Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
130 Cards in this Set
- Front
- Back
|
What are the 2 major locations of atheroscleoric disease that requires angioplasty
|
aorto-iliac
fem popiteal |
|
|
What is the inflow location of atherosclerotic disease
|
aorto-iliac
|
|
|
What is the outflow location of atherosclerotic disease
|
fem-pop
|
|
|
What other locations have atherosclerotic disease that may require angioplasty
|
tibial-pedal and renal
|
|
|
What types of lesions typical respond well to angioplasty
|
short stensosis that are non-calcified
|
|
|
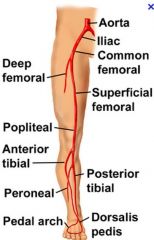
When refering to tibial pta what is really being referred to
|
posterior tibial
anterior tibial peroneal artery |
|
|
What is the anatomy of the lower extremity arteries
|
|
|
|
What is the anatomy of the iliac arteries
|
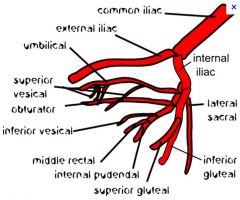
internal iliac goes posteriorly
|
|
|
What direction does the internal iliac artery go
|
posteriorly
|
|
|
Why are IR docs more hesitant to do tibial (meaning anterior, posterior or peroneal) artery PTA
|
the risk are greater
|
|
|
What are the indications for PTA of the tibial arteries and peroneal artery
|
limb salvage
rest pain gangrene or ulcers graft salvage |
|
|
Do you typically experience rest pain with an ABI less than 0.4
|
yes
|
|
|
What is considered hemodynamically significant
|
greater than 50% stenosis
|
|
|
What does 50% stenosis correspond to in cross-sectional area
|
75% reduction
|
|
|
What amount change in blood pressure across a stenotic area is considered significant at rest
|
10mmhg
|
|
|
What are indirect signs of hemodynamic significant stensosi
|
collaterals
decrease kidney size |
|
|
When do you measure pressure of a stensois
|
if u are unsure if the pressure gradient is hemodynamically significant
|
|
|
What two measurements are important in PTA
|
length and diameter
|
|
|
What is the optimal balloon diameter
|
10% larger than the normal unaffected vessel
|
|
|
What is the optimal balloon length
|
spans the lesion and does not extend more than 1 cm on either side
|
|
|
What is the size of the guide wire for standard balloons
|
0.035 inches
|
|
|
What is the size of the guide wire for small vessel balloons
|
0.018 inch
|
|
|
Where are smaller vessel balloons typically used
|
coronary arteries
tibial vessels |
|
|
What is the size of a ballon for the renal artery
|
6mm
|
|
|
What is the size of a ballon for the common iliac artery
|
10mm
|
|
|
What is the size of a ballon for the external iliac artery
|
8mm
|
|
|
What is the size of a ballon for the SFA
|
6mm
|
|
|
popitieal vessel
tibial vessels |
5mm
3-4mm |
|
|
What should occur prior to performing PTA
|
heparinized to prevent thrombosis
|
|
|
What should you do if a thrombosis occurs
|
give TPA
|
|
|
Do infrarenal aortic and Iliac vessels have good prognosis
|
yes, 70-80% typically stay patent in 3-5 years
|
|
|
Do femorpopiteal and infrapopiteal have good long term patency
|
not as good 20-80%
|
|
|
What is the treatment of choice of FMD
|
PTA without stent placement
|
|
|
What is the success of doing angioplasty for renal vascular disease
|
85% (atherosclerosis is less at 64%)
|
|
|
What are the complications of PTA
|
puncture site (hematoma, psuedoaneurysm)
PTA site (acute thrombosis,rupture) Distal (thromboembolism, cholesterolembolism) |
|
|
What are the complications at the puncture site
|
puncture site (hematoma, psuedoaneurysm)
|
|
|
What are the complications at the PTA site
|
PTA site (acute thrombosis,rupture)
|
|
|
What are the complications at the distal site
|
Distal (thromboembolism, cholesterolembolism)
|
|
|
What are the 2 MC complications
|
hematoma at the puncture site and acute thrombosis at the PTA site
|
|
|
What also commonly occurs following PTA
|
intimal dissection (technically not a complication unless it obstructs flow)
|
|
|
What happens to the intima when the balloon is blown up
|
it cracks and will cause a focal dissection
|
|
|
Where are stents used most commonly
|
iliac arteries
|
|
|
What is the rationale for using a stent
|
better immediate result and better long term patency
|
|
|
What are 2 ways a stent can be deployed
|
primary or secondarily
|
|
|
What is meant by deploying a stent primarily
|
?
|
|
|
What does it mean to deploy a stent secondarily
|
this means if the results of the PTA are suboptimal a stent can be used as a secondary option. Primarly just means starting out with a stent
|
|
|
Besides the iliac vessels where else are stents uses
|
renal arteries and heart
|
|
|
What are 2 types of stents that are available
|
the balloon expandable
self expanding |
|
|
What is the prototype of the balloon expandable stent
|
palmaz stent (genesis is another type of balloon expandable stent)
|
|
|
What is needed to deploy the palmaz stent
|
a balloon
|
|
|
What is an example of a self expanding stent
2 |
wallstent
Nitinol stent |
|
|
What is an advantage of the nitinol family of stents
|
less shortening
|
|
|
Why is a palmaz stent not commonly used for the SFA
|
because people cross there legs and it may crush the stent
|
|
|
What is a stent graft
|
a metallic stent covered with fabric (dacron, gortex)
|
|
|
What is the MC indication for a stent graft
|
infra-renal abdominal aortic disease
|
|
|
What is the MC stent graft used in the US
|
Zenith stent graft
|
|
|
What does a zenith stent graft look like
|

deploys with suprarenal fixation which increases stability
|
|
|
What is a type 1 endoleak
|
leak at proximal and distal attachments
|
|
|
What must be done to treat common iliac artery aneurysm
|
use covered stent that extends into the external iliac artery
|
|
|
Why is important to embolized the internal iliac artery if you are treating a common iliac artery aneurysm with a graft stent
|
if you dont you will get a type 2 endoleak
|
|
|
What is a mneuomic for the branches of the internal iliac artery
|
I Love Going Places In My Very Own Underwear:
Ileolumbar Lateral sacral Gluteal (superior and inferior) Pudendal (internal) Inferior vesicle (uterine in females) Middle rectal Vaginal Obturator Umbilical |
|
|
What is fibrinolysis
|
another name for thrombolytic therapy
|
|
|
What is used for fibrinolysis
|
tissue plasminogen activator
|
|
|
What is plasmin
|
this is a byproduct of plasminogen and spits fibrin into fibrin split products
|
|
|
What is fibrinolysis used for
|
acute or subacute thrombus in native vessels or grafts
|
|
|
What is a loose cutoff for the use of fibrinolysis
|
less than 2 wks
|
|
|
What is a very common indication for fibrinolysis
|
clottted grafts
|
|
|
What are the contraindications of fibrinolysis
|
recent surgery
GI bleeding recent stroke brain mets threatened limb (do embolectomy) |
|
|
What should be done in the case of motor or sensory deficit in a limb
|
embolectomy
|
|
|
What are some fibrinolytic agents
|
TPA
Urokinase Tenecteplase reteplase (recombinant TPA) |
|
|
Do pts undergoing fibrinolytic therapy often undergo adjunctive heparin therapy
|
yes
|
|
|
What is the normal dosage of TPA
|
1mg/hr
|
|
|
How is TPA administered
|
through a side hole catheter lodged in the thrombus
|
|
|
What labs should be followed on a patient on TPA
|
H/H
PTT (bc on heparin) Fibrinogen (important) |
|
|
What is the lowest fibrinogen can go
|
150
|
|
|
When does lysis most commonly occur
|
with in 24-48 hours
|
|
|
What are the complications of fibrinolysis
|
bleeding (puncture site or systemic)
Embolization |
|
|
How long do you typically allow fibrinolytic therapy to occur
|
48 hrs then discontinue
|
|
|
What is the most feared complication of fibronlysis
|
bleeding into the brain
|
|
|
What percent of pts undergoing fibrinolysis have bleeding in the brain
|
0.4%
|
|
|
What are some indication of therapeutic embolization
|
control of GI bleeding
treatment of fibroids palliate malignancy traumatic injury (organ bleeding) |
|
|
What are 4 embolic agents that are commonly used
|
liquids
particulates coils balloons |
|
|
What are 2 types of liquids that are used for embolization
|
alcohol and glue
|
|
|
What are 2 types of particulates that are used as embolic agents
|
gelfoam and ivalon
|
|
|
What 2 tpes of embolic agents are not commonly used
|
liquids (very specialized indications)
balloons |
|
|
What are the 2 most commonly used embolization agents
|
particulates
coils |
|
|
What are the exmples of particulates
|
gelfoam
polyvinyl alcohol (Ivalon) collagen embospheres |
|
|
How is Ivalon specified
|
by size (150-200 microns etc)
|
|
|
Are collagen and embospheres also specified by size
|
yes
|
|
|
Are gelfoams considered a temporary agents
|
yes usually will embolize for 2-3 wks
|
|
|
Is collagen commonly used as an embolization agent
|
no
|
|
|
What are the common sizes of coils
|
0.018 ir 0.035 inches
|
|
|
What are the shapes that coils are seen
3 |
striaght, looped and shaped
|
|
|
Why is GI bleeding embolization not as common
|
medical treatment has improved and cauterization with an UGI is now commonly done
|
|
|
What is the treatment if cauterization and medical treatement of an upper GI bleed fails
|
gelfoams or coils
|
|
|
What must you be sure to do if you are treating a GI bleed with coils or gelfoams
|
embolize the collaterals
|
|
|
What is the treatment of lower GI bleeding
|
microcoils, gelfoam, Ivalon
|
|
|
What is the risk of infarction with lower GI bleeding embolizaton
|
5-20%
|
|
|
What is the more common indication upper or lower GI embolization
|
lower
|
|
|
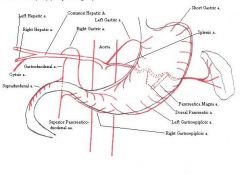
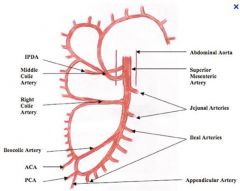
What major abdominal arterial vessel supplies the stomach and doudenum
|
celiac
|
|
|
What are the vessels of the celiac
|
left gastric
hepatic, GDA splenic |
|
|
What are the vessels of the celiiac axis
|
|
|
|
What supplies the midgut
|
the superior messenteric artery
|
|
|
What are the vessels of the SMA
|
|
|
|
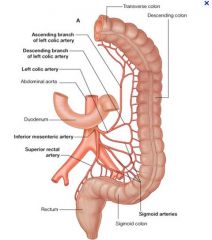
What are the vessels of the inferior mesenteric artery
|
|
|
|
Does the SMA supply the descending colon
|
not normaly
|
|
|
What supplys the left colon, sigmoid and superior rectum
|
IMA
|
|
|
Where is the MC location of the origin of the IMA
|
left pedicle of L3
|
|
|
Where is the MC location of the origin of SMA
|
right pedicle of L1
|
|
|
What is the success of treating a mallory weiss and gastric tear
|
80 %
|
|
|
What is the success rate of doudenal
|
50-70 % (lower because of the collaterals between the celiac and SMA)
|
|
|
Can vasopressin be used to treat lower gi bleeds
|
yes
|
|
|
What must you follow if vasopressin (ADH) is used
|
sodium levels
|
|
|
When is uterine artery embolization performed
|
post partum bleeding
ectopic bleeding post surgical bleeding fibroids |
|
|
What is uterine artery embolizaton MC used for
|
the treatment of fibroids
|
|
|
What is the embolic agent that is most common
|
embospheres (plastic micropspheres)
|
|
|
Why do the fibroids die and the normal myometrium stay intact following uterine artery embolization
|
there are collaterals to the uterus and the normal myometrium does not require as much blood as the the fibroids
|
|
|
What liver malignancy are treated with embolization
4 |
HCC
metastatic carcinoid metastatic islet cell tumors metastatic sarcomas |
|
|
Besides liver malignacies what else is commonly treated with palliative embolization
|
kidney lesion
osseous mets |
|
|
What is embolization for palliation of malignancy done with
|
mixture of lipiodol, chemotherapy and particulate agents
|
|
|
What does TIPS stand fro
|
transjugular intrahepatic portosystemic shunt
|
|
|
What are the vessels that get distended with portal htn
|
umbilical
gastro-esophageal IMV-mesenteric rectal spontaneous splenorenal shunts |
|
|
What are the indications for TIPS
|
variceal bleeding
ascites (refractive to medical tx) |
|
|
What is hepatohydrothorax
|
ascites that goes into chest because of holes in the diaphragm
|
|
|
How is the TIPS placed
|
through the jugular vein into the hepatic vien through the hepatic parenchyma into the portal vein
(right hepatic vein to right portal vein) |
|
|
What is the goal portosytemic gradient
|
less than 12mmhg (portal pressure - right atrial pressure)
|
|
|
What is the diameter of TIPS
|
8mm to 12mm
|
|
|
What type of stents are typically used
|
uncovered (wallstent) and covered (Viatorr)
|
|
|
What are the immediate complications of TIPS
|
bleeding
liver failure renal failure stent migration |
|
|
What is the MELD score used for regarding TIPS
|
determines who will survive TIPS procedure
|