Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
189 Cards in this Set
- Front
- Back
|
medication for n/v which causes eps?
|
reglan
|
|
|
labs needed after incidental adrenal mass found? 3
|
catecholamines
electrolytes dexmethasone suppression test |
|
|
when should you surgically remove an adrenal mass? 3 criteria
|
- functional mass
- signs of malignancy - > 4cm |
|
|
mechanism of dz in TSS?
|
exotoxin production
|
|
|
drug of choice for htn in scleroderma
give 2nd choice too |
1. ace-i (captopril)
2. ccb will also help raynaud's but aren't first line. |
|
|
tx for localized, moderate and severe psoriasis involving nail and joints?
|
localized-- betamethasone
moderate-- puva severe with nail/ joint involvement-- mtx |
|
|
mngt of staff exposed to newly dx'd pt with tb with a neg ppd?
what if ppd is +? |
repeat in 3 months
if + start INH |
|
|
tx for severe mono
|
corticosteroids
|
|
|
next step after abnormal catecholamines levels found in pheos?
|
give alpha blockade then mri
|
|
|
electrolyte imbalance caused by vit b12 tx in pernicious anemia?
|
hypokalemia
increase k+ uptake by new rbcs deplete it |
|
|
battery of tests for suspected lead toxicity?
what if pt needs chelation? |
cbc, iron studies and retic count r/o iron def
if chelation needed: cmp, ua |
|
|
3 or more polyps, villous features and > 1cm in size..what screening?
|
colonoscopy in 3 yrs
|
|
|
in immunosuppressed pt, pulm sxs w/ sinus sxs. dx?
|
aspergillosis
|
|
|
after a neurological exam c/w brain death, which is the next step to confirm?
|
apnea test
high co2 > 60 low ph < 7.28 |
|
|
when do u know dka has resolved? 4 criteria
|
1 glc < 200
2 anion gap wnl 3 hco3 ~ 18 4 hungry pt |
|
|
mngt of dvt after first episode vs recurrent dvt?
|
warfarin or lwmh for at least 3 mo after first event.
(can dc warfarin at six mo depending on bleeding risk) recurrent dvt warrants life long tx |
|
|
3 main physical findings of pseudo-tumor cerebri
|
1 ha
2 visual loss/ obscurations 3 pulsus synchronous tinnitus (pulse tempo like whooshing sound in pt's ear) |
|
|
tx of choice for ocd
|
psychotx
med of choice is ssri |
|
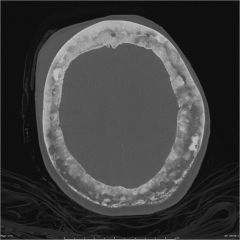
dx?
w/u? tx? |
paget's dz of bone (cottom wool on ct with bone thickening)
ca++ and akp levels biphosphonates |
|
|
causes of mat?
|
- hypoxia
- copd - electrolyte imbalances (k+, mg+) - heart dz (cad, vpt, htn..) - meds (theophylline..) |
|
|
indications for TIPS
|
failure of emergent or recurrent endoscopy to resolve variceal bleeding
|
|
|
pt with joint pain with sclerotic lesions and bowing of long bones..dx?
|

paget dz
|
|
|
which med to control tourette's tics?
which med if a/w ocd or impulsive disorder? |
tics--dopamine blockers (fluphenazine, pimozide..)
ocd--ssris |
|
|
Serious complication fo Erb's palsy?
|
diaphragmatic paralysis 2/2 phrenic nerve involvement
|
|
|
how often should baby be fed?
|
2-3 hrs
|
|
|
effective lenght of tx for latent tb?
|
9mo inh
|
|
|
mngt of warfarin in s/o hit
2 points |
- stop warfarin with heparin (warfarin alone induces venous necrosis)
- wait till plts go > 150k to restart while pt on nonheparin drug. |
|
|
failure to pass stool in newborn w/ ground glass mass or soap bubble sign on abd xr?
|
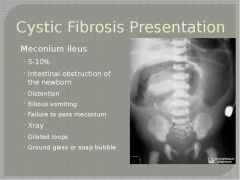
cystic fibrosis
|
|
|
lung nodules in an RA pt?
|
caplan 's syndrome
|
|
|
mngt for hiv pt dx'd with syphilis of unknown date?
whats the tx? |
- do csf to assess for neurosyphilis
- im pnc x 3 wks |
|
|
mngt of papillary ca of thyroid?
|
1 u/s of thyroid and nodes
2 if node < 1cm--> lobectomy - if node > 1cm--> thyroidectomy |
|
|
mngt of breast cyst?
|
1 aspirate
2 no residual mass?--> check if recurred with u/s 4-6 wks 3 all other mngt is mm and excision |
|
|
hiv pt who develops thrombocytopenia. whats the tx?
what condition of immunocompetent hosts is this similar to? |
1 start azt (zidovudine)..increases plt production
2 itp |
|
|
f/u of viral load?
|
6-8 wks until undetectable; then q3mo
|
|
|
fetal heart condition a/w maternal dm?
px? |
- hcom
- self-limited |
|

dx?
|
poison ivy dermatitis
(linear vesicular lesions with serous fluid) |
|
|
pt with sjogren's and submandibular mass. what ca?
|
b-cell nonhodgkin's ( sjogren's causes b-cell activation)
|
|
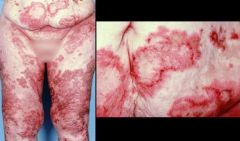
pt p/w late onset dm and this rash..dx?
|
glucagonoma
|
|
|
1- when should you suspect physiologic jaundice in newborn?
2- difference btn g6pd def and hemoglobinopathies in newborn? |
1- after 24 hrs of birth
2- hemoglobinopathies don't present early after birth bc fetal hmg predominates * suspect hemolysis in newborn with unconjugated jaundice in first 24 hrs of life |
|
|
age appropriate for heimlich maneuver?
|
> 1 yo
|
|
|
1- bp after tpa?
2- when is it ok to begin dvt ppx after tpa? |
1- = or < 180/105
2- after 24 hrs of tpa |
|
|
GBS ppx in pregos?
|
pnc 4 hrs before delivery
* asxs infants can be observed wo tx |
|
|
pt w h/o hashimoto's and enlarged thyroid.. dx?
|
thyroid lymphoma
|
|
|
mngt of torsades in stable and unstable pt?
|
- stable--> mg+
- unstable--> unsynchronized cardioversion |
|
|
difference btn GBS, botulism and tick paralysis..
|
1. tick!
2. GBS takes longer (days-weeks) vs. TP (hrs-days); csf normal in TP. 3. botulism--> descending paralysis, cn affected and pupillary dysfunction. |
|
|
recommended lenght of therapy w/ ssri depending on depressive episodes?
|
- one episode.. can dc after 6mo-1 yr
- 2 or +.. for life |
|
|
pt with prolonged malnutrition is fed. she then develops volume overload, low k and mg.. dx?, tx?
|
refeeding syndrome
tx: correct low phosphate |
|
|
pt who p/w hypertension, dm, osteoporosis, and emotional lability and the low k is found..dx?
|
r/o cushing's
dexamethasone suppression test. |
|
|
pt w/ anxiety and insomnia takes natural supp. then develops high lfts..which supp?
|
kava
|
|
|
side effect of ginko biloba?
side effect of ginseng? |
- bleeding
- psychosis and SJS |
|
|
tx for cryptococcal meningitis?
|
amphotericin B and flucytocine for 2 weeks..then switch to fluconazole if there's improvement
|
|
|
indications for cytoscopy and stone removal?
|
stone> 10mm
|
|
|
knee injury a/w dashboard trauma in mva?
|
pcl tear
|
|
|
side effect of isotretinoin?
|
teratogenic
high trigs |
|
|
which vessel involved in diverticular bleed?
|
artery of vasa recta
*venous bleeding is a/w hemorrhoids |
|
|
bitemporal hemianopsia with hyperpigmentation after adrenectomy bl...dx?
|
nelson syndrome
|
|
|
tx for warts contraindicated in pregnancy, bleeding, mucosal application and dm?
2- first line medical tx for warts? |
1- podophyllin
2- trichloroacetic acid |
|
|
criteria for parathyroidectomy in asxs pt?
|
1- 1mg > normal
2- dexa < - 2.5 3- renal failure |
|
|
diabetes
skin pigment liver dz think.. |
hemochromatosis
|
|
|
when do you use dopamine?
|
cardiogenic shock and hypotension
|
|
|
pts for whom bariatric sx is recommended?
|
bmi > 40
bmi > 35 with comorbidities |
|
|
side effect a/w saw palmetto?
|
htn
|
|
|
- prematurity
- gross motor delays (crawls but then doesn't walk) - scissoring gait dx? test to confirm? |
1- spastic cerebral palsy
2- mri |
|
|
pt p/w hyperthyroid sxs but RAIU is low..dx?
|
silent thyroiditis
|
|
|
1- tx for tca induced arrhythmia?
2- tx for cardiotoxic effects of tcas? |
1- lidocaine
2- nahco3 |
|
|
1st and 2nd line tx for skin squamous cell ca?
|
1st = xrt
2nd = 5-FU |
|
|
approach to pt w/ delayed gastric emptying? 3 steps
|
1- r/o obstruction--> egd
2- r/o compressing masses-->ct 3- r/o neuropathy--> gastric emptying scan |
|
|
pt w/ elevated lfts but almost normal akp and bilirubin..dx?
next test? |
dx: autoimmune hepatitis
test for ana and anti-smooth ab |
|
|
pt p/w ascending paralysis, sensory loss and bladder dysfunction..
dx? next step? |
dx: transverse myelitis
do MRI to r/o cord compression * guillain barre does not have sensory loss |
|
|
hiv drugs side effects:
nrtis (didanosine, azt, abacavir..) as a class? as individuals? nnrtis (efavirenz, nevirapine..) as a class? as individuals? pis as class (indinavir..) |
nrtis as a class = lactic acidosis
didanosine--> pancreatitis zidovudine--> anemia/ neotropenia abacavir--> hypersensitivity nnrtis as class = SJS efavirenz--> teratogenic neVirapine--> liVer toxicity pis = gi intolerance / lipodystrophy iNdinavir--> reNal toxic |
|
|
test for young pt who p/w with seborrheic dermatitis?
|
check hiv
|
|
|
pt w/ peripheral nerve problems (bell's), with erythema nodosum and hypercalcemia..think of?
|
sarcoid
|
|
|
return of period after stopping ocp?
|
90-3 mo beyond that needs w/u for amenorrhea
|
|
|
kid who was playing w/ cats, p/w localized LAD an fever..dx?
tx? |
cat scratch dz
tx: azythromycin |
|
|
how is cat scratch dz different from toxo? 3
|
1- toxo most commonly with cervical LAD
2- toxo p/w eye involvement but uveitis 3- mostly asx in immunocompetent pts (unlike CSD = fever) |
|
|
tx for brain mets?
|
xrt
|
|
|
pt with recent hospitalization, nm or high tsh, low t3 and normal t4..think?
|
euthyroid sick syndrome
|
|
|
mngt of hyperthyroidism in pregnancy?
what if pt doesnt know she is pregnant? |
- PTU in first trimester
- methimazole after 2- if taking MMI, switch to PTU |
|
|
tx to prevent cluster ha long term?
short term? tx acute epidoses? |
verapamil
2- steroids 3- sumatriptan |
|
|
pt w/ h/o multiple births, Dysuria, Dyspareunia and Dribbling urine..dx? next step?
|
dx: urethral diverticulum
step: transvg u/s |
|
|
when should you choose ablation of a cervical neoplasia? 3
|
1- normal colposcopy
2- glandular lesion 3- no invasion *o/w LEEP |
|

pt w/ bacteremia, in icu..bullae--> ulceration with necrosis
dx? |
ecthyma gangrenosum
look for pseudomonas |
|

purulent ulcer with violaceous borders?
|
pyoderma gangrenosum
|
|

lesions running along lymphatic channels in an outdoorsy pt?
tx? |
sporotrichosis
tx: itraconazole |
|

pt w/ maxillofacial procedure who p/w painless mass w/ sinus tracts?
tx: |
actinomycosis
tx: penicillin |
|
|
when is the tx for asx bacteriuria indicated? 3
|
- pregnancy
- urology procedures - hip replacement (foley will be needed) |
|
|
3 drugs that can cause isolated elevations of cr 2/2 decreased secretions by tubules?
|
- cimetidine
- probenecid - tmp |
|
|
contraindications for mmr vx 5
|
- pregnancy
- immunocompromised or given ivig - thrombocytopenic s/p vx - severe fever - all to neomycin or gelatin |
|
|
- malabsorptive diarrhea
- abd pain - migratory arthralgias dx? dx test? tx? |
dx- whipple's dz
test- small bowel bx tx: rocephin or pnc |
|
|
3 parameters to determine liver failure (ESLD)
|
- INR
- BIL - Cr |
|
|
htnsv of choice for pt taking lithium?
|
ccb and bb
|
|
|
parameters for parathyroidx based on ca++ and 24hr urine ca++?
|
ca++ > 11.5
24hr urine Ca++ > 400 |
|
|
why is gastrin not recommended in pt with hyperca++ and ppi tx? mngt?
|
hypercalcemia rises gastrin levels as well as ppi tx
- pt must be off ppi x 2 weeks and nml ca++ before checking gastrin if looking for men1 |
|
|
clinical manifestations of ileus? 4
|
3-5 d of:
- po intolerance - diffuse abd pain - no flatus - n/v and bloating |
|
|
2 parameters to use vanco po instaed of flagyl po?
when do you add flagyl iv? |
1. wbc > 15k
2. cr > 1.5x nml - when there's ileus |
|
|
toc for akathisia?
|
bb (propanolol)
|
|
|
mngt of salmonellosis?
|
supportive
no need for abx |
|
|
when are abx indicated in salmonellosis?
abx of choice? |
- children < 1yo
- immunosuppressed - elderly> 50 w/ artherosclerotic dz (prevent bacteremia and endocarditis) - cipro, bactrim or rocephin |
|
|
when is phototx in infant indicated?
|
total bili btn 15-20
|
|
|
how to differentiate btn folate and b12 def?
|
homomcysteine and mma level high in b12 def
- only hmocysteine high in folate def |
|
|
condition to which pt with subchorionic hematoma is at risk?
|
spontaneous abortion
|
|
|
in a patient with hyperca++ and nml pth. how do you know is familial hypercalcemia?
|
low urine ca++. hence name Hypocalaciuric
|
|
|
m/s condition a/w gonococcal arthritis?
|
tenosynovitis
|
|
|
pt gets stuck w/ hiv needle..mngt depending on vl?
|
low vl--> 2nrtis x 4wks
high vl--> 2nrtis + 1 pi x 4wks |
|
|
well's criteria? 5
score? |
- dvt sxs 3pt
- recent sx or > 3d immobile - hr>100 - hemoptisis - ca - score>4 bad |
|
|
difference btn acute glaucoma and uveitis?
|
glaucoma
- halos - n/v - increased pressure uveitis - irregular pupil - wbc on anterior chamber by slit lamp |
|
|
clinical features of allergic broncho-pulmonary aspergillosis?
dx approach? tx? |
- h/o asthma or cf
- coughing blood or brownish plugs/sputum - cxr shows upper lobes infiltrates dx: 1- skin test..serum aspergillus igE if +..if cxr neg---> hrct scan tx: glucocorticoids (prednisone..) can add itraconazole but not 1st line |
|
|
toc for postherpetic neuralgia?
alternative tx? |
tca (amytriptyline)
gabapentin if tca ci'd |
|
|
pt w/ mono who needs a node bx?
|
if lad persists for > 4 wks
|
|
|
toc for pid
alternative tx |
- cefoxitin + doxy x 14 d
- clinda + gentamycin x 14 d in pnc all |
|
|
presenting sxs of Li toxicity? 2
precipitants? 3 |
- gi sxs (n/v/d)
- neuro deficits p/ later when Li crosses bbb - diuretics, aceis and nsaids |
|
|
mngt of acute arterial occlusion of the ext?
|
1- a/c w heparin
2- angiography for tpa vs sx |
|
|
blood tests to determine sle activity? 2
|
- complements
- anti-dsdna |
|
|
pt p/w exertional sob, fatigue, syncope, ruq pain, peripheral edema, poor apetite..prob dx?
mngt? |
dx: phtn
1- tte 2- cath 3- vasoreactivity test (adenosine..) 4- if reactive..ccb / not reactive..endothelin bosentan or pde5 |
|
|
pt w/ high h/h..work up?
|
1- repeat lab
2- check ep- low? PV --> check jak - high? ct or pulseox (rcc or osa) |
|
|
difference btn amebiasis vs hydatid cyst?2
|
- hydatid often asx unless mass effect or ruptured cyst (bilary obstruction...) while ameba p/w fever, diarrhea and ruq pain.
- hydatid cyst are a/w dogs...ameba with mexico travel |
|

ataxia, lethargy, tachycardia with this rash in teenager..dx?
|
inhalant abuse
|
|
|
tx options for testicular ca?
|
orchiectomy
then: - surveillance if stg 1 - ctx - rxt if refuses ctx and noncompliant for surveillance |
|
|
clinical features of macular degenaration? 4
|
central vision problems:
- trouble reading, driving - pt needs more light - lines get distorted - scotomas |
|
|
w/u for hyperaldosteronism
|
- aldosterone concentration / plasma renin ratio
- nacl challenge test - ct |
|
|
1- presentations which give concern for endometrial ca? 3
2- approach for dx? |
- any postmenopausal woman w/ uterine bleeding
1. - premenopausal women > 45yo w menometrorrhagia - women w/ opposing estrogen states (obese, anovulatory) who persist having bleeding 2. pvu/s before bx..bx can be f/u by d/c |
|
|
mngt for pt w/ hyperuricemia wo sxs?
|
none
|
|
|
newborn that gets cyanotic with breastfeeding and improves with crying..dx? test?
|
- choanal atresia
- nasal catheter can't pass |
|
|
mngt of lead poisoning depending on severeity?
|
mild <44 no tx just remove from source
moderate btn 45-69 gets succimer po severe > 70 gets iv dimercaprol or edta |
|
|
test sequence for pcp dx?
|
- sputum induction
- bal - bx ---> helpful if pt had pentamidine ppx |
|
|
s/p renal transplant pt develops renal failure. bx shows basophilic inclusions..dx?
|
bk virus nephropathy
|
|
|
vent settings for ARDS tx? 3
|
low tv
high peep high rr |
|
|
u/s surveillance for aaa?
|
3-4 cm ---> q2-3 yrs
> 4cm ---> q6-12mo |
|
|
abx for skin mrsa infections? 3
|
- tmp-smx
- doxy - clindamycin |
|
|
pt w/ h/o ibd who has increased akp and lft..dx?
- typical presentation? |
1ry sclerosing cholangitis
- asx..if sxs, fatigue and itching |
|
|
a pt tx'd for depression who develops new onset dm and high bmi/ obesity..which drugs? 3
|
- olanzapine
- risperdal - quetiapine |
|
|
mngt with rhogam?
|
mom (-) ---> give at 28wks
mom (+) --> no need. baby has to be checked for hdn mom (-) w/ blood mix during labor ---> another dose |
|
|
when do you screen for dm in pregnancy?
|
24-28 wks
|
|
|
kid p/w fracture after minor fall, found to have splenomegaly, anemia and low plts..dx?
|
gaucher dz
|
|
|
dx criteria for pcos? 3
|
- menstrual iregularities
- hyperandrogenism - evidence of polycystic ovaries on u/s |
|
|
- indications for mv replacement in mvr?
- f/u for noncandidates for sx? |
- severe mvr w/ sxs
- asx mvr w/ new onset afib, lvh or phtn - tte q2 yrs |
|
|
indications for 3% ns?
|
- na < 120
- seizures, ams - h/o marathon runner, ectasy or polydypsia |
|
|
drug to prevent gouty attack after initiation of allopurinol?
|
colchicine
|
|
|
pt whom inr can be at goal btn 2-3 after mechanical valve replacement? 3
|
- lv normal size
- normal ef - nsr |
|
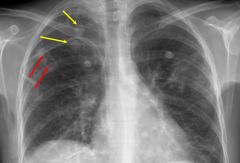
pt w/ h/o iv drug use who p/w sob and cough. cxr has this nodular opacities..dx?
|
septic pe
|
|
|
methods for the dx of schistosomaisis..2
|
- urine showing eggs
- cytoscopy with bx if urine test neg |
|
|
features of drug induced sle..3
|
- fever
- arthralgias/ myalgias - NO renal, hematologic or cns problems unlike clinical SLE |
|
|
eye pain s/p 12-24 hr of trauma, visual disturbance. on pe hypopion and retinal vessels nonvisualized..dx?
|
endophthalmitis
|
|
|
pt c/o large floater like a house fly going in and out of central view..dx?
|
retinal detachment
|
|
|
mngt of sarcoidosis with hilar lad and en. 2 points
|
- hilar lad and en require no tx if asx. only pulmonary sx are tx'd with strd
- if strd fail, use mtx |
|
|
pancreatitis inducing drugs (DIIVA)
|
- Diuretics
- IBD .. sulfazalazine - Immunosuppresors..azathioprine - Valproate - Abx..(metronidazole, tetracycline) |
|
|
tx of choice for catatonic schizophrenia?
|
benzos
|
|
|
most common complication of TURP?
|
retrograde ejaculation
|
|
|
features of hemochromatosis 7
|

- joint pain mainly on 2nd and 3rd mcp
- decreased libido - tanned skin - new dx dm - hepatomegaly - restrictive cmp - pseudo-gout features like: hooked osteophytes and rhomboid crystals on joint tap. |
|
|
vx avoided if egg allergy?
difference btn reactions to eggs w/ vx? who cannot receive live vx? |
- influenza and yellow fever
- hives only? ---> can give inactivated vx - asthma, pregnancy, immunosuppressed |
|
|
mngt of siadh
|
restrict h2o----> salt tablet and diuretics----> demeclocycline or lithium
|
|
|
pt w/ h/o iud has Actinomyces on pap smear,,mngt?
|
only tx if sxs present.
|
|
|
tx for hyponatremia in asx pt w/ edematous state?
|
main tx is h20 restriction
- 3% ns only if sxs and na < 120 *edematous state means: chf, cirrhosis... |
|
|
main clinical features of Pick's dz 4
|
- social inhibition (inapropriate comments, incontinece)
- dont care about condition rather than not knowing - repetitive and stereotyped behavior (same foods, same phrase..) - uncommon amnesia at presentation |
|
|
pt is using black cohosh for pms. what side effect?
|
hypotension
|
|
|
pt with venous insufficiency starts taking horse chesnut. what side effect?
|
bleeding, like gingko
|
|
|
agent to tx htn in aortic dissection?
|
bb
|
|
|
drugs and presentation of drug induced lupus
3drugs 4 sxs |
drugs:
procainamide hydralazine penicillamine sxs: fever myalgias arthralgias rash (discoid rare) |
|
|
1st and 2nd tx for hemochromatosis
|
1. biweekly phlebotomy
2. deferoxamine chalation |
|
|
how to differentiate tsh pituitary tumor from thyroid hormone resistance syndrome?
|
- resistance syndrome presents as hypothyroid state rather than thyrotoxic
- elevated alpha subunits are characteristic of pituitary adenomas |
|
|
when it's not necesary to taper steroids? 3
|
- tx < 3weeks
- < 5mg - every other day dosing |
|
|
differences btn necrotizing fasciitis and clostridial cellulitis? 3
|
1. in NF pain is disproportional to skin changes vs CC where pain isnt a significant finding.
2. NF has blue/gray patches with possible blisters vs CC has drainage of foul smelling d/c 3. NF involves the deep tissues (fascia/muscle/fat) vs CC only the skin |
|
|
indication for orchiopexy in undescending testes?
|
indicated if no descent by 6 mo
|
|
|
pt presents w/ bone pain and low dexa scan values. pth is high and po4 is low. ca is wnl..
dx? why is ca normal? |
dx: vit D def.
- ca is low bc pth increases bone resorption to maintain ca levels |
|
|
drugs for recent MI pts 5
|
1. asa + plavix
2. BB 3. ACEI 4. statin 5. add k sparing diuretic if ef < 40% |
|
|
drugs that cause digoxin toxicity? 4
clinical features? 4 |
drugs:
- amiodarone - verapamil - quinidine - spironolactone sxs: - n/v - fatigue/ poor apetite - color changes - st depression on ekg |
|
|
3 most common causes of MAT?
toc for copd pts? |
1- hypoxia
2- copd 3- electrolyte imbalance - verapamil for copd/ bb first line for noncopd |
|
|
mngt of acute cholangitis? 4 steps
|
1. ivf, cx, abx
2. ercp 3. biliary drainage (if ercp fails..no stones) 4. elective cholex..no need for urgent cholex |
|
|
in botulism, when do you use equine immunoglobulin vs human?
|
equine --> foodborne and wound botulism
human--> in infants to avoid anaphx and allergies |
|
|
rational for urinary retention post op? 2
|
1. anesthesia
2. ivf bolus can overdistend bladder so it cant contract |
|
|
interaction between li and hctz?
|
hctz increases levels of li by dumping na so the body reabsorbs na with li.
|
|
|
meds assoc/ w digoxin toxicity? 4
|
- verapamil
- amiodarone - quinidine - spironolactone |
|
|
pt just had a molar preg evacuated. whats the counsel and f/u?
when do you stop surveillance? mngt if abnormal test in surveillance? |
- advise to use contraception
- f/u bhcg x 1wkly - stop surveillance after 3 normal consecutive bhcg's - if high bhcg--> ctx |
|
|
pt has sarcoid by cxr..how do you confirm dx?
|
- lung bx
- if unclear, do liver * dont do liver first 2/2 morbidity and other granulomatous dz make hard to distinguish |
|
|
what risk factors for lead poisoning? 3
when do you begin to treat? mention mono and dual tx.. |
- house built < 1978
- pica - immigrant poor child - at blood lead level > 45 ---> succimer - at > 70 ---> dual tx (dimercaprol + edta) |
|
|
pt with dementia and frquent falls due to instability..dx?
causative agent if pt hallucinations get worse? |
- lewy body dementia (classic-hallucinations)
- check if given dopamine agonist (can exacerbate hallucinations) |
|
|
asthmatic pt with > 20% decreased peak flow from baseline..dx?
tx? |
asthma exacerbation
tx: oral or iv steroids |
|
|
pt has pernicious anemia. what would you see on egd?
|
- absent rugae on stomach
2/2 autoimmune metaplastic atrophic gastritis |
|
|
pt p/w le nodules and hilar adenopathy on cxr. explain tx?
|
- no tx is needed as this signs are c/w good chance of spontaneous remission.
|
|
|
pt for which hep B tx is reserved? 3
|
- immunosuppressed
- severe hepatitis/ failure ( poor anticoagulation...) - concomitant hep C |
|
|
doc for chronic prostatitis, alternative regimen and lenght of tx?
|
- quinolones
- bactrim - 6-12 wks |
|
|
tx for narcolepsy?
|
methylphenidate
|
|
|
pt has hiv and syphilis of unknown onset? next step?
whats the tx for syphylis infection? |
- check csf to r/o neurosyphylis
- benzathine x 3 wks |
|
|
pt overdoses on sulfonyureas. injection of dextrose doesnt help. what drug is indicated?
|
octreotide.
* can decrease insulin release |
|
|
drugs that intervene in the metabolism of warfarin? 5
|
- quinolones
- amiodarone - fluconazole - cephalosporins - erythromycin |
|
|
maintenance of a pt with chronic afib wo heart dz?
what if pt has lvh? what if pt has chf? what if pt has no chf? |
- flecanide
- amiodarone if lvh or chf - no chf?.. sotalol |
|
|
pt w/ addison's, dm1 and thyroid dz..dx?
|
schmidt's syndrome.
|
|
|
drugs ass/w worsened psoriasis? 4
|
- acei
- bb - nsaids - li |
|
|
when is a fna indicated in presence of thyroid mass? 3
|
- mass on u/s w/ a normal tsh
- mass suspicious for ca - high tsh with a cold/hypofnx nodule after iodine scintigraphy |