Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
47 Cards in this Set
- Front
- Back
|
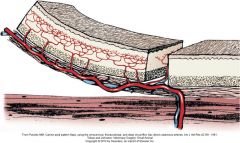
what is an axial pattern flap and how does it differ from other flaps?
|
contain direct cutaneous artery and vein. allow for larger flap with better survival
|
|
|
how far can an axial pattern flap be rotated? why?
|
up to 180 degrees at its base
greater rotation can cause venous congestion |
|
|
what are the 2 differrent ways you can create an axial pattern flap?, and how are they different?
|
peninsular or island
peninsular has intact skin at its base, protects vascular pedicle. the drawback is the dog ear at point of rotation with island flap the skin is incised along all edges and flap is rotated on the vascular pedicle. island are more cosmetic, but more susceptible to vascular damage. |
|
|
name several specialized forms of axial pattern flaps
|
composite or compound flaps
myocutaneous flaps |
|
|
overall success rate of apfs?
some advantages of them? |
overall success: 87-100%
although tips are prone to necrose, overall survival is at least 50% better than subdermal pkexus flaps can be placed directly over bone/tendon/ligament dont need staged procedures early closure |
|
|
why might obese patients have higher failure rates?
|
harder to find blood supply
doppler can help |
|
|
which vessels are easies/hardest to find
|
easiest: caudal superficial epigastric
hardest: superficial cervical artery |
|
|
major diff between cats and dogs in terms of cutaneous vasculature?
|
dogs have higher density of tertiary vessels than cats, especially on trunk--less cutaneous circulation for cats
|
|
|
major diff in healing wounds between dogs and cats
|
cats have slower epitheliazation, contraction, GT formation
50% less wound strength at 7 days GT forms around edges in cats rather than across entire bed cats more affected by loss of SQ (its recommended to retain SQ in cats with flaps) |
|
|
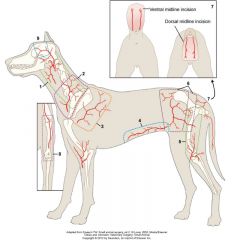
1.caudal auricular
2.omocervical 3.thoracodorsal 4.caudal superficial epigastric 5.lateral genicular 6. deep circumflex iliac 7/lateral caudal 8.superficial brachial superficial temporal |
|
|
name a few other axial pattern flaps not shown in diagram
|
angularis orbis: (labial commisure), usues for palatal, facial, nasal defects
superficial brachial:centered over dorsal third of elbows flexor surface, good for antebrachial and elbow defects lateral caudal: base of tail |
|
|
should drains be placed with axial pattern flaps?
|
almost always indicated, except for very small area, or areas not amenable. should not course directly under the flap?
|
|
|
which are the most robust flaps
|
thoracodorsal and caudal superficial epigastric
|
|
|
what vessel is the omocervical flap based on?
some uses? where does vessel originate |
superficial cervical artery (cervical cutaneous)
uses: head, neck, facial, ear, cervical , shoulder, axillary, palate (experimental) superficial cervical branch of omocervical artery originate at the level of the prescap LN and course cranial to scapula in dorsal direction |
|
|
landmarks of omocervical flap:
|

caudal icision along border of scap spine. cranial incision cranial to scapula width equidistant to width between incision and cranial border of scapula. peninsular can go also to level of contralateral scapulohumeral joint. L-shaped should be shorter.
|
|
|
what vessel is thoracodorsal flap based on? uses?
|
thoradorsal artery
uses for thoracic, shoulder, forelimb, axillary defects |
|
|
landmarks for thoracodorsal flap
|

vessel originates caudal to the shoulder at level of acromion and continues dorsally along scapular spine
very similar to omocervical except cranial incision is along caudal scapular spine. |
|
|
complications of thoracodorsal flap
|
partial tip necrosis in 70% when flaps used to repair distal limb defects.
one study percent necrosis ranged from 2-53%, mean 21% |
|
|
thoracodorsal flaps and cats?
|
paricularly useful because of small leg-trunk ratio. 98% survival experimentally. can even cover carpus.
|
|
|
where does the deep circumflex iliac artery exit the abdomen?
uses? |
cranioventral to ilial wing, and then divides in dorsal and ventral branches (both can be used for flaps)
dorsal flap: ipsilateral flank, lateral lumbar, pelvic, lateromedial thigh, over greater trochanter. ventral: lat abd wall, pelvic, sacral success rates not reported for either technique. |
|
|
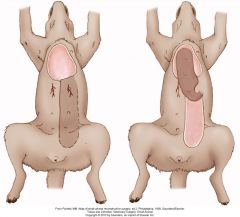
vessel for caudal superficial epigastric flap?
uses? |
caudal superficial epigastric artery: exits at the inguinal canal
uses: caudal abdominal, flank, inguinal, preputial, perineal, thigh, stifle defects. dorsal body reconsrtucts, full thickness body wall defects in cats. can even reach distal libs in some animals |
|
|
caudal superficial epigastric technique
|

skin incised on midline beginning just behind caudal teat (base of prepuce included in male dogs). maximum flap length is to second teat
ditance between teat and midline is measured and equidsitant incision is made lateral to teat flap undermined deep to supermammarius mm and superfical to rectus sheath |
|
|
outcome specifics with caudal superficial epigastric
|
in intact females the mammary glands remain functional.
(can do OVH) 30% complication Experimentally 95% success Clinically 90% success |
|
|
where is the cranial superficial epigastric vessel? uses?
|
based on short cutaneous branches of cranial superficial epigastric artery, located in the hypogastric area caudoventral to thoracic cage
uses: sternal wounds |
|
|
technique cranial superficial epigastric
|
base of flap is just caudal to ribcage
width determined by 3rd teat flap length includes teat 3,4, and sometimes 5. in male dogs just cranial to tip of prepuce include panniculus |
|
|
outcome cranial superficial epigastric
|
ecperimentally without rotation: 87%
vessel much shorter than caudal superficial epigastric, mor susceptible to vasc injury, anatomy less reliable. no diff in survival between peninsular an island clinical results in 1 dog only:93% flap survival |
|
|
what vessel is angularis oris flap based on?
|
sngularis oris artery, includes tributaries of facial artery and vein, and inferior and superior labial arteries
|
|
|
angularis oris flap technique
see pg. 1265 deep structures include branches of facial nerve, auriculotemporal nerve, parotid duct, facial vein. |

|
|
|
complications of angularis oris flap
|
movement of flap with respiration
nasal discharge flap necrosis when accompanied by maxillectomy, can see billowing of myocutaneous flap b/c communication with nasal cavity usually resolves with 10 days |
|
|
technique and uses of superficial temporal artery
|

uses: maxilofacial, medial eyelif, palate
base defined by caudal aspect of zygomaic arch caudally and lateral orbit and rim rostrally width limited by eye and ear and equal to zygomatic arch length no more than to dorsal rim of contralateral orbit |
|
|
outcome superficial temporal
|
experimentally flaps extending to dorsal orbital rim of contralateral eye: 93% dog, 99% cat
69% for flaps extending to contralateral zygomatic arch, so not recommended |
|
|
caudal auricular flap--what vessel based on?
uses? |
based on: caudal auricular axial pattern flap based on sternocleidomastoideus branches of caudal auricular artery
uses: neck, facial area, dorsal head, ear |
|
|
caudal auricular technique
|

base of flap at the depression between wing of atlas and vertical ear canal. dorsal and ventral inciions parallel and centered over lateral cervical area.
length can extend to spine of scapula |
|
|
outcome caudal auricular flap?
|
survival reported 85% in dogs
may be better for cats keeping the flap short may help |
|
|
superficial brachial flap: vessel? uses? outcome?
|
based on superficial brachial artery, branch of brachial artery
uses: reconstruction of antebrachial and elbow defects (does not extend to carpus) experimentally:98% survival less tobust in reality--not recommended |
|
|
technique superficial brachial
|
parallel incisions along shaft of humerus (slowly taper together dorsally)
should end before reaching greater tubercle |
|
|
genicular flap vessel? uses? outcome?
|
vessel: genicular branch of medial saphenous vein
artery extends cranially over medial aspect of stifle and terminates over craniolateral surface uses: defects from stifle to tarsus medial or lateral outcome: no clinical reports. experimental: 89% flap necrosis ranged from 11-33% |
|
|
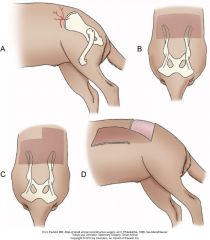
genicular flap technique
|
base of flap 1cm proximal to patella
and 1.5 cm distal to tib tub on lateral aspect dorsal and ventral incisions parallel to femoral shaft keep flap short |
|
|
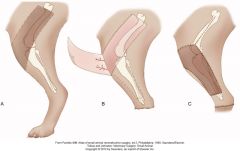
reverse saphenous conduit flap
uses? how does it work? |
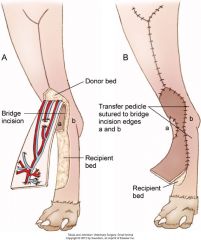
uses: distal aspect hindlimb
dependent on reverse flow through anastomoses between branches of cranial tibial and saphenous arteries and between medial and lateral saphenous veins at level of tarsus, cranial branch of saphenous artery anastomoses with superficial branch of cranial tibial artery to form common digital artery. could be a composite flap including proximal tibia (bone)!, in theory |
|
|
outcome reverse saphenous?
|
venous congestion b/c reverse flow through vens. usually subsides within a few days
limited clinical results experimentally, survival rate 100%in 15dogs in another study: complete failure in 17% and 33% with branches of cranial and caudal vascular branches respectively. angiography recommended to ensure that both branches are present |
|
|
lateral caudal flap
vessel? uses? |
based on right and left caudal arteries and veins which branch from the caudal gluteal arteries and veins. located ventral to coccygeal vertebrae
uses: perineal and caudodorsal pelvic regions |
|
|
lateral caudal flap technique
|
cranial border is a horizontal line at the level of tail attachement
dorsal or ventral midline incision made over tail tail amputated between cd2/cd3 flap is rotated. outcome: only experimental: 79% survival |
|
|
latissimus dorsi myocutaneous flap. what vessel (s) is it based on? uses?
|
latissimus has V shaped vascular pattern.
single dominant pedicle relies on thoracodorsal artery: supplies dorsal portion of the muscle ventral portion supplied lateral thoracic arteries uses: enables closure of myocutaneous defects like body wall less pliable and elastic so dimensions must be careful |
|
|
latissimus dorsi myocutaneous flap technique
|
caniodorsal point: ventral to acromion and caudal to triceps
skin incised from this point to level of head of thirteenth rib ventral border at the thoracic skin fold, level to lower third of humerus paradoxical respiratory movement may be seen when used as thoracic body wall reconstruction |
|
|
what is the most common cause of flap necrosis? why does this happen
|
inadequate blood supply
flap elevation tension hematoma/seroma-flap pressure |
|
|
what are some ways to monitor flaps? when do they usually declare themselves by?
|
color
warmth bleeding most declare themselves by day 6 can prick middle of flap to see if it bleeds doppler and fluorescein are very unreliable in 1 study of superficial temporal flaps in dogs, fluorescence at days 0 and 3 did not correlate with survival at day 7. |
|
|
ways to salvage a failing flap:
|
if under to much tension, release the edges
if infection, C&S in humans, VAC helps other things that have been looked at with conflicting results: pentoxyfilline, dextrans, vasodilators, Ca blockers, hyperbaric O2 |