![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
117 Cards in this Set
- Front
- Back
|
Right Ventricle Failure
|
increases peripheral vascular capillary pressure>fluid leak edema increases right ventricular pressures>jugular venous distension |
|
|
Left Ventricle Failure
|
increases back pressure of blood into the pulmonary circulation (edema) life threatening |
|
|
Vasodilators
|
decreasing cardiac work decreasing oxygen consumption increasing cardiac output |
|
|
Vasodilators
|
isosorbide dinitrate hydralazine |
|
|
Vasodilators Side Effects
|
reflex tachycardia |
|
|
Diuretics
|
eliminating excess sodium and water from the kidneys reduce volume overload (edema) |
|
|
Diuretics
|
Loops (most efficient/high ceiling; drug of choice) potassium sparing (helps minimize potassium loss from thiazides and loops) |
|
|
Beta-Blockers
|
decrease heart rate and force of contraction Metoprolol, Carvedolol calms the heart down to prevent further damage |
|
|
Cardiac Glycoside
|
inhibits Na+/K+ ATPase indicated for: severe left ventricular insufficiency (+Acel & Diuretic) increases contraction in the atrial and ventricular myocardium |
|
|
Blood Flow
|
-into right ventricle -contraction forces pulmonary valve open -into pulmonary trunk -blood unloads CO2 & loads O2 -left atrium contraction of left ventricle forces aortic valve open -aorta>body>venae cavae |
|
|
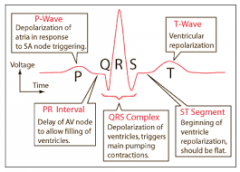
Electrocardiogram
|
|
|
|
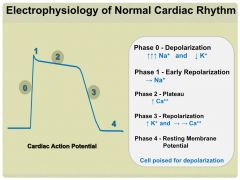
Cardiac Action Potential |
|
|
|
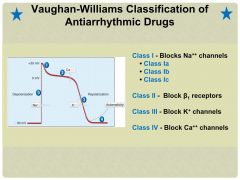
Vaughan-Williams Classification of Antiarrhythmic Drugs |
|
|
|
Quinidine
|
Class 1A (Sodium Channel Blockers) -also blocks K+ channels, 1st antiarrhythmic used,good oral bioavailability -side effects: ventricular paroxysmal tachycardia -Anticholinergic properties: GI disturbance & cinchonism |
|
|
Cinchonism
|
tinnitus, blurred vision, sweaty skin |
|
|
Procainamide
|
similar to quinidine except side effects include lupus erythematosus-like syndrome (long time use) but also less toxic can be used as a local anesthetic |
|
|
Lidocaine
|
-drug of choice for acute ventricular tachycardias, emergency termination of VT, post cardioversion or during open heart surgery -least cardiotoxic Na+ channel blockers -administered IV ONLY |
|
|
Mexiletine
|
can promote synergism |
|
|
Flecainide
|
-poorly tolerated and limited to experienced providers -reserved for life threatening supraventricular arrhythmias |
|
|
Propranolol, Metoprolol, and Esmolol
|
Class 2-Beta Blockers -antiarrhythmic agents by depressing automaticity; also has direct effect on cardiac membrane receptors -Adverse Effects: bradycardia, hypotension, fatigue, bronchospasm -safe drugs with few serious side effects |
|
|
Propranolol
|
Drug of choice for treating cardiac arrhythmias resulting from hypertension |
|
|
Metoprolol
|
most widely used beta-blockers for arrhythmias less bronchospasms than propranolol |
|
|
Esmolol
|
very short acting for acute emergency therapy (IV only) |
|
|
Amiodarone
|
Class 3- K+ Channel Blocker very broad spectrum antiarrhythmic & very potent, most commonly used antiarrhythmic mainstay of therapy for atrial fibrillation |
|
|
Amiodarone Side Effects and Other Considerations |
Drug can accumulate in many different tissues including the heart, eye (corneal microdeposits), skin (photodermatits), and lungs (pulmonary toxicity) drug will be discontinued in over half of patients |
|
|
Two Classes of Ca++ Channel Blockers
|
Non-Dihydropyridines- angina, arrhythmias, decrease conduction velocity and the firing rate |
|
|
Verapamil & Diltiazem
|
Verapamil has greater action in the heart than on vascular smooth muscle Major Indication: Supraventricular tachycardia |
|
|
Adenosine
|
-Inhibits Ca++ & K+ channels (decreases conduction velocity at the AV node) -Drug of choice for abolishing acute PSVT -Extremely short duration -Side Effects: facial flushing, headache, hypotension, and shortness of breath |
|
|
Arrhythmias are caused by:
|
electrolyte disturbances and overstimulation of the heart and can originate anywhere in the heart |
|
|
Common Types of Arrythmias are:
|
-Premature contractions (Ventricular) -Flutters (atrial and ventricular) -Fibrillations (atrial and ventricular) |
|
|
Ischemia
|
Sudden, severe, pressing chest pain starting substernal & radiate to left arm caused by an imbalance between myocardium oxygen requirement and oxygen supply |
|
|
Effort Angina
|
-fixed obstruction in the coronaries -triggered by exercise, cold, stress, or heavy metals -therapeutic goal is to increase oxygen delivery (vasodilation) |
|
|
Variant Angina |
-spasms of coronaries -triggered by alcohol, drinking cold liquids, REM sleep (occurs at rest or at work) -goal is to increase oxygen delivery (decrease vasospasms) |
|
|
Unstable Angina |
recurrent episodes of small platelet clots which can also precipitate local vasospasm goal is to increase oxygen delivery (decrease platelet aggregation) |
|
|
Nitrovasodilators
|
Stable Angina/Effort Angina |
|
|
Nitroglycerin
|
-Donates Nitric Oxide which promotes increased myocardial blood supply & decreased pre-load (venous vasodilation) and afterload (arterial vasodilation) -Drug of Choice for stable angina -preferred route: sublingual (prophylactic therapy-transdermal patch) |
|
|
Nitroglycerin
|
Tolerance (nitrate-free periods) Reflex tachycardia (paradoxical increase in oxygen demand) |
|
|
Isosorbide Dinitrate
|
same as nitroglycerin except duration of action is considerably longer |
|
|
Ca+ Channel Blockers
|
|
|
|
Ca++ Dihydropyridines
|
increase smooth muscle relaxation (vasodilation) |
|
|
Ca++ Non-Dihydropyridines
|
Angina- increase smooth muscle relaxation, decrease heart rate and contractility |
|
|
Diltiazem
|
variant and unstable angina- has greater effect in the vasculature than does Verapamil & therefore produces more incidence of reflex tachycardia |
|
|
Verapamil
|
Ca++ Channel Blocker -Relatively selective for the myocardium and is less effective as a systemic vasodilator -Primary effect: depress SA node and AV conduction (decrease O2 demand & vasospasms) -Good choice for prophylaxis |
|
|
Nifedepine & Nicardipine
|
Prototype of the dihydropyridine group -Causes arterial vasodilation Chronic Stable & Unstable Angina -not as effective as other vasodilators or beta-blockers |
|
|
Drug of Choice for Treating Variant Angina
|
Non-Dihydropyridines |
|
|
Beta-Adrenergic Receptor Blockers
|
Hypertension, Arrhythmias, Myocardial Infarction, Angina (decrease heart rate & contractility, reduce work) |
|
|
Propranolol
|
contraindicated in asthmatics & patients with COPD |
|
|
Metoprolol
|
generally safer in patients with asthma and diabetes |
|
|
Other Therapies for Angina
|
Clopidogrel- decrease platelet aggregation Atorvastatin- HMG-CoZ Reductase Inhibitor |
|
|
The ABCs of Angina Management
|
Be: more physically active Control: blood pressure, cholesterol, body weight |
|
|
Calculating Blood Pressure
|
BP=COxPVR Cardiac Output: heart rate, contractility PVR: smooth muscle tone (kidney plays a major role in regulation) |
|
|
Controlling Moment-to-Moment Blood Pressure
|
Blood pressure>Baroreceptors "stretch">signaling to VMC>sympathetic/parasympathetic outflow>heart rate, stroke volume(arterial & venous dilation/constriction)>cardiac output/TPR>BP returns to normal |
|
|
Mechanisms Responsible for Long-term Blood Pressure Control |

|
|
|
Beta-Blockers
|
Highly recommended for first-line therapy in hypertension when concomitant disease is present Use cautiously in patients with acute heart failure or diabetes Side Effects: hypotension, fatigue, bradycardia |
|
|
Beta-Blockers for Hypertension
|
-Propanolol -Metoprolol-most commonly used |
|
|
Labetalol
|
effects (3:1) B1:A1 this combined effect is desirable for treating hypertensive emergencies & pheochromocytoma |
|
|
Esmolol
|
very short half life, used for hypertensive emergencies |
|
|
A1-Blockers
|
-First dose syncope -Seldom used as monotherapy in hypertension -Primarily used to treat benign prosthetic hypertrophy Side Effects: syncope, reflex tachycardia, orthostatic hypotension, sexual dysfunction |
|
|
Prazosin
|
selective antagonist, decreases PVR rarely used as single agent to treat hypertension |
|
|
Phentolamine
|
primarily used to manage pheochromocytoma & another hypertensive emergencies |
|
|
Vasodilators
|
-Decrease PVR Oral: Hydralazine&Minoxidil (long-term) Parenteral: Nitroprusside(short-term) Ca+ Channel Blockers(Verapamil, Diltiazem, & Nifedipine) Side Effects: hypotension, reflex tachycardia |
|
|
Hydralazine
|
-oral -Almost always given with beta-blocker, a diuretic and/or a nitrate Monotherapy is accepted in gestational hypertension |
|
|
Minoxidil
|
-used for moderately severe hypertension -Almost always given with beta-blocker, a diuretic and/or a nitrate *hypertrichosis* |
|
|
Sodium NItroprusside
|
-Parenatal (must be given by IV infusion) -Used for hypertensive crisis, malignant hypertension, and severe heart failure -Contains cyanide (poison risk) |
|
|
Calcium Channel Blockers (Hypertension) |
Non-Dihydropyridine: more cardioselective -decrease in PVR -safe to use in asthmatics -Side Effects: constipation, flushing, hypotension |
|
|
ACE Inhibitors
|
-Reduces PVR with no reflex cardiovascular response -inhibits the enzyme that hydrolyses angiotension 1 to angiotension 2 -ACE inhibitors also directly inhibit the degradation of Bradykinin Side Effects: dry cough, hypotension, skin rash |
|
|
Captopril
|
first-line antihypertensive and a good choice for initiating therapy in patients with severe heart failure Contraindicated: pregnancy, angioedemia |
|
|
Lisonopril (and all other -prils) |
all prodrugs |
|
|
Losartan (and other -sartans) |
-Developed as alternatives to ACE inhibitors -Block Angiotensin Receptor (AT1) |
|
|
Hydrochlorothiazide
|
-Block Na+/Cl- transporter thereby inhibiting NaCl reabsorption |
|
|
Reserpine
|
Blocks release of neurotransmitter (NE) at postganglionic terminal -First effect therapy to be used -Side Effects: sedation, nightmares, mental confusion, depression |
|
|
Clonidine and a-Methyldopa
|
a-Methyldopa- nightmares, mental confusion, and depression (used to treat hypertension during pregnancy) |
|
|
General Risk Factors for Hypertension
|
obesity family history high salt diet smoking excessive alcohol consumption African American diabetes |
|
|
Therapeutic Uses for Diuretics
|
-Congestive Heart Failure -Chronic Renal Failure -Pulmonary Edema -Cerebral Edema -Hypertension -Glaucoma -Hypercalcemia |
|
|
Acetazolamide
|
-MOA: inhibition of CA> inhibition of bicarbonate reabsorption -Benefits: Glaucoma (most common), mountain sickness -Adverse Effects: potassium wasting, allergic rxns |
|
|
Dorzolamide
|
Carbonic Anhydrase Inhibitor -MOA: same as Acetazolamide -Benefits: glaucoma -Differences: site of action, topical admin, minimal side effects |
|
|
Mannitol
|
-MOA: no utilization of a transport system; always administered IV -Benefits: mainstay of treatment of patients with acute renal failure, good for decreasing brain volume and intracranial pressure Side Effects: dehydration & hypernatremia |
|
|
Furosemide
|
(Most Efficacious Diuretic Available) -MOA: inhibits the Na+,K+,2Cl- symporter -Indications: congestive heart failure, hypertension, drug of choice for acute pulmonary edema & peripheral edema, acute renal failure -Adverse Effects: ototoxicity, hypotension, dehydration, allergic rxn |
|
|
Hydrochlorothiazide |
-most widely used diuretic -MOA: block Na+,Cl- transporter thereby inhibiting NaCl reabsorption -Indications: hypertension, CHF, diabetes insipidus Adverse Efects: hyponatremia & hypotension, hyperlipidemia, allergic rxns |
|
|
Spironalactone
|
(not very efficacious) -MOA: synthetic steroid that inhibit aldosterone receptors in the collecting tubule -Benefits: drug of choice in hepatic cirrhosis, useful in counteracting K+ wasting associated with other drugs, CHF, hyperaldosteronism Adverse Effects: hyperkalemia, gynecomastia |
|
|
Three Phases of Clot Formation
|
2. Platelet Phase 3. Coagulation Phase |
|
|
Vascular Phase
|
damage to the blood vessels lead to vascular spasm of the smooth muscle in the vessel wall |
|
|
Platelet Phase
|
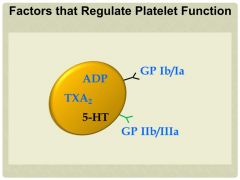
-damaged endothelium release von Willebrand Factor, which makes the surfaces of the endothelial cells "sticky" -platelets sticking to the surfaces of endothelial cells change morphology becoming "activated" and release ADP & TXA2 -the clump initiate the coagulation phase (thrombin, fibrinogen, and fibrin) |
|
|
Coagulation Phase
|
-fibrin entraps and stabilizes the initially loose platelet plug
|
|
|
Strategies to Prevent Thrombosis
|
-inhibit platelet function -inhibit fibrin formation |
|
|
Heparin
|
-indirect inhibitor of thrombin -anticoagulant (cofactor for anti-thrombin 3) -arterial emboli, acute deep vein thrombosis, MI &DIC -drug of choice for pregnant women -bolus IV injection followed by continuous infusion -Adverse Effects: bleeding, hypersensitivity |
|
|
Warfarin
|
-inhibits production of activated vitamin K ("new" coagulation factors) -primarily to prevent formation of venous thrombi -100% oral bioavailability -excessive bleeding, teratogen |
|
|
Factors that Regulate Platelet Function
|
|
|
|
Aspirin
|
inhibits TXA2 production -makes platelets less "sticky" sot that clot cannot form Adverse Effects: excessive bleeding |
|
|
Clopidogrel
|
Antiplatelet-inhibits function ADP -makes platelets less "sticky" so that clot cannot form -highly recommended in patients undergoing placement of coronary stint |
|
|
Alteplase (tPA)
|
-"fibrin selective" drug -preferentially binds to and activates plasminogen that is bound to fibrin VERY EXPENSIVE |
|
|
Protamine Sulfate
|
antidote for Heparin toxicity |
|
|
Vitamin K1
|
antidote for Warfarin toxicity |
|
|
Hemostasis
|
after being damaged |
|
|
Thrombosis
|
formation of a blood clot inside a blood vessel |
|
|
Extrinsic Pathway
|
-very rapid but only good for small clots |
|
|
Intrinsic Pathway
|
-slow but produces larger clots |
|
|
Hypochromic Anemia
|
(microcytic, hypochromic) results from iron deficiency |
|
|
Megaloblastic Anemia
|
(macrocytic, normochromic) Results from B12 or Folic Acid deficiency |
|
|
Ferrous Sulfate
|
Absorption-small intestine (vitamin C can help) |
|
|
Deferoxamine
|
(iron overdose) |
|
|
Cobalamin
|
-megaloblastic: helps regulate adequate production of tetrahydrofolate -neurologic damage: regulates the conversion of methylmalonyl-CoA to succinyl-CoA |
|
|
Folic Acid Deficiency
|
Susceptible: strict vegetarians/vegans, pregnant, alcoholics |
|
|
Folic Acid
|
helps regulate adequate production of tetrahydrofolate (required for DNA synthesis), anemia can occur within months -oral ingestion |
|
|
Causes of Anemia
|
-Increased Demand -Decreased Production -Blood Loss -Bone Marrow Disease -Sickle Cell Disease |
|
|
Type 1 (Familial Hyperchylomicronemia)
|
-Deficiency of lipoprotein lipase -not associated with increase in CHD Therapy: low fat diet |
|
|
Type 2A (Familial Hyperchylomicronemia)
|
-defect in synthesis/processing of LDL -increases risk for ischemic heart disease Therapy: Diet, Niacin+BABR |
|
|
Type 2B (Familial Combined Hyperlipidemia)
|
-overproduction of VLDL -similar to above Therapy: Diet, Niacin+BABR |
|
|
Type 3 (Familial Dysbetalipoproteinemia)
|
-defect in apolipoprotein E -increases risk for vascular disease Therapy: Niacin + Fibrate |
|
|
Type 4 (Familial Hypertriglyceridemia)
|
-overproduction/ decreases removal of VLDL TG -increases risk for ischemic heart disease Therapy: Diet, Niacin and/or Fibrate |
|
|
Type 5 (Familial Mixed Hypertriglyceridemia)
|
-elevated cholesterol and greatly elevated TG -overproduction/decreased removal of VLDL and CM Therapy: Diet, Niacin and/or Fibrate |
|
|
Atorvastatin
|
-useful in all types of hyperlipidemias -increases LDL receptors -small increase in HDL levels -contraindicated in pregnancy/nursing mothers |
|
|
Niacin
|
-most effect agent for increasing HDL -most prominent side effect: prostaglandin-induced cutaneous flushing |
|
|
Bile Acid Binding Resins
|
Primary role: to facilitate the formation of micelles which promote processing of dietary fat |
|
|
Colestipol & Cholestyramine
|
-lower cellular cholesterol -increase LDL receptors -Gritty, may affect the absorption of other drugs |
|
|
Genfibrozil & Fenofibrate
|
increase VLDL clearance adverse reactions are rare |
|
|
Ezetimibe
|
selectively inhibits NPC1L1 (a transport protein) |