![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
58 Cards in this Set
- Front
- Back
Finding Diagnosis |
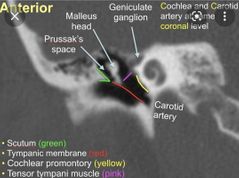
Soft tissue attenuation region in left middle ear cavity, expanding the Prussak space, eroding scutum and ear ossicles, extending into mastoid. Cholesteatoma |
|
|
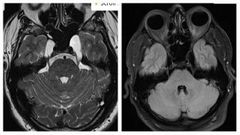
How cholesteatoma appear in MRI? |
It restricts diffusion Not enhancing ( if it does it is chloroma) |
|
|
What are the types of cholesteatoma? |
Pars flaccida Pars tensa |
|
|
Differences BTW acquired and congenital cholesteatoma? |
Acquired ( pars flaccida) Scutum eroded first Congenital (pars tensa) Inner ear involved earlier More common than flaccida |
|
|
What are the complications of acquired cholesteatoma ( pars flaccida) ? 4 |
They grow onto Prussak's space Erosions to First scutum, then long process of incus It make a fistula with the lateral semicircular canal Affect facial nerve |
|
|
Best sequence for assessment of cholesteatoma? |
EPI DWI Single shot echo planer |
|
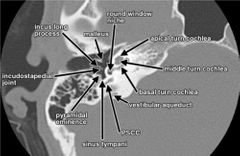
Name structures |
|
|
|
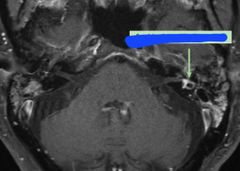
Perilymphatic fistula ( labyrinthine fistula) Commonest cause Commonest involved canal ? Classic history? 2 |
Cholesteatoma Lateral semicircular canal Sudden Fluctuating sensorineural hearing loss Vertigo |
|
|
Other complications of cholesteatoma ? 4 |
Facial nerve Intracranial extension ( tegment tempani) Sigmoid venous sinus ( thrombosis) EAC auto mastoidectomy |
|
|
Otitis media common in ---- age group ---- syndrome ? Why? |
Pediatric Down syndrome, horizontal configuration of eustachian tube |
|
|
When to call it chronic otitis media radiologically? |
If fluid persist more than 6 weeks |
|
|
Differences BTW otitis media and cholesteatoma? 3 |
OM mucosal thickening, no erosions, never displace ossicles Cholesteatoma non dependent mass, erosions, displaces ossicles |
|
|
Complications of Otitis media? 4 |
Coalescent mastoiditis ( erosion of mastoid septae) Facial nerve palsy Dural sinus thrombosis Meningitis, labyrinthitis |
|
|
If dural vein thrombosis occur what are the 2 complications might happen? |
Venous infarction ( mix cytotoxic and vasogenic edema) Hydrocephalus from altering CSF drainage |
|
|
What is labyrinthitis ossificans? What age group? Risk factor? In those cases ----- is contraindicated |
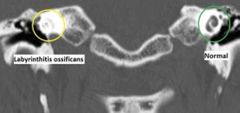
Is calcifications of cholea 2-18months Meningitis Cochlear implant |
|
Finding Diagnosis Causes 4 |
Enhancement of left semicircular canal Labyrinthitis URTI Acute otomastoiditis Meningitis ( bilateral usually) |
|
|
What are the 6 segments of facial nerve? |
Cisternal segment ( intracranial) Canalicular segment ( meatal) Labyrinthine segment Geniculate ganglion Tympanic segment Mastoidal segment Through sylomastoid foramen to extratemporal segment |
|
|
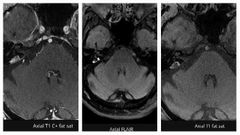
What are the facial nerve segments that show enhancement? 3 |
Labyrinthine Geniculate ganglion and tympanic Mastoid The rest not enhancing |
|
|
What diseases causes enhancement of cisternal, canalicular and extratemporal enhancement of facial nerve ? 4 |
Bell's palsy Lymes, Ramsey hunt and cancer |
|
|
How the enhancement of facial nerve will be in cancer ؟ |
Nodular enhancement |
|
|
Differences BTW Bells and Ramsey hunt syndrome |
Bell's usually viral, enhancement will be in the canalicular segment Ramsey is reactivation of HSV also CN5 can be involved |
|
|
When I say conductive hearing loss in you female, you say ? |
Otosclerosis ( otospongiosis) |
|
|
What are the types of Otosclerosis?2 |
1 fenestral type ( conductive HL) 2 cochlear type ( sensorineural HL) more severe form |
|
|
Findings in type 1 Otosclerosis? |

Bone resorption of the fissula ante fenestram anterior to oval window |
|

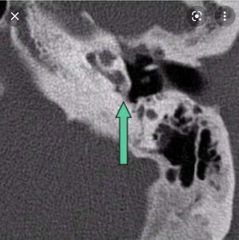
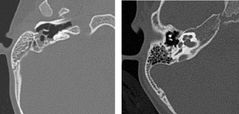
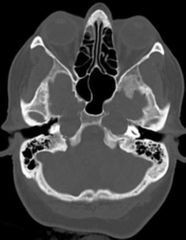
Finding Diagnosis |

CT through the left temporal bone demonstrates a circumscribed region of demineralisation immediately anterior to the oval window, in the bone between the cochlea and vestibule. Fenestral Otosclerosis |
|
|
What is fissula ante fenestram ? |
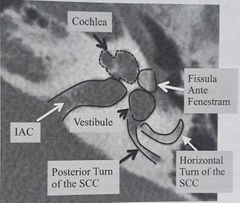
Is anterior to oval window Bone between cochlear and vestibule |
|
Finding Diagnosis Buzzword |

Retrofenestral type Otosclerosis Double ring or halo sign |
|
|
Treatment of Otosclerosis? |
Stapedectomy with cochlear implant If less severe ( fluoride) 😅 |
|

Aunt minnie Risk factor ? Classic symptom? |

Superior semicircular canal dehiscence Increased ICP Noise induced Vertigo ( Tullio's phenomenon) |
|
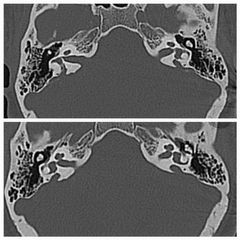
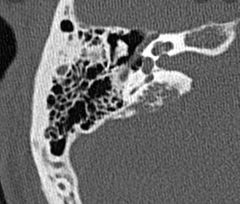
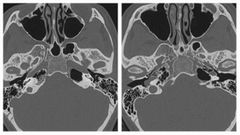
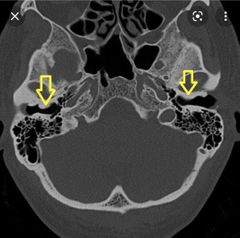
Finding ( aunt minnie) Diagnosis Classic history |
Bilateral large vestibular aqueducts (VAs). The VA measures 3 mm at the operculum and 2.5 mm at its mid-portion. Left hearing aid device is noted
Image of how normal vestibular Aqueduct should be less than the posterior semicircular canal Progressive sensorineural HL ( usually bilateral) they are not born deaf |
|
|
Most common cause of congenital sensorineural hearing loss? |
Large Vestibular Aqueduct syndrome |
|
|
Association with large vestibular aqueduct syndrome? |
Cochlear deformity near 100% ( absence of bony modiolus) |
|
|
What are the two opposite ends of cochlear congenital malformations? |
Michel's aphasia ( most severe) Mondini malformation ( least severe) |
|
|
What is Mondini malformation? Pathophysiology? Clinical symptoms? Associations? 2 |
Normal cochlear is 2.5 turns Mondini has 2 turns only The second and third are fused and form a cystic apex Sensorineural HL with preserved high frequency sounds ( basal turn is normal) Large vestibular aqueduct syndrome Enlarged vestibule |
|

Finding Diagnosis |
The vestibular aqueducts are enlarged bilaterally with incomplete partition between the middle and apical cochlear turns and unusually bulbous vestibules (Mondini anomaly). |
|

Finding Diagnosis Associations 2 |
Absent cochlear, vestibular Aqueduct and vestibule
Michel's aplasia ( complete labyrinthine aplasia) Anencephaly and thalidomide exposure |
|
|
How michel's aplasia looks different than labyrinthitis ossificans? |
Look at vestibular aqueduct it is normal in labyrinthitis ossificans and absent in Michel's aplasia |
|
|
Timing in utero for Mondini and Michel's aplasia to happen? |
Michel's aplasia early 3rd week ( total deafness) Mondini later 7th week ( high frequency sounds can be heard) |
|
Finding Likely diagnosis Associated syndrome? |
Moth eaten, permeative lytic lesion in the right petrous temporal bone involving the vestibular aqueduct. Endolymphatic sac tumor Von Hipple Lindau syndrome |
|
Finding Diagnosis Classic MRI finding? 2 Associated syndrome? |
T1 hyperintense, T2 hyperintense, multilobulated mass in the right petrous bone at the location of the vestibular aqueduct. DWI normal. Endolymphatic sac tumor T2 bright and intense enhancement Von Hipple Lindau syndrome |
|
|
Most common inner ear tumor is? |
Paranganglioma of jugular fossa ( glomus jugulare or jugulotympanicum tumor) |
|
|
Paranganglioma in MRI appearance? |
Salt and pepper Highly vascular with flow voids |
|
Finding Diagnosis |
Bilateral cystic enlargement of Meckel's cave containing CSF. Petrous apex encephalocele ( herniation of meckel's cave) |
|
Finding Diagnosis |
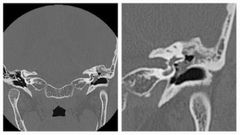
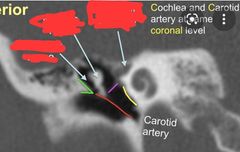
There is an aberrant right ICA, which enters the skull base through an enlarged inferior tympanic canaliculus just in front of the jugular bulb. Then courses anteriorly along the cochlear promontory in a typical fashion to join the petrous ICA. There is a relative narrowing as it turns forward in the tympanic canaliculus. The aberrant ICA bulges up into the hypotympanum and abuts /bulges the inferior eardrum outward. It also abuts the malleus insertion |
|
|
Aberrant internal carotid artery Classical history Pathophysiology |
Pulsatile tinnitus Involution C1 cervical internal carotid artery then collateral develop from the corticotympanic artery It can be seen as vascular lesion with pulsatility behind tympanic membrane by ENT |
|
|
Apical petrositis Is a complication of Complications of apical petrositis? 6 |
Otomastoiditis but rare Osteomyelitis of skull base Vasospasm of ICA Subdural empyema Venous sinus thrombosis Temporal lobe stroke Meningitis |
|

Finding Diagnosis |
Bone resorption of the petrous apex with no obvious lesion Apical petrositis |
|
|
What is the syndrome which is a complication from apical petrositis? |
Gradenigo syndrome |
|
|
What is Gradenigo syndrome ? Classical symptom? Classical triad? |
6th cranial nerve palsy from apical petrositis if it involves Dorello's canal Lateral gaze palsy Otomastoiditis Face pain neuropathy Lateral rectus palsy |
|
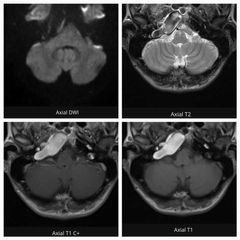
Finding Diagnosis |
Within the right petrous apex is a large lobulated lesion with strikingly increased intrinsic T1 signal, heterogeneously low T2 signal and no contrast enhancement. The lesion demonstrates low DWI signal and diffusion values somewhat facilitated compared to normal brain parenchyma. It is separate from the inner ear structures and middle ear cavity. Cholesterol granuloma |
|
|
Classical finding in cholesterol granuloma in MRI? |
T1 and T2 bright ( with hemosiderin lining) No diffusion restriction Faint peripheral enhancement |
|
|
Pathophysiology of cholesterol granuloma? Most common symptom? |
Obstruction of the air cells with repeated cycles of hemorrhage and inflammation leading to expansion of the bone and remodelling Hearing loss |
|
|
Commonest petrous apex lesion is ? |
Cholesterol granuloma |
|
|
Petrous apex cholesteatoma how different than middle ear cholesterol? |
Cholesteatoma of petrous apex is an epidermoid and it is congenital not acquired Slow growing with bone remodelling like cholesterol granuloma |
|
|
Differences BTW cholesteatoma and cholesterol granuloma of the petrous apex ? |
Cholesteatoma dark T1, bright T2, restrict on DWI Cholesterol granuloma bright T1 and T2 with no diffusion restriction |
|
|
Finding Diagnosis Risk factors Organisms |
Soft tissue thickening along the left external auditory canal. Extensive skin thickening and subcutaneous inflammatory change in the pre and post auricular regions. Heterogeneously enhancing soft tissue thickening extending superiorly along the temporalis and subgaleal space of the temporal bone. No appreciable focal hypodense collection within the region. Malignant otitis externa ( necrotising otitis externa) Diabetes ---> pseudomonas AIDS ----> aspergillus |
|
|
What is external auditory canal exostosis ? Common in ? |
Overgrowth of bone in the external auditory canal
Surfers with recurrent infections
|
|
|
In external auditory canal atresia What ENT people want to know? 3 |
Is it bone or soft tissue Is it covering normal middle and inner ear Is there aberrant course of facial nerve |