Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
265 Cards in this Set
- Front
- Back
|
5 layers of epidermis
|
Stratum corneum, lucidum, granulosum, spinosum, basale
(Can Liza grow seven babies?) |
|
|
Fingerprints are made from this layer.
|
Dermis
|
|

|
Simply a change in skin color 1 cm or less, without any elevation or depression in relation to the adjacent skin
Freckles, tattoos, hyperpigmentation, purpura Macule |
|
|
Large macules greater than 1 cm in size, without any elevation or depression in relation to the adjacent skin
Vilitigo, vascular nevus (“salmon patch”), nevus flammeus Patch |
|

|
A solid lesion elevated above the adjacent skin less than 1 cm in diameter
Warts, molluscum contagiosum, nevi Papule |
|

|
A solid lesion elevated above the adjacent skin greater than 1 cm in diameter
Eczema, psoriasis, tinea corporis Plaque |
|

|
A solid palpable lesion greater than 1 cm in diameter, frequently centered in the dermis or subcutaneous fat
Nodule |
|

|
(Small blisters) A circumscribed fluid-filled lesion less than 0.5 cm in diameter
Vesicle |
|

|
(Large blisters) A circumscribed fluid-filled lesion greater than 0.5 cm in diameter
Bulla |
|

|
Raised flesh-colored or erythematous papules or plaques that are transient lesions; they generally last less than 24 hours and may change shape and size
Wheal |
|

|
(desquamation) abnormal
accumulation or shedding of visible epidermis Scale |
|

|
Shallow losses of tissue involving only the epidermis; heals without a scar
Erosion |
|

|
Scab: hard, rough surface formed by dried sebum, exudate, blood or necrotic skin
Crust |
|

|
Honey-colored crusts (usually a sign of superficial infection)
Impetiginization |
|

|
Linear ulcers or cracks in the skin
Fissure |
|

|
Thickened skin with accentuated skin lines
Lichenification |
|

|
Due to extravasation of red blood cells into the skin (does not blanch)
Purpura |
|

|
Visibly enlarged or dilated small blood vessels on the skin surface
Talengestasia |
|

|
(Scratch marks) linear or punctate erosions induced by scratching
Excoriations |
|

|
A pebbly epidermal surface cause by a tight grouping or confluence of papules
Papillomatosis |
|

|
excessive hair growth
Hypetrichosis |
|

|
(Defect deeper than erosions), involve the dermis or deeper layers and usually heal with scarring
Ulcer |
|

|
Swollen and softened by an increase in water content; the appearance skin gets when left in water too long
Maceration |
|

|
Irregular, rough and convolutes surfaces
Verrucous |
|

|
A many-colored lesion
of concentric rings Iris |
|

|
Round like a ring
Annular |
|

|
Shaped like a net
Retiform |
|

|
Occur in proximity to one another to form a distinct larger entity
Grouped |
|

|
Resembling a cluster of flowers
Corymbiform |
|

Describe this.
|
5 cm sharply marginated erythematous annular plaque with scale on the left proximal superior medial leg
|
|

Describe this.
|
Oval, salmon-red, 2 cm plaque with a fine collarette of scale at periphery with scattered salmon-red papules and plaques on the superior chest
|
|
|
Rubbing a lesion causes a urticarial flair
|
Darier's Sign
|
|
|
Pinpoint bleeding after scale is removed
|
Auspitz's Sign
|
|
|
Pushing a blister causes further separation of the dermis
|
Nikolsky's Sign
|
|
|
Demonstrates hypersensitivity reaction
|
Patch Test
|
|
|
Minor trauma leads to new lesions at site of trauma
|
Koebner's Phenomenon
|
|
|
Labs and special exams review
|
|
|

|
Primary lesions include: discrete, skin-colored or pearly-white, raised or dome-shaped, waxy-appearing, firm papules 1 mm to 5 mm in diameter with a central keratotic plug which gives an umbilicated surface (looks like a belly button)
Molluscum Contagiosum |
|
|
What is the secondary lesions of molluscum contagiosum?
|
Secondary lesions include: crust formation on involuting lesions, excoriations on some papules, and mild scarring
|
|
|
What is the distribution of Molluscum Contagiosum?
|
MC has a macrodistribution
They are found alone or in clusters on the face, trunk, lower abdomen, pubis, inner things, axilla, and genitalia |
|
|
What is the configuration of Molluscum Contagiosum?
|
Configuration is grouped, usually within the region of onset
The number of lesions varies from 1 to 20 up to hundreds |
|
|
What is the differential diagnosis for Molluscum Contagiosum?
|
Molluscum Contagiosum
Flat Warts Condylomata Acuminata Syringoma Sebaceous Hyperplasia Invasive Fungal Infection i.e. cryptococcosis, histoplasmosis, coccidioidomycosis |
|
|
How do you diagnose Molluscum Contagiosum?
|
Diagnosis can be confirmed by incising one of the papules, smearing the contents from the center of a papule between two glass slides, staining (with Wright’s, Giemsa’s or Gram’s stain), and then viewing diagnostic anucleate homogeneous ovoid “molluscum bodies” under low magnification.
When the clinical findings are confusing and the smear is negative, do a biopsy. |
|
|
How do you treat Molluscum Contagiosum?
|
Children: conservative, non-scarring methods
Adults: genital lesions should be treated definitively to prevent spread by sexual contact New lesions that are too tiny for detection may appear after treatment and may require additional treatment. |
|
|
How is molluscum contagiosum spread?
|
Lesions are spread by autoinoculation from picking or rubbing or shaving
Advise patients against such things while lesions are present |
|

|
Veruca Vulgaris
|
|
|
What pertinent history questions do you want to ask about warts?
|
Ask if the patient is taking a mediation that may decrease cell-mediated immunity (i.e. prednisone, cyclosporine, chemotherapeutic agents)
Ask if the patient is a transplant recipient (these patients have warts that can be very resistant to treatment) Ask if the patient handles raw meat, fish, or other types of animal matter in one’s occupation (i.e. butcher). This increases susceptibility. |
|
|
What is the primary lesion of a wart?
|
Primary lesions include: tiny firm flesh-colored papules that interrupt skin lines or dermatoglyphic lines when on palms or soles. Can also see filiform (threadlike) papules, especially on the eyelid and facial areas.
|
|
|
What are the secondary lesions of warts?
|
Secondary lesions include: grey-white scaling and “black dots” or thrombosed capillaries
|
|
|
What is the distribution for warts?
|
VV have a macrodistribution
|
|
|
What is the scientific name for warts?
|
Veruca Vulgaris
|
|
|
What is the configuration for Veruca Vulgaris?
|
VV have a grouped or corymbiform configuration
May coalesce into clusters that can be up to 5 cm in diameter |
|
|
What is the differential diagnosis for Veruca Vulgaris?
|
Verruca vulgaris
Calluses Corn Verrucous carcinoma of skin Squamous cell carcinoma |
|
|
How is veruca vulgaris transmitted?
|
By touch
|
|
|
How is veruca vulgaris diagnosed?
|
Warts are diagnosed on their clinical appearance, but a biopsy can be performed if the diagnosis is in doubt. A skin biopsy will distinguish VV from other tumors and growths.
VV displaces the skin lines. |
|
|
How is veruca vulgaris treated?
|
Debridement
Keratolytic therapy (salicylic acid) Imiquimod (Aldara) 5-fluorouracil (Carac) Suggestive therapy Cryotherapy Dinitrochlorobenzene (DNCB) Glutaraldehyde Cantharone: Tends to produce doughnut warts, a wart with a central clear zone at the site of the original wart Intralesional bleomycin sulfate |
|

|
Seborrheic Dermatitis
|
|
|
What pertinent history questions would you ask someone with Seborrheic Dermatitis?
|
How frequently does she shampoo?
With what does she shampoo her hair? Does she frequently wear wigs? Infrequent shampooing, inadequate body hygiene, and climate conditions, especially long spells of wet weather, exacerbate existing cases and precipitate conditions |
|
|
What are the primary lesions of Seborrheic Dermatitis?
|
Primary lesions: dull, sharply demarcated red patches
|
|
|
What are the secondary lesions of Seborrheic Dermatitis?
|
Secondary lesions: loose, easily dislodged yellow or white scale
|
|
|
Where does Seborrheic Dermatitis manifest?
|
Post-auricular folds
Concha of the ears Eyebrows Mid-glabella Perinasal, nasolabial, and mental creases of the face Mid-chest and inframammary creases Upper back |
|
|
How do you treat Seborrheic Dermatitis?
|
Medicated Shampoo
Topical Antifungal Agents Thick crusts can be removed by applying overnight corticosteroid oil (Dermasmooth) and washing in AM Short-term topical steroids |
|
|
What is the prognosis for Seborrheic Dermatitis?
|
SD can be chronic. It is important to frequently reinforce treatment and maintenance regimens with patients. After the initial visit have patients RTC after 4 weeks.
|
|
|
What is the presentation of Pityriasis Rosea?
|
Rash abruptly begins with a single 2 to 10 cm round to oval lesion (the herald patch), which is usually salmon colored
The complaint of “ring worm” and the use of OTC antifungal creams. Within a few days to several weeks (average, 7 to 14 days) the disease enters the eruptive phase. Smaller lesions appear and reach their maximum number in 1 to 2 weeks. This phase tends to resolve over 6 weeks, but variability is common. *Only one occurance. If reoccurance, think eczema* |
|
|
What are the primary lesions of Pityriasis Rosea?
|
Primary lesions include: an erythematous to salmon-colored plaque measuring 1-2 cm in diameter. The first appearing lesion is called the “herald patch.”
|
|
|
What are the secondary lesions of Pityriasis Rosea?
|
Secondary lesions include: a collarette (or ring) of scale on the papules or plaques
|
|
|
What is the distribution of Pityriasis Rosea?
|
PR has a macrodistibution and includes the neck, chest, back, abdomen, arms, hips, and proximal thighs
PR has a “Christmas tree” distribution (this means that the lesions appear as a linear descending pattern much like the dropping branches of a pine tree) |
|
|
How do you differentiate Pityriasis Rosea from Tinea Corporis?
|
KOH
|
|
|
How do you treat Pityriasis Rosea?
|
There is no specific therapy. PR is a benign self-limiting disease that resolves on its own in a 6 to 12 week time period. It heals without permanent scars or marks, and recurrence is rare.
The following treatments can be suggested if patients are distressed with extensive lesions: Medium potency group IV or V steroid cream (triamcinalone cream) used BID x 3 weeks, avoiding face, axilla, and groin, when there is significant itching UV light Avoid hot showers, overheating or activity that raises body temperatures. This can increase itching. |
|

|
Psoriasis
|
|
|
What are the primary lesions of Psoriasis Vulgaris?
|
Primary lesions include: sharply marginated erythematous papules or plaques
|
|
|
What are the secondary lesions of Psoriasis Vulgaris?
|
Secondary lesions include: silver-white scale Scales are loose and easily removed by scratching. Removal of scale results in the appearance of minute blood droplets and this is called Auspitz’ sign.
|
|
|
What factors adversely influence Psoriasis Vulgaris?
|
Alcohol
Drugs (antimalarials, beta-blockers, ACE-I, indomethacin, interferon, lithium carbonate) Physical trauma Stress Sunlight Other factors: smoking, obesity, dyslipidemia |
|
|
What is the distribution of Psoriasis Vulgaris?
|
PV has a macrodistribution and can occur on any skin surface.
Scattered, discrete lesions, like a rash, are generally concentrated on the trunk and scalp, less on the face, and usually spare the palms and soles. EXTENSOR surfaces |
|
|
What are the physical findings of Psoriasis Vulgaris?
|
Nail changes include pitting, subungal hyperkaratosis, onycholysis, and yellowish-brown spots under the nail plate. (This is called oil spots. Oil spots are is pathognomonic for psoriasis).
Arthritis (in 10% of cases) |
|
|
How do you diagnose Psoriasis Vulgaris?
|
The diagnosis of psoriasis is made on clinical grounds. However, a skin biopsy or fungal study may be performed to rule in or rule out other possible diagnosis.
Antistreptolysin titer is increased in acute guttate psoriasis. |
|
|
How do you treat Psoriasis Vulgaris?
|
Topical agents
Phototherapy (narrow band UVB 3x/week) Systemic agents (chemotherapy drugs, hard on liver) |
|
|
A rash on limbs and trunk that is often preceeded by strep throat.
|
Guttate psoriasis
Antistreptolysin titer is increased in acute guttate psoriasis |
|

|
Onset can be acute (days) or insidious (over 2-16 weeks)
Begins as tiny papules that are geometric or polygonal in shape and can evolve into plaques Lichen Planus |
|
|
What are the primary lesions of Lichen Planus?
|
Primary lesions include: red to deep violet, flat-topped, 1 to 10 mm, sharply defined, shiny papules. These papules may be separate or tightly grouped. Thse primary lesions can have Wickham’s striae (white lines), seen best with hand lens after application of mineral oil.
|
|
|
What are the secondary lesions of Lichen Planus?
|
Secondary lesions include: scale, excoriations (due to itching), or hyperpigmentation as lesions resolve.
Erosions are common with mucosal LP. Atrophy and scarring is common with LP of the scalp. |
|
|
What is the distribution of Lichen Planus?
|
LP has a macrodistrubution
Lesions are distributed to the flexural surfaces of joints and forearms, dorsal hands, extensor shins, lateral neck, buttocks, lumbar region, glans penis, and mouth The face, scalp, palms, and soles are only rarely involved |
|
|
What is the configuration of Lichen Planus?
|
Grouped
|
|
|
What is the differential for Lichen Planus?
|
Lichen Planus
Cutaneous Lupus Erythematosus Psoriasis Eczematous Dermatitis Lichen Simplex Chronicus Pityriasis Rosea |
|
|
How do you diagnose Lichen Planus?
|
Biopsy! Lichen planus has a characteristic histology on biopsy
|
|
|
How does Lichen Planus present?
|
Severely itchy rash, often accompanied with sores in the mouth, in adults in their fourth, fifth, and sixth decades of life
Papulosquamous disease Planar Polygonal Pruritic Polished Purple Puzzling Koebnorizes |
|
|
What 2 diseases is Lichen Planus associated with?
|
There is a strong association of LP with chronic liver disease and hepatitis
|
|
|
How do you treat Lichen Planus?
|
If drug-induced, eliminate suspect medication
Superpotent topical steroids Intralesional steroid injections Systemic corticosteroids (1 mg/kg/day x 7 days, 40 for 7 days, 20 mg x 7 days, and then slowly tapering at a rate of 2.5mg/week) Narrow-band UVB Course, without treatment, 6-36 months Kids will usually outgrow LP of nails, but for all nail dystrophies: biotin 2.5 mg/day, AmLactin above matrix, and nail strengthening coating (Dermanail) |
|

|
A 16-year-old female comes to your office complaining of a pruritic generalized eruption of gradually increasing intensity over the prior 4 months
Scabies |
|
|
What are the primary lesions of scabies?
|
Primary lesions include: tiny discrete vesicles and erythematous papules, some of which evolve into burrows (the classic telltale lesions of scabies) in the interdigital webs of the hands, wrists, antecubital fossae, points of the elbows, nipples, umbilicus, lower abdomen, genitalia, and gluteal cleft
|
|
|
What are the secondary lesions of scabies?
|
Secondary lesions include: excoriations, ulcerations, hemorrhagic crusts and lichenification (these may replace the primary lesions due to the intense itch)
|
|
|
Where is scabies found?
|
Lesions are found on the finger webs, finger margins, flexor surface of the wrists, elbows, axillary folds and ankles
|
|
|
What are the symptoms of Scabies?
|
Itching (especially at night) that progressively worsens over 2-3 weeks and can persist indefinitely, thus the appellation, “the seven year itch”
Rash on hands, feet, wrists umbilicus, waistband area, axillae, ankles, buttocks, or groin Symptoms (rash and itching) in several members in the same family |
|
|
How do you diagnose scabies?
|
Diagnosis is made by identifying scabies mites, eggs, egg casings (hatched eggs) or feces (scybala) under the microscope. This is called a ectoparasite examination.
|
|
|
What is Ectoparasite Examination?
|
A drop of mineral oil is applied to the most likely lesion (usually a vesicle on the finger web or wrist is chosen). The site is then scraped with a 15-surgical blade. (Remember, to scrape con gusto! No bleeding, no bug). The scrapings are placed on a glass slide, a cover slip is applied, and examinated on low power under the microscope.
|
|
|
How do you treat Scabies?
|
After a warm bath apply permethrin (Elimite cream, Acticin cream) or lindane (Kwell) cream or lotion (only used if other agents fail or are not tolerated) to skin from “head to toe” and wash off 12 hours later, usually overnight. Repeat 1 week later.
Nails should be cut short and medication should be applied under nails vigorously with a toothbrush. If indicated, other family members and contacts should be treated simultaneously All bed linen and undergarments should be washed in hot water after treatment is completed |
|
|
What kind of follow-up should you do with Scabies?
|
Because of resistance, careful follow-up and a possible second treatment should be considered. Have patients RTC 2 to 4 weeks after treatment. Remember, symptoms or nodules may persist for weeks or months after the mites have been eradicated on the buttocks, groin, scrotum, penis, and axillae.
It is normal to itch for up to 2 months after treatment |
|
|
Erythema with scale-forming yellowish plaques on the eyebrows, nasolabial folds, glabella, and presternal area best describes:
|
Seborrheic Dermatitis
|
|
|
An acute eruption of violaceous, pruritic, polygonal, shiny, flat-topped papules involving the flexor surfaces is suggestive of which of the following?
|
Lichen Planus
|
|
|
Which of the following diseae can affect the skin, nails, and joints?
|
Psoriasis
|
|

|
A 19-year-old presents with a minimally pruritic rash as seen on the other side.
The lesion on the right arm was the first to appear followed a week later by the remaining lesions. What is the most likely diagnosis? Pityriasis Rosea |
|
|
Thickening of the epidermis secondary to scratching best describes:
|
Lichen Simplex Chronicus
|
|
|
Oil spots is pathognomonic for:
|
Psoriasis
|
|
|
What are the 4 key ingredients for acne?
|
Follicular hyperkeratinization
P. acnes Sebum overproduction Inflammation |
|
|
What is the most common cause of acne?
|
Hormones and Stress
|
|
|
What's the scientific name for clogged pores?
|
Microcomedones
|
|
|
What are white heads?
|
Closed comedones
|
|
|
What are black heads?
|
Open comedones
|
|
|
What are 3 inflammatory lesions of acne?
|
Red papules
Pustules Nodules/cysts |
|
|
What is your differential diagnosis for acne?
|
Acne Vulgaris
Rosacea Perioral Dermatitis Acne-like Drug Eruptions Gram Negative Folliculitis Pseudofolliculitis Barbae “Hot-tub” Pseudomonas Folliculitis |
|
|
What labs are required to diagnose acne?
|
No laboratory examinations required. However, if there is a suspicion of endocrine disorder free testosterone, follicle-stimulating hormone, luteinizing hormone, and DHEAS should be tested to exclude hyperandrogenism and polycystic ovary syndrome. (Note: In the overwhelming majority of acne patients, hormonal levels are normal).
|
|
|
What would you expect to see on physical exam of Grade I: Superficial, non-inflammatory?
|
Open/Closed comedones.
|
|
|
What would you expec to see on physical exam of Grade II: Superficial Inflammation
|
Comedones, mild to moderate papules/pustules
|
|
|
What would you expect to see on physical exam of Grade III: Deep Inflammatory
|
Moderate papules/pustules, few nodules
|
|
|
What would you expect to see on physical exam of Grade IV: Severe Nodulystic
|
Papules, pustules, multiple nodules, cysts
|
|

What grade of acne?
|
Grade I-II: Comedonal Acne
|
|

What grade of acne?
|
Grade III: papulo/papulopustular acne.
|
|

What grade of acne?
|
Grade IV: Nodulocystic Acne
|
|
|
How do you treat Grade I acne?
|
First Line
Topical retinoids Benzoyl peroxide Comedone extraction Second Line Alpha hydroxy acid products Salicylic acid products |
|
|
How do you treat Grade II acne?
|
First Line
Topical retinoids Benzoyl peroxide Topical antibiotics Second Line Azelaic acid |
|
|
How do you treat Grade III acne?
|
First Line
Topical retinoids Topical benzoyl peroxide Oral antibiotics Second Line Intralesional steroid injections Hormonal therapies Isotretinoin |
|
|
How do you treat Grade IV acne?
|
First Line
Isotretinoin, isotretinoin, isotretinoin… Oral contraceptives Second Line Intralesional steroid injections Incision and drainage of cysts Short courses of Prednisone |
|
|
How do Comedolytics work?
|
Combat clumping of cells and follicular plugging, anti-inflammatory.
|
|
|
How does Benzoyl Peroxide work?
|
Anti-inflammatory, antimicrobial to P. acnes (prevents development of antibiotic resistant P. acnes strains).
|
|
|
How do oral antibiotics work for treating acne?
|
Target P. acnes, anti-inflammatory
|
|
|
How do hormonal therapies work for treating acne?
|
Hormonal Therapies: Reduce circulating androgens
|
|
|
What antibiotic could cause Steven-Johnson Syndrome?
|
SMX/TMP (Bactrim)
|
|
|
How does Isotretinoin (Accutane) work?
|
*Oral retinoid (isotretinoin): Decreases sebum, corrects epidermal desquamation, anti-inflammatory, antimicrobial
Usually 20-week therapy Metabolized in liver, thus liver disease/cirrhosis is contraindicated. |
|
|
What precautions must you follow when prescribing Isotretinoin?
|
Baseline labs
2 forms birth control (abstinence is one) Labs each month: LFT, lipids, hcg 30 days of pills, no refills Office visit each month |
|
|
What are the standards in treating acne?
|
Combination therapy is standard of care for mild-moderate acne
Discontinue antibiotics when inflammatory lesions resolve (2-4 months) Continue topical retinoids to maintain remission Hormonal therapy is useful in androgen-driven acne Isotretinoin is standard of care for severe acne |
|
|
Acne, hirsutism, and irregular periods may be a sign of what disorders?
|
Hyperandrogenism and/or polycystic ovarian disease
|
|

"I leak."
"I have acne in my axilla." |
Hidradenitis Suppurativa
|
|
|
What is Hidradenitis Suppurativa?
|
Acne in the axilla
Painful red papules and/or nodules Inflamed discharging papules and/or nodules Thighs, vulva, axilla Double or bridged comedone |
|
|
How do you treat Hidradenitis Suppurativa?
|
Incision and drainage
Weight loss Intralesional injections (Kenalog 2.5 to 10 mg/ml) Antibiotics (Minocycline 100 mg BID) Isotretinoin (1mg/kg/day x 20 weeks) Surgical excision |
|

|
Presents with a localized papular and eczematous eruption (scaly) with tiny pinpoint pustules in the perioral, perinasal, or periocular areas of the face
Lacks comedones, nodules and cysts Topical acne medications will exacerbate the condition The disease steroids made famous Perioral Dermatitis |
|
|
How do you treat Perioral Dermatits?
|
NOT WITH STEROIDS!!!'
Simplify topical regimens (avoid routine use of moisturizers unless absolutely necessary) Stop BPO or steroids Mild to moderate cases use one or more of the following: Metronidazole cream (MetroGel 1% or 0.75%) q d Sodium sulfacetamide 10% (Klaron) qd Clindamycin lotion qd Erythromycin solution q d Pimecrolimus cream 1% (Elidel), and tacrolimus 0.03%, 0.1% ointment (Protopic) may by helpful Severe cases: Use a topical medication with an oral antibiotic for 4 to 6 weeks* Doxycycline 100 mg BID Tetracycline 500 mg BID Minocycline 100 mg BID *Once the condition is resolved, the antibiotic is stopped or tapered |
|

|
45 yo female with history of flushing and red face, worse over past 5-6 years, now getting “pimples” and nose looks like “Rudolph’s” in family photos.
Rosacea |
|
|
How does Rosacea present?
|
Complaining of episodic flushing, redness, and pimples on the face
Dry or red eyes, scratchiness, burning or tearing, and a sense of a foreign body being in the eye (ocular rosacea may precede skin manifestations in up to 20% of people) Enlarged blood vessels on the cheeks |
|
|
What precipitating factors can exacerbate rosacea?
|
Exposure to sun, stress, spicy foods, alcohol, hot drinks such as coffee, excessive washing of the face, or irritating cosmetics.
|
|
|
What would you expect to see on physical exam with Rosacea?
|
Papules and papulopustules on the central third of the face (forehead, nose, cheeks, and chin- the so called “flush/blush” areas)
Telangiestases and marked sebaceous hyperplasia Blepharoconjunctivitis (red, scratchy eyes) Rhinophyma (enlarged nose) |
|
|
What serious disease can develop secondary to rosacea?
|
Corneal ulcers
|
|
|
How do you treat Rosacea?
|
Patients should be advised to avoid significant environmental triggers
Apply a daily sunscreen Topical medications such as Metrogel 1% qd or Finacea gel qd are the most frequently prescribed first line therapy. Sodium sulfacetamide and sulfur topicals such as Klaron, Rosac, Plexion are also effective and used BID. |
|
|
How do you treat Rosacea if topical treatment is ineffective?
|
If topical treatment is ineffective, an oral antibiotic can be prescribed. Tetracycline 500 mg BID or doxycycline 100 mg BID noticeably improves rosacea within 3 weeks. Oracea, an anti-inflammatory low-dose doxycycline, is also effective and taken 40 mg qd.
|
|
|
How do you treat Rosacea if tetracycline and doxycycline are ineffective?
|
If tetracycline or doxycycline is not effective there are alternative antibiotics that can be used such as amoxicillin, azithromycin, or clarithromycin
Pulse Dye Lasers and Intense Pulsed Light are light treatments that can be used to destroy larger telangiectatic vessels |
|

|
Pimples and pustules in hair-bearing areas such as the face, scalp, thighs, chest and body folds. The patient usually describes them as “razor bumps” or “ingrown hairs”.
Sore on the distal nose, near the tip of the nose, or involving an eyelash Papules may be itchy Clean gym-strict about cleaning equipment Treadmill, weight machines Takes a shower at gym after soaking in hot tub Folliculitis caused by Pseudomonas aeruginosa |
|
|
What is the differential diagnosis for folliculitis?
|
Insect bites
Folliculitis/Hot tub folliculitis Acne vulgaris Transient acantholytic disease (Grover’s disease) |
|
|
What are the lesions associated with folliculitis?
|
Follicular papules, vesicles, pustules, may be crusted
|
|
|
How do you diagnose folliculitis?
|
In cases that are resistant to treatment, a bacterial culture should be done
Culturing and treating of family members should be considered in cases of chronic bacterial folliculitis |
|
|
How do you treat folliculitis?
|
Encourage good personal hygiene, including bathing, hand washing, and keeping nails short and clean
Wash with an antibacterial soap such as a benzoyl peroxide preparation (Benzac AC 5% gel or wash) Apply mupirocin 2% (Bactroban) to the NASAL vestibule TID x 5 days to eliminate the S. aureus carrier state Treat with Dicloxacillin 250-500 mg QID or a cephalosporin, such as Cephalexin 1-4 g/day in two divided does. Minocycline 100 mg BID or Septra DS BID can be used for MRSA. |
|
|
How do you treat Hot Tub Folliculitis?
|
Symptomatic relief-mild to mod topical steroid
Acetic acid compresses 20 minutes 2-4 times a day If systemic involvement, persistent infections, or immunosuppressed consider oral fluoroquinolone- such as ciprofloxacin (ex: 500-750mg po bid x 7-14 days) Prevention is preferred |
|

|
Very common inherited condition
Benign hyperkertinization of hair follicles Triceps, thighs, buttocks, and cheeks Characteristic look and feel rough small bumps-sandpaper texture sometimes inflamed, excoriated, hyperpigmented Asymptomatic to slightly pruritic Treatment often prompted by cosmetic concerns Often improves in adulthood Keratosis Pilaris |
|
|
How do you treat Keratosis Pilaris?
|
Treatment
Soapless cleansers Emollients and Keratolytics Lactic acid lotions- AmLactin, Lac-Hydrin Alpha-hydroxy acid lotions- Glytone, glycolic body lotions Urea cream- Carmol Salicylic acid- Salex Topical steroid creams (short period only) Topical retinoids |
|

|
Onset is heralded by an aura of itching and burning 12 hours before a visible lesion
Lesions have recurred at approximately the same site each time The patient clearly describes an evolution from a red welt to bump, blister, and crust Evolution of each lesion is about 10 days from start to finish Herpes Simplex Virus |
|
|
What are the physical findings of herpes?
|
Vesicular lesions that can ulcerate or form a crust
Infrequently, regional lymphadenopathy occurs |
|
|
How do you diagnose herpes?
|
The diagnosis of HSV is usually based on clinical appearance and history. When necessary, however, a Tzanck preparation can be done to determine the presence of HSV or VZV (it does not distinguish between these two viruses).
|
|
|
How do you treat herpes?
|
Options include one of the following:
Valacyclovir (Valtrex) 2 g twice daily for 1 day taken 12 hours apart Famciclovir (Famvir) 500 mg, Single dose of 1500 mg Acyclovir 400mg TID x 5 days CANNOT USE ORAL ANTIVIRALS UNDER THE AGE OF 12 |
|
|
When should oral antivirals be prescribed for an HSV outbreak?
|
Oral antivirals must be administered during the prodromal stage (first 48 hours) for optimal results.
|
|

|
Not contagious.
Sharply demarcated rash on hands, elbows, knees. Blister (HSV) is often aura to EM, but does not cause EM. |
|

|
Tender, red rash on the face, particularly in and around the nose and mouth
Small bumps with honey-colored crusts or blisters Itch Impetigo |
|
|
Describe the rash/lesions that are associated with impetigo.
|
Rash that spreads quickly and is poor to heal
Lesions are usually asymptomatic; however occasionally they itch and are painful |
|
|
What kind of primary and secondary lesions make up impetigo?
|
Bullae or vesicles with clear contents
Plaques with peripheral scale Crusts, typically honey-colored, but sometimes brown or hemorrhagic Begins as a crust or thin-roofed, fragile vesicle or bulla that ruptures, leaving a oozing eruption capped with a thick, “honey-crusted” lesion that appears “stuck on” |
|
|
What non-lesion physical findings are associated with Impetigo?
|
Regional lymphadenopathy
The face is commonly involved, particularly in and around the nose and mouth Loose white peripheral scale Hypopigmentation once rash is resolved Hyperpigmentation once rash is resolved |
|
|
How do you diagnose Impetigo?
|
Diagnosis is based on history and clinical appearance
Bacterial culture and sensitivity testing are recommended if standard topical or oral treatment does not result in improvement 50% of patients may have an increased white blood count |
|
|
How do you treat Impetigo?
|
Use antibacterial soaps twice daily
Use a warm washcloth and antibacterial soap to gently remove the crusts. Crusts should be removed because they block the penetration of antibacterial ointments. Lesions can also be soaked in warm water TID to help soften crusting and ease debridement. Apply Mupirocin 2% (Bactroban) ointment or cream TID to lesions and INSIDE OF NOSTRILS until lesions are cleared, usually 10 days. Once clear, mupirocin 2% ointment can also be applied inside the nostrils TID x 5 days each month to reduce bacterial colonization in the nares. Use an oral antibiotic, such as cephalosporin (Keflex) 250 to 500 mg QID x 7 days or dicloxacillin 500 mg BID x 7 days in conjunction with topical antibiotics in those patients with widespread involvement. If bacterial cultures reveal MRSA tetracyclines, trimethoprim/sulfamethoxazole (Bactrim), clindamycin, or linezolid are effective oral antibiotics. Good hygiene and hand washing should be encouraged. Household spread is common otherwise. If skin care is not reviewed with the patient, the chance of re-infection or persistent infection is high. Skin care details should include adjuvants to topical antibiotics. The easiest adjuvants to use for patients are the bleach bath (1 cup of bleach in a bathtub of 12 inches water and with supervision), mixing vinegar and water at a 1:4 ratio for rinsing the area, and chlorhexidine scrubs. |
|

|
Acute phase: poorly defined erythematous patches, papules, and plaques with scale
Chronic phase: lichenification (thickening of the skin with accentuation of skin markings) Atopic Dermatitis |
|
|
What two diseases are associated with atopic dermatitis?
|
Asthma and allergic rhinitis
Triad of ectopy 1. Eczema (atopic dermatitis) 2. Allergies 3. Asthma |
|
|
What are some physical findings you'd expect to see in atopic dermatitis?
|
*Allergic shiners
Morgan-Dennie lines *Pityriasis alba *Atopic palms *Ichthyosis Keratosis Pilaris *Most helpful findings in adult cases |
|
|
How do you diagnose Atopic Dermatitis?
|
If there is a question of tinea, perform a KOH to differentiate between tinea and eczema
|
|
|
How do you treat Atopic Dermatitis (Nummular Eczema)?
|
Lubricate the skin with an emollient (Cetaphil cream, CeraVe cream) TID and immediately after bathing
Eliminate excessive lengthy bathing, hand washing, and abrasive washcloths. Use a gentle soap (Cetaphil) while bathing. Do not scratch Use Group V steroid creams of ointments for red, scaling skin BID x 2 weeks. Use I or II creams or ointments for lichenified skin BID x 2 weeks. When the condition is under control, the frequency and potency of the topical steroid is reduced and discontinued. Antibiotics may be used to suppress S. aureus. Use cephalexin (Keflex) 500 mg BID x 10 days or Dicloxacillin 500 mg BID x 10 days. Minimize airborne allergens and dust Antihistamines are useful in treating children with coexistent allergies, hives or allergic rhinoconjunctivitis In severe cases, use Prednisone 1mg/kg x 10-14 days Phototherapy can induce remission in patients with recalcitrant chronic atopic dermatitis |
|
|
How does the sliding scale treatment work for atopic dermatitis?
|
Ask the patient to point out pink, red, and white spots:
Basic Rules: Short nails, short bath (3 min), cotton clothing, and cool environment; laundry- hypoallergenic detergent with no bleach or fabric softener Bath care: Antibacterial soap to skin from the neck down (do not use on face) for three minutes Bath with one ounce of emollient bath oil for 3 minutes After bath, pat dry. Do not rub. Apply emollient to entire body. Morning: Emollient to entire body, even if no inflammation (nothing red or pink). AND Medium strength topical steroid to red areas on body Lower strength topical steroid to slightly red or pink areas on body Lower strength topical steroid to pink or red areas on face Afternoon Emollient to all skin. Evening Emollient to entire body, even if no inflammation (nothing red or pink on body). AND Medium strength topical steroid to red areas on body. Lower strength topical steroid to slightly red or pink areas on body. Lower strength topical steroid to pink or red areas on face. |
|
|
Why wouldn't you use Triamcinalone for eczema?
|
Too potent for face
Not potent enough for body Overwhelms antifungal properties in combo Wrong vehicle in wrong place Wrong medicine for wrong diagnosis Too many large tubes with too many refills Patients use it for other problems when not often indicated |
|
|
What are three adverse effects of topical corticosteroids?
|
Atrophic Changes:
Skin Fragility Telangiectasia Purpura Striae Masking or promotion of infections Steroid exacerbated acne and acne-like conditions |
|
|
What are three key differential features of allergic contact dermatitis (to differentiate between atopic dermatitis?)
|
More localized distribution
Varied spectrum of pruritis No family history of atopy |
|
|
What are the differential features of Dyshidrotic Eczema/Pompholyx?
|
>5% of all hand eczema cases
Recurrent vesicles and fissures Symmetric over hands and feet Regular hand barrier therapy important |
|

|
Annular patch with distinctive raised, red, scaling, snake-like border, clearing areas in the center.
Lesions are annular, single or multiple, with central clearing, and a scaly “active border” Tinea Corporis |
|
|
Inflamed, scaly patches with areas of hair loss or hairs that are broken off close to the surface of the scalp (often called “black dot”). Tender pustular nodules or plaques called kerions may occur.
|
Tinea Capitis
|
|
|
lesions are bilateral, fan-shaped, or annular plaques with a slightly elevated scaly “active border”. It generally involves the upper thighs, the crural folds, and pubic area and buttocks but spare the scrotum and penis.
|
Tinea Cruris
|
|
|
Scale, maceration, and fissures on the foot.
|
Tinea Pedis
|
|
|
Thickened, crumbly nails, scale buildup under nails, nail discoloration.
|
Tinea Unguium (nail)
|
|
|
How do you diagnose fungus?
|
SCRAPE BORDER
Do KOH: “If it scales, scrape it!” Quick, easy to diagnose in office Only 2 times KOH required: 1. Absolutely sure not fungus 2. Absolutely sure is fungus |
|
|
How do you treat Tinea Corporis?
|
Use topical antifungal such as ketoconazole (Nizoral), econazole (Spectazole), oxiconazole (Oxistat) BID x 4 weeks or until lesions resolve
Use systemic antifungal agents, such as terbinafine (Lamisil) 250 mg po qd x 2-4 weeks when multiple lesions are present |
|
|
How do you treat Tinea Capitis?
|
Topical therapy is INEFFECTIVE
Use micronized griseofluvin 20 to 25 mg/kg/day in divided doses with milk or food until clinically cured, generally 2 to 4 months |
|
|
How do you treat Tinea Cruris?
|
Use broad spectrum antifungal agents such as ketoconazole (Nizoral), econazole (Spectazole), oxiconazole (Oxistat) BID x 4 weeks or until lesions resolve
Use a moderate strength steroid (Westcort 0.2% cream) BID x 10 days in combination with a topical antifungal |
|
|
How do you treat Tinea Pedis?
|
Use broad-spectrum antifungal agents such as ketoconazole (Nizoral), ciclopirox (Loprox), or clotrimazole (Lotrimin) applied BID x 1 month, then qd x 1 month
Use Burrow’s solution compresses TID x 10 min for oozing and maceration Keep feet dry (especially between the toes), frequently change socks, and decrease wetness by airing shoes out regularly |
|
|
How do you treat Tinea Unguium?
|
Topical therapy is ineffective
Use terbinafine (Lamisil) 250 mg/day x 6 weeks for fingernails and 250 mg/day x 12 weeks for toenails |
|

|
The main symptoms are reddish-brown slightly scaly patches with sharp borders. The patches occur in moist areas such as the groin, armpit, and skin folds. They may itch slightly and often look like patches associated with other fungal infections, such as ringworm.
Erythrasma |
|
|
What bacteria causes erythrasma?
|
Corynebacterium minutissimum
|
|
|
How do you diagnose Erythrasma?
|
Examination with a Wood’s lamp will usually produce a pink or coral-red fluorescence
KOH is negative |
|
|
How do you treat erythrasma?
|
Topical antibacterials
Azole-group antifungals (clotrimazole, econazole, miconazole, oxiconazole, tioconazole) Clindamycin lotion, erythromycin lotion Systemic therapy Erythromycin, azithromycin Posttreatment prophylaxis Cleansing with antibacterial soap, loose clothing, proper aeration of intertriginous ski |
|

|
A common superficial YEAST caused by the hyphal form of Malassezia furfur (previously known as Pityrosporum ovale and Pityrosporum orbiculare)
Patients present because of cosmetic concerns about their “blotchy pigmention” otherwise seen as hypopigmented or hyperpimented macules on the upper back, chest, arms, face, and legs Occasionally, mild pruritis Tinea Vesicolor |
|
|
What's the distribution of Tinea Vesicolor?
|
Distributed to central regions: upper trunk, upper arms, neck, abdomen, axillae (spares creases or intertriginous areas)
|
|
|
How do you diagnose Tinea Vesicolor?
|
SCRAPE!
KOH examination is positive, which have been described as having the appearance of “spaghetti and meatballs” Wood’s light examination is used to demonstrate the extent of the infection and my help to confirm the diagnosis, because lesions often fluoresce an orange-mustard color when the Wood’s light is help close to lesions in a dark room |
|
|
How do you treat Tinea Vesicolor?
|
Topical treatment includes: Ketoconazole 2% shampoo applied for 10 minutes daily, followed by a shower, or selenium sulfide suspension 2.5% applied for 10 minutes, followed by a shower, every day for 7 consecutive days
Oral treatment may be used in patients with extensive disease and those who do not respond to convention treatment or have frequent recurrences. Options include a single dose of Ketoconazole (Nizoral) 400 mg and repeated in 7 days if needed or Fluconazole (Diflucan) 300-400 mg given as a single dose and repeated if needed after 2 weeks. Prophylactic application of ketoconazole cream or shampoo once or twice weekly may prevent recurrences |
|

|
Idiopathic, asymptomatic, ring shaped grouping of dermal papules
Lesions are skin-colored or red firm papules, with no epidermal change (scale) Although any part of the cutaneous surface may be involved, lesions are most often symmetrically distributed on dorsal surfaces of hands, fingers, feet Graunuloma Annular |
|
|
How do you treat Granuloma Annular?
|
The patient should be reassured of the benign nature of this condition
Potent topical steroids Intralesional triamcinolone acetonide (Kenalog) in a dose of 2 to 4 mg/mL with a 30-gauge needle. This may be repeated in 4 to 6 week intervals. Sometimes with a punch biopsy, the GA will go away. |
|

|
Itching is produced by sensory nerve irritation as it turns sharply and enters the spinal canal
No cutaneous manifestations in acute cases Lichenified and hyperpigmentation seen in chronic cases Treatment: Inexpensive back scratcher! Nostalgia Paresthetica |
|
|
A Tzank smear demonstrating multinucleated giant cells indicates which condition?
Scabies Tinea Versicolor Impetigo Herpes Simplex Virus (HSV) |
HSV
|
|
|
Mupirocin (Bactroban) ointment is indicated for the treatment of a localized case of:
Impetigo Atopic Dermatitis Tinea Pedis Cellulitis |
Impetigo
|
|
|
Which of the following does NOT exacerbate the flushing of rosacea:
Cigarette smoking Stress Caffeine Spicy foods |
Cigarette Smoking
|
|
|
Comedonal acne is best treated with:
Benzoyl peroxide Topical antibiotics Oral antibiotics Retinoids |
Retinoids
|
|
|
How do you know if a lesion is worrisome?
|
First, know what normal looks like!
Second, ask questions Is it changing in size, color, or shape? Is it bleeding? Does it “come and go” or does it stay? How long has it been there? |
|
|
Generally flat (macule) brown with melanocytic nests at the junction of the dermis and epidermis
|
Junctional Nevus
|
|
|
Brown papule with combined histiologic features of junctional and dermal nevi
|
Compound Nevus
|
|
|
Skin colored or light brown (pinkish) raised (papule) with nests of melanocytes in the dermis
|
Dermal Nevus
|
|
|
Well circumscribed, round or ovoid lesions
2-6 mm in diameter Lesions vary greatly in size, histologic characteristic overlap, surface appearance, hair or no hair Blue, red, gray and black are not usually seen in these nevi Can look like "fried egg" |
Benign Melanocytic Nevi
|
|
|
Subcutaneous squamous epithelial lining (sac wall) with contained keratinous debris
Scalp variant known as pilar cyst Scrotal lesions often multiple Favored sites are head region, neck and trunk Variable clinical course Inflammation when contents “leak” into dermis Multiple lesions in children or in adults |
Epidermal Cyst
|
|

|
Epidermal Cyst
If fixed, worry about carcinoma. |
|
|
Pilar Cyst
Not fixed. Get bigger with time. SEND TO PATHOLOGY! |
|

|
Keloid
|
|
|
Halo Nevus
|
|

|
Sebhorreic Keratosis
|
|
|
Most common macules, papules, plaques over the age of 30
Verrucous, waxy, velvety- tan black “Stuck On” Face, neck, trunk not palms, soles, or mucous membranes Single, but often multiple Not true moles Thickened epidermis basaloid or squamous cells Various colors white, pink, brown, black and all in between |
Sebhorreic Keratosis
|
|
|
Sudden outbreak of multiple SKs can signal underlying visceral cancer (most commmon Stomach Adenoma)
|
Sign of Leser Trelat
|
|
|
SK Treatment
|
If there is any question regarding the clinical diagnosis, shave biopsy (removal) is imperative
Some will describe irritation, itching… when removing, important to note irritated seborrheic keratoses and method of removal for insurance purposes Cryotherapy is appropriate, with immediate follow-up if the lesion has not resolved in 30 days |
|
|
Fibrous growth found on the distal limbs and upper back
Irregular tan pigmentation and a fuzzy border Palpation will reveal a firm button-like tumor in the dermis and, with lateral compression, the lesion will depress downward (a positive “pucker” sign) |
Dermatofibroma
|
|
|
Usually bright red
May be multiple Asymptomatic Middle-age to elderly Trunk> extremities Can remove with cauterization |
Cherry Angioma
|
|
|
Very common in persons will oily complexions
Rasied papules with a central dell 3 to 7 mm in size White or yellowish in color Central face > trunk May mimic basal cell carcinoma (BCC) |
Sebaceous Hyperplasia
|
|
|
Dark red-violaceous
Elderly Blanchable Soft On the lips and ears |
Venous Lake
|
|

|
Venous Lake
|
|

|
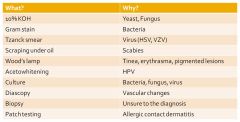
Caused by inflammed cartilage secondary to sun exposure
Chondrodermatitis nodularis chronicua helicus (CNH) |
|
|
Most common form of skin cancer
Pearly boder with telangestasia on outer rim, not in center. Metastasis is rare and usually associated only with tumors that have been neglected Treatment is needed to prevent local destruction of normal tissue A suspected BCC should be biopsied both to establish the diagnosis and treatment |
Basal Cell Carcinoma
|
|
|
What are the 5 types of basal cell carcinoma?
|
Nodular (most common): smooth, translucent gray to gray-pink papule or nodule
Ulcerating: central punched-out ulcer and a raised translucent border Pigmented: papules or nodules with flecks of brown pigmentation interspersed with gray translucent areas Morpheiform: yellow papules or plaques with dilated surface vessels Superficial: shallow plaque with a pearly border |
|
|
How do you treat basal cell carcinoma?
|
Excision
Electrodessication and curettage Imiquimod (Aldara) MOHS micrographic surgery *Most appropriate therapy depends on size, location, histologic subtype of tumor |
|

|
Basal Call Carcinoma
|
|

|
Basal Cell Carcinoma
|
|

|
Syringoma
|
|

|
Skin Tags
|
|

|
Cherry Angioma
|
|

|
Sebaceous Hyperplasia
|
|
|
Earliest lesions of squamous cell carcinoma (SCC) in sun damaged skin
More easily palpated than seen Rough texture like sandpaper Pinkish color: varying sizes Sometimes will be tender or pruritic; most often asymptomatic Usually multiple If untreated, these lesions may progress into a squamous cell carcinoma |
Actinic Keratosis
(If a presumed actinic keratosis has recurred after 2 treatments, a biopsy is warranted to rule out squamous cell carcinoma.) |
|
|
Treating Actinic Keratosis (AK)
|
Liquid nitrogen: “freezing” or “burning”, causes focal ‘frost bite’ destroying the abnormal tissue, allowing the area to heal with healthy epidermis
Topical chemotherapy: application of a topical agent, usually over 3-6 weeks, that will destroy the trouble spots. This is useful when it is difficult to determine the borders of the lesion or when there are too many lesions to destroy individually. |
|
|
Erythematous keratotic papule
Sun-damaged skin Slow or rapid growth May bleed or ulcerate May metastasize Malignant neoplasm of keratinocytes derived from the epidermis in which tumor cells have invaded the dermis May invade locally into fat, muscle, bone or cartilage Can metastasize to regional nodes and distant sites Is generally slow growing |
Squamous Cell Carcinoma
|
|
|
Keratotic, crusted nodule in sun-exposed area
Most frequent risk factor is chronic UV damage Treatment similar to BCC Most common skin cancer in immunosuppressed patients |
Squamous Cell Carcinoma
|
|
|
Arise quickly
Middle-aged to elderly Sun-exposed surfaces Dome shaped Hyperkeratotic center Frequently SCC |
Keratocanthoma
|
|
|
Frequently seen in children
Pink to red-brown Papule/ Nodule Bleed very easily Head, Neck > trunk Treat as melanoma...can be preursor. |
Spitz Nevi
|
|
|
Melanoma ABCs
|
A- Asymmetry
B-Border Irregularity C- Color D- Diameter > 6mm E- Evolution Itching can also be early symtom (may be tenderness) |
|
|
Melanoma Risk Factors
|
Red or blond hair
Marked freckling on the upper back Family history of melanoma Actinic keratosis Outdoor teen summer job |
|
|
What to tell patients with melanoma, or those at high risk.
|
Avoid unnecessary sun exposure.
Seek the shade. Cover with clothing. Wear a broad-spectrum sunscreen with SPF 30 or higher. Avoid tanning parlors. Examine skin every month, professionaly every year. |
|
|
Treatming Melanoma
|
Surgery
Adjuvant medical treatment High-dose Interferon only FDA approved therapy Some prolongation of relapse-free survival, unclear if overall survival is improved No other treatment: chemotherapy, radiation, vaccines, proven yet to improve survival |
|
|
A 1-cm pearly papule with central umbilication and telangiectasias on the left temple of a 67-year-old male is most likely:
Rosacea Basal Cell Carcinoma Impetigo Sebaceous gland hyperplasia |
Basal Cell Carcinoma
|
|

|
Spitz Nevi
|
|

|
Spitz Nevus
|
|

|
Squamous Cell Carcinoma
|
|

|
Squamous Cell carcinoma
|
|

|
Keratocanthoma
|
|

|
Keratocanthoma
|
|

|
Dermatofibroma
|
|

|
Basal Cell Carcinoma
|
|

|
Basal Cell Carcinoma
|
|
|
The use of cold temperature to treat disease
Cause epidermal-dermal separation above the basement membrane Stinging, burning pain that peaks during thawing (about 2 minutes after treatment is over) Intense edema or a blister forms 3 to 6 hours later, flattens in 2 to 3 days, and sloughs off in 2 to 4 weeks |
Cryotherapy
|
|
|
Treatment of choice for verruca vulgaris
|
Cryotherapy
|
|
|
Treatment of choice for Actinic Keratosis
|
Cryotherapy
|
|
|
Proper method of biopsy for Acrochordan (skin tag)
|
Scissors
|
|
|
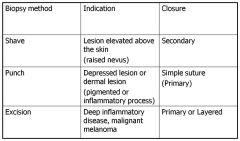
Lesions appropriate to shave for biopsy
|
Nevus
Basal cell carcinoma Squamous cell carcinoma Acrochordon Hypertrophic actinic keratosis |
|
|
Lesions apprpriate to punch for biopsy
|
Ulcerated:
Basal cell carcinoma Squamous cell carcinoma Melanoma |
|
|
Proper method to biopsy a rash or inflammatory condition
|
Punch a new lesion and one not excoriated
|
|
|
Proper method to biopsy a blister or bullous.
|
Punch straddles the blister edge and normal skin
|
|
|
Areas to discuss before performing biopsy.
|
Patient medication allergies
Is patient anti-coagulated (Coumadin, Plavix, ASA) Does patient have a pacemaker? Previous vasovagal reactions Informed patient consent Discuss the actual procedure and anticipated diagnosis Scar, Bleeding, Infection, Recurrence Discuss potential complications |
|
|
Methods to making a less painful injection
|
Inject needle quickly and smoothly
Infiltrate slowly Use small needle (30 gauge) Use topical anesthesia-cryo or cream Distract patient Verbal distraction (talk about puppies) Mechanical distraction (pinch) Sodium Bicarbonate reduces pain |
|
|
Biopsy Techniques
|
|
|
Signs and symptoms of analgesic overdose
|
Perioral and digital numbness
Lightheadedness, tinnitus, visual disturbances Fine twitching and seizures CV symptoms- hypotension, arrhythmias, respiratory and cardiac arrest |
|
|
Used to remove lesion in total
Used to sample some of large lesion Best biopsy for blistering or inflammatory conditions Usually sutured or left to granulate Anesthesia need to be deeper in skin |
Punch biopsy
|
|
|
Allows pathologist to see entire lesion
Used to remove entire lesion Deeper anesthesia Usually performed with sterile technique Always closed with sutures Try to orient with skin tension lines |
Excision
|
|
|
Shape of the incision made during excision
|
Fusiform
|
|
|
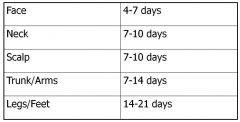
Suture Removal Timetable
|