Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
94 Cards in this Set
- Front
- Back
|
Regarding constipation, what is colonoscopy useful for?
|
Useful to identify lesions which narrow or occlude the bowel
|
|
|
Regarding constipation, when is radiography useful (plain films of the abdomen or barium enema)?
|
Useful to detect structural causes of constipation and fo rthe diagnosis of megacolon and megarectum
|
|
|
Regarding constipation, when are colonic transit tests warranted?
|
Useful in patients whose major complaint is infrequent defecation
|
|
|
A patient presents with excessive straining, incomplete evacuation and occult bleeding. Is this primary or secondary constipation?
|
Secondary
|
|
|
A patient presents with a CC of constipation with abdominal pain and rectal bleeding. Is this primary or secondary constipation?
|
Secondary
|
|
A patient presents with changes in voice register, cold intolerance and constipation. The constipation is secondary to what disease?
|
Hypothyroidism
|
|
|
On rectal exam, you note a gaping and asymmetrical anal opening. What kind of secondary constipation disease does this suggest?
|
Neurologic disorder impairing sphincter function
|
|
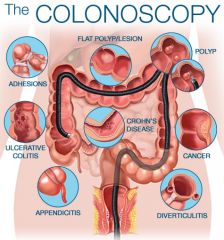
Patient's over 50 with constipation should always get what?
|
Colonoscopy for colon cancer; complete examination of the colon necessary to exclude a structural disease (colon cancer, colonic stricture) w/ recent change in bowel habits, blood in stool, or weight loss
|
|
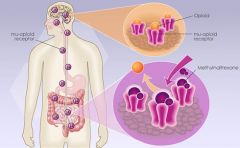
What kind of drugs are significantly associated with constipation?
|
Opioids for chronic pain; diuretics, antidepressants,antihistamines, antispasmodics (calcium channels), anticonvulstants (calcium channels) and aluminum containing antacids
|
|
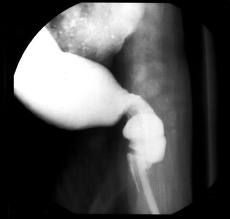
A patient presents with a proximally enlarged bowel which is narrowed distally. What is occuring in this disease?
|
Hirschsprung's disease; absence of ganglion cells in distal bowel results in overstimulation of nerves in affected region, resultin gin contraction (similar to achalasia)
|
|
A patient who recently returned from Africa reports constipation. They note that a few weeks ago they had fever and malaise. What should you consider?
|
Chaga's Disease; caused by Trypanosoma cruzi via insect vector
|
|
A patient presents with prolonged and excessive straining before elimination. You decide a patient has defecatory or rectal evacuation disorders; what kind of primary constipation is this?
|
Pelvic Floor Dysfunction
|
|

A young female presents with less than 1 bowel movement a week. She notes a lack of urge to defecate, malaise, and fatigue. What kind of primary constipation is this?
|
Slow - transit constipation;
|
|
|
How can you measure colonic transit time?
|

Pt swallows radiopague markers in gelatin capsule; abdominal x ray 120 hours after ingestion; retention in colon of radiopaque markers 5 days after ingestion = slow transit
|
|
|
What kind of conservative treatment must be attempted before anorectal testing?
|
Increased dietary fiber and liquids, elimination of medications with constipating side effects
|
|
How long does it take to expel a 50ml water filled balloon normally?
|
1 minute; abnormal expulsion indicates impaired evacuation
|
|
What does pelvic floor dysfunction refer to?
|
Inability to empty rectum effectively bc of incoordinated abdominal, rectoanal, and pelvic floor muscles; constipation is functional
|
|
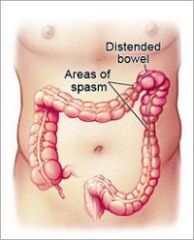
A patient presents with recurrent abdominal discomfort 3-5 days a month in the last 3 months associated with improvement with defecation, onset associated with a change in frequency and appearance of stool. What is the diagnostic of?
|
Irritable Bowel Syndrome
|
|
|
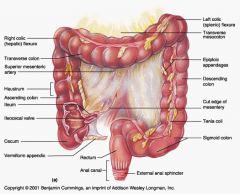
What are the four functions of the colon?
|
1. absorption of water/electrolytes
2. absorptoin of short chain FA 3. storage and transport of undigested/waste material 4. elimination of undigested material/waste products |
|
Endoscopy reveals a 'leaky' ileocecal valve. How would you expect this to affect transit time?
|
Slows transit time bc when the ascending colon contracts it will push contents back through valve, increasing transit time
|
|
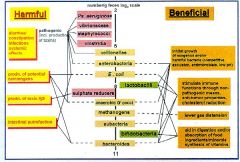
Are there dominantly aerobic or anaerobic species in the colonic microflora?
|
Anaerobic
|
|
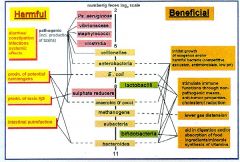
What essential things do microflora in our colon produce?
|
K, B1, and B2 (vitamins)
also short chain fatty acids when these organisms die If bacteria were eliminated the intestines would atrophy |
|
What is required for ileocecal sphincter emptying?
|
The colon must be empty; if so, pressure and chemical irritation relax sphincter and excite peristalsis
|
|

What is the large intestine transit time?
|
48-72 hours; average is around 65 hours
|
|
What effect does sympathetic stimulation have on GI valves?
|
Closes them down; pyloric, ileocecal, anal (fight or flight)
|
|
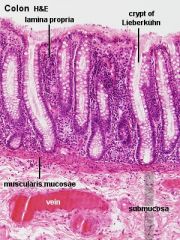
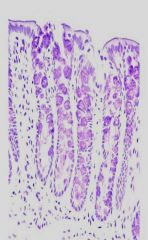
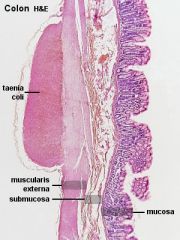
Describe the histology of the colon?
|
FLAT, simple columnar epithelia, crypts with no villi, huge goblet cell density, lots of lymphocytes in lamina propria (purple dots when stained w/ H&E) - might see lymph nodules
|
|
What do the colonic crypts secrete?
|
Mainly secrete alkaline mucus; mucus secretion increased by parasympathetic stimulation
|
|
What sympathetic nerve innervates the proximal colon?
|
Vagus
|
|
Which nerves innervate the distal colon, rectum and anus?
|
Pelvic nerves (S2-S4)
|
|
What is the sympathetic input to the rectum and anal canal?
|
Hypogastric plexus
|
|
What ganglion supplies the sympathetic input to the distal colon?
|
Inferior Mesenteric Ganglion
|
|
Which nerve ganglion supplies the proximal colon?
|
Superior Mesenteric Ganglion
|
|
Which nerves innervate the external anal sphincter?
|
Pudenal nerves
|
|
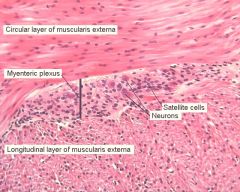
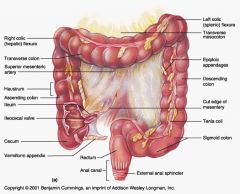
Why doesn't the myenteric plexus completely surrounding the large intestine?
|
It is only under the tenae coli, which are three longitduinal muscle bands that contract to form the haustra
|
|
What is the function of haustral contractions?
|
To mix chyme; enhances fluid/electrolyte absorption
Propels fecal material (mass movements) |
|
Describe the frequency of haustral contractions
|
appear/disappear every 30-60s; require contraction of longitudinal and circular SM
|
|
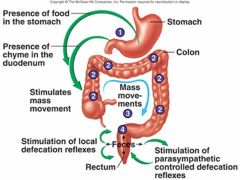
Distension of what two structures would cause mass movement in the colon?
|
Gastrocolic reflex (distention of stomach) and duodenocolic reflex (distension of duodedenum)
|
|
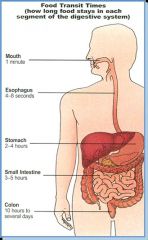
How long does it take food you eat to reach the large intestine?
|
6-8 hours
|
|

Which plexus carries the intrinsic defecation reflex (stretching of internal anal sphincter)?
|
Myenteric plexus
|
|
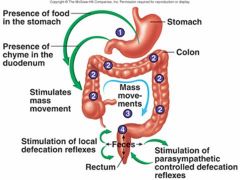
Describe the intrinsic defecation reflex
|
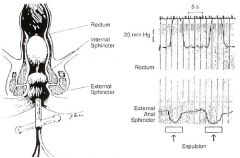
Stretching of internal anal sphincter causes upstream muscularis to contract and internal sphincter to relax
|
|
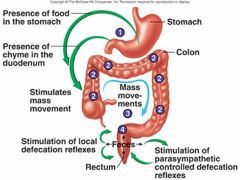
Describe the parasympathetic defecation reflex
|
Stretching of rectum sends sensory signals to spinal cord, splachnic nerves return signals intensifying peristalsis
|
|
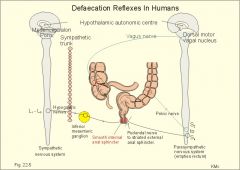
Describe the sequence of events when you want to go to the bathroom
|
Pudendal nerve activity to external anal sphincter is inhibited by input from higher brain centers -> external anal sphincter relaxes and higher centers stimulate pelvic floor muscle activity and other defectory actions -> defecation occurs
|
|
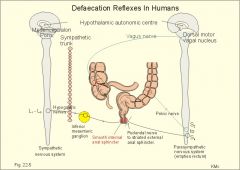
Describe the sequence of events when you don't want to go to the bathroom
|
Pudendal nerve activity is enhanced and the external anal sphincter contracts stronger -> defecation not allowed -> internal anal sphincter contracts and the urge to defecate subsides -> cycle repeats every 10-20 minutes
|
|
What is the function of the pudendal nerves?
|
External anal sphincter tone
|
|
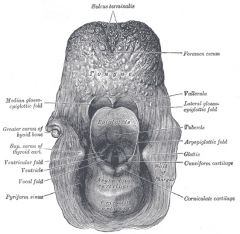
Where do fishbones always get stuck?
|
epiglottic vallecula
|
|
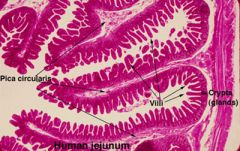
What is a characteristic morphological feature of the duodenal and jejunal lumen?
|
Circular folds/valves of Kerckring
|
|
Where is the ligament of treitz located?
|
At the duodenojejunal flexure
|
|
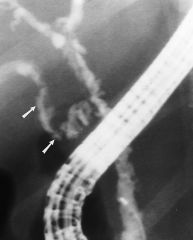
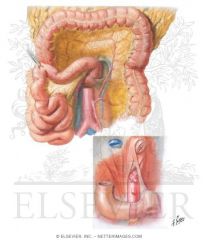
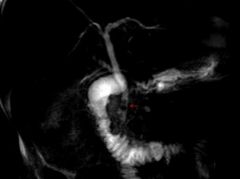
Which part of the biliary system has a spiral appearance?
|
Cystic duct
|
|
What do the hepatic and cystic duct join to form?
|
Common bile duct
|
|
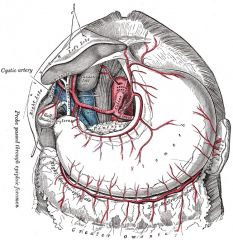
Which arteries are along the greater curvature of the stomach?
|
Gastroepiploic artery (left and right gastroomental)
|
|
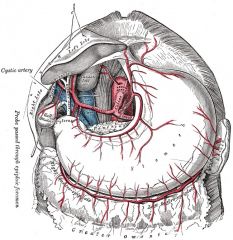
Which arteries run along the lesser curvature of the stomach?
|
Gastric arteries (right and left)
|
|
|
In an abdominal scan, where does the gas bubble in the stomach always migrate to?
|
the highest point - if laying down it will migrate up toward the pylorus, if standing up it will migrate to the fundus
|
|
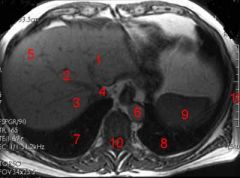
Which aorta is always adjacent and to the left of the vertebra?
|
Abdominal aorta
|
|
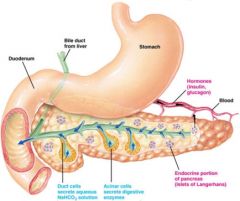
Where does the tail of the pancreas point to?
|
Spleen
|
|
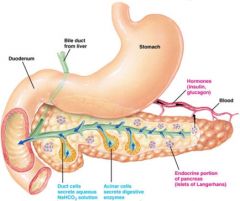
Where does the head of the pancreas connect?
|
Duodenum
|
|
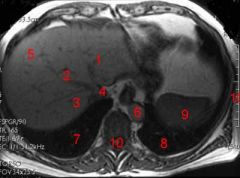
what is the relation of the inferior vena cava to the abdominal aorta?
|
the IVC is always to the left of the AA
|
|
|
What is the input, output, and function of the insular cortex in relation to ANS?
|
I: VMN of thalamus
O: Amygdala F: viscerosensory cotex for taste, visceral sensation and pain/temp |
|
A patient presents with an inability to taste, feel visceral sensation or pain and temp. What autonomic CNS structure might be damaged?
|
Insular Cortex
|
|
What is the input, output, and function of the anterior cingulate gyrus in relation to ANS?
|
I: PFC, amygdala
O: PFC, amygdala (reciprocal) F: Initiates motor/autonomic responses associated with emotional stimuli |
|
What is the input, output, and function of the amygdala in relation to ANS?
|
I: Brainstem, thalamus (pain/temp), cerebral cortex (processed sens. info)
O: hypothalamus, brainstem, spinal cord F: Coordinate autonomic, endocrine, and motor component of emotional response |
|

What is the function of the periventricular hypothalamus?
|
Circadian rhythms (suprachiasmatic nucleus SCN)
|
|

A patient presents with messed up sleep cycles. What ANS related neural structure might be damaged?
|
Periventricular area of the hypothalamus; coordinates circadian rhythms via suprachiasmatic nucleus (SCN)
|
|

What is the function of the medial area of the hypothalamus?
|
Response to stress via paraventiruclar nucleus PVN
|
|

A patient presents with a diminished stress response. Which ANS related neural structure might be damaged?
|
Medial area of hypothalamus; diminished stress response due to PVN damage
|
|

What is the function of the lateral area of the hypothalamus?
|
Arousal; sleepwake cycle; feeding/drinking
|
|

A patient has a diminished desire to eat or drink. You suspect a neurological lesion where?
|
Lateral hypothalamus
|
|
|
Which tract conveys taste/visceral sensation from nucleus of solitary tract to hypothalamus?
|
Dorsal Longitudinal Fasiculus
|
|
|
Which tract originates from the PVN and lateral hypothalamic zone to the autonomic nuclei of the brainstem and spinal cord?
|
Hypothalamospinal tract; main hypothalamic output
|
|

How can you explain the phenomenon of referred pain?
|
The proximity of visceral afferent fibers to the general somatic afferent fibers from the skin for pain produces this phenomenon
|
|
Where are the preganglionic neurons of the sympathetic system located?
|
IML cell column (T1-L3) of spinal cord
|
|
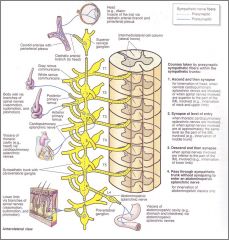
What are the two destinations of the sympathetic nervous system neurons?
|
Sympathetic trunk
Prevertebral ganglia (pass sympathetic trunk without synapse to enter splanchnic nerve) |
|
What does the prevertebral ganglia give rise to?
|
Splanchnic nerve
|
|

What neurontransmitters are used by the sympathetic nervous system?
|
Norepenephrine, and Ach/muscarinic cholinergic neurons
|
|

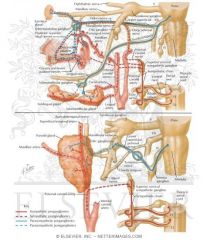
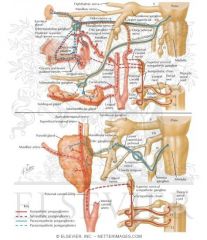
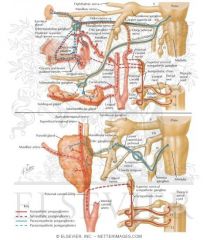
A branch of CNVII, which ganglion innervates the lacrimal gland, mucosa of nose and palate?
|
Pterogopalatine ganglion
|
|

A branch of CNVII, which ganglion innervates the submandibular and lingual gland?
|
Submandibular gland
|
|
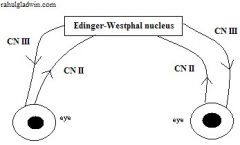
A nucleus of CNIII, what nucleus controls the sphincter papillae and ciliaris muscle?
|
Edinger-Westphal nucleus
|
|
Which parasympathetic division is involved with micturition, defecation, and sexual function?
|
Sacral division, S2-S4
|
|
|
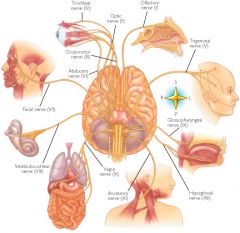
Which four cranial nerves make up the parasympathetic cranial division?
|
CN III, VII, IX, X
|
|

What NT is used by postganglionic parasympathetic innervation?
|
Ach/muscarinic cholinergic receptor
|
|

Activation of CN V2 branches of the greater palatine nerve, lesser palatine nerve, and nasopalantine nerve all result in what?
|
RUNNY NOSE
|
|

If histamine in an allergic reaction activates the petrosal nerve pathway of CNVII what is the end result?
|
LACRIMATION
|
|

If the chorda tympani nerve pathway of CN VII is activated what is the end result?
|
SALIVATION via submandibular/sublingual salivary glands
|
|
If the CN IX pathway is activated what is the end result?
|
Salivation via parotid gland
|
|
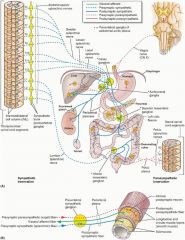
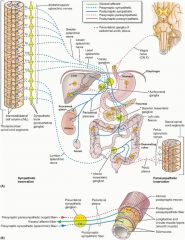
Which cranial nerve supplies major nerve supply to GI tract?
|
CN X; controls GI motility via myenteric plexus in the foregut and hindgut
|
|

Activation of CN V2 branches of the greater palatine nerve, lesser palatine nerve, and nasopalantine nerve all result in what?
|
RUNNY NOSE
|
|
The sacral division of the ANS supplies nerve supply to what structure?
|
Hindgut (last 1/3 of transverse colon, descending colon, sigmoid colon, rectum
|
|
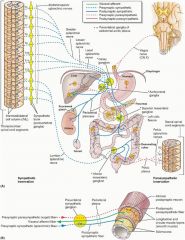
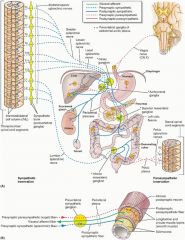
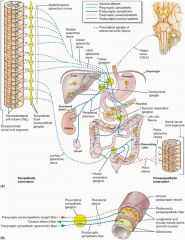
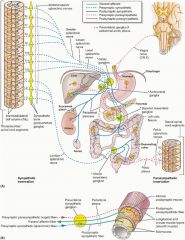
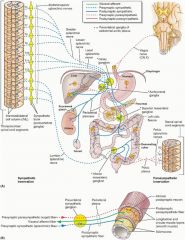
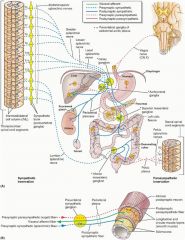
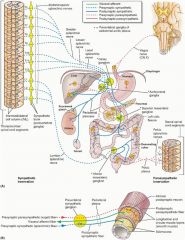
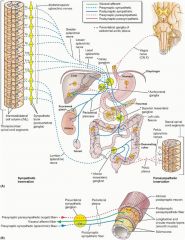
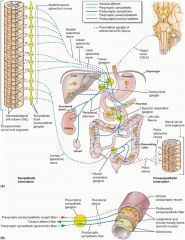
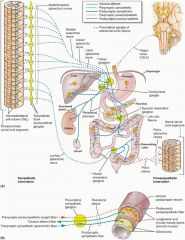
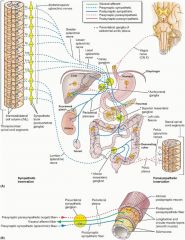
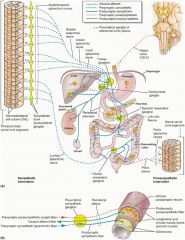
Describe the sympathetic and parasympathetic innervation of the foregut?
|
S: Greater splanchnic nerve (T5-T9) > Celiac Ganglion > Target
PS: Vagus Nerve |
|
If histamine in an allergic reaction activates the petrosal nerve pathway of CNVII what is the end result?
|
LACRIMATION
|
|
If the chorda tympani nerve pathway of CN VII is activated what is the end result?
|
SALIVATION via submandibular/sublingual salivary glands
|
|
|
Describe the sympathetic and parasympathetic innervation of the midgut?
|
S: Lesser (T10-T11) and least (T12) splanchnic nerves > superior mesenteric ganglion > target
PS: Vagus nerve |
|
If the CN IX pathway is activated what is the end result?
|
Salivation via parotid gland
|
|
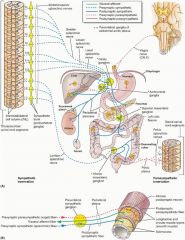
Describe the sympathetic and parasympathetic innervation of the hindgut?
|
S: Lumbar splanchnic nerves (L1-L3) > inferior mesenteric ganglion > target
PS: Pelvic splanchnic nerves (S2-S4) > pelvic plexus > target |
|
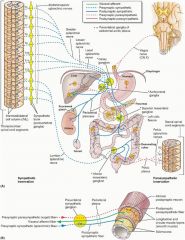
Describe the sympathetic and parasympathetic innervation of the internal anal sphincter?
|
S alpha-1 adrenergic receptor
PS: pelvic splanchnic nerves relaxation via VIP, NO or both |
|
Which cranial nerve supplies major nerve supply to GI tract?
|
CN X; controls GI motility via myenteric plexus in the foregut and hindgut
|