![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
54 Cards in this Set
- Front
- Back
|
Renal involvement in lupus nephritis involves... |
All components of the kidney -Glomerulus (commonest) -Tubulointerstitium -Vasculature |
|
|
Pathogenesis of lupus nephritis |
-Immune complexes - composed of DNA and anti-DNA antibody (directed against nucleosomes); may also have chromatin, C1q, SSA, SSB and other antigens -Immune deposits primarily in mesangium and subendothelial and subepithelial regions of GBM; also TBM (tubular basement membrane), vessels -Complement activaiton via classical pathway |
|
|
Injury mediators in lupus |
TNF-alpha IL-6 TGF-B INT-gamma PDGF Chemokines |
|
|
Lupus nephritis in the European population |
-16% with SLE had LN (protein > 0.5 g, cellular casts or high BUN/creatinine) at diagnosis
-After 10 yr follow up: 28% had LN -Much smaller black population |
|
|
Lupus nephritis in US population |
-Within 1 yr of diagnosis of SLE - 32% -After 9-yr follow up - 47%, ESRD 4% -Much larger black population |
|
|
US medicaid population + lupus nephritis |
-At 5 yr of diagnosis of SLE - 21% -Eventually majority - 75% or more |
|
|
Racial differences in LN |
-Race: Blacks, Hispanics, Asians > Whites (non-whites develop LN earlier on course of SLE, have a younger age at diagnosis (<33)) |
|
|
LN immunofluroescence findings |
-Positive for everything - "full house" IF -IgG, IgA, IgM, C3, C1q |
|
|
EM findings for LN |
-Deposits in mesangium, subendothelial, and subepithelial locations -Deposits may also occur in TBM, interstitium, and blood vessels -Tubuloreticular inclusions in glomerular endothelial cells (also found in HIVAN) |
|
|
Vascular findings in LN |
Thrombotic microangiopathy (TMA) -Isolated or with other LN manifestations -Anti-phospholipid antibodies positive 1) Lupus anticoagulant 2) Anticardiolipin antibody 3) Antibody against VW factor convertase (ADAMTS13) |
|
|
Tubulointerstitial disease in LN |
-With or without immune deposits is not uncommon -Prognostic |
|
|
LN WHO Type I - pathology |
Minimal mesangial LN 1) LM: normal 2) IF: mesangial deposits 3) EM: mesangial deposits Typically no renal manifestations (UA normal) |
|
|
LN WHO Type II - pathology |
Mesangial proliferative LN 1) LM: mesangial hypercellularity/expansion 2) IF: mesangial deposits 3) EM: mesangial deposits |
|
|
LN WHO Type III pathology |
Focal and segmental LN 1) LM: <50% glomeruli effected 2) IF + EM: deposits in mesangium, subepithelial, subendothelial; glomerular tuft necrosis + crescents (proliferation of epithelial cells of glomerulus) --> these two features mean disease is active |
|
|
LN WHO Type IV pathology |
Diffuse proliferative LN 1) LM >50% glomeruli affected 2) IF and EM: Deposits in mesangium, subepithelial, subendothelial - wire loops, glomerular tuft necrosis + crescents (proliferation of epithelial cells of glomerulus) --> these two features mean disease is active |
|
|
LN WHO Type V pathology |
Membranous LN 1) LM: like idiopathic membranous glomerulonephropathy (deposits subepithelial) - thickened BM 2) IF: "full house" immunofluorescence 3) EM: like idiopathic MGN with deposits and tubuloreticular inclusion More benign than type III/IV |
|
|
LN WHO Type VI pathology |
Advanced sclerosing LN 1) LM: global sclerosis of >90% glomeruli |
|
|
Clinical presentation of LN |
-Abnormal UA: proteinuria, active urinary sediment (RBCs, cellular casts) -Proteinuria - glomerular range (>1 g/day), including nephrotic -Abnormal kidney fxn -Uncommon without systemic manifestations of SLE -Kidney biopsy can show LN in absence of any clinical or lab abnormalities (rare) |
|
|
If you see tubuloreticular inclusions, think... |
lupus or HIV associated nephritis |
|
|
Diagnosis of LN |
-UA -Random urine for protein and creatinine -Renal electrolyte panel, Ca, PO4, albumin -Sedimentation rate, ANA, C3, C4, and anti-dsDNA -Additional serology - anti-SSA (Ro), anti-SSB (La), anticardiolipin antibody, lupus anticoagulant, anti-sm (smith) -> [highly specific but only 30-40% sensitive] -Renal ultrasound -Kidney biopsy (categorize class + guide therapy) |
|
|
Serology findings that indicate active disease |
Low C3, C4, and high dsDNA antibodies indicate active disease |
|
|
Most serious forms of LN? |
Diffuse or focal proliferative lupus nephritis (Class III or Class IV) |
|
|
Risk factors for progression of LN at presentation |
-Black/Hispanic -HTN -Elevated creatinine -Degree of proteinuria -Anemia (Hct <26) -Severity of tubulointerstitial nephritis + crescents |
|
|
Treatment for LN for all patients |
1) Optimal BP control - target BP < 130/80 -ACE-i/ARB ideal agent -Diltiazem - if you can't use ACEI/ARB -Do not use dihydropyridine Ca-channel blockers alone (worsen proteinuria) - can use with ACEI/ARB 2) Reduce proteinuria - goal <0.5g/day or at least 60% of baseline -ACEI/ARB; Diltiazem if not tolerated 3) Optimize lipid profile to reduce cardiovascular risk -Statins |
|
|
Immunosuppression treatment in LN |
-Goal: induce remission (proteinuria <0.5 g/day, inactive urine sediment, stabilization, or improvement of kidney fxn) -Induction phase -Maintenance phase -Therapy depends on histologic type -- need biopsy! -Shift away from cyclophosphamide and in favor of MMF (micophenolate mofetil) |
|
|
Treatment for Membranous LN (Class V) |
-General measures as first line
-Prednisone + MMF if no response to general measures |
|
|
Treatment for Focal proliferative LN (Class III) |
-Prednisone + MMF - for lower risk pts only |
|
|
Immunosupression treatment for severe Class III and Class IV |
1) Induction: glucocorticoids + cyclophosphamide (for severe disease) or MMF (milder disease) (given for 2 yrs) 2) Maintenance: MMF is better - same effect but with fewer side effects than cyclophosphamide |
|
|
Epidemiology of lupus |
-Mainly young women -Higher incidence in blacks vs whites |
|
|
Kidney presentation of lupus |
-Nephritic, nephrotic or both -Hematuria +/- RBC casts |
|
|
Systemic sx of lupus |
Rash, arthralgias, alopecia, pericarditis HTN common Hypocomplementemia (C3 and C4) |
|
|
Classic antibody in nucleus |
ANA (dsDNA) |
|
|
LM findings in lupus nephritis |
By class: 1) Normal 2) Global or segmental mesangial hypercellularity only 3) + 4) Focal or diffuse endocapillary proliferative - can have crescents and necrosis 5) Membranous produces nephrotic syndrome |
|
|
IF findings in lupus nephritis |
-Granular mesangial and capillary wall deposits of all Ig and complements - "full house pattern" -TBM and vesicular wall deposits common |
|
|
EM findings in EM |
Deposits in any compartment |
|
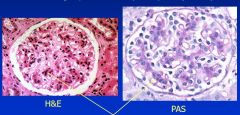
Class? Findings? |
Mesangial proliferative lupus nephritis (Class II) |
|
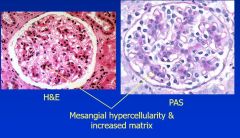
Class? |
Mesangial proliferative lupus nephritis - Class II - see mesangial hypercellularity and expansion |
|
Class? |
Class II IgG deposits |
|
|
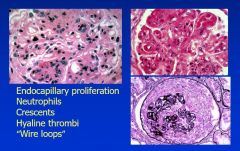
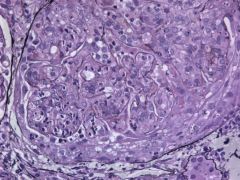
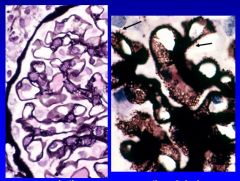
Light microscope findings for Class III and IV LN? |
|
|
|
Main difference between Class III and Class IV? |
Degree of glomeruli involvement |
|
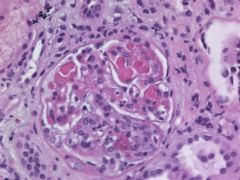
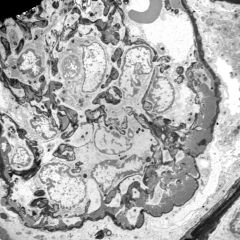
Findings? Class? |
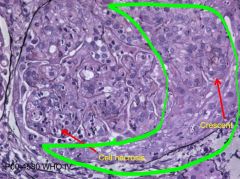
Class III/IV - crescents + cell necrosis |
|
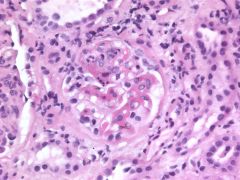
Findings? Class? |
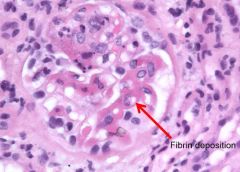
Class IV - fibrinoid deposits (diffuse proliferative LN) |
|
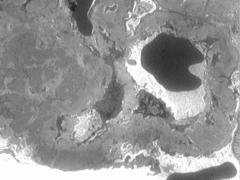
What are the deposits in this glomeruli? |
Thrombi |
|
Class? |
Class V - membranous LN |
|
|
Differentiate membranous LN from idiopathic MGN? |
With MGN, see IgG and C3 only on IF Also, don't see mesangial deposits with idiopathic MGN |
|

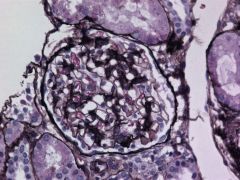
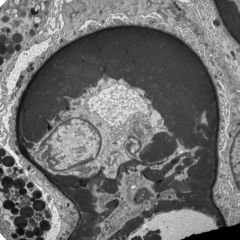
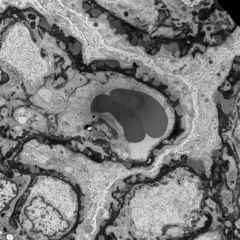
Findings? Likely classes? |
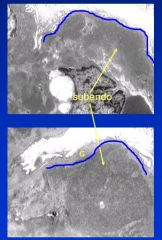
Subendothelial deposits - likely Class III/IV Blue line = glomerular basement membrane |
|
Where are the immune complex deposits located? |
In the mesangium - almost all forms of lupus have some mesangial deposits |
|
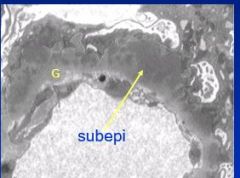
Where are these immune complexes deposited? |
Immune complexes are deposited subendothelially |
|
Findings? |
Wire looping of capillaries - massive amount of deposits between BM and endothelial cells - massive thickening of capillary wall (Class III/V) |
|
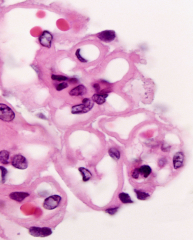
Findings? Class? |
Thick capillary walls on H+E - membranous class V (not as thick as wiring looping capillaries) |
|
Findings? Class? |
Spikes are indicative of excess basementmembrane material formed by the podocyte around an immune complex deposit as areaction to the subepithelialdeposit. Found only in membranous glomerulonephritis (and Class V of lupus nephritis). |
|
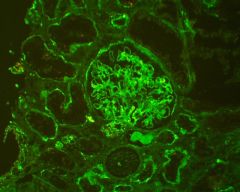
Class of lupus? Where are immune complexes located? |
Membranous Class V - granular deposits along capillary wall (subepithelial) but full house IF as opposed to membranous GN that is just IgG and C3 |
|
Class? |
Class V membranous - subepithelial deposits create spikes of BM |
|
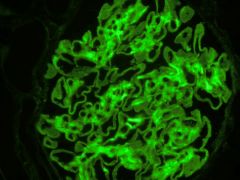
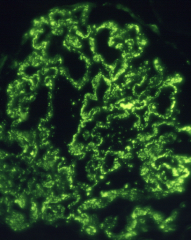
Immunofluorescence findings? |
-Deposits in the glomerular capillary wall, mesangium, tubular basement membrane, vascular wall immune deposits -IgA, IgG, IgM, C3, C4, C1q (full house IF) |