Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
48 Cards in this Set
- Front
- Back
|
Describe the anatomy of the testes
|
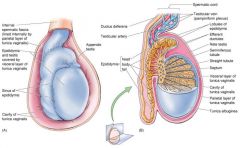
- Testes are 2 oval shaped compound tubular glands that produce sperm in response to gonadotrophins
- The are suspended in the sac-like scrotum by the spermatic cord which keeps their temperature low so that sperm production can continue - Each testis is surrounded by a capsule of 3 layers: 1. Tunica vaginalis = parietal and visceral parts derived from the peritoneum, with a cavity in between. The epididymis is also surrounded by this 2. Tunica albuginea = fibrous connective tissue 3. Tunica vasculosa = loose connective tissue with blood vessels - Posteriorly, the capsule forms the madiastinum testis that contains many interconected channels which provide a passageway for the sperm to enter the duct system - Deep to the tunica, strong connectign tissue septa extend into the testis, dividing it into about 250 pyramid-shaped lobules - Each lobule contains 1-4 highly convoluted semineferous tubules, in which the spermatozoa are produced |
|
|
Describe the contents of and the structures surrounding the testes and spermatic cord
|
Rule of 3:
- 3 surrounding layers 1. External spermatic fascia = external oblique muscle 2. Cremaster muscle and fascia = internal oblique muscle (think cremasteric reflex) 3. Internal spermatic fascia = transversalis fascia Contents: - 3 arteries: 1. Testicular artery - from aorta at L1/L2 2. Cremasteric artery 3. Artery to vas deferens - 3 Nerves 1. Genital branch of genitofemoral nerve (to cremaster muscle) 2. T10 to testes → pain of testicular trauma is referred to the T10 umbilical region 3. Ilioinguinal nerve (outside cord) - 3 others: 1. Vas deferens 2. Pampiniform (venous) plexus 3. Lymphatics to T10 → drain into the abdomen (NOT the groin so look for metastatic spread in para-aortic lymph nodes) |
|
|
What is the scrotum?
|
- Cutaneous sac consisting of 2 layers:
1. Pigmented skin and dartos fascia 2. Fascial layer including dartos muscle → wrinkled appearance of scrotum - Contains: 1. Testes 2. Epididymis 3. Lower end of spermatic cord |
|
|
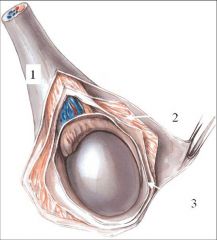
How do the testes get into the scrotum?
|
1. Testes develop on the posterior abdominal wall (7 weeks)
2. A fold of peritoneum (processus vaginalis) descends into the labioscrotal folds (developing scrotum) 3. As it passes through the developing abdominal wall it carries the fascial layers of the abdominal wall with it = layers of the spermatic cord 4. Testes descend behind the procussus vaginalis, being led by the gubernaculum, and ends up in the scrotum 5. At, or shortly after birth connection with the peritoneal cavity is closed = an easy route for indirect herniae |
|

What is this?
|
- Right sac is normal, left scrotal sac is empty
- Non-descending testis known as an ectopic testis - Must be surgically removed / pulled down as likely to metastasize if remains in the abdomen as to warm |
|

What is this?
|

- A sebaceous cyst = the commonest cause of a 'swelling down below'
|
|

What is this?
|
- Varicocoele = pampiniform plexus becomes varicose
- Left pampiniform plexus drains into the left renal vein so if a left sided varicocoele it may indicate a blockage at the kidney |
|

What is this?
|
- Hydrocoele = fluid in the cavity of the tunica vaginalis
- May be caused by a patent processus vaginalis, trauma, infection (eg. epididymo-orchitis), a tumour (so a new development should always be scanned), or testicular torsion |
|

What are the differential diagnoses for this?
|
- Hot, swollen testes:
1. Inflammation of testes / epididymis e.g. due to inflammation = orchitis or epididymitis 2. Torsion of the testes = testes has high horizontal lie and is very tender = medical emergency - Especially beware testicular torsion → 6-24 hours may be able to untwist and keep the testis. 24+ hours and the testis must be removed |
|
|
What is the ductus deferens and describe its path
|
- Vas deferens is the continuation of the epididymus on each side of the scrotum
- Straight muscular tube - Transports sperm from the epididymis to the prostatic urethra during the emission phase of ejaculation - Its terminal portion (called the ampulla) and the duct of the seminal vesicle form the ejaculator duct which opens into the prostatic urethra - Path: 1. Ascends in the spermatic cord 2. Traverse inguinal canal 3. Tracks around lateral pelvic wall 4. Pass between bladder and ureter 5. Forms dilated ampulla 6. Opens into common ejaculatory duct with the prostatic urethra - Rich autonomic innervation of smooth muscle fibres of the ductus deferens permits rapid contraction which propel the tube's contents towards the ejaculatory ducts - During ejaculation the ejaculatory duct and the duct of the seminal vesicle dilate to facilitate the entry of the sperms and seminal gland secretions into the prostatic urethra |
|

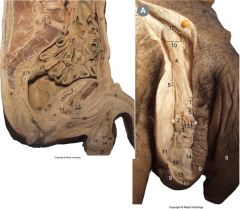
Label this diagram - especially 8, 29 and 35
|
8 = vas deferens
29 = seminal vesicle 35 = ureter |
|
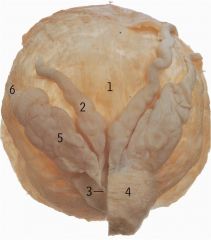
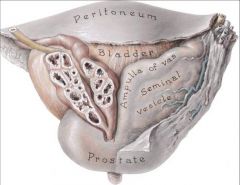
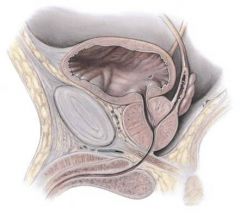
Label this (note 6 lies anterior to 5)
|
1 - Bladder
2 - Urethra 3 - Ampulla 4 - Prostate 5 - Seminal vesicle 6 - Vas deferens |
|

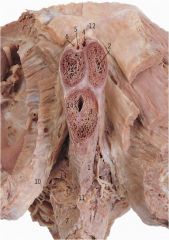
Label the parts of the urethra
|
13 = Bladder neck
19 = Prostatic urethra 14 = Membranous urethra 28 = Spongy urethra 8 = Penile urethra 27 = Sphincter urethrae |
|
|
Describe the features of the seminal vesicles and the ejaculatory duct
|
- Seminal vesicles are found above the prostate between the bladder and the rectum
- The secrete a fructose-rich, alkaline fluid that makes up 70% of ejaculated semen - The duct of the seminal vesicles joins the vas deferens at the ampulla behind the prostate - Together they form the 1-cm ejaculatory ducts that pass forward into the prostate - The ejaculatory ducts pierce and divide the prostate into lobes, and open into the prostatic urethra just before it leaves the prostate |
|
|
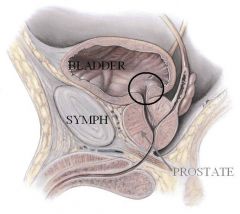
Describe the prostate
|
- Chestnut size gland that surrounds the prostatic urethra at the base of the bladder
- Composed of numberous small, compound alveolar glands from which excretory ducts originate and open independently into the prostatic urethra - It is divided into 5 lobes by the ejaculatory ducts = lateral x2, anterior, posterior and median - Because of its position the median lobe tends to push into the urethra and bladder when abnormal - Fibromuscular gland with many crevices → prostate infection may take 3-4 months to clear - The secretion of the gland forms about a 1/3 of the ejaculate volume and contains prostagladins, proteolytic enzymes and citric acid - The posterior surface is palpableby rectal examination - it should feel regular and firm with a midline groove - The prostate secretes seminal fluid into the urethra during ejaculation - Inferior to the prostate there are 2 small bulbourethral glands that secrete a sugar-rich mucous into the membranous urethra |
|
|
Why is the venous drainage of the prostate gland clinically significant?
|

- Prostate venous plexus drains into internal iliac veins
- The vertebral venous plexus also drains into here - Consequently a metastasis in the brain or skull may have orginated as prostatic cancer, as can spread upward |
|
Label this diagram
|
|
|
|
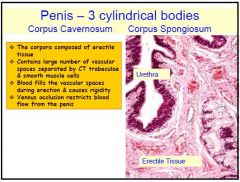
Describe the anatomy of the penis
|
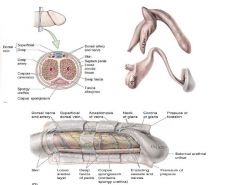
- Penis has 3 sections:
1. Root = rixed attachment to the perineum and pubic arch 2. Body = the free pendlous part 3. Glans = the sensitive distal end that inclues the external opening of the urethra - The penis is surrounded by 3 cylinders of erectile tissue = corpus cavernosum x2, each containing a deep artery (branch of internal pudendal) and forming the dorsum of the penis (extensions of the crura in the root of the penis), and a corpus spongiosum surrounding the spongy urethra, forming the ventral surface and the whole of the glans penis (extension of the bulb of the penis at the root) - The majority of the vessels and nerves supplying the penis are found on the dorsal side (note named when penis erect) and are branches of the internal pudendal artery - Each cylinder of erectile tissue is surrounded by a fibrous capsule called the tunica albuginea |
|
Label this diagram
|
1 - ventral surface of penis / tunica albuginea
2 - Corpus cavernosum 3 - Corpus spongiosum 4 - Dorsal vein 5 - Dorsal artery 6 - Dorsal nerve |
|
|
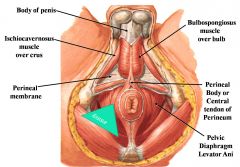
Where is the perineal body in a male?
|
- Between the bulb of the penis and the anus
|
|
|
Why are urethal catheterisations carried out (5)?
|
1. Remove urine in a patient who can't micturate
2. Irrigate bladder 3. Obtain an uncontaminated sample of urine 4. Biopsy of the bladder 5. Dilate constricted urethra |
|
|
Describe 2 disorders affecting the prepuce
|

1. Phimosis
- Prepuce cannot easily be retracted over the glans penis - May block urethra - Medical circumcision needed in the infant / adult 2. Paraphimosis - Retraction of the prepuce results in such constrictionof the neck of the glans that drainage of blood and lymph is affected - Medical circumcision needed |
|
|
Describe the parts of the urethra
|
1. Prostatic urethra = through prostate
2. Membranous urethra = through urogenital diaphragm 3. Spongy urethra = through corpus spongiosum |
|
|
What is oligozoospermia?
|
Clinical condition where this is an abnormally low number of spermatozoa in the semen. In azoospermio, no sperms appear in the ejaculate
|
|
|
What is cryptorchid testis?
|
- Maldescended testis = spermatogenesis is impaired because of the elevated temperature
- The germ cells are absent, while the Sertoli cells and Leydig cells secrete male sex hormones - Crytorchid testes are associated with increased incidence of malignant testicular tumours |
|
|
What is orchitis?
|
- Inflammation of the testis
- Occurs in some individuals who suffer mumps after puberty - Results in impaired spermatogenesis, occasionally leading to seminiferous tubule degeneration or at times, infertility |
|
|
Describe the features of testicular tumours
|
- Rare
- Most arise from germ cells - High degree of malignancy - The tumours present as a swelling or lump in the testis |
|
|
Describe the anatomy and function of the epididymis
|
- Has a head, body and tail segment
- It is located on the superior and posterolatereal surface of the testis - Its main function is sperm transport, maturation and storage - During their passage through the epididymis the sperms undergo structural maturation and become motile, the capabilities that are essential for successful fertilization - They are stored in the tail segment until ejaculation |
|
|
Describe diseases of the prostate
|
1. Benign prostatic hyperplasia
- The prostate gland enlarges in old age - Sex hormone dependent - Symptoms include urinary obstruction and bladder irritation 2. Prostatic cancer - Second most common cause of cancer-related deaths in men - Genetic, hormonal and environmental factors implicated in its pathogenesis - Blood levels of prostatic-specific antigen produced by normal or abnormal prostatic epithelial cells is often elevated in prostatic disorders - This finding is one of a range of diagnostic tests used to assess and differentiate between prostate hyperplasia, prostatitis (inflammation) and carcinoma |
|
|
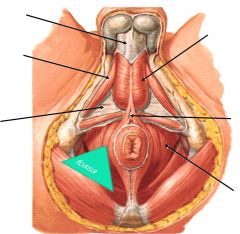
Describe the outcome of urethral damage
|
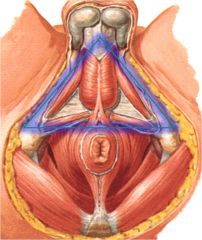
- The perineal membrane extends across
the urogenital triangle (blue glow) and leads to the formation of two potential spaces the superficial and deep perineal spaces or pouches - The deep pouch contains the membranous part of the urethra and some muscles, whilst the superficial pouch contains the spongy urethra - Fracture of the bony pelvis can lead to rupture of the membranous urethra with leakage of urine into the deep pouch Forceful blows to the perineum can rupture the spongy urethra and lead to extravasation into the superficial pouch |
|
|
Describe the histology of the testes
|
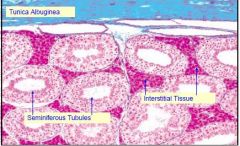
- Fibrous septa divide each testis into about 300 lobules, each containing 1-4 seminiferous tubules
- Seminiferous tubules are closed loops that contain 2 cells types: 1. Spermatogonia that undergo meiosis to give rise to haploid spermatozoa 2. Sertoli cells that support the developing sperm and secrete testicular fluid into the tubules - In between the seminiferous tubules there are vessels and clusters of testosterone secreting Leydig cells - The sperm pass into the rete testis, which are convulated networks of ducts lined by simple cuboidal cells with microvilli and a long flagellum |
|
|
What are the functions of Sertoli cells?
|
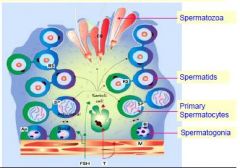
- Support, protection & nutritional regulation of developing spermatozoa – mediate the exchange of nutrients & metabolities
- Phagocytosis – during spermiogenesis excess spermatid cytoplasm (“residual body”) digested by Sertoli cell lysosomes - Secretion of fluid for sperm transport; also secrete “androgen-binding protein” controlled by FSH & testosterone; secrete “inhibin” which supresses synthesis and release of FSH - Produces “Mullerian-inhibiting hormone” that promotes regression of Mullerian (paramesonephric ducts) in the male fetus - Form the “blood-testis barrier” – few substances from the blood are found in the testicular fluid; spermatogonia have free access to materials from blood – occluding junctions between Sertoli cells form a barrier to transport of large molecules; thus advanced stages of spermatogenesis are “protected” from blood-borne noxious substances |
|
|
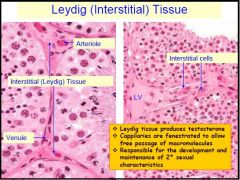
Describe the functions of the leydig cells
|
|
|
|
Describe the microstructure of the male duct system
|
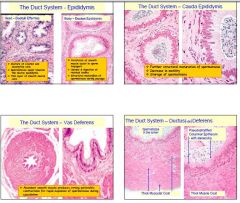
- The epididymis is formed by tall columnar epithelia with long microvilli (stereo-cilia)
- Testicular fluid is partly absorbed by this - The epididymis is surrounded by a fibrous capsule that is separate from the testis except at the head where the testis and epididymis join |
|
|
Describe the microstructure of the seminal vesicles
|
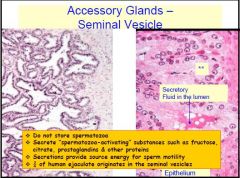
- Each seminal vesicle is formed from a slightly coiled tube that is 15cm long
- It is covered by 2 layers of smooth muscle and an external fibroelastic layer - The tube is lined by tall, secretory columnar epithelium - The ejaculatory ducts have no muscular coverings and are lined by columnar cells and smaller rounded cells |
|
|
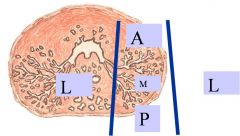
Describe the microstructure of the prostate gland
|
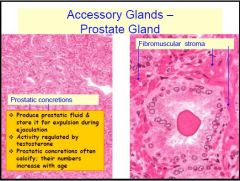
- Composed of 3 concentric rings of glanfs surrounded by smooth muscle and a fibrous capsule
- The smooth muscle contracts during ejaculation to squeeze the prostatic secretion into the urethra - 3 types of glands: 1. Inner periurethral glands = surround and secrete directly into the urethra 2. Outer periurethral glands = secrete into the urethra via short ducts 3. Peripheral zone glands = rings of glands is incomplete anteriorly and secrete via long ducts - Inner and outer periurethral comprise of the central zone |
|
|
Describe the microstructure of the penis
|
|
|
|
Describe the basic anatomy and neurovascular supply of the breast
|
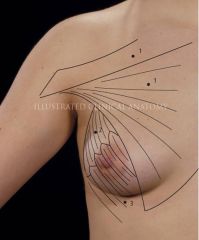
- Breast is a soft hemispherical organ lying in the superficial fascia of the anterior thoracic wall
- Between the 2nd - 6th ribs - Between the base of the breast and the underlying fascia is the retromammary space which allows the breast some movement - Medially the breast is adjacent to the lateral border of the sternum - Axillary tail of the breast extends laterally along the border of pectoralis major - The nipple is surrounded by a circular pigmented area - the areolar, which contains sebaceous glands called the tubercles of Montgomery - Lies on top of serratus anterior and pectoralis major (so if there is SA problems check the breast for lumps) - Arterial supply • Laterally by the lateral thoracic and acromiothoracic arteries off the axillary artery • Medially from the perforating and intercostal arteries off the internal thoracic artery from the subclavian artery • Also receives segmental supply from the 2nd to 6th anterior intercostal branches • Breast surgery may sometimes damage medial branches, leading to poor wound healing - Innervation: - Sympathetic supply to the smooth areolar muscle → in pregnancy and on the pill the nipples look darker |
|
|
How may breast lumps be classified?
|
1. Physiological
2. Benign 3. Malignant |
|
|
Describe the microstructure of the breast
|
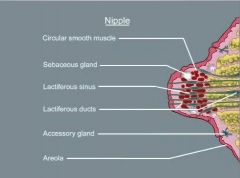
- The breast is composed of 15-20 milk-secreting lobules, each drained by its own lactiferous duct
- It is subdivided into lobules by the suspensory ligaments of Cooper, which originate as fibrous bands from the superficial fascia |
|
|
How may the breast be divided?
|

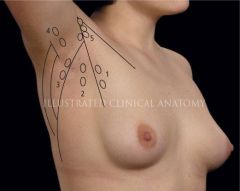
- May be divided into 4 quadrants
- Useful for describing where lumps are |
|
|
What benign lumps may arise in the breast?
|
- Arise from the connective tissues
1. Fibroadenomas - 'mobile mouse' = solid, well-defined hard lump which flees and moves under fingers on palpation. Arise form fibrous and glandular tissue and have a minimal risk of becoming malignant 2. Lipomas - often found on the skin of the breast and the reast of the body 3. Sebaceous cysts - found in the skin 4. Fat necrosis - following trauma → hollows in fat causing non-spherical appearance of breast |
|
|
Describe malignant lumps of the breast
|
- Usually hard, irregular and tethered to their surroundings
- May be associated with axillary lymphadenopathy - Roughly 90% of breast cancers arise from the epithelium of the ducts and 10% from the lobules |
|
|
Describe breast cysts
|
- Tender, smooth and fluctuant
- Occur with increasing frequency as the peri-menopausal period approaches |
|
|
Describe the lymphatic drainage of the breasts
|
- 75% of the breast lymph drains laterally to the axillary lymph nodes, which are arranged in 5 clusters
1. Anterior 2. Posterior 3. Lateral 4. Central 5. Apical - Superiorly these drain into the infraclavicular and lower cervical nodes - Inferior thoracics drain inferiorly into the internal thoracic chain to the diaphragm and anterior abdomen, and medially to the parasternal nodes, which may cross the midline and involve the other breast - Some of these nodes are often the 1st site of cancer spread - Surgical excision of suspicious breast lumps may involve sentinal, selective or total removal of axillary lymph nodes - This may lead to swelling of the arm, known as lymphoedema |
|
|
What is Peau D'Orange
|

- Not the colour of breast skin, but refers to the dimpling of subcutaneous oedema
- Caused by the breast skin becoming oedematous due to lymphatic blockage |
|
|
What is the triple method for ascertaining breast lumps?
|
1. Clinical examination
2. Fine needle aspiration cytology 3. Breast imaging using ultrasound or mammograpy |
|
|
What is an inverted nipple?
|

- Nipple is pulled inwards rather than being out
- Doesn't mean anything if has been present since puberty - However, if turns inwards later on is associated with tethering related to malignancy |