Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
104 Cards in this Set
- Front
- Back
|
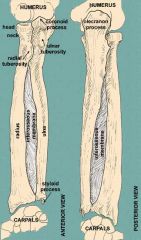
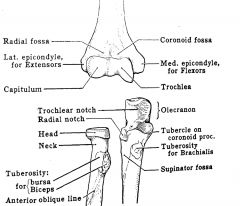
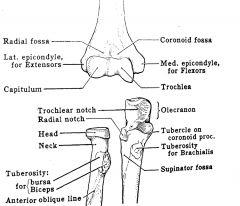
What is considered lateral; radius or ulna
|
radius
|
|
What does the capitellum of the humerus articulate with
|
the radius
|
|
|
What does the trochlea of the humerus articulate with
|
the ulna
|
|
|
Which bone contains the olecrannon
|
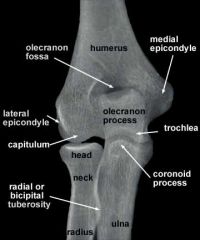
the ulna (this wraps around the trochlea)
|
|
|
What is inbetween the olecrannon and the trochlea
|
Not best picture...see next slide for the location
|
|
|
Where is the coronoid process of the elbow
|
not labeled but is opposite the olcranneon process and forms the groove for the trochlea
|
|
|
What is the bigger bone at the elbow
|
the ulna
|
|
|
What bone articulates with the capitellum of the humerus
|
radius
|
|
|
What is the bigger bone at the elbow
|
the ulna
|
|
|
What bone articulates with the capitellum of the humerus
|
radius
|
|
|
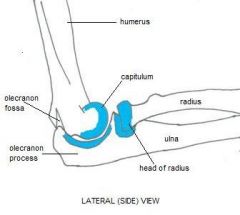
Where is the trochlea and capitellum of the humerus
Where do the extensor and flexor tendons attach |
|
|
|
Where is the trochlea and capitellum of the humerus
|
|
|
|
Where is the radialcapitellum line
|
|
|
|
Can a radialcapitellum line be drawn on any view of the elbow
|
yes, it should always pass through the capitellum no matter what view
|
|
|
When is the anterior humeral line normally drawn
|
a true lateral along the anterior aspect of the distal humerus
|
|
|
What should the anterior humeral line pass through when it is drawn on the lateral elbow xray
|
middle 1/3 of capitellum
|
|
|
What is the location of the fat pads around the elbow
|
extrasynovial and intracapsular
|
|
|
Where are the two fat pads located
|
anterior and posterior (distal humerus)
|
|
|
What does the normal anterior fat pad look like
|
a triangular shaped radiolucency just above the capitellum seen on the lateral view of the elbow
|
|
|
Should a posterior fat be normally visualized on lateral x ray
|
no
|
|
|
What does the anterior fat pat look like in the presence of a joint effusion
|
elvated and convex outwards
|
|
|
What is the anterior fat pad in the presence of a joint effusion said to look like
|
a spinnaker sail of a sail boat
|
|
|
Where is the posterior fat pad located
|
distal posterior humerus just above the distal portion of the olcreanon process
|
|
|
What % of people with a posterior fat pad sign have a fx
|
70-90%
|
|
|
What is the MC elbow fracture in children
|
supracondylar fracture
|
|
|
What percent of all fractures in children are supracondylar fractures
|
60%
|
|
|
What is the mc age of children that have supracondylar fractures
|
3-10
|
|
|
What is the MC mechanism of injury of a supracondylar fracture
|
fall on outstretched arm with extension at the elbow
|
|
|
What are 2 complications of supracondylar fractures
|
cubitus varus ( bowed inward angulation of the distal segment of a bone or joint) and brachial artery injuries
|
|
|
What is the anterior humeral line important for diagnosing
|
displacement of the capitellum, dislocation
|
|
|
What commonly happens to the capitellum in supracondyar fractures
|
the capitellum is displaced posteriorly so the anterior humeral line will pass through the anterior 1/3 or miss the capitellum completeley
|
|
|
what is the mc elbow fracture of an adult
|
fracture of the radial head
|
|
|
What is the MC mechanism of injury of a radial head fracture
|
fall on outstretched hand
|
|
|
What is a chisel fracture
|
a longitudinal fracture through the radial head
|
|
|
What is the 2nd MC fracture in adults
|
olecranon fractures
|
|
|
What are the 2 mc mechanism of injury of an olecranon fracture
|
FOOSH (fall on outstretched hand) or direct blow
|
|
|
What does the olecranon and coronoid process form
|
the trochlear notch
|
|
|
Is an olecranon fracture intrarticular
|
yes bc it passes into the trochlear notch
|
|
|
What is the mc direction of an olecranon fracture
|
transverse
|
|
|
Does a transverse olecranon fracture cause a wide space
|
yes, there is distraction of the distal portion of the olecranon fracture bc it is being pulled by the tricep
|
|
|
What is the radial capitaleum line useful for finding
|
capitellum movement bc of a supracondylar fracture or dislocation of the elbow,
|
|
|
Are olcraneon fractures association with elbow dislocation
|
yes
|
|
|
What is a potenial problem of an olecranon fracture
|
non-union
|
|
|
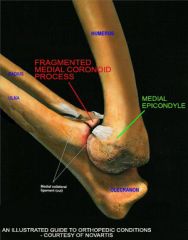
What is the 3rd mc fracture of the elbow in adults
|
fracture of the coronoid
|
|
|
What 2 other injuries is a coronoid process fracture associated with
|
radial head fractures and elbow dislocations
|
|
|
What happens to the elbow if the coronoid process fracture is left untreated
|
instability leading to dislocation. Greater than 50% of the coronoid must remain intact for stability to be intact
|
|
|
What is the MC dislocation in children
|
elbow dislocation
|
|
|
What is the 1st and 2nd MC dislocation in adults
|
1-shoulder
2-elbow |
|
|
How do elbow dislocations MC occur
|
fall on extended/abducted arm
|
|
|
How is an elbow dislocation classified
|
by the ulna relative to the humerus
|
|
|
What is MC; anterior or posterior elbow dislocations
|
posterior (80-90%)
|
|
|
What is the MC mechanism for an anterior dislocation
|
strong blow to posterior aspect of flexed elbow
|
|
|
What is associated with neurovascular injuries; anterior or posterior dislocations
|
anterior
|
|
|
What is a monteggia fracture dislocation
|
fracture of the proximal ulna with anterior dislocation of the radial head
|
|
|
What is a nursemaids elbow
|
this is when the radial head slips out of a loose annular ligament in a child
|
|
|
What age do nursemaids elbows most commonly occur
|
2-4 years of age
|
|
|
What is the mechanism of injury of a nursemaids injury
|
tugging of an extended arm
|
|
|
Are x-rays sensitive for detecting nursemaids elbow
|
no, it is mostly a clinical diagnosis and often will see nothing on x-ray or maybe mild subluxation
|
|
|
What should be done when examining a pediatric elbow
|
get a normal opposite side for comparison
|
|
|
What are 3 areas that lead to pitfalls in patholgoy
|
trochlea
lateral epicondyle olecranon |
|
|
What is the appearance of the trochlea in a child
|
fragmented
|
|
|
What is the appearance of the lateral epicondyle in a child
|
1 or more ossification centers
|
|
|
What is the appearnance of the olecranon
|
2 or more ossification centers
|
|
|
What is the order of ossification of the elbow (CRITOE)
|
capitellum
radial epiphysis internal (medial) epicondyle (closer to the ulna) trochlea olecranon external (radial) epicondyle |
|
|
What is the age of critoe
|
C- 1
R- 3 I- 5 T-7 O-11 |
|
|
Why is it important to know the order of ossification of the pediatric elbow
|
because if these are out of order then there is a fracture
|
|
|
What is the cause of a fracture of the medial epicondyle
|
pull of the ulnar collateral ligament
|
|
|
What is the cause of a fracture of the medial epicondyle
|
cause by throwing motion
|
|
|
What age does a fracture of the medial epicondyle occur
|
around the age of 12 years (little league)
|
|
|
What is a fracture of the lateral condyle considered in a child
|
a salter 4 injury
|
|
|
What is the mechanism of injury of a fracture of the lateral condyle
|
traction/avulsion
|
|
|
What is the MC age for a lateral condyle injury
|
4-10
|
|
|
Why are condyle fractures of the elbow worrisome
|
they may be associated with growth abnormalities
|
|
|
When does the apophysis of the olecranon fuse
|
18 years
|
|
|
When does the apophysis of the olecranon appear
|
9 years
|
|
|
Can the apopyhsis become fractured
|
yes, associated with throwing
|
|
|
What is a pitfall of the olecranon apophysis fusing
|
it fuses anterior to posterior and therefore there may be a small cleft of lucency posteriorly as the olecranon is fuses on the posterior margin which may be mistaken for a fracture
|
|
|
What percent of fractures are upper extremity
|
almost 50%
|
|
|
What is the most common injury of upper extremity injuries
|
FOOSH or direct blow
|
|
|
What is the most common body part injured in skate boarding
|
forearm
|
|
|
What is the appearance of the radius and ulna on lateral view
|
superimposed on eachother
|
|
|
What is the appearance of the radius and ulna in supination view
|
the radius and ulna are parellel to eachother
|
|
|
What portion of the forearm is most commonly fractures
|
the distal 1/3 (75%)
|
|
|
What does a monteggia and galleazzi fracture have in common
|
a fracture and dislocation of other bone
|
|
|
What is the mechanism of a monteggia fracture
|
direct blow or forced pronation during a fall
|
|
|
What is a monteggia fracture
|
fracture of proximal ulna (with distal fragment angulated dorsally) and an anterior dislocation of the radial head
|
|
|
What is a monteggia equivalent
|
combination of proximal radial fracture and ulnar shaft fracture
|
|
|
What are the complications of the monteggia fracture
|
limitation of movement and non-union
|
|
|
What is more common: galeazzi fracture-dislocation or monteggia fracture-dislocation
|
galeazzi
|
|
|
What is a galeazzi fracture
|
fracture of the distal 1/3 of the radius with shortening and posterior dislocation of the distal ulna
|
|
|
What are the complications of a galleazzi frx
|
non-unionn or delayed union
malunion |
|
|
What bone is fractured in a monteggia fracture
|
ulna
|
|
|
What bone is fractured in a galeazzi fracture
|
radius
|
|
|
What is acute plastic bowing
|
deformation of the bone secondary to longitudinal stress
|
|
|
What is the age group that acute plastic bowing occurs
|
2-5
|
|
|
What is the pathophysiology of acute plastic bowing
|
numerous microfractures on concave surface of the bone with intact cortex and convex surface
|
|
|
What is the mc location of acute plastic bowing
|
forearm
|
|
|
What is the most common radiographic finding of acute plastic bowing of the elbow
|
bowing of the ulna with fracture of the radius
|
|
|
What is the mechanism of acute plastic bowing
|
FOOSH
|
|
|
What is seen on bone scan of a pt with acute plastic bowing
|
increased uptake on the concave surface of the bone where numerous microfractures have occured
|
|
|
What is a nightstick fracture
|
a fracture of the ulna from direct trauma
|
|
|
What portion of the ulna do nightstick fractures most commonly occur
|
the middle 1/3rd
|
|
|
What is an apophysis
|
growth plate
|
|
|
What is an apophysis
|
growth plate
|