Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
57 Cards in this Set
- Front
- Back
|
3 small bowel diseases which show dysregulation in their immune system
|
IBD
coeliac primary immune def |
|
|
name some mucosal tissues of the human body
|
GI tract (salivary gglands- anal canal), resp tract, uro-genital tract, mammary glands
|
|
|
name some secondary lymphoid tissues
|
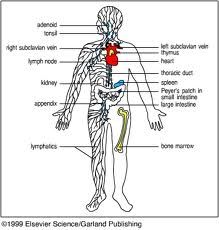
remember: peyer's patches in small intestine (ileum)
|
|
|
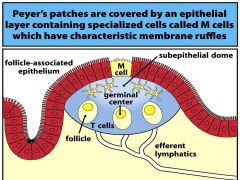
what specialised epithelial cells are present in Peyer-s patches (ileum)
- what are their characteristics |
|
|
|
what are the function of M cells at the epithelial surfaces of Peyer's patches?
- by what transport mechanism - what happen's on the lamina propria side? |
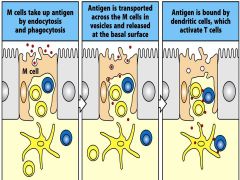
M cells in close proximity to underlying immune cells.
TRANSPORT ANTIGENS--->lamina propria side: co-stimulatory signals |
|
|
apart from M cells in Peyer's patches of the ileum, what other cells in the epithelium are important for the gut's immune defence
|

& CD8 killer T cells
|
|
|
villi (in addition to peyer's patches) also contain immune cells.
- which are in the lamina propria |
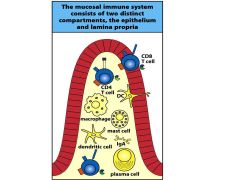
CD4, mac, mast, dendritic, plasma cells
|
|
|
how are activated effector T cells sent to their destined place in the lamina propria of the small intestine?
|
T cells 'homed' to peyer's patched → dendritic cells present antigen → T cells activated → lymph →blood → appropriate chemokines & receptors attract effector T cells to gut.
|
|
|
which receptor do activated effector cells bind to on the endothelium of gut capillaries to enter the villi where they will act
|
MadCAM-1
|
|
|
which Ig predominates in the humoral intestinal response produced by plasma B cells
- role |
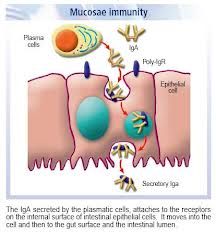
80% IgA- AGGLUTINATION & NEUTRALISATION at mucosal sites (also at other mucosal tissues)
|
|
|
Intraepithelial Lymphocytes (IELs): T cell (CD8) expression of which integrin anchors them in the epithelium
|
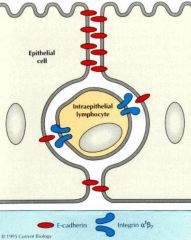
αE:β7
|
|
|
what cell type are the majority of IELs? (intraepithelial lymphocytes)
- how do they respond to epithelial cell infection |
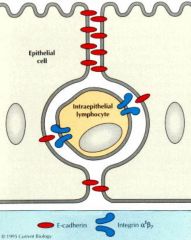
CD8+ Killer T cells
- kill infected cell via perforin/granzyme & Fas-dependent pathways |
|
|
in mucosal hyperresponsiveness, T cells show a higher level of activation & a stronger response where there shouldn't be.
- what molecules are absent to prevent dendritic and T cell maturation? |
chemokines
|
|
|
IgA def is a primary immunodef, what disease does is predispose to
|
coeliac's disease
|
|
|
food allergy demonstrates what type of hypersensitivty
- cells involved? - common symptoms |
IMMEDIATE type 1 IgE-mediated
cross-link on MAST cells - vomiting (intestinal contraction) - diarrhoea - puritis (itching_, urticaria (itching), anaphylaxis (rare) : from wide haematogenous dissemination |
|
|
which enzyme is present in coeliac's disease that modifies gluten so it can be presented to CD4 T cells (MHCII) causing an autoimmune response?
- what type of hypersensitivity reaction does it show |
tTG (tissue transglutaminse)
can be used for dx - DELAYED type 4 hypersensitivity: Tcells & macrophages |
|
|
how to dx (Ix's) for coeliac's disease
|
BIOPSY
serology: IgA & tTG |
|
|
2 types of autoimmune inflammatory hepatobiliary cirrhosis
|
autoimmune hepatitis
primary biliary cirrhosis (? primary sclerosing cholangitis- suggested) |
|
|
autoimmune hepatitis is a type of autoimmune inflammatory hepatobiliary cirrhosis...which shows loss tolerance against liver tissues
- which 3 serum antibodies can be detected on Ix |
antibodies to:
- nuclear antigens (ANA) - smooth muscle (ASM) - liver kidney microsomala antigens (LKM1) |
|
|
PBC (primary biliary cirrhosis) is a type of autoimmune inflammatory hepatobiliary cirrhosis...showing chronic cholestatic LIVER disease with small & medium INTRAhepatic duct destruction.
- which serum antibody can be detected in high concs? |
IgG AMA (antimitochondrial ab's) 98% - M2 subtype
|
|
|
only therapy for PBC
|
UDCA (ursodeoxycholic acid)
|
|
|
where's the control centre for energy homeostasis ( integrates neural & hormonal)
|
hypothalamus
|
|
|
what controls short-term satiation
|
PEPTIDES produced in the STOMACH & GI tract
|
|
|
what controls long-term body weight
|
HORMONES
|
|
|
which peptides controlling short-term satiation is released from the I-cells of the duodenum & jejunum
- in response to what - effect |
CCK in response to FAT & PROTEIN
seonsory --> hindbrain |
|
|
which2 peptides controlling short-term satiation is released from the L-cells of the GI tract
- in response to what - effect |
1) PeptideYY (PYY) AFTER meals
-inhibits gastric emptying - satiation 2) GLUCAGON-LIKE peptide-1 (GIP-1) on INDEIGESTION - inhibits gastric emptying - satiation |
|
|
which 2 peptides controlling short-term satiation is released from the OXYTINIC cells of the duodenum & jejunum
- in response to what - effects |
1) OXM- AFTER meal
- reduces appetite 2) GHRELIN - BEFORE meals - increases lipogenesis - hunger |
|
|
2 hormones that communicate to hypothalamus to alter energy balance (increase energy burn)
- which cells release them - which malfunctions in obesity |
LEPTIN- adipose
INSULIN- pancreatic ISLET's of Langerhan's (endocrine) |
|
|
what's the effect of reduced leptin levels (normally produced from adipose cells)
|

mimics STARVATION = unrestrained appetite, increased fat deposition, reduced energy burn
|
|
|
how does ORLISTAT work to reduce obesity
SE's |
inhibits pancreatic lipase
decreases triglyceride dig & absorption SHORT-term x. cramping, severe, diarrhoea |
|
|
LORCASERIN is a new anti-obesity drug. which receptor does it antagonise
|
5-HTc receptor antagonists
|
|
|
histology of normal small bowel
|
JEJUNUM- tallest villi, plicae circularis, goblet cells and crypts of Lieberkuhn
ILEUM- Peyer's patches, smaller villi & crypts, less prominent plicae, goblet cells |
|
|
2 reasons why the bowel can become ischaemic
|
OCCLUSION in mesenteric arteries:
- thromboembolism - atherosclerosis PERFUSION insufficiency: - shock - strangulation - drugs - hyperviscosity |
|
|
which part of the GI wall suffers from ischaemia first (i.e. the most metabolically active)
|
mucosa- can replace quickly
(muscle damage cannot replace quickly) |
|
|
3 outcomes of ischaemic bowel
|
- RESOLUTION
- FIBROSIS, stricture, chronic ischaemia, 'mesenteric angina' - GANGRENE, perforation, peritonitis, sepsis, death |
|
|
what's Meckel's diverticulum
what ar ethe complications |
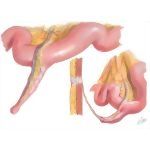
incomplete regression of vitello-intestinal duct, outpouching connected to umbilicus 2ft above ileocaecal valve:
X. bleeding, pain, perforation, divertilculitis |
|
|
primary tumours of small bowel are rare:
- 3 types |
LYMPHOMOA- (MALTomo- Bcell derived)
CARCINOID- locally invasve, produce hormones CARCINOMAS- Chron's & coeliac disease, presents late. |
|
|
secondary mets to small bowel are common:
from which 3 cancers |
ovarian
colorectal stomach |
|
|
S&Ss appendicitis
|
umbilical colic --> constant RIF
vomiting, constipation (or diarrhoea) tachycardic, shallow breaths, fever guarding peritonitis: wash-board rigidity, lay still ↑WCC & CRP |
|
|
pathology of acute appendicitis
- specific loc of wall? |

acute inflammation- neutrophils, eosinophils...
MUCOSAL ulceration exudate, pus |
|
|
3 complications of acute appendicitis
|
perforation/ rupture --> peritonitis --> sepsis
abscess fistula |
|
|
associations with coeliac disease
|
HLA-B8
dermatitis herpetiformis childhood DM |
|
|
pathological features of coeliac disease biopsy
|
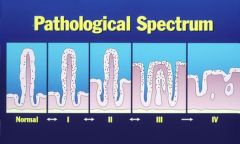
IELs (CD8) damage epithlial cells = villous ATROPHY
MALABSORPTION ↑IELs & ↑inflam cells in lamina propria PROXIMAL bowel worse |
|
|
S&Ss coeliac disease
- intestinal - extra-intestinal -general |
STEATORRHOEA
abdo pain & bloating N&V mouth ulcers & angular stomatitis, glossitis (B12 def) ↓weight, fatigue, weak, anaemia, osteomalacia failure to thrive asymp! |
|
|
5 complications of coeliac disease
|
anaemia
GI T-cell lymphomas (rare) small bowel carcinoma gall stones ulceration & strictures |
|
|
surgical criteria for bariatric surgery
|
BMI>35 + co-morbidities
or BMI>40 achieved 5% weight loss tried ALL non-surgical Rx medically & psychologically stable non-smoker |
|
|
3 types bariatric surgery
|
BYPASS - reversible
BAND SLEEVE |
|
|
common diseases causing malabsorption 6: CCCCBP
|
COELIAC
CHRON's Chronic PANCREATITIS CIRRHOSIS Biliary obstruction/ cirrhosis = ↓bile Post-infection uncommon: (pancreatic ca, drugs, Short bowel syndrome) |
|
|
S&Ss malabsorption
|
diarrhoea, steatorrhoea
↓weight, faitgue anaemia (pallor, conjunctivae, ulcers, stomatitis, koilonychia) glossitis bleeding/ bruising (VitK def) oedema (↓protein) |
|
|
Ix's for ?malabsorption
|
FBC, coagulation (vit K), U&Es (hydration), LFTs (albumin), Ca (vit D def), COELIAC serology (IgA, tTG)
STOOL (fat, infection) ENDOSCOPY + BIOPSY RADIOGRAPHY- X-ray, USS, ERCP, CT, MRI |
|
|
contraindications for artificial enteral feedin gsupport via NG/NG/PEG/PEJ
|
ulcers
obstruction perforation fistulas facial injury |
|
|
define acute and chronic intestinal failure
|
gut not able to supply nutritional & hydrational needs
ACUTE <2wks: mucositis, post-chemo CHRONIC- short gut syndrome |
|
|
causes of chronic intestinal failure
|
SHORT BOWEL SYNDROME- iatrogenic or congenital
Vascular (ischmia) Neoplasia Dysmotility Severe CIRRHOSIS Iatrogenic |
|
|
management of short bowel syndrome
|
supportive/ symptom control -Rx: PPIs, loperamide, codeine
PARENTERAL feeding (long-term) TRANSPLANT (last resort) |
|
|
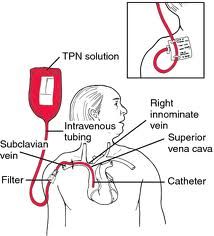
some complications of parenteral feeding
|
!!!PNEUMOTHORAX, puncture ARTERY, THROMBOSIS, SEPSIS!!!!
inappropriate use liver disease bone disease line fracture/ break psychosocial |
|
|
clinical features of refeeding syndrome
|
CV & resp FAILURE
bone marrow suppression- immunosuppression SEIZURES Metabolic disturbances: ↓K, ↓Mg, oedema, glucose metabolism shift, ↓vits |
|
|
commonest western cause small intestinal obstruction
|
adhesion (eg after surgery, prev intraperitoneal inflam)
or hernia |