![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
537 Cards in this Set
- Front
- Back
|
What is a closed-ended question? |
A question that limits the information from the client. Only a set number of responses is allowed. |
|
|
"What brings you to therapy?" is an example of a ________-ended question. |
open |
|
|
The most important question to ask a client during the subjective interview is ___________________. |
What are your goals? |
|
|
The best way to prevent the spread of disease is to _______. |
Wash hands |
|
|
To be classified as a restraint in an acute care setting, it must be a physical restraint. |
No. There are also pharmacological restraints. |
|
|
A common problem following prolonged bed rest is a drop in BP with a change in position also known as: |
Orthostatic hypotension |
|
|
Name the two conditions discussed in lecture one that are commonly seen in Patients admitted to ICU. |
Critical illness polyneuropathy (CIP) and Critical illness myopathy (CIM) |
|
|
You are treating a patient in the ICU with respiratory failure. He is developing distal extremity weakness, wasting, sensory loss, paresthesias, and decreased DTRs. What is the likely diagnosis? |
CIP |
|
|
Name the two conditions discussed in lecture one that are commonly seen in Patients admitted to ICU. |
Critical illness polyneuropathy (CIP) and Critical illness myopathy (CIM) |
|
|
You are treating a patient in the ICU with respiratory failure. He is developing distal extremity weakness, wasting, sensory loss, paresthesias, and decreased DTRs. What is the likely diagnosis? |
CIP |
|
|
This ICU related condition is also known as acute steroid myopathy. |
CIM |
|
|
You are treating a patient in the ICU when generalized weakness (especially in the large proximal muscles), decreased DTRs, but no loss of sensation. What is the likely diagnosis? |
CIM |
|
|
What is an observable finding called? Ex/ skin integrity |
Sign |
|
|
Always start your subjective interview with a(n) _______-ended question. |
Open |
|
|
In your own words, how would you describe pain affect? |
How much a person is bothered by their pain....not the intensity. |
|
|
Name the 4 pain scales covered in lecture 1. |
NRS, VAS, faces and non-verbal |
|
|
Cutaneous pain is usually well _______. |
localized |
|
|
Somatic pain can be divided into the following four categories: |
Deep somatic Somatovisceral Viscerosomatic Somatoemotional |
|
|
Pain that is felt at a site distant from its cause is known as: |
Referred pain |
|
|
Pain that corresponds to specific spinal root(s) is known as: |
Radiating pain |
|
|
Pain that corresponds to specific spinal root(s) is known as: |
Radiating pain |
|
|
The area of skin that is innervated by a single spinal nerve is called a |
Dermatome |
|
|
Pain from this structure is typically described as throbbing. |
Arterial |
|
|
Information from a client's chart should be put in the ____ section of a SOAP note. |
Hx |
|
|
A description of your next session or sessions with a client should be described in which section of a SOAP note? |
Plan |
|
|
Systemic or Musculoskeletal? Does not occur for years without progressing. |
Systemic |
|
|
Systemic or Musculoskeletal? Described as knife life, cutting, boring. |
Systemic |
|
|
Systemic or Musculoskeletal? Awakens person at night without obvious recent injury. |
Systemic |
|
|
Systemic or Musculoskeletal? Described as knife life, cutting, boring. |
Systemic |
|
|
Systemic or Musculoskeletal? Awakens person at night without obvious recent injury. |
Systemic |
|
|
Systemic or Musculoskeletal? Symptoms are typically changed by rest or position. |
Musculoskeletal |
|
|
Systemic or Musculoskeletal? Pain may be accompanied by other symptoms such as fever, changes in vision, bilateral symptoms, GI symptoms, etc. |
Systemic |
|
|
Systemic or Musculoskeletal? Described as knife life, cutting, boring. |
Systemic |
|
|
Systemic or Musculoskeletal? Awakens person at night without obvious recent injury. |
Systemic |
|
|
Systemic or Musculoskeletal? Symptoms are typically changed by rest or position. |
Musculoskeletal |
|
|
Systemic or Musculoskeletal? Pain may be accompanied by other symptoms such as fever, changes in vision, bilateral symptoms, GI symptoms, etc. |
Systemic |
|
|
The ______ pleura is insensitive to pain, therefore conditions can be quite advanced before recognized. |
Visceral |
|
|
The four components of pharmacokinetics are... |
Absorption Distribution Metabolism Elimination |
|
|
What is the term for the excessive and unnecessary use of medications? |
Polypharmacy |
|
|
What is the term for the time it takes for the amount or concentration of a drug to fall by 50% in the body (typically in the plasma). |
Half-life or t1/2 |
|
|
What is the term for the level at which initiation of alteration of cellular activity begins? |
Threshold level |
|
|
In pharmacology, what does TD50 and ED50 stand for? |
Toxic dose Effective dose |
|
|
How do you calculate the therapeutic index? |
TD50 / ED50 |
|
|
Benzodiazepines are used for anxiety and have the suffix ______ or ______. |
-zepam or -zolam |
|
|
Lunesta and Ambien are anti-anxiety medications that are often prescribed to help individuals fall asleep. These drugs are agonists to the neurotransmitter _______. |
GABA |
|
|
Name a few of the drugs in the antieplileptic/anticonvulsant category. |
Klonopin, oxcarbazepine, keppra, Dilantin, trileptal, tegretol |
|
|
In class we discussed three mechanisms of action for antidepressants. Name them. |
MAOIs SSRIs SNRIs |
|
|
Most antipsychotics are _______ antagonists. |
Dopamine |
|
|
What is a common and expected, but usually undesirable action of a medication? |
Side effect |
|
|
Most of the antiParkinsonian drugs are ______ agonists. |
Dopamine |
|
|
Drugs for the treatment of Alzheimer's usually involves increasing the concentration of the neurotransmitter __________. |
Acetylcholine |
|
|
What is an unexpected, severe, and dangerous reactions which may occasionally occur with a medication? |
Adverse drug reaction |
|
|
Name the three drug administration routes. |
Topical Parenteral Enteral |
|
|
Which administration route has the largest first-pass effect? |
Enteral |
|
|
What is the term that describes the percentage of unchanged medication that reaches systemic circulation? |
Bioavailability |
|
|
If you want a drug to pass more easily through tissues throughout the body....you should make it _________-soluble. |
Lipid |
|
|
Metabolism or biotransformation of drugs primarily occurs in the ______. |
Liver |
|
|
Drugs bind to specific receptors, preventing naturally occurring (endogenous) chemicals from binding to the receptor. In so doing, if a drug enhances cell activity, it is called an __________. |
Agonist |
|
|
Antagonist drugs are divided into two categories....name them. |
Competitive Non-competitive |
|
|
What is the difference in dose vs dosage? |
Dose is how much is given at one time. Dosage includes the frequency and duration. |
|
|
What is the difference in dose vs dosage? |
Dose is how much is given at one time. Dosage includes the frequency and duration. |
|
|
Blood cells in adults originate in the _______. |
Bone marrow |
|
|
Antiepileptics are also known as: |
Anticonvulsants |
|
|
An immature RBC is called a |
Reticulocyte |
|
|
A life-threatening disorder that involves widespread clotting and hemorrhaging. |
Disseminated intravascular coagulation |
|
|
Which lab test primarily assesses the extrinsic coagulation pathway? |
PT |
|
|
Which lab test primarily assesses the intrinsic coagulation pathway? |
PTT or aPTT |
|
|
Normally, the body responds to endothelial tissue injury via the __________ clotting path first. |
Extrinsic |
|
|
In the chloride shift, chloride levels tend to be higher when CO2 levels are _______. |
Low |
|
|
In respiratory acidosis, the kidneys can attempt to compensate by increasing the level of ________ into the blood. |
Bicarbonate |
|
|
Excessive vomiting and/or diarrhea will ______ the pH. |
Raise |
|
|
What does CBC stand for?
|
complete blood count |
|
|
What is the normal range for RBCs
|
4.2-5.4 million/microliter |
|
|
Will dehydration falsely raise or lower your RBC count?
|
raise |
|
|
What is the normal range for Hgb?
|
|
|
|
If your Hgb is less than ____, exercise is contraindicated but basic ADLs may be OK.
|
8
|
|
|
What is the normal range for HCT?
|
37-52 (% of RBCs in whole blood) |
|
|
If your HCT is less than _____, exercise is contraindicated, but basic ADLs may be OK.
|
25% |
|
|
HCT should be about 3x greater than _______.
|
Hgb |
|
|
What is the normal range for MCVs?
|
80-100micrometer3 |
|
|
If a person is sick or injured, you might expect their ESR to ____________ (increase or decrease).
|
increase |
|
|
The normal range for WBCs is ____________cell/microliters
|
4,500-11,000
|
|
|
The normal range for platelets is ____________cells/microliters
|
150,000-450,000
|
|
|
If the platelet count is less than _________, exercise is contraindicated but basic ADLs may be OK.
|
20,000 |
|
|
What components are in the medical CBC shorthand diagram
|
WBC
Hbg HCT Plts |
|
|
Name the three lab tests that are related to clotting ability or potential.
|
PT, PTT and INR |
|
|
What is the normal PTT time?
|
60-70 seconds |
|
|
What is the normal PT time?
|
|
|
|
What is the normal range for INR?
|
.8-1.0 |
|
|
A PT should use caution when treating a patient with an INR greater than __________.
|
4.0 |
|
|
What is the normal range for sodium?
|
135-145 mEq/L |
|
|
Sodium level is a major determinant of ___________.
|
fluid volume |
|
|
The normal range for potassium is _______.
|
3.5-5.0 mEq/L |
|
|
Potassium is a critical determinant of _____________________.
|
cell excitability |
|
|
The normal range for chloride is ______________.
|
95-105 mEq/L |
|
|
What is the normal range for calcium?
|
9-11 mg/dL |
|
|
What is the normal range for magnesium?
|
1.5-2.5 mEq/L |
|
|
What is the normal range for bicarbonate?
|
22-28 mEq/L |
|
|
The key function of bicarbonate is to _______.
|
assist in the maintenance of normal pH
|
|
|
Normal blood pH is from _______ to __________.
|
7.35 to 7.45 |
|
|
What is the range of normal blood glucose?
|
80-120 mg/dL |
|
|
Name the two renal function lab tests that may be elevated with kidney dysfunction.
|
creatinine and BUN
|
|
|
What is the normal range for creatinine?
|
.5-1.5 mg/dL |
|
|
What is the normal range for BUN?
|
5-30 mg/dL |
|
|
Which values are in the medical shorthand for metabolic labs? |
NA K Cl HCO3 BUN Creatinine Glucose |
|
|
What is the normal for total cholesterol?
|
less than 200 mg/dL |
|
|
Normal O2 sats should be between __________ and ____%.
|
95 and 100 |
|
|
What is a common tool used in the ICU to assess a patient's status, track progress, and estimate parameters such as length of stay and mortality risk?
|
APACHE II |
|
|
If you receive a blood transfusion using your own blood, it is called an _________ transfusion.
|
autologous |
|
|
What blood type is the universal donor?
|
type O |
|
|
Name the five reasons for a person to go into shock (low BP which leads to decreased arterial blood circulation and insufficient profusion).
|
hypovolemic, cardiogenic, obstructive, septic, and neurogenic |
|
|
Name some of the causes of anemia.
|
blood loss destruction of erythrocytes decreased production of erythrocytes |
|
|
Leukocytosis is diagnosed if a person's WBC count is greater than _____.
|
10,000 |
|
|
Leukopenia is diagnosed if a person's WBC count is less than _____.
|
5,000 |
|
|
Thrombocytosis is diagnosed when the platelet count is greater than _________.
|
450,000 |
|
|
Thrombocytopenia is diagnosed when the platelet count is less than ______.
|
150,000 |
|
|
Name the inherited autosomal recessive disorder that changes the shape of RBC and leads to anemia, stroke, vasoocclusion, fatigue, hypoxia, and jaundice.
|
Sickle Cell Disease |
|
|
Name the inherited disease that causes chronic hemolytic anemia due to extremely thin, fragile erythrocytes.
|
thalassemia |
|
|
Name the disease that is an inherited X-linked recessive bleeding disorder.
|
hemophilia |
|
|
What is disseminated intravascular coagulation?
|
Condition that leads to simultaneous hemorrhaging and clotting. Life-threatening. |
|
|
Name the disease that is the most common inherited bleeding disorder.
|
von Willebrand's disease |
|
|
The drugs Warfarin (Coumadin) and Heparin are all in the drug class called ____________.
|
anticoagulants |
|
|
Aspirin and Plavix are in the drug class called _______.
|
antiplatelets |
|
|
Aspirin inhibits the action of platelets by blocking both the ____I and ____II enzymes.
|
COX |
|
|
Statin drugs are used to lower __________.
|
cholesterol |
|
|
The drug Neupogen is used to increase the number of ___________ in the blood.
|
WBCs |
|
|
The drug Epogen or Procrit is used to increase the number of __________ in the blood.
|
RBCs |
|
|
If your pH is high, CO2 is low and bicarbonate is nornal, what is the diagnosis? |
Uncompensated respiratory alkalosis
|
|
|
If your pH is low, CO2 is high and bicarbonate is normal, what is the diagnosis? |
Uncompensated respiratory acidosis |
|
|
If your pH is low, CO2 is high and bicarbonate is high, what is the diagnosis? |
Partially compensated respiratory acidosis |
|
|
If your pH is low normal, CO2 is high and bicarbonate is high, what is the diagnosis? |
Fully compensated respiratory acidosis |
|
|
If your pH is high, CO2 is normal and bicarbonate is high, what is the diagnosis? |
Uncompensated metabolic alkalosis |
|
|
If your pH is high, CO2 is high and bicarbonate is high, what is the diagnosis? |
Partially compensated metabolic alkalosis |
|
|
If your pH is normal high, CO2 is high and bicarbonate is high, what is the diagnosis? |
Fully compensated metabolic alkalosis |
|
|
If your pH is low, CO2 is normal and bicarbonate is high, what is the diagnosis? |
Uncompensated metabolic acidosis |
|
|
If your pH is low, CO2 is low and bicarbonate is low, what is the diagnosis? |
Partially compensated metabolic acidosis |
|
|
If your pH is low normal, CO2 is low and bicarbonate is low, what is the diagnosis? |
Fully compensated metabolic acidosis |
|
|
If your pH is high, CO2 is low and bicarbonate is low, what is the diagnosis? |
Partially compensated respiratory alkalosis |
|
|
If your pH is high normal, CO2 is low and bicarbonate is low, what is the diagnosis? |
Fully compensated respiratory alkalosis |
|
|
The five cardinal signs of inflammation are... |
Rubor Calor Dolor Tumor Loss of function |
|
|
Immediately after an injury to a vessel, the vessel _______. |
Vasoconstricts |
|
|
After a vessel injury, platelets start to adhere to the damaged vessel wall and release.... 1. ______ and ______ to increase platelet aggregation. 2. ______ and ______ to increase vessel permeability and dilation. 3. ______ to increase WBCs to the area. |
Thromboxane and PAF Serotonin and histamine Growth factor |
|
|
Activated mast cells release: 1. 2. 3. |
Serotonin Histamine Prostaglandins |
|
|
The medical term for hardened, dry non-viable tissue in a wound bed is called _________. |
Eschar |
|
|
Coagulation factors are formed in this organ. |
Liver |
|
|
Fibrinogen only converts to fibrin at the ______ site. |
Wound |
|
|
Which specific type of WBC is the first to arrive and aggregate at the site of injury? |
Neutrophils |
|
|
Typically, non-human cells (bacterial) are marked for destruction by __________ or by WBCs recognizing a non-human molecular pattern on the surface of their cells. |
Antibodies |
|
|
The growth of new blood vessels is called _____. |
Angiogenesis |
|
|
To fill in a wound, new granulation tissue must be made. The primary cell responsible for this tissue formation are _______. |
Fibroblasts |
|
|
Name the two processes for wound healing. |
Repair Regeneration |
|
|
Name the two processes for wound healing. |
Repair Regeneration |
|
|
If a wound is closed with sutures, staples, skin glue, etc....it will heal via ______ intent. |
Primary |
|
|
What are the three phases of wound healing? |
Hemostasis/Inflammatory Proliferation (fibroplastic) Maturation |
|
|
Name some key vitamins or other blood components that are key to wound healing. |
Vitamins A, C, E, K, zinc and protein |
|
|
Muscle relaxants and antispasmodic both work by serving as agonists to the neurotransmitter _____. |
GABA |
|
|
The following prefixes and suffixes are all representative of this class of drug. cort -olone -onide pred -some |
Corticosteroids |
|
|
The main problem with COX-2 specific inhibitor NSAIDS is _________. |
Clotting....leading to stroke or MI |
|
|
Bacteria produce either _________ or _________ to damage human cells.
|
endotoxins exotoxins
|
|
|
Which type of virus embeds itself into DNA to produce new RNA. This new RNA creates proteins that embed into the host cell membrane creating a channel which dooms the host cell?
|
RNA
|
|
|
Which type of virus produces new RNA which becomes antigen on the cell surface, so the human immune system will kill the host cell...thus the method is called "indirect."
|
DNA
|
|
|
The end product of the clotting cascade is the formation of ____________.
|
fibrin |
|
|
This type of exudate is thin, clear yellow and watery. It is typically found in the early stages of inflammation.
|
serous
|
|
|
The extrinsic arm of the clotting cascade can best be tested using the _______ lab test.
|
PT |
|
|
Endothelial injuries such as infections, burns, hypoxia, acidosis, shock and cardiopulmonary arrest typically involves the __________ pathway in the coagulation cascade.
|
intrinsic
|
|
|
As the wound fills in with granulation tissue, the overall size of a wound starts to shrink, this is due to which cell?
|
myofibroblasts
|
|
|
Following an injury, which COX pathway leading to the formation of prostaglandins is most active? (causes more platelet aggregation)
|
Cox 1
|
|
|
The suffix -fenac and -profen represent this type of drug class.
|
NSAID
|
|
|
The suffixes: -olone -onide -sone represent this type of drug class. |
corticosteroid
|
|
|
What is a pathogen?
|
A disease-causing agent
|
|
|
The term antigen can represent two things....can you describe them?
|
1. a substand that when introduced into the body stimulates the production of antibodies. 2. the self-identifying molecules on the surface of cells |
|
|
What is the specific portion of an antigen that elicits an antibody response called?
|
epitope
|
|
|
The skin/mucosal barriers and the non-specific inflammatory response together make up the 1st line of immune defense called ______________ immunity.
|
innate
|
|
|
Which type of vaccination would be expected to last for a lifetime (or many years)?
|
active immunity...you are given a weakened pathogen and the body makes antibodies in response (including some memory cells).
|
|
|
Class I HLA markers are found on ________ cells.
|
all
|
|
|
Class II HLA markers are found on _________ cells.
|
select white blood
|
|
|
Neutrophils are also known by this abbreviation...
|
PMNs
|
|
|
Pus is mostly composed of ____________, debris and dead pathogens.
|
neutrophils
|
|
|
Which two types of myeloid phagocytic cells are involved in allergic responses?
|
basophils and eosinophils
|
|
|
Which type of lymphocyte is key for humoral immunity?
|
B
|
|
|
Which type of lymphocyte is key for cell-mediated immunity?
|
T
|
|
|
Antibodies are produced by __________ cells.
|
plasma
|
|
|
B cells will only convert to plasma cells after confirmation from ___________ cells.
|
helper t
|
|
|
Cytotoxic T cells only recognize antigens in the grasp of Class ____ HLA markers.
|
I
|
|
|
Helper T cells only recognize antigens in the grasp of Class ____ HLA markers.
|
II
|
|
|
To activate a helper T cell, the match with a class II marker and antigen on a WBC must be confirmed with a _________ protein.
|
CD4
|
|
|
To activate a cytotoxic T cell, the match with a class I marker and antigen on an infected cell much be confirmed with a _____ protein
|
CD8
|
|
|
Name the cells that are large granular lymphocytes that are able to kills infected and transformed cells without match confirmation. (but still need cytokine activation)
|
NK cells
|
|
|
This autoimmune disorder is unique in that is often produces antibodies against many different tissue components including RBCs, neutrophils, platelets, organs, tissues, etc.
|
Systemic Lupus Erythematosus (SLE)
|
|
|
What is the name for a hospital acquired injection?
|
nosocomial
|
|
|
Name the six modes of disease transmission.
|
contact enteric vector airborne droplet vehicle |
|
|
Which type of immune cell is most impacted by HIV infection?
|
T helper
|
|
|
Name the viral disease that primarily affects the liver.
|
hepatitis
|
|
|
Which type of hepatitis is transmitted via a fecal/oral route from he ingestion of contaminated food or water.
|
HAV
|
|
|
Which disease is caused by the same virus that causes chicken-pox?
|
shingles
|
|
|
Name some of the common super bugs.
|
MRSA VRE pseudomonas acinebacter baumannii C-Diff |
|
|
This disorder primarily affects children and may be a cause of the development of asthma.
|
RSV (respiratory syncytial virus)
|
|
|
Most often infects bones and especially common infection after joint replacements.
|
Staph
|
|
|
Gas gangrene is caused by ____________.
|
Clostridial myonecrosis
|
|
|
This disease is highly contagious and affects all tissues but mostly associated with the lungs.
|
Tuberculosis
|
|
|
Multi-systemic disease that is spread by a tick-borne spirochete. It's the most prevalent vector-borne infectious disease in the US.
|
Lyme disease
|
|
|
This class of medications often as these suffixes: -cillin -cycline -micin -mycin |
antibiotics
|
|
|
This class of medications often has this suffix: -nazole |
antifungal
|
|
|
This class of medications often has this suffix: -vir |
antiviral
|
|
|
What are some general symptoms/signs of infection?
|
fever, chills, sweating, malaise, N/V
|
|
|
Which PT practice area are most likely to work with patients with bloodborne pathogens? (trick question)
|
all
|
|
|
Universal precautions is now called __________ precautions.
|
standard
|
|
|
There are three types of transmission-based precautions, can you name them?
|
airborne droplet contact |
|
|
The best way to prevent the spread of infection is to ____________.
|
wash your hands
|
|
|
Your employer will have an _________ ________ plan where you can find all of the policies and procedures related to bloodborne pathogen management.
|
exposure control
|
|
|
If you encounter a potential bloodborne pathogen (blood splash, etc)...what should you do first?
|
decontaminate
|
|
|
When should you tell your supervisor after encountering a potential bloodborne pathogen?
|
immediately after decontamination
|
|
|
How long should you wash your hands?
|
30 seconds
|
|
|
Which body fluids are potentially contaminated with bloodborne pathogens?
|
all
|
|
|
Patients isolated due to an airborne pathogen are placed in a _________ pressure room.
|
negative
|
|
|
If you are treating a patient with a _________ or _________ pathogen, it is vital that you wear a moisture resistant mask.
|
airborne or droplet
|
|
|
The posterior pituitary releases:
|
ADH and oxytocin
|
|
|
Anterior pituitary releases:
|
ACTH FSH GH LH TSH |
|
|
Thyroid releases:
|
T3 T4 calcitonin |
|
|
The ____________ controls the release of hormones from the pituitary gland.
|
hypothalamus
|
|
|
Adrenal medulla secretes:
|
catecholamines (norepinephrine and epinephrine)
|
|
|
Adrenal cortex secretes:
|
cortisol aldosterone |
|
|
Cortisol is released in response to stress, injury or infection. Increased cortisol leads to increased __________.
|
glucose
|
|
|
Increased cortisol leads to a(n) __________ in BP.
|
increase
|
|
|
Catecholamines cause a(n) ___________ in HR as well as an increase in contractile force.
|
increase
|
|
|
ADH is known as ____________ _______ hormone.
|
anti-diuretic
|
|
|
Aldosterone is key in maintaining ______________ balance. If aldosterone is elevated, BP will ________.
|
fluid/electrolyte increase |
|
|
Increased T3 and T4 from the thyroid gland will __________ cellular metabolism.
|
increase
|
|
|
Increased calcitonin will ___________ the level of Ca++ in the blood.
|
decrease
|
|
|
As part of the HPA axis, elevated cortisol inhibits the __________ and ___________. It also decreases the activity of most WBCs.
|
pituitary and hypothalamus
|
|
|
In the RAAS system, if your blood pressure is low...will the release of renin increase or decrease?
|
increase
|
|
|
The parathyroids release PTH, this hormone increases blood levels of ___________.
|
Ca++
|
|
|
Name the three types of cells in the pancreas involved in glucose regulation.
|
alpha, beta, delta
|
|
|
If your blood glucose is too high, will insulin release increase or decrease?
|
increase
|
|
|
Glucagon is needed to convert glycogen to _________ in the liver.
|
glucose
|
|
|
The most common form of hyperthyroidism is called ___________ disease.
|
Graves |
|
|
Hyperthyroidism is similar to which animal (in Katy's world)?
|
rabbit
|
|
|
Hypothyroidism is similar to which animal (in Katy's world)?
|
turtle |
|
|
The most common medication to give to a person with low thyroid function is _________.
|
levothyroxine or Synthroid |
|
|
Normal TSH levels (updated levels) are between ____ and _____.
|
.5 to 3 |
|
|
What is the difference between Cushing's syndrome and Cushing's disease?
|
Cushing's disease: due to decreased ACTH from the pituitary gland |
|
|
Conn's syndrome is due to an excess release of ______________ from the adrenal glands.
|
aldosterone |
|
|
Addison's disease is an insufficient amount of hormones released from the ____________.
|
adrenal glands |
|
|
An individual with untreated Addison's disease would likely have a _______ blood pressure.
|
low |
|
|
Which type of diabetes can lead to ketoacidosis?
|
|
|
|
Which type of diabetes is most common?
|
type 2 |
|
|
Which type of diabetes causes islet cell antibodies?
|
type 1 |
|
|
Which type of diabetes usually needs insulin as a treatment?
|
type 1 |
|
|
Why are individuals with diabetes prone to slow healing (infected) wounds?
|
-impaired immune system -poor vision (can't see wound until advanced) -poor sensation (don't notice wound until advanced) -changes in foot mechanics increases pressures on the foot in areas that are not designed for pressure. |
|
|
What is HHNC?
|
hyperglycemic, hyperosmolar nonketotic coma (common in type 2 diabetics) |
|
|
Which life-threatening condition is best described as extremely low glucose levels and can affect both type 1 and type 2 diabetics.
|
insulin shock |
|
|
Individuals with diabetes should be advised to exercise in the _______ (time of day).
|
AM |
|
|
Individuals with type 1 diabetes should avoid exercise during peak ______ times.
|
insulin
|
|
|
PKU is a disorder that occurs when a person can't process ____________________.
|
phenylalanine |
|
|
Wilson's disease occurs when a person can't metabolize ___________________.
|
copper |
|
|
Osteoporosis is diagnosed when a person's bone mineral density is greater than _____ standard deviations lower than normal.
|
2.5 |
|
|
Osteomalacia is a _______________ of the bones without a change in bone matrix.
|
softening |
|
|
Most exercise research suggests that the best intervention for someone with osteoporosis is to focus on _______________________.
|
strengthening, resistance training (without impact) |
|
|
This disorder is characterized by cyclical bone resorption and bone formation that leads to skeletal fragility.
|
Paget's disease
|
|
|
What are the hallmark findings in someone with metabolic syndrome?
|
abdominal obesity dyslipidemia HTN insulin resistance prothrombotic state proinflammatory state |
|
|
A high level of TSH is often a sign of a hypo-functioning ______________.
|
thyroid
|
|
|
Hypoglycemic agents work by either increasing insulin secretion or inhibiting ________ production.
|
glucose |
|
|
The outermost layer of the epidermis is the ________ _________. |
Stratum corneum |
|
|
True or false. The epidermis has its own (contained) blood supply. |
False |
|
|
The dermis has ______ layers. |
2 |
|
|
Name the two layers of the dermis? |
Reticular Papillary |
|
|
Name the specialized WBC in the skin which is key to immune functioning. |
Langerhans cell |
|
|
What is the common way to estimate the total surface area that is involved after a burn injury? |
Rule of Nines |
|
|
Eczema is often known by another term. What is that term?
|
|
|
|
Impetigo and cellulitis are caused by this type of pathogen.
|
bacteria |
|
|
Name the condition that is characterized by inflammation of the dermis and subcutaneous tissues...and the infection spreads through tissue spaces.
|
cellulitis |
|
|
Name the disease that is a chronic, auto-immune disorder that leads to itchy, white plaques on the skin.
|
psoriasis |
|
|
Acanthosis nigricans can be sign that a person is _______________.
|
diabetic |
|
|
Who is most at risk for a pressure injury?
|
those who are bedridden, W/C bound, or unable to change position. Also, those with impaired sensation. |
|
|
Describe a stage 1 pressure injury.
|
intact skin with non-blanchable erythema. |
|
|
Describe a stage 2 pressure injury.
|
partial-thickness skin loss involving the epidermis down to the superficial dermis
|
|
|
Describe a stage 3 pressure injury.
|
full-thickness skin loss involving damage or necrosis of the subcutaneous tissue. undermining is present, but not tunneling.
|
|
|
Describe a stage 4 pressure injury.
|
full-thickness skin loss which penetrates the fascia. damage to muscle, tendon, ligament, bone. often see undermining and tunneling. |
|
|
If you can't visualize the full extent of a pressure injury, you should document the stage as ________________.
|
unstageable |
|
|
Describe a typical venous insufficiency ulcer.
|
lower leg or ankle irregular in shape and shallow lots of exudate good granulation |
|
|
Describe a typical arterial insufficiency ulcer.
|
on the feet (metatarsal heads, tips of toes, malleoli, areas of trauma or rubbing of footwear look punched out necrotic base minimal granulation gangrene |
|
|
Describe a typical neuropathic ulcer.
|
painless located on the bottom of the foot well defined margins with a callus surrounding the wound. |
|
|
There are four degrees of burn depth injury, name them.
|
superficial partial thickness (2nd degree) deep partial thickness (2nd degree) full thickness (3rd degree) subdermal (4th degree) |
|
|
Which type of burn injury is shiny and red with blisters?
|
superficial partial thickness |
|
|
Which type of burn injury is mottled red/white?
|
deep partial thickness |
|
|
Which type of burn injury is grey?
|
full-thickness |
|
|
Which type of burn injury is black and charred?
|
subdermal |
|
|
Autografts are divided into sheet grafts and ____ grafts.
|
mesh |
|
|
Why would you select a mesh graft? |
The donor site is smaller. |
|
|
Autografts can be divided into full-thickness grafts and ______________ grafts.
|
split-thickness
|
|
|
Why would you use a full-thickness graft?
|
excellent cosmetic result and often used on areas that are weight-bearing or prone to friction.
|
|
|
Allografts are made using __________ skin.
|
cadaver |
|
|
Following a burn injury, if arterial occlusion is suspected, what procedure will be done?
|
escharotomy |
|
|
Using the rule of nines, how much TBSA is both arms in an adult?
|
18% |
|
|
sing the rule of nines, how much TBSA is one leg in an adult?
|
18%
|
|
|
Using the rule of nines, how much TBSA is both legs in a child?
|
26% |
|
|
Using the rule of nines, how much TBSA is one arm in a child?
|
9% |
|
|
When is the emergent/resuscitation phase of burn care done?
|
About 48-72 hours after injury...when the client is hemodynamically stable. |
|
|
How long does the acute phase of burn care last?
|
Until all of the wounds are closed. |
|
|
The most common type of scarring are _______________ scars.
|
hypertrophic |
|
|
The shoulder should be positioned in which position to avoid a contracture following a burn injury?
|
arm abduction to 90-110 decrees and externally rotated |
|
|
The MCP joints should be positioned in ____ degrees of flexion following a burn injury.
|
90 |
|
|
What is the general term for several diseases in which the wall of an artery becomes thicker and less elastic?
|
arteriosclerosis
|
|
|
The most common type of arteriosclerosis is ____________________. |
atherosclerosis |
|
|
The formation of intraarterial plaques are partially due to the conversion of macrophages/monocytes into ________________ cells. |
foam |
|
|
The normal level of C-reactive protein is greater than or equal to ______________. |
3.0 mg/dL (elevated levels are associated with CV disease) |
|
|
What is the term for when a localized area of an artery becomes dilated...and all three arterial wall layers are weakened? |
aneurysm |
|
|
Hypertension is diagnosed when the systolic blood pressure is above ______ and the diastolic blood pressure is above _______. |
90 140 |
|
|
Hypertension is a two-fold problem...it could be due to increased peripheral resistance or increased ____________ or both. |
blood volume |
|
|
If a person has intermittent episodes of small artery constriction causing temporary pallor and cyanosis of the digits they may be diagnosed with _____________ disease. |
Raynaud's |
|
|
The quick clinical test that can suggest a DVT is the _______________ sign. |
Homan's |
|
|
Patients with a DVT and on heparin can resume PT in 12-24 hours. True/False |
False. It is up to the PT, PTT and INR blood results and perhaps a follow-up Doppler. Always check with the team before initiating mobilization. |
|
|
Gangrene is most associated with __________ ______________ ulcers. |
arterial insufficiency |
|
|
An accumulation of lymph fluid in the plural cavity following thoracic surgery or in an individual with lymphoma is called a ______________________. |
chylothorax |
|
|
For single lead ECG interpretation in this course, we will look at Lead ____. |
II |
|
|
The leads in the positive direction (for P wave) are the _______________________ leads. |
I, II, aVF, V4, V5, V6 |
|
|
ST depression is indicative of a ______MI or ____________. |
Non-ST elevation MI (NSTEMI) - permanent damage ischemia (reversible) |
|
|
What does PTCA stand for? |
percutaneous transluminal coronary angioplasty |
|
|
What does a CABG stand for? |
coronary artery bypass graft |
|
|
Name the sternal precautions. |
no pulling/pushing with arms no lifting greater than 10 lbs avoid shoulder horizontal abduction and ER no shoulder flexion past 90 degrees no assistive devices no driving or sitting int he front seat with airbags All for 4-6 weeks. |
|
|
Immediately following an open heart procedure, avoid increasing the HR more than ____ bpm over the resting heart rate. |
20 |
|
|
The most common type of angina is called ____________ angina. |
stable |
|
|
Myocardial infarctions are typically described as either transmural or _____________. |
subendocardial |
|
|
Most MI occurs in the AM, because _____ tends to be higher. |
blood pressure |
|
|
Name some of the common signs/symptoms of a MI. |
sudden, prolonged pressure or pain in the center of the chest pain that spreads from chest to neck/jaw/shoulders or arms pallor perspiration shortness of breath |
|
|
ST segment elevation is a sign of a __________. |
transmural MI (STEMI)....along with T-wave inversion and signficiant (large) Q waves |
|
|
STEMIs are caused by a _______________. |
complete block of a coronary artery |
|
|
When differentiated ST depression....and deciding between unstable angina and a NSTEMI, the key is to look for elevated levels of ______________. |
troponin (indicitive of a NSTEMI) |
|
|
A great early marker to show cardiac muscle damage is to follow ________ levels. |
GPBB |
|
|
If a patient has a MI and is now discharged to home, what level of cardiac rehabilitation is ongoing. |
Level 1.5 |
|
|
Which type of congestive heart failure leads to pulmonary edema and coughing? |
LV failure |
|
|
Which type of congestive heart failure leads to peripheral edema? |
RV failure |
|
|
Only the ______ value can be diagnosed with prolapse. |
mitral |
|
|
Inotropes are used to increase a patient's ___________ and __________. |
HR and BP |
|
|
Drugs ending with -thiazide and -semide are in which drug class? |
antihypertensives |
|
|
Adrenergic agnonists and adrenergic antagonists are both used to __________ peripheral resistance. |
decrease |
|
|
The mechanisms of action for both ACE inhibitors and ARBs are to inhibit the normal pathways of the _________ system. |
RAAS |
|
|
ACE inhibitors usually have the suffix -________. |
pril |
|
|
Beta-blockers usually have the suffix -_________. |
olol |
|
|
Antihypertensives that end in -ipine block the _______ ions influx in arterial wall muscle cells which leads to vasodilation. |
Ca++ |
|
|
Diuretics inhibit the Na/Cl tranporters in the _____________ to increase the elimination of sodium (and water). |
kidney |
|
|
NTG is thought to raise levels of intracellular _________ which inhibits the contractile properties in vascular smooth muscle. |
cGMP |
|
|
Streptokinase, urokinase, and tPA are all in the drug class known as _________________. |
thrombolytics |
|
|
The congenital heart defect that causes a VSD, narrowed pulmonary valve, displaced aorta and a thickened right ventricle is called ___________________. |
Tetrology of Fallot |
|
|
The congenital heart defect that causes a switch in the placement of the aorta and the pulmonary trunk is called a _______________________. |
transposition of great vessels |
|
|
On an EKG, the p wave represents ___________ depolarization. |
atrial |
|
|
On an EKG, the QRS represents _________________ depolarization |
ventricular |
|
|
The primary pacemaker in the heart is the ____ node. |
SA |
|
|
On an EKG, one small horizontal box represents ____ seconds. |
.04 |
|
|
On an EKG, one small vertical box represents ____ mV. |
.1 |
|
|
On an EKG, the T wave represents ____________ repolarization. |
ventricular |
|
|
How many leads are traced in a typical EKG? |
12 |
|
|
How many leads are bipolar? |
3: AVR, AVL and AVF |
|
|
Which leads would give you the best view from the top of the heart looking downward? |
AVR, AVL and I |
|
|
Which leads would give you the best view of the bottom of the heart looking upward? |
II, III and AVF |
|
|
Which section of the EKG tracing represents the right coronary artery? |
bottom left (II, III and AVF) |
|
|
If you see a QRS complex once every one large box on an EKG, the heart rate is ______bpm. |
300 |
|
|
The two leads to see an axis shift is lead I and _____. |
AVF |
|
|
Typically the QRS complex is in the ____ direction in lead I and AVF. |
positive |
|
|
If a person has a normal rhythm but it is slow...about 45 bpm, he/she may be diagnosed with ____________. |
sinus bradycardia |
|
|
The most severe type of heart block is _____. |
complete heart block or 3rd degree |
|
|
The _____ interval can vary is a person has a wandering ____ pacemaker. |
atrial |
|
|
When a person has an "extra" beat...or...there is an occasional extra atrial following by ventricular contraction, he/she can be diagnosed with __________________. |
premature atrial contraction |
|
|
Which is worse....atrial fibrillation or atrial flutter? |
atrial fibrillation |
|
|
First degree AV heart block usually leads to an increased ____________ interval. |
PR |
|
|
What is the dysrhythmic condition that can be caused by a number of drugs? |
Torsades de Pointes |
|
|
This value represents the pressure of oxygen dissolved in the blood.
|
PaO2 |
|
|
For the purposes of this class, we consider HCO3 to be a weak ________.
|
base |
|
|
Normal oxygen content is between _____ and ____%.
|
15-22 |
|
|
Normal oxygen saturation is between ____ and ____%.
|
96-100 |
|
|
What is the general term that means there is a general lack of oxygen in the whole body
|
hypoxia |
|
|
Walking pneumonia is typically caused by a _____.
|
bacterium called mycoplasma pneumonia |
|
|
In a hospitalized patient, aspiration pneumonia often affects the _________ _________ lobe of the lung.
|
right upper |
|
|
Bacterial pneumonia typically affects the _________ lobes of the lung.
|
lower |
|
|
What is the term for an accumulation of liquid or solids in the lung tissue?
|
consolidation |
|
|
What is the term for an escape of fluid into a neighboring body cavity?
|
effusion |
|
|
One of the contraindications for chest PT is an intracranial pressure of greater than ____.
|
20 |
|
|
A patient with a long history of TB would likely have ______________ in their lungs. These are an accumulation of old/inactive WBCs.
|
granulomas |
|
|
For all obstructive airway diseases, the patient has difficulty getting the air __________ the lungs.
|
out |
|
|
For all restrictive airway diseases, the patient has difficulty getting the air ________ the lungs.
|
in |
|
|
TLC is increased in a patient with a ____________ lung disease.
|
obstructive
|
|
|
COPD represents which two diseases?
|
chronic bronchitis and emphysema |
|
|
Which disorder is characterized as a reversible obstructive lung disease caused by a reaction to a stimuli?
|
asthma |
|
|
Which disease is described as an inherited disease of the exocrine glands that affects the liver, GI and respiratory systems?
|
cystic fibrosis |
|
|
Which restrictive lung disease is described as an accumulation of fibrous or connective tissue in the lungs due to chronic inflammation?
|
pulmonary fibrosis |
|
|
Typically you would expect the V/Q ratio to be ___.
|
1 |
|
|
In areas with restricted blood flow in the lungs but normal ventilation, the V/Q ratio is _____.
|
high |
|
|
Throughout most of the lung during a pulmonary embolism event, the body has low O2 due to the overall _______ V/Q ratio in the lungs.
|
low |
|
|
A common suffix for glucocorticoids is _________.
|
-sone |
|
|
Anti-histamines block the ____ receptors and thereby block the release of histamine.
|
H |
|
|
Rescue inhalers, such as albuterol, work as bet-2 agonists which lead to an increase of __________ which relaxes bronchial smooth muscle.
|
cAMP |
|
|
Which ventilator setting does ALL of the work for the patient?
|
control ventilation |
|
|
Which ventilator modes can lead to hyperventilation in patients?
|
ACV and AV |
|
|
Which vent setting allows for unsupported breaths, but when the patient does receive a supported breath it matches with the patient's effort?
|
SIMV |
|
|
If you needed to adjust the amount of pressure in the alveoli at maximum exhalation, you would adjust the ___________.
|
PEEP |
|
|
If you needed to adjust the amount of pressure in the alveoli at maximum inhalation, you would adjust the ________.
|
PIP |
|
|
Name the breathing pattern that is characterized by repeated cycles of deep breathing followed by shallow breaths or cessation of breathing.
|
Cheyne-Stokes respiration |
|
|
Name the volume of air from normal inspiration to maximal inspiration.
|
inspiratory reserve volume |
|
|
Name the volume of air from normal expiration to maximal expiration. |
expiratory reserve volume |
|
|
Name the term to describe all of the air that can fill the lungs from maximal inspiration to a state where all air is removed from the lungs....even more than can be removed through maximal expiration.
|
total lung capacity |
|
|
What is the volume of air that can be forcefully exhaled in one second called?
|
forced expiratory volume 1 |
|
|
What is the volume of air that can be maximally forcefully exhaled?
|
forced vital capacity |
|
|
The coordinated contraction of smooth muscles that propels contents through the digestive tract is known as: |
peristalsis |
|
|
The musculo-membranous tube that extends from the base of the skull to C6 is known as the ___________. |
pharynx |
|
|
Name the two structures that border the stomach. |
Lower esophageal sphincter and the pyloric value |
|
|
What is the major hormone that regulates acid secretion in the stomach? |
gastrin |
|
|
Gastrin stimulates parietal and chief cells to release: |
Parietal: HCL Chief: Pepsinogen |
|
|
What is the function of the gall bladder? |
store and concentrate bile |
|
|
Name some of the functions of the liver. |
make blood-clotting factors fat metabolism bile production bilirubin metabolism carbohydrate metabolism vitamin and mineral storage protein metabolism filter the blood immunological functions production of albumin synthesis of angiotensinogen |
|
|
What is GERD? |
gastrointestinal esophageal reflux disease |
|
|
The most effective pharmacological drug class for treating GERD is: |
proton pump inhibitors |
|
|
Peptic ulcer disease is usually caused by: |
bacterial infection (H. pylori) |
|
|
Idiopathic inflammatory bowel disease incorporates two conditions, name them: |
Crohn's disease and ulcerative colitis |
|
|
True of False. It is possible for individuals with Crohn's disease to have integumentary symptoms. |
true |
|
|
Diverticulosis can lead to _______________ when there is inflammation. |
diverticulitis |
|
|
Celiac Sprue is a disorder that is caused by an intolerance to _________________ and leads to mucosal injury in the small intestine. |
gluten |
|
|
The two key lab tests for liver function are: |
ALT and AST |
|
|
Normal AST is between ____ and ____. |
8 to 48 |
|
|
Normal ALT is between _____ and ____. |
7 and 55 |
|
|
If a person has an liver disorder which is causing excessive amounts of bile to spill into the blood they will likely be diagnosed with: |
jaundice |
|
|
Why does phototherapy work to address neonatal jaundice in infants? |
The light is absorbed and convert the bilirubin into an easier to eliminate product. |
|
|
A generalized or localized inflammatory process of the peritoneum. |
peritonitis |
|
|
Appendicitis pain typically starts in the ______ region. |
periumbilical |
|
|
The suffix -ectomy means |
surgical removal |
|
|
The suffix -desis means: |
fusion |
|
|
The suffix -plasty means: |
to modify or reshape |
|
|
Most cancer deaths are due to __________ cancer. |
lung |
|
|
True or false. The more primitive the malignant cell, the better the prognosis. |
false |
|
|
Single biggest risk factor for developing cancer is _____________________ |
older age |
|
|
The TNM classification for cancer stands for: |
tumor lymph nodes metastases |
|
|
If a person has T2N0M0, he/she is at a stage ___. |
2 |
|
|
If a person has T1N2M1, he/she is at a stage ___. |
4 |
|
|
If a person's tumor is completely gone, he/she will be in ___________ remission. |
complete |
|
|
If a person's tumor is neither growing or shrinking, he/she will be a ______________ phase. |
stabilization |
|
|
True or false. A person after radiation and surgery due to cancer can develop lymphedema at any time, even years later. |
True |
|
|
Put in order from most likely to metastasize to least likely. basal cell squamous cell melanoma |
melanoma squamous cell basal cell |
|
|
Explain the process of urine formation starting at the glomerulus. |
glomerulus, bowman's capsule, PCT, descending loop of henle, ascending loop of henle, DCT, collecting duct, papillary ducts, minor calyx, major calyx, renal pelvis, ureter, bladder, urethra |
|
|
The key test of renal function is: |
Glomerular Filtration Rate (GFR) |
|
|
Normal GFR is approximately greater than: |
70-90 (just an approximation) |
|
|
Most of the volume of filtrate is reabsorbed in the ___________. (part of the kidney) |
PCT |
|
|
Urine is mostly comprised of _________. |
water |
|
|
Tubular secretion mostly occurs in the __________ and _________ in the kidney. |
renal tubules and collecting ducts |
|
|
Which urethral sphincter is under voluntary control? |
external |
|
|
Leukocytes in the urine could be a sign of a _______________. |
UTI |
|
|
Most UTIs are caused by this type of bacteria. |
E. Coli |
|
|
Urine typically has a _________ pH. |
low (acidic) |
|
|
Most kidney stones are comprised of _______ __________. |
calcium oxylate |
|
|
True or false. Most kidney stones are diagnosed in the winter months. |
false |
|
|
Chronic kidney disease can lead to ___________, which can in turn negatively impact the kidneys. |
hypertension |
|
|
The two types of dialysis discussed in this course is: |
hemodialysis peritoneal dialysis |
|
|
A common condition affecting older men that can lead to prostate cancer is: |
BPH |
|
|
True or False. All HLA markers should be matched exactly for a successful transplant. |
false. |
|
|
The main problem affecting individuals following a transplant is _____________.
|
hypertension |
|
|
Activation of the RAAS system leads to vaso____________.
|
constriction |
|
|
Assuming there are sufficient enzymes available to degrade a medication. The concentration of a drug should decrease using a _______ order process.
|
first
|
|
|
What is the formula to calculate clearance of a drug?
|
(conc. of drug in urine x urine rate)/ conc. of drug in plasma
|
|
|
The suffix -ase is used for which drug class?
|
thrombolytics (clot-busters) such as strektokinase
|
|
|
The suffix -azole is used for which drug class?
|
antifungals |
|
|
The suffix -caine is used for which drug class?
|
local anesthetic such as lidocaine
|
|
|
The suffix -cillin is used for which drug class?
|
penicillin-based antibiotic
|
|
|
The root "cort" is used for which drug class?
|
corticosteroid such as hydrocortisone
|
|
|
The suffix -floxacin is for which drug class?
|
quinolone-based antibiotic such as ciprofloxacin
|
|
|
The suffix -mycin or -micin is used for which drug class?
|
antibiotic
|
|
|
The suffix -olol is used for which drug class? |
beta blocker
|
|
|
The suffix -pam is used for which drug class? |
antianxiety such as diazepam
|
|
|
The suffix -parin is used for which drug class?
|
antithrombotic / anticoagulant such as heparin
|
|
|
The prefix pred- is used for which drug class?
|
corticosteroid such as prednisone
|
|
|
The suffix -pril is used for which drug class?
|
ACE inhibitor such as captopril or lisinopril
|
|
|
The suffix -profen is used for which drug class?
|
NSAID such as ibuprofen
|
|
|
The suffix -sartan is used for which drug class?
|
Angiotensin II receptor antagonist or ARB
|
|
|
The suffix -semide is used for which drug class?
|
diuretic such as furosemide
|
|
|
The suffix -sone is used for which drug class?
|
corticosteriod
|
|
|
The suffix -statin is used for which drug class?
|
cholesterol-lowering
|
|
|
The prefix sulfa- is used for which drug class?
|
antibiotic; anti-inflammatory
|
|
|
The suffix -terol is used for which drug class?
|
beta agonist / bronchodilator such as albuterol
|
|
|
The suffix -vir is used for which drug class?
|
antiviral
|
|
|
The suffix -zolam and -zepam is used for which drug class?
|
benzodiazepine
|
|
|
Drugs such as Wllbutrin, Celexa, Lexapro, Prozac, Paxil, Xoloft, Cymbalta, and Effexor are all antidepressants and are known as _______ or ________ for their mode of action.
|
SSRI SNRI |
|
|
Antipsychotics are typically ______________ antagonists.
|
dopamine
|
|
|
Anti-Parkinsonian medications are often __________________ agonists.
|
dopamine
|
|
|
Warfarin and Coumadin work by limiting the effectiveness of the ____________ cascade.
|
clotting
|
|
|
Normal WBC count?
|
4,500 to 11,000 cells/microliter
|
|
|
Normal neutrophils as percentage and count?
|
56% 1800-7800 cells/microliter |
|
|
Normal lymphocytes as percentage and count?
|
34% 1000-4800 cells/microliter |
|
|
Normal monocytes as percentage and count?
|
4% 0-800 cells/microliter |
|
|
Normal eosinophils as percentage and count?
|
2.7% 0-450 cells/microliter |
|
|
Normal basophils as percentage and count?
|
.3% 0-200 cells/microliter |
|
|
Normal RBC count? |
4.2 - 5.4 x 106 cells/microliter
|
|
|
Normal Hgb level?
|
12-18 g/dL
|
|
|
Normal Hct percentage?
|
37-52% of RBCs in whole blood
|
|
|
Normal MCV in size?
|
80-100 micrometer3
|
|
|
Normal MCH?
|
28-33pgs
|
|
|
Normal MCHC?
|
33-36g/dL
|
|
|
Normal reticulocyte percentage (out of total RBCs) and count?
|
.5-1.5% 25-75 x 103 cells/microliter |
|
|
Normal platelet count?
|
150,000-450,000 cells/microliter
|
|
|
Normal MPV?
|
7.5-11.5 femtoliters
|
|
|
Erythropoietin is primarily produced in the ____________ of adults.
|
kidneys
|
|
|
The four values that are shown in the medical shorthand for a CBC are:
|
WBC, Hgb, HCT, Platelets
|
|
|
The clotting cascade starts with the __________________ pathway and is tested with which lab test?
|
extrinsic PT |
|
|
Normal INR?
|
.8-1.0
|
|
|
If a patient's INR is greater than ______, you should treat them with caution.
|
4.0
|
|
|
Normal sodium?
|
135-145 mEq/L
|
|
|
Normal potassium?
|
3.5-5.0 mEq/L
|
|
|
Normal chloride?
|
95-105 mEq/L
|
|
|
Normal calcium?
|
9-11 mg/dL
|
|
|
Normal magnesium?
|
1.5-2.5 mEq/L
|
|
|
Normal bicarbonate?
|
22-28 mEq/L
|
|
|
Normal PaCO2?
|
35-45 mmHg
|
|
|
Normal creatinine?
|
.5-1.5 mg/dL
|
|
|
Normal BUN?
|
5-30 mg/dL
|
|
|
The seven values that are included in the medical shorthand for metabolic lab values are:
|
sodium, potassium, chloride, bicarb, BUN, creatinine, and glucose
|
|

What is the etiology of this wound?
|
chronic venous insufficiency |
|

What is the etiology of this wound? |
Pressure injury |
|

What is the etiology of this wound? |
arterial insufficiency |
|

What is the etiology of this wound? |
chronic venous insufficiency |
|

What is the etiology of this wound? |
neuropathic or diabetic wound |
|

What is the depth of involvement? superficial partial thickness full thickness |
full-thickness (there is no dermis or epidermis in this wound) |
|

What is the etiology of this wound? |
Pressure injury |
|

If there was bone visible in this wound, what would be the correct stage? |
Stage IV |
|

What is the etiology of this wound? |
arterial insufficiency |
|

What is the etiology of this wound? |
pressure injury |
|

What is the stage (this wound is not open) |
stage I
|
|

What is the etiology of this wound? |
Neuropathic or diabetic |
|

What is the etiology of this wound? |
Pressure injury |
|

How would you stage this wound? |
Unstageable |
|

What is the most likely etiology for this edema? |
lymphedema |
|

|
PAC (premature atrial contraction) |
|
|
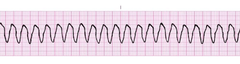
V-tach |
|
|
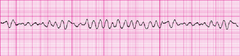
V-fibrillation |
|
|
atrial flutter |
|

|
atrial fibrillation |
|
|
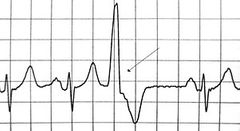
premature ventricular contraction (PVC) |
|

|
Complete heart block (3rd degree) |
|

|
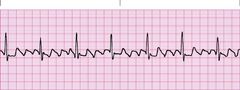
first degree heart block |
|

|
sinus bradycardia |
|
|
sinus tachycardia |
|
|
|
|