential for cardiac arrhythmias. Resuscitation and ventilator support should be available during and after dose administration of both magnesium sulphate and calcium gluconate. |
|
|
100
EM37 ANZCA version [2001-Aug] Q57, [2002-Mar] Q52, [Jul06] Q81, [Apr07] (Similar reported question in [Apr96] [Aug96] [Apr97]) Systemic vascular resistance index (SVRI) is calculated from A. systemic vascular resistance multiplied by body surface area B. systemic vascular resistance divided by body surface area C. mean aortic and central venous pressure difference divided by cardiac output D. cardiac index divided by the mean aortic and central venous pressure difference E. none of the above |
ANSWER A
SVRI = SVR x BSA |
|
|
17. What is the correct order of Fat: blood coefficients? N2O, D, S, I
A. Des < N2O < Iso < sev B N20 < Des < sev < iso C N20 < des < sev~iso |
C
N2O 2.3 D 27 S 47 I 45 |
|
|
33. New- Patient with mastocytosis. Intraop they are likely to develop:
A. Severe hypertension B. Severe Hypotension C. Anaphylaxis D. Problems with rocuronium or vecuronium |
B
Other options not recollected, have been made up since. |
|
|
92
RH12b [Mar92] To operate on the anterior 2/3rds of the ear you would need to block: A. Mandibular n B. Maxillary n C. Vagus n D. Greater auricular n |
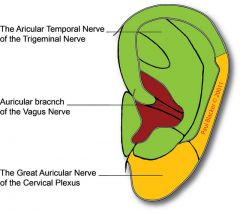
ANSWER A
|
|
|
48. AC62b ANZCA version [2003-Apr] Q144, [2004-Apr] Q98, [2004-Aug] Q44, [Jul06] Q23
The most commonly reported cause of awareness during general anaesthesia for a non-obstetric procedure is A. equipment failure B. human error C. lack of premedication D. recreational drug use E. the use of total intravenous anaesthesia |
ANSWER B
'In those events with a known cause the most common was the accidental delivery of insufficient volatile due to vapouriser or circuit problems' Awareness during general anaesthesia Anaesthesia 2002:57:549-56 |
|
|
58. AT27 [Apr07] Q108
Following a left sided pneumonectomy, a left intercostal drain is placed and connected to an underwater drainage system. In the postoperative period A. A leakage of air is expected from the drain B. The patient should be nursed in the right lateral decubitus position C. The underwater seal drain should be left on continuous free drainage D. The underwater seal drain should be left on continuous free drainage, and connected to wall suction for 5 minutes every hour E. The underwater seal drain should remain clamped and be released for a short period every hour |
ANSWER E
To prevent a sudden mediastinal shift presumably. |
|
|
80.IC90 Repeat- Trauma patient best indicator of good resuscitation (?)-
A. Lactate level B. Heart rate C. Blood pressure D Acidosis (?) |
ANSWER A
CEACCP 2006 Fluid & trauma Lactate: provide patient is young fit and well. Not in patient with liver failure |
|
|
35. New- Post epidural and LSCS, the next day patient have persistent paraesthesia anterior thigh. What other injuries would indicate more of nerve roots instead of peripheral nerve injuries
A. Weakness on hip flexion and thigh adduction B. Weakness on knee flexion and plantar flexion C. Urinary incontinence D. Foot drop |
ANSWER A
Paraesthesia anterior thigh suggest L2/3 nerve roots Hip flexion L1,2,3 Thigh Adduction L2,3,4 Knee flexion L5/S1 Plantar Flexion S1/2 Foot drop L4,5/S1 |
|
|
107 TMP-107 [Mar10] [Aug10]
Baby with Tracheo-oesophageal fistula found by bubbling saliva and nasogastric tube coiling on Xray. BEST immediate management? A. Bag and mask ventilate B. Intubate and ventilate C. position head up, insert suction catheter in oesophagus (or to stomach?) D. Place prone, head down to allow contents to drain E. Insert gastrostomy |
ANSWER C
|
|
|
89 TMP-Jul10-048
Amniotic fluid embolism. Cause of death in first half hour ? A. Pulmonary hypertension B. Malignant arrhythmia C. Pulmonary oedema D. Haemorrhage E. |
ANSWER A
first severe pulmonary vasoconstriction ,Rt ventricular failure ,then Lt ventricular failure and pulmonary oedema ,embolism is probably a misleading name,its actual pathology is anaphylaxis to foetal tissues |
|
|
66. New- The below would increase A-a oxygen gradient Except
A. Increase FIO2 B. Decrease FIO2 C. Decrease cardiac output D. Increase shunt |
ANSWER B
A-a gradient * increases 5-7mmHg for every 10% increase in FiO2 * increases with age * increases with increased shunt * V/Q mismatch * defect in diffusion |
|
|
ET03 [Repeat] Jehovah's witness refused blood- you have told him you refuse to do the surgery/anaesthesia for his own good. Ethical principle: |
ANSWER D? |
|
|
103
MC30b ANZCA version [2004-Aug] Q128, [2005-Apr] Q55 A patient with pulmonary hypertension secondary to lung disease presents for a laparotomy. Regarding this patient's anaesthetic management A. an alpha-agonist is the inotrope of choice B. hypothermia is protective against rises in pulmonary artery pressure C. isoflurane will tend to decrease pulmonary artery pressure D. ketamine is an appropriate anaesthetic agent E. right heart failure is not a concern |
A - alpha agonist is the inotrope of choice.
Strictly speaking alpha agonists are vasoconstrictors more than inotropes, but the word inotrope is used quite broadly often enough. Other answers are all false. |
|
|
14. Repeat- Child after gas induction, LMA insertion without IV cannula- desaturate to 90%. Next step of action?
A. Bag with LMA insitu B. Bag without LMA insitu C. IM suxamethonium D. IM atropine |
Ans B
Remove offending stimulus 100% O2 with CPAP, deep anaesthetic Optimize airway with gentle jaw thrust Morgani maneuver Drugs Propfol 0.5mg/kg Sux 0.5mg/kg atrop 0.2mic/kg IM sux if no IV Refractory latngospasm: SLN block, Transtracheal lig through cric mem |
|
|
50. New- Most common cause of paediatric post anaesthesia cardiac arrest
A. Drug error B. Respiratory cause C. Multifactorial D. Cardiac problem (?) |
Ans: D Cardiac
Anaesthesia & analgesia Aug 2007 vol 105 no 2 344-350 Pediatric Perioperative Cardiac Arrest (POCA) Registry from 1998 to 2004, 193 arrests (49%) were related to anesthesia. Medication-related arrests accounted for 18% of all arrests Cardiovascular causes of cardiac arrest were the most common (41% of all arrests) Hypovolemia from blood loss Hyperkalemia from transfusion of stored blood Respiratory causes 27% Airway obstruction laryngospasm |
|
|
45 AB50 ANZCA version [2005-Sep] Q120 |
Answer C |
|
|
41. Post CEA on ward, patient seizes. BP has been hard to control. What to do to prevent further seizures?
A: Add another antihypertensive B: Start antiplatelet drugs C: Start anticonvulsants D: Do angio and stent E: Nimodipine |
ANSWER A
Eur J Vasc Endovasc Surg. 2011 Feb;41(2):229-37. Epub 2010 Dec 4. Cerebral hyperperfusion syndrome is a preventable cause of stroke after carotid endarterectomy (CEA). It manifests as headache, seizures, hemiparesis or coma due to raised intracranial pressure or intracerebral haemorrhage (ICH). There is currently no consensus on whether to control blood pressure, blood pressure thresholds associated with cerebral hyperperfusion syndrome, choice of anti-hypertensive agent(s) or duration of treatment. |
|
|
56. New- You see a man in his 60s in clinic 1 week prior to laparoscopic cholecystectomy. He has dilated cardiomyopathy with an ejection fraction of 30%, but does not get dyspnoeic with normal activities of daily living. What is the most appropriate management of his heart failure?
A. amiodarone 100mg bd B. digoxin 250mcg daily C. enalapril 2.5mg bd D. metoprolol 100mg bd E. diltiazem slow release 240mg daily |
ANSWER C
|
|
|
7. Repeat- Neonate to drug addicts found by grandmother in the house, brought into ed, mildly jaundice, slight tachycapnic. ABG PH 7.54, PaCO2 46, pO2 74, HCO 43
A. Septicaemic B. Pyloric stenosis C. Opiod overdose D. Meningitis E. Hepatitis |
ANSWER B
Both bicarb and Co2 moving in same direction, must be mixed disorder. Mixed metabolic alkalosis and respiratory alkalosis |
|
|
46. New- After transfusion of 5 unit of FFP what is least likely to occur
A. Haemolytic reaction B. Hypocalcaemia C. Infection D. Hyperkalaemia |
ANSWER D
A. FALSE: can occur if not matched B. FALSE: likely to occur if tranfused >1ml/kg/min C. FALSE: viral transmission possible D. TRUE: FFP does not contain potassium |
|
|
112 MC59b ANZCA version [2003-Apr] Q125, [2003-Aug] Q85, [2005-Sep] Q69, [Mar06] Q48 [Mar10] [Aug10]
In the management of torsades de pointes (polymorphic ventricular tachycardia), all the following drugs may be useful EXCEPT A. amiodarone B. isoprenaline C. [[lignocaine] D. magnesium E. phenytoin |
ANSWER A
Amioderone Contraindicated in torsades. |
|
|
AB58 ANZCA version [Jul07] Q141
A young woman with type 1 von Willebrand disease presents for a dilatation and curettage. She is a Jehovah's Witness. You consider administering intravenous desmopressin in an attempt to reduce haemorrhage. Which of the following statements regarding desmopressin is FALSE? A. it is a synthetic substance and is acceptable to Jehovah's Witnesses B. it is likely to reduce haemorrhage in this patient C. it should be given 30 minutes prior to surgery as an infusion D. its duration of effect is approximately 5 days E. the intravenous dose is 0.3 mcg.kg-1 |
ANSWER D
Elimination half life 2.4-4-4 hrs |
|
|
29. New- Subarachnoid haemorrhage patient. What percentage rebleed in the first 24hours
A. <5% B. 5-10% C. 10-15% D. 15-20% E. >20% |
ANSWER A
A is correct according to OHA 2nd Ed p408 - 4% risk of rebleed in 1st 24 hours Roughly 1% per day after 1st 24 hours. 30% in the first 28 days. |
|
|
ST19 ANZCA version [2002-Mar] Q62, [2002-Aug] Q59, [2005-Apr] Q58, [2005-Sep] Q50
A diagnostic test has a sensitivity of 90% and a specificity of 99% in detecting a certain disease. From this we can conclude that A. the false positive rate of this test is 1% B. the false negative rate of this test is 1% C. the positive predictive value of this test is 90% D. the negative predictive value of this test is 90% E. this test would be a useful screening test for this disease |
ANSWER A
Sensitivity = TP / (TP + FN) Specificity = TN / (TN + FP) Positive Predictive Value = TP / (TP + FP) Negative Predictive Value = TN / (TN + FN) False Positive Rate = 1 - spec False Negative Rate = 1 - sens False positive rate = FP / (TN + FP) = 1 – spec False negative rate = FN / (TP + FN) = 1 - sens |
|
|
85 TMP-Jul10-044 |
ANSWER E |
|
|
69. New- Interscalene block after injection of 2ml bupivacaine- patient seizure. Most likely injected to
A. Dural cuff B. Vertebral arteries C. Internal carotid arteries D. Jugular veins E. Subarachnoid (?) |
ANSWER B
|
|
|
136. Iron deficiency
A. decreased serum ferritin, increased serum iron B. decreased serum ferritin, absence of bone marrow iron C. decreased serum ferritin, normal serum iron D. increased serum ferritin, decreased serum iron E. increased serum ferritin, decreased total iron binding capacity |
ANSWER B
|
|
|
TMP-131 Repeat- Troponin can be detected for how long:
A. 1-3 Days B. 5-14 days C. 7-21 days D. >28 days |
5-14 Days
CEACCP Vol 8 no 2 2008 pg 62 Continuing breakdown of myofibrillary bound complex explains the prolong elevation of both troponins for up to 10 days after infarction. |
|
|
AT08c [Apr97] [Jul98] [2001-Apr] Q50, [2001-Aug] Q31, [2003-Apr] Q3, [2003-Aug] Q54, [2005-Apr] Q38, [Jul05] [Mar06]
The most appropriate method for improving oxygenation during one lung anaesthesia, after institution of an FiO2 of 1.0, is application of A. 5cm H2O CPAP to the non-dependent lung B. 10cm H2O CPAP to the non-dependent lung C. 5cm H2O PEEP to the dependent lung D. 5cm H2O CPAP to the non-dependent and 5cm H2O PEEP to the dependent lung E. intermittent re-inflation to the non-dependent lung |
A - CEACCP and group consensus
C if you want to go by Miller |
|
|
51. New- Post cervical spine op, there is bulging noted under the incision sit:E. Patient desaturated, combative, keep pulling off the oxygen facemask. Next course of action
A. Aspirate the collection with a 19G needle and syringe B. Awake fibreoptic intubation with minimal sedation C. Direct laryngoscopy and intubation after sevoflurane/O2 gaseous induction D. Direct laryngoscopy and intubation after propofol/suxamethonium induction E. Intubation via intubating LMA |
ANSWER C
CEACCP |
|
|
93
TMP-Jul10-054 Malignant hyperthermia. The number of people in the community at any given time with a predisposition is called the: A. Prevalence B. Incidence C. Occurrence D. Denominator E. Numerator |
ANSWER A
Incidence measures the rate of occurrence of new cases of a disease or condition. Prevalence measures how much of some disease or condition there is in a population at a particular point in time. Other options not recollected, have been made up since. |
|
|
71
E46 Mar2011 Acromegaly due to excess of growth hormone. Why hard to do direct laryngoscopy? A. Distorted facial anatomy B. Macroglossia C. Glottic stenosis D. Prognathe mandible E. Arthritis of the neck |
ANSWER B
|
|
|
118 MN38 ANZCA version [2004-Apr] Q124, [2005-Apr] Q100, [2005-Sep] Q94, [Jul07] [Apr08] [Aug08] [Aug09][Mar10] [Aug10]
Respiratory function in quadriplegics is improved by A. abdominal distension B. an increase in chest wall spasticity C. interscalene nerve block D. the upright position E. unilateral compliance reduction |
ANSWER B
|
|
|
138. A 62 year old man has chronic renal failure. You notice his total serum calcium is 2.05 mmol/L. This is because he has
A. high serum vitamin D B. hypoparathyroidism C. primary hyperparathyroidism D. secondary hyperparathyroidism E. tertiary hyperparathyroidism |
ANSWER D
|
|
|
82. New- Atrial-Septal Defect murmur is best heard at
A. ASD? B. Tricuspid valve C. Pulmonary valve D. Mitral valve E. Aortic valve |
ANSWER C
http://emedicine.medscape.com/article/162914-overview#showall Blood flow across the ASD does not cause a murmur at the site of the shunt because no substantial pressure gradient exists between the atria. However, ASD with moderate-to-large left-to-right shunts result in increased right ventricular stroke volume across the pulmonary outflow tract creating a crescendo-decrescendo systolic ejection murmur. This murmur is heard in the second intercostal space at the upper left sternal border. |
|
|
AC155 [Apr07]
A patient with severe COPD on home oxygen is having an excision of a submandibular tumour under local anaesthesia. The best way to prevent fire in the operating room is: A. seal the surgical site from the patients airway with adhesive drapes B. use bipolar instead of monopolar diathermy C. decr FIO2 to maintain sats 97% D. use alcoholic chlorhex instead of iodine E. add nitrous oxide to the inhaled gases to reduce the FiO2 and provide sedation |
ANSWER B
* A. seal the surgical site from the patients airway with adhesive drapes - potentially correct: "Oxygen is heavier than air, and can therefore accumulate * B. use bipolar instead of monopolar diathermy - definitely correct: "The cutting mode of diathermy is more likely to ignite fuels than the coagulation mode, and fires are more likely with monopolar diathermy than bipolar" (Muchatuta and Sale, Fires and explosions, Anaesth&IC, 2007, 8:11) * C. decr FIO2 to maintain sats 97% - almost certainly incorrect: " * D. use alcoholic chlorhex instead of iodine - definitely incorrect: "Alcohol-based antibacterial skin preparations are one of the more common causes of surgical fires since the withdrawal of flammable anaesthetic agents. * E. add nitrous oxide to the inhaled gases to reduce the FiO2 and provide sedation - definitely incorrect: "Nitrous oxide also supports combustion and is broken down to produce oxygen, nitrogen and heat." (Muchatuta and Sale, Fires and explosions, Anaesth&IC, 2007, 8:11) |
|
|
115
NN05 ANZCA version [2004-Aug] Q17, [2005-Apr] Q63, [Apr07] (Similar question reported in [1985] [Aug96] [Jul97] [Jul98]) The carotid sinus derives its nerve supply from the A. vagus nerve B. glossopharyngeal nerve C. ansa cervicalis (hypoglossi) D. middle cervical ganglion E. stellate ganglion |
ANSWER B
|
|
|
39
ECG- which does NOT have abnormal Q waves: A: Digoxin toxicity B: Anterior myocardial infartion C: Previous AMI D: LBBB E: Wolff-Parkinson-White syndrome |
ANSWER A |
|
|
75. Compared to retrobulbar block, peribulbar block is associated with |
No correct answer.
Retrobulbar: -Incr risk retrobulbar haem and optic n damage -Rapid akinesis -Doen't block CN VII (patient can close eye)
http://www.openanesthesia.org/retrobulbar_vs-_peribulbar_block/
|
|
|
2. Repeat- Main heat loss in anaesthetic for neonate |
ANSWER B |
|
|
96 TMP-Jul10-062 [Aug10]
In pregnancy the dural sac ends at: A. T12 B. L2 C. L4 D. S2 E. S4 |
ANSWER D
|
|
|
31. New- The safe maximal pressure for endotracheal cuff at the lateral side of the trachea
A. 0-10 cm water B. 10-20 cm water C. 20-30 cm water D. 30-40 cm water E. 40-50 cm water |
Ans C
AJCC 2011:20:109-118 <20 cmH2O increased chance of VAP >30 cmH2O impaired trancheal capillary perfusion |
|
|
126 AM41 ANZCA version [2004-Aug] Q15, [Mar06] Q11, [Jul07]
The most frequently reported clinical sign in malignant hyperpyrexia is A. arrhythmia B. cyanosis C. sweating D. tachycardia E. rigidity |
ANSWER D
The signs and symptoms of the acute episode are: * Increased CO2 production (the most sensitive indicator) * Tachycardia * Muscular rigidity * Increased body temperature (relatively late) * Metabolic and respiratory acidosis * Masseter spasm * Tachypnoea (if spontaneous respiration) Late signs are: * Complex arrhythmias * Cyanosis * Hypotension * Electrolyte abnormalities * Rhabdomyolysis Differential diagnosis (Ali et al, 2003 * Thyroid storm * Neuroleptic malignant syndrome * Iatrogenic overheating * Heat illness * Pheochromocytoma * Sepsis * Cocaine, ecstasy overdose * Hypoxic encephalopathy * Faulty equipment for measuring temperature, carbon dioxide * Intrathecal injection of inappropriate radiological contrast agent * Sudden cardiac arrest in a patient with occult myopathy |
|
|
104. New- Neonate desaturate faster than adult at induction because |
??? |
|
|
12. TMP-Jul10-036
Which is NOT a disadvantage of drawover vaporiser versus plenum vaporiser? A. Temperature compensation B. Cannot use sevoflurane C. Small volume reservoir D. Flow compensation E. |
B - Sevo can be used
Diadvantages 1. Poor temperature compensation (OMV suffer from a reduction in vapour ouput at lower temperatures) 2. Difficult to use sevoflurane (sevo requires high concentrations, therefore require extra wicks to maximise output, however loss of latent heat of vaporisation rapidly lowers its performance. Two OMVs are required to provide adequate sevo conc for induction) 3. Small volume reservior (OMV contains 50ml, which empties rapidly) 4. Basic temperature compensation 5. Less easy to observe spont vent with self inflating bag 6. cumbersome in paedatric use Advantages of draw over 1. easy to set up 2. in circuit 3. low resistance 4. mobile 5. non agent specific 6. no need for pressurized gas supply 7. robust, reliable 8. easily serviced |
|
|
Which is the best predictor of poor prognosis with aortic stenosis?
A. chest pain B. paroxysmal nocturnal dyspnoea C. syncope D. E. |
ANSWER B
Mean survival Onset of angina 2-4.7 yrs Onset of syncope 0.8-3.7 yrs Onset of heart failure 0.5-2.8 yrs (uptodate) |
|
|
106. New- Suxamethonium dosage higher in neonates compare to adult because
A. Increased volume of distribution B. Increased pseudocholinesterase activity C. More receptors D. Higher cardiac output (?) E. Decreased sensitivity of nicotinic ACH receptors to suxamethonium F. Faster diffusion away from neuromuscular junction |
ANSWER A
|
|
|
76. Repeat- Diastolic dysfunction Not caused by
A. Adrenaline B. Myocardial fibrosis C. Aortic stenosis D. Hypertension |
ANSWER A
Adrenaline increases the efflux of Ca, therefore aiding relaxation (lusitropy) |
|
|
10. New- Patient indicated for prophylaxis of infective endocardititis
A. amoxicillin orally 2 hours prior B. amoxicillin IV 1 hourly prior C. amoxicillin IV just before incision D. cefazolin IV 1 hour prior |
ANSWER C
Therapeutic Guidelines 2008 Prevention of endocarditis ORAL 1 hour before Amoxillin 2g orally or 50mg/kg Allergic to penicillin: Clindamycin 600mg orally or 20mg/kg OR Cephazolin 2g orally or 50mg/kg OR Azithromycin or Clarithromycin 500mg orally or 15mg/kg INTRAVENOUS just before procedure Ampicillin 2g IV or 50mg/kg Allergic to penicillin: Clindamycin 600mg IV or 20mg/kg IV OR Cefazolin or Ceftriaxone 1g IV/IM or 50mg/kg IV/IM IM 30 minutes before the procedure |
|
|
62.
SZ18b ANZCA version [2006-Mar] Q148, [Jul06] Q35 Infra-renal aortic cross-clamping usually results in A. decreased cardiac contractility B. decreased coronary blood flow C. decreased renal blood flow D. minimal change in cardiac output E. increased heart rate |
ANSWER C
Despite not being all that intuitive. |
|
|
24. Repeat- Finding on haemophilia A patient
A. Female haemarthrosis B. Male haemarthrosis C. Normal PT, abnormal APTT D. Abnormal PT, normal APTT |
ANSWER C
OHA 2nd ed pg 212 |
|
|
54. How can intraop hyperfibrinolysis be best diagnosed?
A. TEG B. PT C. APTT D. INR E. Clotting time |
ANSWER A
Aside: Euglobulin lysis time: test measures overall fibrinolysis. Mix citrated platelet poor plasma with acid in glass tube. This precipitate clotting factors, which is called euglobulin fraction. (fibrinogen, PAI-1, tissue plasminogen activator (tPA), plasminogen, factor VIII and some alpha 2-antiplasmin.) CaCl2 is added at 37C and fibrinolysis observed by eye or spectrophotometer as a function of optical density. |
|
|
During caesarean section a meconium stained floppy apnoeic baby is delivere:D. When the midwife gives you the baby, it is apnoeic, cyanotic with heart rate of 90 bpm. What do you do next
A. Give naloxone B. Dry and stimulate C. Start chest compressions D. Give positive pressure ventilation E. Suction the trachea |
E as per australian resus council
|
|
|
90. New- Post partum sudden collapse, suspected amniotic fluid embolism. The consistent finding is:
A. Low C3, C4 B. Increase complement C. Increase tryptase D. Increase histamine? E. petechial rash |
ANSWER A
CEACCP 2007 The suggestion that AFE may be related to anaphylaxis led Nishio and colleagues to measure tryptase concentrations. They reported concentrations of 67.2 ng ml-1 (normal ,10 ng ml-1). However, others have found normal tryptase but low complement concentrations |
|
|
131. New - When stimulating the ulnar nerve with a nerve stimulator, which muscle do you see twitch?
A. opponens abducens B. abductor pollicis brevis C. adductor pollicis brevis D. extensor pollicis E. flexor pollicis brevis |
ANSWER C
Ulnar nerve supplies the intrinsic muscles of the hand, except LOAF Lateral Lumbricals, Opponens pollicis, Abductor pollicis brevis, Flexor pollicis brevis |
|
|
47. Severe asthmatic- tachycapnia, HR120, speaking in words, pH 7.45, pCO2 46, pO2 96, HCO3 24. Then given nebulised salbutamol continuously, nebulised ipratropium bromide, and hydrocortisone- The next step:
A. Inhaled helium/oxygen B. IV aminophylline C. IV magnesium D. IVsalbutamol E. Intubation and ventilation |
ANSWER Magnesium
Updated choices from 2013A paper BTS/SIGN 2003 British guideline on the management of asthma Thorax 58 |
|
|
LUSCS for failure to progress. Spinal is inserted uneventfully. Next day the patient has foot drop. The most likely cause is?
A. epidural haematoma B. lumbosacral palsy C. sciatic nerve palsy D. common peroneal palsy E. ? |
ANSWER B
"Peripheral nerve lesions are usually associated with a long labour and the use of forceps" "Postpartum foot drop is caused by damage to the lumbosacral trunk or, less frequently, the common peroneal nerve. The lumbosacral trunk (L4, L5) is compressed between the ala of the sacrum and the descending fetal head. It may also occur during a forceps delivery. The result is a unilateral foot drop with loss of sensation and/or paraesthesia along the lateral calf and foot." "Common peroneal nerve damage may occur due to improper or prolonged positioning during lithotomy and the sensory deficit may be limited to the dorsum of the foot." Epidural haematomas extremely rare (1:168,000 from review in Anaesthesiology 2006; 105: 394)and obstetric palsies are much more common than complications related to neuraxial blocks. Sciatic nerve injury would cause a foot drop but would also affect knee flexion (hamstrings) and all muscles in lower leg and foot. Common peroneal nerve palsy less likely in this case as there is no mention of stirrups or 'excessive knee holding' |
|
|
111. Repeat- Best indicator of return function of laryngeal muscle
A. Sustained head lift 5 sec B. Sustained leg lift 5 sec C. TOF 0.9 D. DBS no fade E. Tetanus 50Hz |
ANSWER C
|
|
|
123 SG59 [Apr07]
Blunt liver trauma can be treated non surgically if A. No peritoneal signs B. Low Grade injury on CT scan C. Severe COPD D. Haemodynamically stable E. US confirms <500mls peritoneal fluid collection (i thought this was a paracentesis result) |
ANSWER D
|
|
|
60. New- Patient ingested 500mg/kg aspirin. In ICU, the most effective method to remove aspirin
A. IV fluid B. Haemodialysis C. Sodium bicarbonate infusion D. Frusemide |
ANSWER B
Alkalinization of the urine Sodium bicarbonate is given in a significant aspirin overdose (salicylate level greater than 35 mg/dl 6 hours after ingestion) regardless of the serum pH as it enhances elimination of aspirin in the urine. It is given until a urine pH between 7.5 and 8.0 is achieved. Dialysis Hemodialysis can be used to enhance the removal of salicylate from the blood. Hemodialysis is usually used in severely poisoned patients; for example, patients with significantly high salicylate blood levels [ 7.25 mmol/L (100 mg/dL) in acute ingestions or 40 mg/dL in chronic ingestions], or significant neurotoxicity (agitation, coma, convulsions), renal failure, pulmonary edema, or cardiovascular instability Hemodialysis also has the advantage of restoring electrolyte and acid-base abnormalities while removing salicylate |
|
|
97
TMP-Jul10-064 [Aug10] Pregnant woman presents with narrow complex tachycardia HR 190, stable BP 100/60. No response to vagal manoevures. Management? A. Adenosine 6mg B. DCR C. Amiodarone D. Atenolol E. ? |
ANSWER A
|
|
|
44. Repeat- Allergic question, which is true
A. Collect tryptase 8hours B. RAST test most sensitive/ specific C. Absent of trytase exclude anaphylactic D. Skin and intradermal test- sensitivity, specificity |
ANSWER D
Skin prick is easy to perform, safe and provides the best sensitivity/specificy combo. However it requires a skilled proceduralist Interdermal has higher sensitivity but higher anaphylaxis rate. RAST is 100% specific but only 75% senstive. Used to determine if pt has IgE antibodies to particular agents. It does not diagnoses anaphylaxis (as this requires 2 IgE to crosslink) |
|
|
36. Repeat- Nerve supply to the upper eyelid-
A. Ophthalmic branch of trigeminal and parasympathetic from ciliary ganglion B. Ophthalmic branch of trigeminal and sympathetic from superior collicus ganglion C. Maxillary branch of trigeminal and sympathetic from superior collicus ganglion |
B.
Other options not recollected at time of original question writing, and have been made up. |
|
|
ANZCA Version [Apr07]
Reverse splitting of the 2nd heart sound is caused by A. acute pulmonary embolism B. ASD C. complete LBBB D. severe MR E. pulmonary HT |
ANSWER C
Split during inspiration : Normal Split during expiration = Reverse splitting *Aortic stenosis *hypertrophic cardiomyopathy *left bundle branch block (LBBB) * ventricular pacemaker Split during both inspiration and expiration = fixed split S2 * atrial septal defect (ASD) * ventricular septal defect (VSD). |
|
|
102
PP84b ANZCA version [2005-Sep] Q141 Tracheo-oesophageal Fistula (TOF) A. is associated with cardiac anomalies in approximately 60% of cases B. is associated with oesophageal atresia in approximately 20% of cases C. is more common in males than females D. is usually left sided E. does not usually require contrast studies for diagnosis |
ANSWER E
A False association with cardiac lesion 25% B False: Association with oesophageal atresia 80-90% C False: Male to female apparently 1:1 D False: usually posterior aspect of trachea just proximal to carina E True Failure to pass a NG tube with the feeling of distal resistance at the blind end of the upper oesophageal pouch can confirm diagnosis. X-ray showing NG tube coiled in upper pouch. |
|
|
119.92. In severe asthma you may find:
A. Reduced BP on inspiration unlike normal (ie normally increased on insp) B. Reduced BP on inspiration exaggerated from normal C. Reduced BP on expiration unlike normal D. Reduced BP on expiration exaggerated from normal E. ? |
ANSWER B
Pulsus paradoxus is defined as an abnormally large decrease in systolic blood pressure and pulse wave amplitude during inspiration |
|
|
125. New- Compare to Myasthenia gravis, which signs/symptoms are more likely to represent Eaton Lambert syndrome?
A. Immune antibodies against post-synaptic ion channels B. Associated with thymoma C. Repeated exercise causes weakness to initially improve D. Good response to edrophonium E. Resistant to non-depolarizing muscle relaxants |
C - repeated exercise causes EL syndrome to improve.
Updated with 2013A choices (stem still recalled differently) EATON LAMBERT SYNDROME Myasthenic syndrome Definition: autoimmune NM disorder characterized by IgG Ab to pre-synaptic Ca channels and decreased ACh release •Associated with malignancy 50-60% •Small cell lung Ca CLINICAL •Proximal muscles weakness, esp lower limbs •Strength improves with activity •Although 30% demonstrate fatigability •Myalgia •Tendon reflex is absent •Ocular/bulbar dysfunction •Autonomic dysfunction ANAESTHETIC IMPLICATIONS •Sensitive to both sux and NDMR TREATMENT •Not reverse by anticholinestases •Immunosuppression with steroid •Plasma exchange |
|
|
133. New - Advantages of off-pump CABG over on-pump CABG
A. decreased transfusion rate B. decreased mortality C. decreased cost D. increased graft patency E. less cognitive impairment F. less stroke |
ANSWER A
CEACCP Hett 2006 Most studies showed no difference in mortality and morbidity. National Adult Cardiac Surgery Database UK Mortality reduced from 2.9% -> 2.3% and complication rate 12% -> 8% Transfusion: Most studies showed a reduction in transfusion and other blood products Effect of extracorporeal circulation and hypothermia affect both platelets and COAG factors Stroke incidence is less in OPCAB in isolated studies. Inflammatory markers rise is reduce in OPCAB C3a, C5a, TNF alpha, IL6&8 AF incidence is the same |
|
|
4. Child with murmur- what would make it more likely for you to investigate if you heard the murmur
A. Loudness 4/6 B. Decreases on inspiration C. Vibratory quality D. Ejection systolic murmur E. Louder on supine |
A
Updated with 2013A choices EXCLUDE ON HISTORY •Good exercise tol/playing •No sig fam hx: HOCM, CCD, sudden unexplained death •No sig perinatal hx: prematurity, maternal diabetes, foetal distress, birth asphyxia •No syndromes or congenital defects •Child >1 yr EXCLUDE ON EXAM •No dysmorphic features, VACTERAL •No thrill •Apex not displaces •Soft, grade <3 •Short duration •No radio-fem delay or rad-rad delay •Femoral pulse not bounding (L-R shunt) or decrease LVOTO •No cyanosis •Diastolic, pansystolic, continuous or very load need investigation |
|
|
34. Repeat- Complication of celiac plexus block
A. Hypertension B. Failure of erection C. Constipation D. Paraplegia E. L3,4 lumbar pain |
ANSWER D
Complications •Severe hypotension may result, even after unilateral block. •Local pain during procedure •Diarrhoea •Intramuscular injection into the psoas muscle. •Bleeding due to aorta or inferior vena cava injury by the needle. •Intravascular injection (should be prevented by checking the needle position with radio-opaque dye). •Upper abdominal organ puncture with abscess/cyst formation. •Paraplegia from injecting phenol into the arteries that supply the spinal cord (prevented by checking the needle position with radio-opaque dye). •Lumbar nerve root irritation (injected solution tracks backwards towards the lumbar plexus). • Sexual dysfunction (injected solution spreads to the sympathetic chain bilaterally) = inability to ejaculate •Pneumothorax •Shoulder/chest/pleuritic pain/hiccupping – diaphragmatic irritation •Haematuria from renal pouncture |
|
|
87. New- Apnoeic oxygenation in obese patient can be increased by
A. Sniffing position B. Prone C. Supine D. Lateral E. Head up |
ANSWER E
Increase FRC allow gravity to shift the weight away from upper torso |
|
|
PZ130 Which drugs below does not need dose adjustment in renal failure patient
A. Buprenorphine B. Morphine C. Tramadol D. ? E. ? |
ANSWER A
|
|
|
135. New - A 60 year old man 24 hours post CABG is confused, oliguric, with BP 80/40, pulse 120. The most appropriate and useful investigation is
A. electrocardiogram B. echocardiogram C. chest x-ray D. arterial blood gas E. coronary angiogram |
ANSWER B
|
|
|
59.RB53 Repeat- Post dural punture headache
A. 24hour bed rest is recommended B. Prone position is worst C. There is an increase incidence with insertion of spinal catheter D. Hearing loss can occur |
ANSWER D
|
|
|
52. New- What drug known to cause prolong QT and risk of Torsades de Pointes
A. Metoclopramide B. Droperidol C. Tranexamic acid D. Magnesium E. Ondansetron |
ANSWER B
Known to occur in neuroleptic-type doses |
|
|
124 AZ (Q120 Aug 2008) Preoperative assessment shows a malampati (ML) score of III and thyromental distance (TMD) of < 6cm. A grade 3 to 4 on Cormark and Lehanes is predicted. Compared to the ML score, the TMD is:
A less sensitive, less specific B less sensitive, more specific C more sensitive, less specific D more sensitive, more specific E equal sensitivity an specificity |
ANSWER B
Evidence based practice of anaesthesiology pp 104-8 Mallampati classification with Samsoon and young modification Sensitivity 60-80% Specificity 53-80% Thyromental distance by Patil 1983 <6 cm possible difficult intubation (many authors consider less sensitive than Mallampati but not really when looking at numbers) Sensitivity60-80% Specificity80-90% Combine Mallampati > grade III + TMD < 6 cm Sensitivity71-80% Specificity92-98% |
|
|
128 PR04 ANZCA version [1985] [Mar95] [Apr97] [Jul97] [Apr98] [Jul98] [2002-Aug] Q11, [2003-Apr] Q39, [2005-Sep] Q46, [Mar06] Q25
The percentage of the population which is heterozygous as regards pseudocholinesterase, thus having a dibucaine number between 30 and 80, is A. 0.04% B. 0.4% C. 4.0% D. 14.0% E. 40.0% |
ANSWER C
|
|
|
91 TMP-Jul10-049
The EARLIEST sign of hypocalcaemia is: A. Tingling of face and hands B. Chvostek’s sign C. Carpopedal spasm D. ? E. ? |
ANSWER A
CATS go numb (Convulsions, Arrythmias, Tetany and numbness/parasthesias in hands, feet, around mouth and lips) |
|
|
11. Circuit disconnection during spontaneous breathing anaesthesia
A. will be reliably detected by a fall in end-tidal carbon dioxide concentration B. will be detected early by the low inspired oxygen alarm C. will be most reliably detected by spirometry with minute volume alarms D. may be detected by an unexpected drop in end-tidal volatile anaesthetic agent concentration E. can be prevented by using new, single-use tubing |
ANSWER D
A. FALSE: Gas analyzer is still connected to patient despite disconnection of circuit, therefore ETCO2 will be normal B. FALSE: Disconnection allows entrainment of room air which will not be detected by low inspired O2 alarm C. FALSE : Depends where the spirometry is taken from, but some spirometry taken near the filter and so a disconnect at the machine will not be detected D. TRUE : Any disconnect will allow entrainment of room air into the circuit and allow escape of the volatiles, thus a drop in the ET-agent. E. FALSE: Single use tubing will not prevent a disconnection. Apnea/disconnect alarms may be based on 1. Chemical monitoring (lack of end tidal carbon dioxide) 2. Mechanical monitoring * Failure to reach normal inspiratory peak pressure, or * Failure to sense return of tidal volume on a spirometer 3. Visual monitoring * Failure of standing bellows to fill during mechanical ventilator exhalation * Failure of manual breathing bag to fill during mechanical ventilation (machines with fresh gas decoupling- the Apollo, Fabius GS, Narkomed 6000) 4. Auditory monitoring - lack of breath sounds in precordial, lack of sound from ventilator cycling, etc. 5. Optic monitoring - Failure of the hanging bellows to fill completely (the "garage door" electronic eye sensor on the Julian) |
|
|
122. Repeat- How to estimate weight in child-
A. (age x 4) + 2 B. (age + 4) x 2 C. (Age x 2) + 4 D. (Age + 2) x 2) |
B - (Age + 4) x 2
One way to remember is the answer has to equal 10kg at one year of age UK APLS group - (Age+4) x 2 Can underestimate in today's fat kids. |
|
|
63. Repeat- The most effective method for cerebral protection in aortic arch aneurysm repair
A. Systemic hypothermia 20degrees B. Antegrade perfusion to carotid arteries C. Retrograde perfusion to jugular veins D. Thiopentone E. Steroid (?) |
ANSWER A
|
|
|
109
SF89 [Mar10] Most likely change on CTG with anaesthesia for non-obstetric surgery at 32 wks: A. Loss of beat to beat variability B. No change C. Late decelerations D. Variable decelerationss E. Uterine contractions |
ANSWER A
# Normal CTG under GA = Loss of beat to beat variability, no decelerations. # Normal CTG under neuraxial block without sedation = No change |
|
|
32. Repeat- Allergy to penicillin- cross reaction to neuromuscular blocker
|
?
Penicillin allergy increases rate of neuromuscular blocker allergy. Cis and atracurium have lowest allergy rates Roc and sux have highest |
|
|
PZ128 Patient on cisapride. What drug NOT to give in recovery?
A. Tramadol B. ? C. ? |
Tramadol apparently is safe
Cisapride is a prokinetic *agonist at muscarinic (M2) and some serotonergic (5HT4) receptors, and as an antagonist at other serotonergic (5HT3) receptors. *increases SM tone, strength and co-ordination Risk of Prolong QTc *inhibit K+ channels *higher doses * reduced metabolism via Cytochrome P450 (e.g. macrolides, azole antifungals, grapefruit juice) * other QTc drugs (e.g. quinidine, sotalol). |
|
|
73
Stellate ganglion block associated with all except: A. Ptosis B. Miosis C. Sweating D. Facial flushing E. Nasal stuffiness |
ANSWER C
Stellate Ganglion produces Horners syndrome * Ptosis * Miosis * Anhidrosis In addition, several other eye signs are present: * Conjunctival injection * Lacrimation |
|
|
88
MN21 [1985] [1986] [1987] [1988] [Mar93] [Apr98] (type A) Which of the following is NOT a feature of long-standing paraplegia above T6? A. Flaccidity of the leg muscles B. Poikilothermia C. Mass autonomic reflex D. Hyperkalaemia after Suxamethonium administration E. Labile blood pressure |
ANSWER A
|
|
|
129 ST22 ANZCA version [2002-Aug] Q81, [2004-Apr] Q88, [2004-Aug] Q78
Recognised weaknesses of systematic reviews include all of the following EXCEPT A. publication bias B. duplicate publication C. study heterogeneity D. inclusion of outdated studies E. systematic review author bias |
ANSWER E
|
|
|
68. Repeat- Patient cough during interscalene block- insertion needle should be directed-
A. Anterior B. Posterior C. Medially D. Laterally E. No change required |
ANSWER posterior
Stimulation of diaphragm : phrenic nerve : needle tip is anterior to plexus Stimulation of trapezoid : needle tip is posterior to plexus |
|
|
137. New - Why should NSAIDs be avoided in pregnant women >30 weeks gestation?
A. cause neonatal acute renal failure B. increased antepartum haemorrhage C. increased rate of pre-eclampsia D. cause closure of the fetal ductus arteriosus E. increase preterm labour |
ANSWER D
|
|
|
EZ93 What is the chemical used in sodalime to indicate exhaustion?
A. ethyl violet B. potassium permanganate C. Methyl red D. Litmus E. Hydroxyperchlorate |
ANSWER A
Components of Sodalime NaOH 5% Ca(OH)2 94% Water Ethyl violet as indicator Binders |
|
|
22. New - 72 year old has had hip replacement surgery and 3 days postop has a pulmonary embolus. He is fully heparinised, but still dyspnoeic, clammy, BP 80/40, pulse 120 and CVP 18. The most appropriate next step is |
Ans: C |
|
|
18. Intravascular thrombosis is common in:
A. HITTS type 1 B. HITTS type 2 C. Haemophylia A D. Von-willebrand disease |
HITTS type 2
Other options not recollected at time of original question writing, and have been made up (and the question stem was as well) |
|
|
SF53 ANZCA version [2001-Apr] Q6, [2001-Aug] Q4, [2003-Aug] Q66, [2004-Apr] Q55, [Mar 10],[Aug10]
Carbon dioxide is the most common gas used for insufflation for laparoscopy because it A. is cheap and readily available B. is slow to be absorbed from the peritoneum and thus safer C. is not as dangerous as some other gases if inadvertently given intravenously D. provides the best surgical conditions for vision and diathermy E. will not produce any problems with gas emboli as it dissolves rapidly in blood |
ANSWER C
|
|
|
49. New- There is evidence to avoid BIS <40 for more than 5minutes because
A. Safe cost B. Increase incident of hypotension C. Increase post op mortality D. Decrease volatile (?) for poor cardiac output patient E. Decrease the incidence of awareness |
ANSWER C
The effect of bispectral index monitoring on long-term survival in the B-Aware Trial. Anesth Analg 2010 BACKGROUND: When anesthesia is titrated using bispectral index (BIS) monitoring, patients generally receive lower doses of hypnotic drugs. Intraoperative hypotension and organ toxicity might be avoided if lower doses of anesthetics are administered, but whether this translates into a reduction in serious morbidity or mortality remains controversial. The B-Aware Trial randomly allocated 2463 patients at high risk of awareness to BIS-guided anesthesia or routine care. CONCLUSIONS: Monitoring with BIS and absence of BIS values <40 for >5 min were associated with improved survival and reduced morbidity in patients enrolled in the B-Aware Trial. |
|
|
57.EZ80 Repeat- A line isolation monitor protects against microshock
A. only if the warning current is set at 10mA B. only if the warning current is set at 30mA C. under no circumstances D. only if the equipment used is grounded E. only if it monitors all the equipment in the region |
ANSWER C
|
|
|
74. Repeat- Most safe side to insert subtenon block
A. Inferonasal B. Inferotemporal C. Medial D. Superonasal E. Superotemporal |
ANSWER A
A review of subTenon's block: current practice and recent development EJA 2005 Access to the space by the infer-onasal quadrant is the commonest approach described because the placement of the cannula in this quad-rant allows good fluid distribution superiorly while avoiding the area of surgery and reducing the risk of damage to the vortex veins Access to all other quadrants have been reported and are essentially similar in principle, such as super-otemporal by Fukasaku and Marron [18], superonasal and inferotemporal by Roman and colleagues [8] and the medial canthal side by Ripart and colleagues [19]. |
|
|
27. New- An elderly lady has a closed neck of femur fracture and presents to ED. She is in chronic AF and on warfarin. INR is 2.6 and she is not bleeding. It is 9am and she is scheduled for repair the following day. According to current guidelines, how should her warfarin be reversed?
A. Prothrombinex 25IU/kg immediately and then 2 units FFP immediately prior to surgery B. No immediate treatment then 2 units FFP immediately prior to surgery C. Vitamin K 1mg IV immediately D. Vitamin K 10mg IV immediately E. Withhold warfarin |
ANSWER C
MJA vol 181 no 9 nov 2004 pg 496 It is night before surgery: if INR >2 give 1-5 mg Vit K1 iv INR <1.5 = proceed with surgery URGENT SURGERY INR <1.9 FFP INR <5.0 FFP + Vit K 1-3mg slow IV INR < 9 FFP Vit K 2-5mg slow IV SEMI URGENT INR <1.9 Vikt K 1mg oral INR< 5.0 Vit K 1.25mg oral, repeat INR INR <9.0, Vit K 2.5-5.0mg, repeat INR ELECTIVE SURGERY Bridging therapy if high risk of VTE Risk factors 1. Acute thrombosis, on treatment > 1month 2. Mechanical heart valve 3. Severe myocardial dysfunction 4. Atrial fibrillation Acute thrombosis <1month IVC filter |
|
|
81. New- Pregnant patient seatbelt, driver- involved in car accident. Suddenly developed severe central chest pain, HR 110, BP 154/80, RR 26, Sat 100%. The most likely cause?
A. Sternal fracture B. Aortic dissection C. Pneumothorax D. Rib fracture E. Myocardial infarction |
ANSWER B
|
|
|
130 AA22 ANZCA version [2005-Apr] Q106
The commonest initial presenting feature in anaphylaxis is A. coughing B. desaturation C. hypotension D. rash E. wheeze |
ANSWER C
|
|
|
79. A volume of fully water-saturated air at 20 degrees is heated to 37 degrees. What will the relative humidity be?
A. 40 % B. 44 % C. 17% D. (20/37) x 100% |
A - ~40%
Absolute humidity @20deg 17g/m^3 - this is how much water in in the air in this example @37deg 44g/m^3 17/44 = 40% |
|
|
127 RH26b ANZCA version [2004-Apr] Q126, [Jul07]
To achieve maximum anaesthesia with minimal risk of trauma to veins, the tip of a needle used for a medial peribulbar injection should be advanced no further past the equator of the globe than A. 5 mm B. 10 mm C. 15 mm D. 20 mm E. 25 mm |
ANSWER B
Equator of the globe is ~10-15 mm measured from the anterior aspect of the globe. (Axial length 21-27 mm) The tip of the needle should be extraconal, close to the orbital wall beyond the equator of the globe; but should stay anterior to the posterior border of the globe, in the peribulbar space. The usual needle depth is 15-20 mm. Medial canthus approach usually <15 mm. Absolute maximum depth is 25 mm inferior lateral. (NYSORA) Therefore usually up to 5 mm pass the equator definitely less than 10 mm. |
|
|
99 MC157 [Mar10] [Aug10]
An 18 yo with Fontan circulation undergoing exploratory laparotomy. On ICU ventilation, saturation is 70%. Which ventilator parameter would you INCREASE to improve his saturation? A. Bilevel pressure B. Expiratory time C. Inspiratory time D. Peak inspiratory pressure E. PEEP |
ANSWER B
CEACCP 2008 Low respiratory rates, short inspiratory times, low PEEP, and tidal volumes of 5 – 6 ml kg-1 usually allow adequate pulmon-ary blood flow, normocarbia, and a low PVR. |
|
|
9. Patient with aortic stenosis, the signs indicate poor prognosis
A. Palpitation B. Radiation to carotid arteries C. Something about characteristic of murmur |
CEACCP Vol 5 no 1 2005 pg 2 Precordial thrill is reasonably specific for severe aortic stenosis
Normal 2.6-3.5 cm Mild 1.2-1.8 cm12-25 mmHg Moderate 0.8-1.2 cm25-40 mmHg Severe 0.6-0.8 cm40-50 mmHg Critical <0.6 cm>50 mmHg Signs of severity 1. Weak plateau pulse 2. Small pulse pressure 3. Late peak systolic murmur 4. Reverse splitting S2 5. S4 6. Signs of LVH |
|
|
108 NV42 [Apr07] [Jul07]
What does C6/7 motor function do? A. flex/extension of fingers B. flex /extend wrist C. shoulder ext rotation / abduction D. elbow pronation/supination E. flexion at elbow |
ANSWER B
|
|
|
40 The QT interval may be prolonged by each of the following EXCEPT
A. high intra-thoracic pressure B. hypothermia C. magnesium sulphate D. suxamethonium E. volatile anaesthetic agents |
ANSWER C
|
|
|
16. Repeat- Which herbal supplement reacts with tramadol?
A. Ephedra B. St John's wort C. Royal jelly D. Ecinacea |
ANSWER B
Ephedra: cardiovascular instability: hypertension, angina acutely and catechol depletion chronically. St J Wort: P450 induction. Interaction with tramadol. Increased sensitivity to anaesthesia. Very important is the induction of metabolism of immunosuppressants, antiretrovirals and anticonvulsants. |
|
|
134. New - After coronary artery bypass graft surgery, the FRC is
A. increased 40% B. increased 20% C. unchanged D. decreased 20% E. decreased 40% |
ANSWER D
Determinants of pulmonary function in patient undergoing coronary bypass operations 1990 The annal of thoracic surgery At discharge, lung volumes were decreased by 19-33% below preoperative values. (did not specify FRC) |
|
|
43
SG62 [Jul07] Patient presents with carcinoid syndrome and developes hypotension intraoperatively. Best drug to treat it is: A. Noradrenaline B. Adrenaline C. Metaraminol D. Octreotide E. Ephedrine |
ANSWER D
the occurrence of intraoperative carcinoid crisis manifesting as bronchospasm or hypotension is treated with IV octreotide 100-200 mcg...Stoelting...drstitch 2013A stem is a bit different. Ocreotide has already been given. Answer for that one is vasopressin |
|
|
26. Repeat- 36yo male with sickle cell anaemia Hct 0.3 with close foot fracture, what is true?
A. The patient should be transfused 2 pint packed cell pre-op B. A spinal can be done safely C. Extended coagulation profile is required D. A sickle cell crisis should be treated with high flow oxygen |
ANSWER B
OHA 2nd ed regional can be safely done Transfusion usually done with consultation with haematologist. CEACCP vol 10 no1 2010 pg 26 Traditionally aim HbS <30% it is no longer routine. If more aggressive approach required consultation with haematologist. |
|
|
132. New - When intubating over a bougie / awake fibreoptic, which direction do you rotate the tube to stop it catching on structures in the glottis
A. no change from normal B. 90 degrees clockwise C. 90 degrees counterclockwise D. 180 degrees E. try either direction |
ANSWER C
|
|
|
53. New- During cardiac catheterisation (?) patient become BP 80/60, HR 110, CVP 16. What is the next most important investigation
A. Echocardiogram B. CXR C. Electrocardiogram D. CT Angiogram |
ANSWER A
American heart Journal 140 (2),Aug 2000, p 279-283 (ref below), some support for tamponade as the culprit with ECHO the next step. "We found that the incidence of tamponade, commonly regarded as a very rare complication of balloon angioplasty, is much higher in the era of newer interventional devices...The presence of hypotension associated with chest pain, dizziness, or bradycardia is not surprising in the setting of tamponade. However, these symptoms alone or in combination often occur after coronary interventional procedures for various reasons. An appropriate index of suspicion is required, and we advocate immediate echocardiography in these situations...Echocardiography can be done within minutes, while the patient is on the catheterization table, and is highly accurate. Echocardiography-guided pericardiocentesis may be performed at the same time with a high degree of success." |
|
|
28. Repeat- Marfan syndrome. is associated with all EXCEPT-
A. Mitral valve prolapse B. Astigmatism C. Aortic stenosis D. Conduction abnormalities E. Dural ectasia |
C. Aortic stenosis
Cardiac Manifestations MVP AR Aortic dissection Conduction abnormalities |
|
|
19. Repeat- Half life of tirofiban?
A. 1 hour B. 2 hours C. 4 hours D. 6 hours E. 8 hours |
B - 2 hours
|
|
|
TMP-104 [Mar10] [Aug10]
Stellate ganglion A. Anterior to anterior scalene B. Posterior to medial scalene C. Inferior to medial scalene D. ? E. ? |
ANSWER A
|
|
|
38 ANZCA Version [Jul07]Q.150
You are asked to see a 60 y.o. male 2 days following a cervical laminectomy because he has new new neurological symptoms in his right arm. The surgical team think these may be due to poor patient positioning. The sign that would most help differentiate c C8-T1 nerve root injury from an ulnar nerve injury is A. loss of sensation in the index finger B. loss of sensation in the little finger C. weakness of the abductor digiti minimi muscle D. weakness of the abductor pollicis brevis m E. weakness of the first dorsal interosseous m. |
ANSWER D
A. FALSE: neither ulnar nerve or C8T1 supply, therefore non differentiating B. FALSE. both ulnar and C8T1 supply therefore non differentiating C. FALSE: both affected by C8T1 and ulnar therefore non differentiating D. TRUE: T1 and median nerve supply, but ulnar does not E. FALSE. both supplied by c8T1 and ulnar nerve therefore non differentiating |
|
|
110. All indicate autonomic neuropathy EXCEPT for:
A. Sinus arrthymias B. Gastric reflux C. Postural hypotension |
ANSWER A
|
|
|
21. The depth at the lips of an ETT for a neonate should be:
A. 8.5cm B. 9.5cm C. 10.5cm D. 11.5cm E. 12.5cm |
Under 1 yr:
weight (kg) + 6cm at mouth, or + 8cm at nose Term (3.5kg): 9.5cm/11.5cm 6 month 11cm/13cm 1yr 12cm/14cm Over age 1 Age/2+12 for lips, +15 for nose |
|
|
101. New- Young pregnant patient with moderate mitral stenosis, normal LV function. The best delivery method
A. Epidural anaesthesia LSCS B. Spinal with LSCS C. Epidural analgesia and normal vaginal delivery D. GA LSCS E. Normal vaginal delivery with remifentanil PCA |
ANSWER C
CAECCP 2009 Management of cardiac disease in pregnancy Vaginal delivery is the preferred mode of delivery for most women with heart disease, unless there are specific obstetric indications or deterioration in cardiac performance necessitating early delivery. MS is a fixed output valvular disease -transmitral gradient is proportional to CO squared, therefore increasing CO by 50%, will increase the gradient 2.3 fold -generally pregnancy will increase NYHA class by One Aims are to keep the patient at they are -maintain preload -normal HR -maintain afterload MS should be evaluated before pregnancy -prophylactic percutaneous mitral balloon valvotomy -NHYA 2-4 or high PTH high risk of complications and death Treat antenatal with diuretic and beta blockers -care should be taken to avoid hypovolaemia -ACEI are contraindicated in pregnancy Labour and post partum are the most dangerous times -Epidural to blunt sympathetic response (attenuate HR, CO, therefore minimised increasing transmitral gradient) -Most delivery, sudden increase in preload with autotransfusion can lead to APO -Cautious use of Syntocinon during 3rd stage. Vasodilation can cause hypotension with compensatory tachycardia leading to overdistention of LA (due to MS) and AF => APO -AF should be electrically cardioverted. |
|
|
5. Repeat- Single lumen intubation after multiple attempts of difficult intubation, you put in a bronchoscope after and the tip is in the trachea. The structure B you seen corresponding to?
|
Trachealis is posterior, use this to orientate
|
|
|
86
TMP-Jul10-045 How quickly does the CO2 rise in the apnoeic patient ? A. 1 mmHg per min B. 2 mmHg per min C. 3 mmHg per min D. 4 mmHg per min E. 5 or ?8 mmHg per min |
ANSWER C
From Miller, 1st minute Co2 increases by 6 mm Hg all subsequent minutes 3 -4 mm Hg |
|
|
105. New- The cause of hypoxia in one lung ventilation
A. Blood flow through non ventilated lung B. Impairment of hypoxic pulmonary vasoconstriction C. Ventilation perfusion mismatched (?) |
ANSWER A
|
|
|
98
Which patients do not get pulmonary hypertension a. ASD b. Chronic thromboembolism c. Tetralogy d. MR e. MS |
ANSWER C
The 4 features typical of tetralogy of Fallot include: 1.right ventricular (RV) outflow tract obstruction (RVOTO) (infundibular stenosis), pulmonary artery stenosis 2.ventricular septal defect (VSD), 3.aorta dextroposition/over-riding aorta (deviation of the aortic origin to the right) 4.Right ventricular hypertrophy. |
|
|
70. New- Post intubation, you manual ventilate and noted patient high airway pressure. What would you do next
A. Open the APL valve B. Auscultate the lung C. Switch to ventilator |
ANSWER B
|
|
|
113. New- A nulliparous woman in labour for 8 hours with epidural analgesia has a fever 37.6 degrees. The most likely reason for this is
A. altered thermoregulation B. chorioamnionitis C. urinary tract infection D. inflammatory response E. neuraxial infection |
ANSWER D
Epidural associated fever is common, ranging from mild hyperthermia to overt fever. Risk Factors 1. Nullparious 2. Prolonged labor 3. PROM Mechanisms postulated 1. Inflammation: most accepted explanation, unknown if it is infectious or non infectious (women with fever and epidural do not have evidence of chorioamonitis on histology) 2. Altered thermoregulation: hyperventilation during labor is diminished, resulting in reduced heat loss. 3. Effect of opioids: opioids suppress IL-2 formation www.anesthesia-analgesia.org/content/111/6/1467.full.pdf |
|
|
78. Lumbo sacral plexus does lead into:
A. Subcostal n B. Ilioinguinal n C. Iliohypogastric n D. Femoral n E. Genitofemoral n |
ANSWER A
|
|
|
42. After a local anaesthetic block in a difficult-to-intubate patient, the patient has a seizure. What would you give?
A. Midazolam 5mg B. thiopentone C. propofol D. Suxamethonium |
ANSWER A
|
|
|
95 TMP-121 [Apr08] [Aug08]
Levosimendan: A. Increases contractility and myocardial oxygen consumption B. Increases SVR C. Binds to troponin C and induces a conformational change D. Increases contractility by increasing calcium influx E. Causes coronary vasodilation but NOT peripheral vasodilation |
ANSWER C
Levosimendan causes conformational changes in cardiac troponin C during systole, leading to sensitisation of the contractile apparatus to calcium ions It increases contractility without increasing oxygen requirements Causes coronary and systemic vasodilation |
|
|
72. New- Modified Cormack and Lehane grade - You cannot see beyond the epiglottis and there is a little space between the epiglottis and the posterior pharyngeal wall (? remembered as epiglottis touching posterior pharyngeal wall)
A. 2a B. 2b C. 3a D. 3b E. 4 |
Ans C
Cormack and Lehane in 1984 original Grade 1:The entire glottis is visible Grade 2:Only the posterior portion of the glottis can be seen Grade 3:Only the epiglottis can be seen, Grade 4: View not even the epiglottis can be seen Yentis and Lee modification Grade 2a:a part of the vocal cords can be observed Grade 2b: Only the arytenoids can be seen Cook modification Grade 3a:epiglottis can be seen and lifted Grade 3b:epiglottis cannot be lifted |
|
|
23. Repeat- The test to diagnose pulmonary embolism
A. CT pulmonary angiogram B. Echocardiogram C. Electrocardiogram D. Ventilation-perfusion scan |
ANSWER A
International Journal of Obstetric Anesthesia (2011) 20, 51-59 CTPA sensitivity 83-100% specificity 89-97% The first imaging test in the evaluation of patient suspected of PE V/Q scan sensitivity 98% and specificity 10% The second choice, for people allergic to contrast or renal function is impaired. |
|
|
61. Repeat- The most effective method of decrease renal impairment in AAA surgery
AZ69a ANZCA version [2003-Apr] Q137 During elective major vascular surgery the best way to reduce the risk of acute renal failure is to maintain a normal A. cardiac output B. central venous pressure C. mean arterial blood pressure D. pulmonary capillary wedge pressure E. renal blood flow AZ69b ANZCA version [2003-Aug] Q129, [2004-Apr] Q77, [Mar06] Q71, [Apr07] Q129, [Jul07] During elective major vascular surgery the best way to reduce the risk of acute renal failure is to maintain a normal A. central venous pressure B. mean arterial blood pressure C. renal blood flow D. systemic vascular resistance E. urine output |
Maintain renal flow
Limit AoX time Avoid supra renal AoX "Although it is clear that a suprarenal cross-clamp will decrease renal blood flow up to 80% an infrarenal cross-clamp also causes a decrease in renal cortical blood flow with an associated decrease in GFR." (Yao and Artusio, 6E Ch 11 p 291) |
|
|
114 Can01-113 What nerve supplies sensation to the larynx above the vocal cords?
A. Internal branch of superior laryngeal nerve B. External branch of superior laryngeal nerve C. Recurrent laryngeal nerve D. Glossopharyngeal nerve E. Palatotonsillar nerve |
A - internal branch
Wikipedia- The internal laryngeal nerve is the internal branch (ramus internus) of the superior laryngeal nerve. It descends to the thyrohyoid membrane, pierces it in company with the superior laryngeal artery, and is distributed to the mucous membrane of the larynx. Of these (sensory) branches some are distributed to the epiglottis, the base of the tongue, and the epiglottic glands; others pass backward, in the aryepiglottic fold, to supply the mucous membrane surrounding the entrance of the larynx, and that lining the cavity of the larynx as low down as the vocal folds. |