![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
244 Cards in this Set
- Front
- Back
|
Most common polyarthritis |
Rheumatoid arthritis |
|
|
What does Anti-CCP stand for? |
Anti-cyclic citrullinated peptide |
|
|
What is ACPA antibody? |
Anti–citrullinated protein antibody – Antibodies present in RA which are detected by CCP and therefore referred to as Anti-CCP. |
|
|
What are entheses? |
Connective tissue between tendon or ligament and bone |
|
|
Supposed pathogenesis of RA |
Presumed autoimmune-driven inflammation of synovial joints leads to destruction ofjoints and peri-articular tissues ± extra-articular features |
|
|
Most common polyarthritis |
RA |
|
|
Where do Rheumatoid nodules locate? |
Back of elbow or back of hands |
|
|
Significance of rheumatoid nodules |
Necessarily seropositive (RF present) and therefore worse prognosis |
|
|
3 RF for RA |
Women (3x) Smoking FHx |
|
|
4 presentations of RA and their relative incidence |
◾ Insidious (70%) – progressively feeling poorer ➙ Worse prognosis ◾ Acute (15%) – wakes up with stiff joints whilst being fine the day before ➙ Better prognosis ◾ Systemic (10%) – low grade fever, weight loss, lethargic ◾ Palindromic (5%) – Symptoms come and go |
|
|
What defines polyarthriris |
≥ 5 joints affected 2-4 is oligoarthritis |
|
|
Name one classification system for RA. Why is it useful? |
EULAR classification Early diagnosis |
|

|
Boutonière's deformity |
|

|
Swan's neck deformity |
|

|
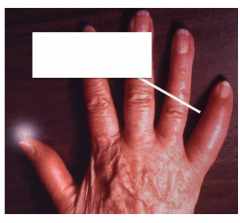
Z-thumb |
|
|
Name 4 deformities in the hand and wrist of RA |
Wrist Ulnar deviation Hands ◾︎ Swan neck ◾︎ Boutonniere ◾︎ Z-Thumb |
|
|
4 X-ray features of OA |
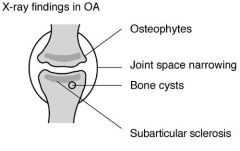
◾ Joint space narrowing ◾ Osteophytes ◾ Subarticular sclerosis ◾ Subarticular cysts |
|
|
4 X-ray features of RA |
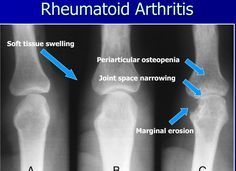
◾ Joint space narrowing ◾ Periarticular osteopenia ◾ Erosion ◾ Soft tissue swelling |
|
|
What are the 4 criteria used in the EULAR diagnostic criteria for rheumatoid arthritis? |
◾ Joint involvement (# and size): many small joints get more points ◾ Serology: RF and ACPA ◾ Acute phase: CPR and ESR ◾ Duration of symptoms: > 6weeks get one point |
|
|
6 clinical features of the joint in rheumatoid arthritis |
Pain Stiffness Swelling Subluxation Joint instability Deformity |
|
|
3 signs of RA in the skin |
Palmar erythema Nodules Vasculitic rash and ulcers |
|
|
Besides the skin and the joints, name 8 other systems affected by RA |
Neurological Cardiovascular Haematological Lymphatics Musculoskeletal Ocular Pulmonary Amyloid |
|
|
4 CV features of RA |
Think of diseases just surrounding but not into the heart Cardio Pericarditis Conduction abnormalities Vascular Coronary vasculitis Aortitis |
|
|
3 neuro features of RA |
Cervical cord compression Mononeuritis multiplex (loss of all modalities of a peripheral nerve due to vascular occlusion) Compression neuropathy (eg carpal tunnel syndrome) |
|
|
1 MSK feature of RA |
Muscle wasting |
|
|
3 ocular features of RA |
Episcleritis Scleritis Keratoconjunctivitis sicca (dry eyes) |
|
|
What mostly distinguishes episcleritis from scleritis |
Scleritis is more painful |
|
|
3 pulmonary features of RA |
Nodules Effusion (exudates due to inflammation) Fibrosis Caplan's syndrome (rare) |
|
|
2 haematological features of RA |
Anaemia Thrombocytosis |
|
|
Three complications of RA |
Septic arthritis AA amyloidosis Side effects of drugs |
|
|
Why may patients with RA have pitting oedema? |
RA ⟹ AA amyloidosis ⟹ nephrotic syndrome |
|
|
What tool enables to assess the progression of RA? Describe it. |
Disease activity score (DAS28) 28 joints: shoulders, elbows, wrists, MCP, PIP, knees ◾︎ Swollen join count ◾︎ Tender joint count ◾︎ ESR/CRP ◾︎ Patient global health (visual analog scale) |
|
|
DAS28 thresholds for remission and severe disease |
DAS28 > 5.1 is severe DAS28 < 2.6 is remission |
|
|
6 broad biochemical tests to do in RA (to assess severity and help diagnose) |
◾ ESR/CRP ◾ FBC ◾ Renal function ◾ Liver function ◾ Urinalysis ◾ Serology: RF and Anti-CCP |
|
|
Which of the 4 presentations of RA has the worst prognosis? |
Insidious |
|
|
Which symptoms of RA lead to the worst prognosis if present? |
Systemic symptoms |
|
|
What is the basic principle for the management of RA |
Treat to target Define a target DAS28 with patient and treat until you reach it |
|
|
4 broad strategies of management of RA |
Education PT/OT Medication Surgery |
|
|
What medication would you use to kick-start the treatment of RA |
Depo-medrone injection (steroid) |
|
|
Name 4 drugs that can effectively modify the progression of RA and outline their MOA |
Disease-modifying anti-rheumatoid drugs (DMARD) Methotrexate (MTX) Folic acid antagonist Hydroxychloroquine (HCQ) Inhibition of cellular enzyme release Sulphasalazine (SSZ) (Unknown) Leflunomide (LEF) Arrests activated lymphocytes |
|
|
About the side effects of DMARD, 1) Which one(s) cause diarrhoea? 2) Which one(s) require FBC? Why? 3) Which one(s) require LFT? Why? 4) Which one(s) require optician review? Why? 5) Which one(s) are teratogenic? |
1) LEF (but also MTX and SSZ) 2) LEF, MTX and SSZ because they may cause myelosuppression 3) LEF, MTX and SSZ because they may cause hepatitis 5) MTX and LEF |
|
|
What monitoring is required for patients under MTX, SSZ, LEF and HCQ (separately)? |
FBC LEF, MTX and SSZ (may cause myelosuppression) LFT LEF, MTX and SSZ (may cause hepatitis) Pregnancy test LEF and MTX Optician review HCQ |
|
|
What is the role of steroid treatment in RA? |
No overall impact on progression of disease Systemic steroids useful in active disease and flare Local injections useful in early disease and flare |
|
|
Criteria for use of biologics in RA |
Two DMARD have been attempted, including MTX and DAS28 > 5.1 |
|
|
Patient with RA remains very symptomatic after MTX course (DAS28 = 4.9). What may you consider? |
Another DMARD (eg HCQ) |
|
|
Patient with RA remains very symptomatic after MTX course (DAS28 = 5.2). What may you consider? |
Another DMARD since she hasn't tried two (even if DAS28 > 5.1) |
|
|
Patient with RA remains very symptomatic after MTX and HCQ course (DAS28 = 4.9). What may you consider? |
Try another combination since DAS28 < 5.1 |
|
|
First biologic that should be attempted in patient with RA |
Anti-TNF |
|
|
Name 3 anti-TNF and their MOA |
Infliximab and adalimumab (destroy TNF) Etanercept (receptor of TNF to neutralise them) |
|
|
Three serious complications of anti-TNF |
New infections Reactivation of TB Increased risk of cancer |
|
|
1st, 2nd and 3rd line of biologics if Anti-TNF have failed (and their MOA) |
Rituximab (anti CD20,i.e. anti middle age B-cells) Abatacept (anti T-cells) Tocilizumab (anti IL-6) |
|
|
How often should rituximab (anti B-cells) be given in RA? |
Twice 2 weeks apart, every 6 months |
|
|
A patient with RA has DAS28 of 5.3, RF -ve and has tried MTX and adalimumab which were unsuccessful. What drug would you try now? |
Abatecept (anti T-cells) or Tocilizumab (anti IL-6) but not rituximab since she is RF -ve. |
|
|
MOA of abatacept (with a bit of details) |
Exogenous CTLA-4 which is an endogenous molecule that blocks T-cell/APC communication |
|
|
Role of NSAIDs in RA |
Can be used in acute flares |
|
|
T/F: Anaemia is a good indicator of RA disease activity |
False, thrombocytosis is. Anaemia can be due to multiple factors (Note: in SLE, thrombocytopenia indicates worse prognosis) |
|
|
4 contraindications to the use of anti-TNF |
Pregnancy Breast feeding Septic arthritis within 12 months Heart failure |
|
|
At what age do we reach our peak bone mass |
20-30 |
|
|
Name 4 factors that negatively affect peak bone mass |
Smoking Teenage pregnancy Anorexia Exercise amenorrhoea |
|
|
Adequate calcium intake per day in mg, milk, cheese matchbox and pot of yoghurt units |
700mg 1 pint of milk 3.5 matchboxes of cheese 3.5 pots of yoghurt |
|
|
Besides age, name 6 factors that accelerate bone loss |
Low oestrogen/Low testosterone Vit D deficiency Corticosteroids (oral) Low weight/Low muscle mass Smoking ETOH XS |
|
|
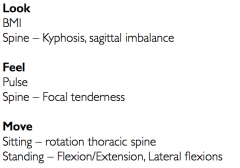
Examination of suspected osteoporosis |
|
|
|
Diagnosis of osteoporosis |
Dual energy X-ray absorptiometry (DXA) |
|
|
What do T-score and Z-score refer to in DXA context |
T-score – Compared to young adult female reference mean |
|
|
WHO diagnostic criteria for osteoporosis |
DXA T-score ≤ -2.5 in the presence of one or more fragility fractures |
|
|
What tool can be used to assess the fracture risk based on bone mineral density? How is the outcome of this tool used? |
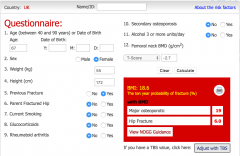
FRAX Provides guidance on whether to treat or give lifestyle advice and reassurance |
|
|
12 primary causes of secondary osteoporosis |
Omit to take Vit D |
|
|
7 drugs that can be considered in osteoporosis |
◾ Vit D/Calcium ◾ Raloxifene (oestrogen-like on bone and anti-oestrogen like on uterus and breast) ◾ Bisphosphonate (push osteoclasts to apoptosis) ◾ Strontium (Ca-like element) ◾ Teriparatide (PTH-like) ◾ Denosumab (RANKL inhibitor) ◾ Cathepsin K inhibitors (cathepsin K is secreted by osteoclasts to break down collagen) |
|
|
MOA of raloxifene |
Selective estrogen receptor modulator (SERM) Oestrogen-like on bone and anti-oestrogen-like on uterus and breast |
|
|
MOA of bisphosphonate |
Push osteoclasts to apoptosis |
|
|
MOA of strontium |

Calcium-like element |
|
|
MOA of teriparatide |
PTH (recombinant form) Intermittent exposure to PTH increases osteoblasts activity (as achieved here) while chronic exposure to PTH increases bone resorption (as in hyperparathyroidism) |
|
|
MOA of denosumab |

RANKL inhibitor (Of note: OPG is also produced by osteoblasts and inactivate RANKL) |
|
|
MOA of cathepsin K inhibitors |
Cathepsin K is secreted by osteoclasts to break down collagen |
|
|
7 RF for bone fracture (3 related to clinical risk of fracture, 4 related to decreased bone mass density) |
Clinical Parental hip fracture Alcohol ≥ 3U/day RA BMD BMI < 22 IBD/AS Immobility Untreated premature menopause |
|
|
Activation of Vitamin D |

|
|
|
5 contraindications to HRT |
Breast cancer (past, current or suspected) Known or suspected oestrogen-sensitive cancer IHD (recent or current) Past or current thromboembolism Untreated HTN Active liver disease with deranged LFT |
|
|
What are SERM? |
Selective estrogen receptor modulator (SERM) The class of drug of raloxifene |
|
|
Two contraindications to SERM (such as raloxifene)? |
DVT/PE Pre-menopause |
|
|
In one line, who is raloxifene recommended to? |
Post-menopausal women with spinal osteoporosis and no DVT/PE hx |
|
|
Major downside of bisphophonate in the treatment of OP |
Very poor bioavailability so lots of precaution in taking and therefore poor compliance |
|
|
What would you instruct to a patient to take bisphosphonate? |
1. After overnight fast 2. With only tap water 3. Do not chew it 4. NBM for 30min afterwards 5. Remain upright for 30min (seated or standing) 6. No Ca supplement for 4h |
|
|
4 contraindications to bisphosphonate (alendronate and risedronate) |
Pregnancy Recent upper GI event Hypocalcaemia Abnormal swallowing |
|
|
Can bisphosphonate (alendronate and risedronate) be given to patient of childbearing age? |
It should be avoided as much as possible and if given, foul-proof contraception should be added. |
|
|
Can bisphosphonate (alendronate and risedronate) be given to men of any age? |
Yes, the risk to pregnancy is only related to blood transmission to placenta |
|
|
Alternative to alendronate and risedronate in patients with OP with recent GI event? |
Zoledronate IV |
|
|
Compare alendronate and zoledronate in terms of: 1) Frequency 2) Route 3) Contra-indications 4) Side effects |
Frequency Weekly (A) vs Annually (Z) Route PO (A) vs IV (Z) Contraindications Pregnancy (A and Z) Hypocalcaemia (A and Z) Upper GI events (A) Abnormal swallowing (A) Kidney disease (Z) Side effects Osteonecrosis of the Jaw (A and Z) Renal impairment (Z>A) Oesophagitis (A) Acute inflammations, eg flu, colitis (Z) Requires normal serum Ca and Vit D (Z) |
|
|
Two contraindications to strontium for OP |
Kidney disease (low eGFR) Thromboembolism Cardiovascular disease |
|
|
One contraindication to denosumab for OP |
Hypocalcaemia |
|
|
4 contraindications for teriparatide in OP |
Hypercalcaemia (opposite to denosumab and bisphosphonate) Previous radiotherapy Previous malignancy (except BCC) Paget's disease |
|
|
Treatment of vertebral collapse |
Vertebroplasty (percutaneous cement injection) |
|
|
A patient on bisphosphonate for OP starts experiencing bad taste and swelling of the jaw. Likely cause? What might you elicit on examination? |

Osteonecrosis of the jaw Examination: Exposure of mandibular or maxillary bone through lesions in the gingiva that do not heal |
|
|
Which bones are most affected by osteonecrosis of the jaw? |
Mandible and maxillary |
|
|
Name 3 treatments of OP that may cause osteonecrosis of the jaw |
Alendronate PO Zoledronate IV Denosumab (RANKL inhibitor) |
|
|
T/F: bisphosphonate and denosumab reduce the probability of all fractures. |
False: they increase the risk of atypical subtrochanteric fracture |
|

Likely story |
Atypical subtrochanteric fracture Patient with OP treated with bisphosphonate or denosumab |
|
|
Pathogenesis of Paget's disease of the bone |
Multinucleate osteoclasts causing increased bone turnover with disorganised woven formation |
|
|
Two genes whose mutations may lead to Paget's disease of the bone |
Sequestome 1 (SQSTM1) RANK-NF-kB |
|
|
What inheritance pattern of Paget's disease is known? |
Autosomal dominant with incomplete penetrance (SQSTM1) |
|
|
Which genetic mutation leads to the worst prognosis of Paget's? Which leads to the earliest onset? |
SQSTM1 for both |
|
|
Most common presentation of Paget's disease of the bone? |
Asymptomatic |
|
|
When symptomatic, most common symptom of Paget's disease of the bone? Name one other symptom |
Pain Deformities |
|
|
Characterise the pain in Paget's disease |
Deep Constant Worse when lying flat Worse with heat |
|
|
6 complications of Paget's disease |
◾ OA – 70% ◾ Nerve compression (deaf 60%, vertigo, spinal stenosis) ◾ Fracture – 10% ◾ Osteosarcoma – 0.4% ◾ High output heart failure (AV connections forming in the bones) ◾ Gout |
|
|
Most, second and third likely site of Paget's disease |
Polyostotic (72%) Pelvis (70%) Vertebra (40%) Femur (30%) |
|
|
T/F Osteoarthritis is a rare complication of Paget's disease |
F: it occurs in 70% of patients |
|
|
Levels of the following in Paget's: ALP Ca Vit D PO4 PTH |
ALP ➚ (or bone-specific ALP) Ca ➙ Vit D ➙ PO4 ➙ PTH ➙ |
|
|
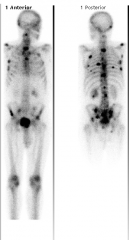
Besides X-ray, what imaging can be used to help diagnose Paget's |
Bone scan (scintigraphy) = SPECT with Tc99 radioactive substance |
|
|
Bone mets (focal areas and not whole bone affected) |
|

|
Normal skeleton (activated areas are symmetrical and correspond to highly active bones) |
|
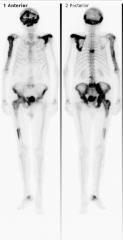
|
Paget's disease: whole bone affected (asymmetrical) |
|
|
Management of Paget's (3) |
Reassure Bisphosphonate Monitor (including for malignancy) |
|
|
T/F: In polyarticular diseases, imaging usually provide the bulk of the information for diagnosis |
False: history and examination does |
|
|
T/F: In polyarticular diseases, lab tests usually provide the bulk of the information for diagnosis |
False: history and examination does |
|
|
Definite diagnostic feature of SLE |
Anti-dsDNA |
|
|
Symmetrical synovitis and morning stiffness in small joints of the hands |
Rheumatoid arthritis |
|
|
For the following 3 broad aetiologies of polyarticular diseases, state whether it is acute or chronic: 1) Infective (eg Lyme) 2) Non-infective inflammatory (eg RA) 3) Non-inflammatory (eg OA) |
1) Acute 2) Acute or Chronic 3) Chronic |
|
|
Name 3 polyarthrites that present with a migratory pattern of joint involvement (comes and goes in some joints to reappear in others). |
Rheumatic fever Gonococcal arthritis Lyme (early phase) |
|
|
Name 5 polyarthrites present with intermittent pattern (come in several joints then complete remission then reappearance) |
Reactive arthritis Rheumatoid arthritis Psoriatic arthritis Polyarticular gout (rare) Sarcoid arthritis |
|
|
T/F: rheumatoid arthritis spare the spine |
False: cervical spine can be affected but not thoracolumbar |
|
|
Name 6 joints (or group of joints) commonly spared by OA |
Upper limb MCP Wrist Elbow Glenohumeral Lower limb Ankle Tarsal |
|
|
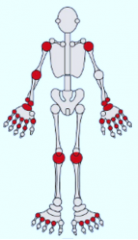
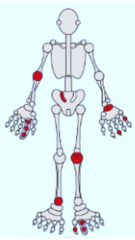
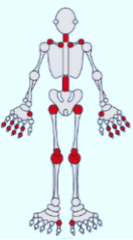
RA (symmetrical and spine and DIP spared) |
|
|
Psoriatic arthritis (any joints in an asymmetrical fashion) |
|
|
AS (axial skeleton and large peripheral joints in an asymmetrical fashion) |
|
|
OA (DIP, base of thumb, knees, hips, lumbar and cervical spine) |
|
|
Which of the following polyarthritis may affect the spine: Psoriatic arthritis Ankylosing spondylitis Osteoarthritis Rheumatoid arthritis Reactive arthritis Lyme Gonococcal arthritis Enteric arthritis |
All can except Rheumatoid arthritis – only cervical Lyme – Not at all Gonococcal arthritis – Not at all |
|
|
3 most common diagnosis in a patient with polyarticular symptoms who is: 1) Female between 25-50 2) Male between 25-50 3) Over 50 |
1) OA, RA, SLE, Fibromyalgia 2) Gonococcal arthritis, reactive arthritis, AS, OA 3) OA, RA, polymyalgia rheumatica |
|
|
How is morning stiffness useful in the differential of polyarticular diseases? |
Inflammatory polyarticular diseases (eg RA) Morning stiffness for > 1hour Non-inflammatory polyarticular diseases (eg OA) Morning stiffness for 15min-1hour |
|
|
Define tenosynovitis. Significance of its presence in polyarticular disease (5 differential) |
Inflammation of the synovial-lined sheaths surrounding tendons elicited on exam as swelling and tenderness along tendons between joints. RA, Gout, Reactive arthritis, gonococcal arthritis, TB and fungal arthritis |
|

Name the skin condition and the polyarticular disease(s) associated with it |
Psoriatic plaque Psoriatic arthritis |
|

Name the skin condition and the polyarticular disease(s) associated with it |
Butterfly malar rash SLE |
|

Name the skin condition and the polyarticular disease(s) associated with it |
Erythema nodosum Enteric arthritis, Sarcoid arthritis |
|

Name the skin condition and the polyarticular disease(s) associated with it |
Rheumatoid nodules RA |
|

Name the skin condition and the polyarticular disease(s) associated with it |
Keratoderma blennorrhagica Reactive arthritis
–derma: skin –rrhagia: discharge |
|

Name the skin condition and the polyarticular disease(s) associated with it |
Palmar erythema RA |
|

Name the skin condition and the polyarticular disease(s) associated with it |
Circinate balanitis Reactive arthritis |
|

Name the skin condition and the polyarticular disease(s) associated with it |
Tophus Gout |
|

Name the skin condition and the polyarticular disease(s) associated with it |
Keratoderma blennorrhagica Reactive arthritis |
|

Name the skin condition and the polyarticular disease(s) associated with it |
Discoid rash SLE |
|

Name the skin condition and the polyarticular disease(s) associated with it |
Pyoderma gangrenosum Enteric arthritis |
|
|
T/F the presence of circinate balanitis indicates that the primary infection was an STI. |
False: it is reactive arthritis and therefore signs relate to immune reactions, not the infection itself which could be GI |
|
|
6 polyarticular diseases that may have a positive ANA |
SLE – dsDNA, Histone, RNP, Ro/La RA – Histone (and RF is a false positive in tests) Sjögren's – Ro/La Polymyositis – Jo1 Scleroderma – Scl70/Topoisomerase Mixed connective tissue disease – RNP |
|
|
A patient with flu-like symptoms has a positive RF. What should you do and suspect? |
Flu which usually causes RF to raise temporarily |
|
|
Significance of low serum complement in polyarticular diseases |
SLE or vasculitis They consume complement by forming immune complexes |
|
|
Suspected mechanism of RA |
1) CD4 T cells trigger production of proinflammatory cytokines by Mϕ (e.g. IL-1 and TNFα) 2) Production of IgM and IgG by plasma cells |
|
|
What two (groups of) joints are typically affected by RA? |
PIP and MCP |
|
|
What is a subluxation? |
A partial dislocation |
|
|
Name 5 seronegative spondyloarthropathies |
Ankylosing spondylitis (AS) Psoriatic arthritis (PsA) Reactive arthritis (ReA) Enteric arthritis (IBD) Undifferentiated spondylitis |
|
|
3 intra or periarticular characteristics of seronegative spondylitis |
Sacroiliac (buttock) pain Peripheral inflammatory arthropathy Enthesopathy (insertional tendonitis) |
|
|
Which is correct: 1) HLA-B27 has high sensitivity and high specificity for ankylosing spondylitis 2) HLA-B27 has high sensitivity but low specificity for ankylosing spondylitis 3) HLA-B27 has low sensitivity but high specificity for ankylosing spondylitis 3) HLA-B27 has low sensitvity and low specificity for ankylosing spondylitis |
2 – 99% of AS patients have it but so does 10% of the population |
|
|
What is HLA-B27 a sensitive marker of? a RF for? a non-sensitive marker of (2)? |
Sensitive for Ankylosing spondylitis (99% have it) Risk factor for reactive arthritis (20% of HLA-B27 positive develop ReA) Non-sensitive for psoriatic arthritis and enteric arthritis Remember PAIR (PsA, AS, IBD, ReA) |
|
|
Demographic mostly affected by AS |
Young (20-40) male |
|
|
Pathological process of ankylosing spondylitis |
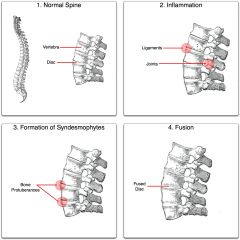
1. Inflammation with fibrosis and ossification of ligaments, tendons and insertions 3. Fusion of the spine |
|

|
Bamboo spine caused by formation of syndesmophytes in ankylosing spondylitis |
|
|
27 year old man with low back pain and pain in the back of his right ankle. Name one possible diagnosis and outline the pathological process explaining his back pain and ankle pain |
Ankylosing spondylitis Back pain – Spinal fusion and microfractures Ankle pain – Enthesopathy (insertional tendonitis) |
|
|
5 extra-articular features of ankylosing spondylitis |
Constitutional + 4A Aortic regurgitation Apical fibrosis Achilles tendinitis Anterior uveitis |
|
|
What fraction of patients with AS have anterior uveitis |
40% |
|
|
4 signs of anterior uveitis |

Dilated ciliary vessels Posterior synechiae (Iris adheres to the lens hence irregular pupil) Keratic precipitate (deposition of inflammatory cells on cornea) Hypopyon (inflammatory cells in the anterior chamber of the eye) |
|
|
Name 4 conditions that may present with anterior uveitis and polyarticular disease |
Spondyloarthropathies (AS, IBD, PsA, ReA) Juvenile rheumatoid arthritis Sarcoidosis SLE |
|
|
T/F: inflammatory markers is a good way of assessing severity of ankylosing spondylitis |
False: there is little correlation |
|
|
Imaging of choice in early diagnosis of ankylosing spondylitis and what you would see |
T2w MRI Romanus lesions (erosion involving the anterior and posterior edges of the vertebral endplates) followed by shiny corners (reactive sclerosis to erosions) |
|
|
Role of XR in ankylosing spondylitis |
Positive only after 8 years of disease Demonstrates symmetrical sacroiliac changes, syndesmophytes, and ossification |
|
|
Patient has ankylosing spondylitis and on examination, there are crepitations in apices. Name 2 potential reasons |
Fibrosis (as an extra-articular feature) TB (caused by anti-TNF alpha) |
|
|
Name and quickly describe one tool used to assess AS disease activity |
BASDAI Self-reporting questionnaire |
|
|
Name and describe one special test to do in OSCE in a patient with AS |
Modified Schöber's test A and B = Dimple of Venus (Posterior-superior iliac spine) C = (A+B)/2 D = C + 10cm above E = C - 5cm below |DE| = 15cm Ask patient to bend forward. Positive if |DE| remains < 20cm |
|
|
6 bad prognostic indicators of AS (3 that happen early, 1 extra sign, 1 blood, 1 aetiological) |
Early: onset, loss of lumbar spine mobility, hip involvement Dactylitis ESR > 30 Sporadic (vs familial) |
|
|
3 lines of management of AS |
1) PT (including hydrotherapy) 2) NSAIDs 3) TNF blockade |
|
|
Besides BASDAI which is useful for formalising history of AS, what formal scoring system exists for examination of AS? Describe it |

BASMI 1) Lateral lumbar flexion 2) Tragus-to-wall distance (displayed) 3) Modified Schöber's test 5) Cervical rotation |
|
|
Demographics at risk of psoriatic arthritis |
20-40 M and F |
|
|
5 common presentations of psoriatic arthritis |
◾︎ DIP (OA-like) ◾︎ Symmetrical polyarthritis (RA-like) ◾︎ Spondyloarthropathy (AS-like) ◾︎ Asymmetrical oligo ◾︎ Arthritis mutilans (severe, deforming and destructive) |
|
|
What clinical feature of psoriasis is predictive of the development of PsA? |
Nail lesions – Occur in 90% of patients with PsA |
|
|
Radiological hallmark of PsA |
Erosive change with bone proliferation, in a predominantly distal distribution |
|

Name the sign and a condition in which it may occur |
Pencil-in-a-cup finger Occurs in PsA |
|
|
What does juxtaarticular osteopenia suggest in polyarticular arthritis? |
RA (not PsA) |
|
|
Besides erosion and bone prolifeartion, name 3 other signs that you would see in a patient with PsA |

Ankylosis Pencil-in-cup deformities Whittling of terminal phalanges (picture) |
|
|
Dactylitis |
|
|
In which 2 conditions does dactylitis occur? |
AS PsA |
|
|
Patient presents with pain in the distal phalange of the big toe, as well as in several joints in both hands. There is also an itchy rash on the skull. X-ray shows bone fusion and some erosion. Blood test reveals high level of uric acid. Diagnosis? |
PsA which can present with hyperuricaemia The rash and X-ray appearance is inconsistent with gout |
|
|
Management of PsA |
PT/OT Mild to moderate NSAID MTX/LEF If spinal or peripheral: SSE Avoid HCQ Severe TNF blockage (etanercept or adalimumab) Cyclcosporin A Retinoids Flares Steroids injection |
|
|
What is the best arthritis to have? Why? |
Reactive arthritis usually remits after 2 year |
|
|
Presentation of reactive arthritis |
Classic triad 1) Monoarthritis 2) Rash - Keratoderma blennorhagica (painless palms and soles pustules) - Circinate balanitis on penis 3) Eye irritation (conjunctivitis then uveitis) |
|
|
In one line, what determines suspicion for reactive arthritis? |
Spondyloarthropathies with associated urethritis, cervicitis or diarrhoea |
|
|
About reactive arthritis following diarrhoea, when does the diarrhoea occur? What organisms (3) mostly cause it? |
Within a month Shigella, salmonella, clostridium (C. diff) |
|
|
About reactive arthritis following urethritis, how does it present? What organism mostly causes it? |
May be asymptomatic Chlamydia |
|
|
4 differentials to reactive arthritis |
HIV Lyme Behcet’s |
|
|
How is reactive arthritis diagnosed? |
History + Examination Raised inflammatory markers Serology Cultures and swabs Joint aspirate to rule out septic or crystal arthropathy |
|
|
Role of joint aspirate in reactive arthropathy |
Rule out septic arthritis and crystal arthropathy |
|
|
Treatment of reactive arthritis |
Usually NSAIDs + Steroid injections will suffice for many patients (Remission occurs in 2 years) Persistent disease DMARDs (eg SSZ) |
|
|
T/F: Treating the primary infection with ABx is very important in controlling reactive arthritis |
False: ABx may have no effect on arthritis |
|
|
Significance of HLA-B27 in reactive arthritis |
HLA-B27 positive is a RF for persistent disease (otherwise useless marker for diagnosis) |
|
|
Distinguish the two types of enteric arthropathy in terms of joints affected, association with IBD symptoms, and incidence |
Peripheral – 2/3 Coincide with symptoms of IBD Mostly knees and ankles Sacroiliitis – 1/3 Independent from symptoms of IBD AS-like |
|
|
Besides the joint and IBD, what clinical features would you look out for in enteric artrhopathy |
Eye Conjunctivitis then uveitis Skin Erythema nodosum Pyoderma gangrenosum |
|
|
Treatment of enteric arthropathy (symptom management, disease-modifying and refractory disease) |
Symptoms NSAIDs + Intra-articular or oral steroids Disease-modifying SSZ Refractory disease Anti-TNF |
|
|
What sign of SLE might you see on ECG? |
Saddle-shaped ST elevation in most leads due to pericarditis (serositis can be caused by SLE) |
|
|
Pathogenesis of SLE (2) |
1. Autoantibodies against nuclear antigens and other antigens ⇒ Direct effect on tissues and immune complex formations 2. Antibody against C1q and C4 complement ⇒ Complement defect ⇒ Cells debris are not collected ⇒ Nuclear antigens are presented to Th cells ⇒ Autoantibodies to nuclear antigens can act |
|
|
What haematological changes are observed in SLE? |
Anaemia of chronic disease + Possibly haemolytic anaemia (due to Ig against RBC) Pancytopenia |
|
|
Name one antibody class that can be tested for in SLE. How sensitive and specific is it? |
Anti-nuclear antibodies (high sensitivity, low specificity) |
|
|
What anti–nuclear antibody is most sensitive to SLE? |
Anti-dsDNA |
|
|
What biopsy investigation can be made in the diagnosis of SLE? |
Biopsy of skin ⇒ Band of immune complex deposition between dermis and epidermis |
|
|
Prognosis of SLE with treatment |
Excellent (> 90% survival at 10 years) |
|
|
Prevalence of SLE F:M ratio Peak age and one demographic particularly at risk |
0.1% F:M = 9:1 Peak age: 45 Afro-Caribbeans (RR=5) and South-East Asian (RR=2) |
|
|
At what stage of SLE is ANA positive |
Very early on (even before symptoms) |
|
|
How does the skin rash correspond to the chronicity of SLE |
Malar (butterfly) rash – Acute Discoid rash – Chronic |
|

|
Discoid lupus |
|
|
How does discoid lupus influences prognosis of SLE |
Indicates milder disease |
|
|
What fraction of patients with SLE develop renal disease? Cardiac disease? Stroke and seizures? Pleurisy? |
60% – Glomerulonephritis 50% – Cardiac 20% – Stroke and seizures 50% – Pleurisy |
|
|
How is skin disease in SLE managed (4)? |
UV avoidance Topical steroids Topical calcineurin inhibitors (eg tacrolimus) Systemic immunosuppressants if resistant |
|
|
How is renal disease in SLE assessed? |
Routinely: Dipstick, U&E, BP Biopsy if suspicious |
|
|
Initial and maintenance management of renal disease in SLE |
Initial Mycophenolate mofetil (MMF) IV methylprednisolone Maintenance MMF Prednisolone Hyroxychloroquine ACE inhibitor, statin, vaccinations |
|
|
Patient with SLE has significant proteinuria but normal U&E. What should you do? |
Treat as renal disease of SLE (this is likely membranous disease) |
|
|
Patient with SLE has normal urine but abnormal U&E. What should you do? |
Biopsy and treat if renal disease |
|
|
What may cause neuro symptoms in SLE? |
◾ Disease itself (vasculopathy or diffuse inflammation) ◾ S/E of medications |
|
|
Two most common neuro presentation of SLE |
Cumulative incidence: 20% Stroke Seizure |
|
|
Name one serological marker that is a RF for neuropsych disease in SLE |
Anti-phospholipid antibodies |
|
|
Patient with SLE has headaches, what may cause it? |
Infection or venous sinus thrombosis (Probably not SLE itself) |
|
|
T/F: if a patient with SLE has delirium, then immunosuppression should be stopped. |
False, infection should urgently be excluded following what intense immunosuppression may be beneficial. |
|
|
Most common cardiac disease in SLE? |
Pericarditis |
|
|
What cardiac diseases are patients with SLE at risk of (3)? Give an approximate prevalence |
Pericarditis – 50% Endocarditis – 30% Myocarditis – 10% |
|
|
T/F: patients with SLE are at increased risk of IHD |
True (> 2x) |
|
|
Most common respiratory disease in SLE |
Pleurisy (serositis) |
|
|
Which of the following is least likely to be heard in a patient with SLE: 1) Pericardial rub 2) An ejection systolic murmur over the RUSE 3) A pansystolic murmur over the apex 4) Third heart sound |
2 – Aortic stenosis is less common 1 – Common due to endocarditis 3 – Common due to mitral regurgitation in endocarditis (mitral valve is the most affected) 4 – Common due to pulmonary hypertension |
|
|
What is a severe albeit rarer pulmonary complication of SLE |
Acute pneumonitis |
|
|
SLE can present with low blood cells of any sort. Which one is associated with more severe disease and poorer prognosis? |
Thrombocytopenia (Note: in RA, thrombocytosis correlates with disease activity) |
|
|
Name 5 biochemical features of haemolytic anaemia |
Normocytic anaemia Positive Coomb's test Raised LDH Low haptoglobin (binding to free Hg for clearance) Raised reticulocytes |
|
|
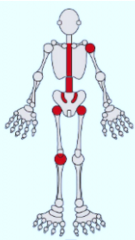
Main 3 (groups of) joints affected in SLE |
PIP Wrists Knees |
|
|
Compare arthralgia in SLE and RA |
SLE – Pain excessive compared to amount of swelling |
|
|
Characterise the arthritis in SLE in terms of joints affected, synovitis, erosion, and deformities |
Joints – PIP, Wrist, Knees Synovitis – Little Erosion – None Deformities – Passively correctable (eg Jaccoud's) |
|
|
4 GI manifestations of SLE |
Oral ulcers Mesenteric vasculitis Pancreatitis Peptic ulcer |
|
|
Which antibody correlates with disease activity in SLE |
dsDNA |
|
|
Besides dsDNA, name 5 other antibodies that may be present in SLE |
Sm Ro/La (crossover with Sjögren's) RNP (mixed connectivity tissue disease) Phospholipids |
|
|
Which two complements are typically measured and low in SLE? |
C3 and C4 |
|
|
Which antibody in SLE is worrisome in neonates? |
Anti-Ro – Indicating neonatal lupus causing complete heart block |
|
|
Two drugs to give to all patients with SLE |
Hydroxychloroquine NSAIDs (eg ibuprofen) (HIPIC) |
|
|
Patient with SLE is started on NSAIDs and HCQ. Next stage in management if disease persists |
Add Prednisolone or azathioprine or methotreaxate to reduce steroid exposure (HIPIC) |
|
|
Patient with SLE is on NSAIDs, HCQ and prednisolone but start experiencing Cushing's. What should you do? |
Replace prednisolone by MTX or azathioprine |
|
|
Patient with SLE is on NSAIDs, HCQ and prednisolone but disease persists. What should you do? |
Either of the following: Increased steroid dose Cyclophosphamide MMF Tacrolimus (HIPIC) |
|
|
Among the following drugs for SLE, which are not safe to use in pregnancy: HCQ NSAIDS Prednisolone Azathioprine MTX MMF Cyclophosphamide |
MTX MMF Cyclophosphamide |
|
|
Name two anti-phospholipids that may be present in SLE |
Anti-cardiolipin Lupus anticoagulant |
|
|
What are patients with anti-phospholipid syndrome at risk of (2) |
Thrombosis Fetal loss in pregnancy |
|
|
How is anti-phospholipid syndrome treated in SLE? |
Long-terms warfarin or heparin if pregnant |
|
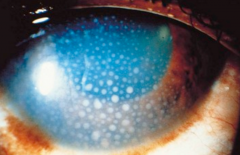
Sign and condition |
Keratic precipitates (deposition of inflammatory cells on cornea) Anterior uveitis |
|
|
What is Z-thumb deformity? When does it occur? |
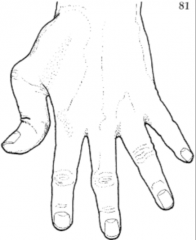
RA |
|
|
In which polyarthritis should HCQ be avoided? |
PsA |
|
|
Passively correctable swan neck deformity. What disease? |
SLE |