![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
299 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
Most Common cause of Rhinitis |
Adenovirus |
|
|
|
Consequences of Rhinitis |
Nasal Polyp |
|
|
|
What are nasal polyps? What causes them? When do you see them? |
-Protrusion of edematous, inflamed nasal mucosa -Due to repeated bouts of rhinitis -occurs in cystic fibrosis (test children with nasal polyps) & aspirin-intolerant asthma ---you don't see allergic nasal polyps in kids >> do a sweat test for CF
|
|
|
|
ASA-intolerant asthma
symptoms? common presentation? Pathogenesis? |
-triad: asthma, aspirin (or NSAID) induced bronchospasms, nasalpolyps -10% of asthmatic adults -Common presentation: 35 yo woman with chronic headaches or fibromyalgia develops occassional bouts of asthma -Pathogenesis: PGs blocked, lipoxygenase pathway left open >> bronchoconstriction >> asthma |
|
|
|
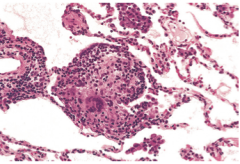
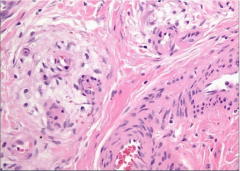
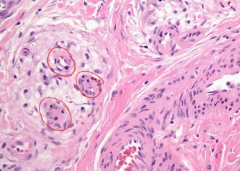
What is an angiofibroma?
Who do you see it in?
How does it present? |
benign tumor of nasal mucosa composed of large blood blood vessels and fibrous tissue
seen in adolescent males
presents with profuse epistaxis |
|
|
|
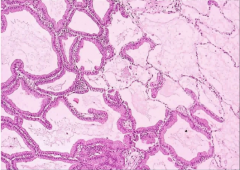
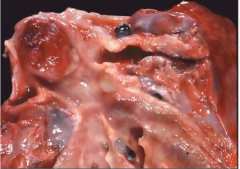
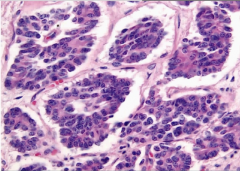
What is a nasapharyngeal Carcinoma?
Who do you see it in?
How does it present? |
-malignant tumor of nasopharyngeal epithelium -associated with EBV -seen in African children & Chinese adults -Biopsy reveals pleomorphic keratin-positive epithelial cells (poorly differentiated squamous cell carcinoma) in a background of lymphocytes -Presents with involvement of cervical lymph nodes |
|
|
|
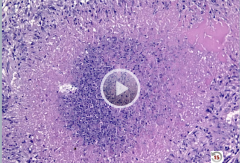
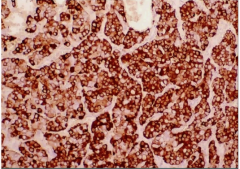
Biopsy: pleomorphic epithelial cells in field of lymphocytes |
Hint: Keratin positive -intermediate filament of epithelial cells
Nasopharyngeal carcinoma
|
|
|
|
Acute Epiglottitis
Cause?
Presentation? |
-Inflammation of epiglottis -H. flu type b is most common in immunized & -non-immunized children -Presentation: high fever, sore throat, drooling with dysphagia, muffled voice, inspiratory stridor -MEDICAL EMERGENCY due to risk of airway obstruction |
|
|
|
Laryngotracheobronchitis
Cause?
Presentation? |
Croup >> parainfluenza virus = most common cause
Presents with hoarse, barking cough and inspiratory stridor |
|
|
|
Vocal Cord Nodule |
-Singer's Nodule -arises on true vocal cord due to excessive use of vocal cords; usually bilateral -composed of degenerative (myxoid) connective tissue -resolves with rest |
|
|
|
Laryngeal Papilloma?
Cause?
Presentation?
Biopsy? |
-benign papillary tumor of the vocal cord -due to HPV6 & 11; papillomas are usually single in adults and multiple in children -Presents with hoarseness -Biopsy: koilocyte change (HPV) -rarely causes laryngeal carcinoma |
|
|
|
Laryngeal Carcinoma?
Risk factors?
Presentation? |
squamous cell carcinoma usually arising from epithelial lining of the vocal caord
Risk factors: alcohol & tobacco >> syndergism; rarely laryngeal papilloma
Presents with hoarseness; other signs include cough & stridor |
|
|
|
Clinical features of pneumonia |
-fever & chills -productive cough w/ yellow-green (pus) or rusty (blood) sputum -tachypnea w/ pleuritic chest pain (due to presence of bradykinin & PGE2) -decreased breath sounds -dullness to percussion -elevated WBC |
|
|
|
Physical diagnostics of lung consolidation
Difference from pleural effusion? |
decreased percussion, increased TVF, egophony, and pectoriloquy = consolidation
Effusion will only have decreased percussion |
|
|
|
Diagnosis pneumonia |
Chest xray sputum gram stain & culture blood cultures |
|
|
|
Complications of Pneumonia |
-abscess formation -empyema -intralveolar exudate >> complete fibrosis of that part of the lung -bacterial dissemination >> meningitis, arthritis, endocarditis |
|
|
What is it? Cause? |
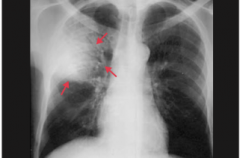
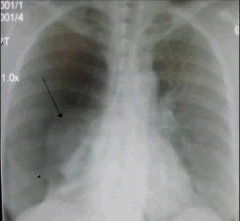
Lobar Pneumonia
-consolidation of an entire lobe (can involve entire lung) -bacterial cause usually; most common causes are Streptococcus pneumonia (95%), Klebsiella pneumonia, and Legionella
|
|
|
|
Streptococcus pneumoniae
Causes which disease? Seen in? Treatment? |
-gram positive dipplococcus -Most common cause of community-acquired pneumonia and secondary pneumonia (viral URI > bacterial pneumonia) -Seen in middle-aged adults & elderly; especially common in immunoglobulin deficiency, those w/ chronic conditions (CHF, diabetes, COPD), and those w/ lack of splenic function
-Treatment: penicillin G |
|
|
|
Pneumococcal pneumonia
Presentation? Complications? Prevention? |
-Presenation: sudden onset of chills, chest pain, rusty sputum -Complications: Empyema, effusion (no residual lung damage) -Prevention: Pneumovax |
|
|
|
Klebesiella pneumonia |
-most frequent cause of gram neg. pneumonia -enteric flora that is aspirated -most commonly affects debilitated and malnourished adults, specifically *diabetics *alcoholics *elderly in nursing homes -thick mucoid capsule >> gelatinous currant jelly sputum -complicated by abscess |
|
|
|
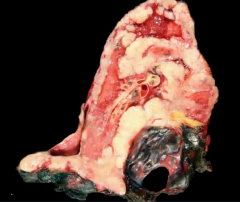
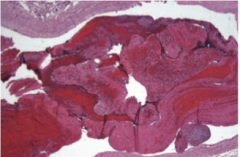
Phases of Lobar Pneumonia |
1. Congestion - due to congested vessels & edema 2. Red hepatization - due to exudate, neutrophils, and hemorrhage filling the alveolar air spaces, giving normally spongy lung a solid consistency 3. Gray hepatization - due to degradation of red cells within the exudate 4. Resolution - Regeneration of alveolar lining via type II pneumocyte stem cells (can cause pleuritis and permanent adhesions) |
|
|

What is it? What characterizes it? Areas involved? |
Bronchopneumonia
-characterized by scattered patchy consolidation centered around bronchioles -acute inflammatory infiltrates from bronchioles into adjacent alveoli -often multifocal and bilateral -caused by a variety of bacteria |
|
|
|
Causes of Bronchopneumonia
Who do you see these causes in? |
1. Staphylococcus aureus - 2nd most common cause of secondary pneumonia; complicated by abscess or empyema (nosocomial) 2. Haemophilus influenzae - common cause of secondary pneumonia and most common cause of exacerbated COPD; elderly 3. Pseudomonas aeruginosa - pneumonia in CF; also neutropenic & ventilated patients (nosocomial); fulminant infection 4. Moraxella catarrhalis - CA pneumonia (esp. in elderly) & 2nd most common cause of exacerbated COPD 5. Legionella pneumophila - CA pneumonia, pneumonia on COPD, or pneumonia in immunocompromised states; transmitted from water source; intracellular - use silver stain; can also use urine antigen -S. pneumoniae & Klebsiella can also cause |
|
|
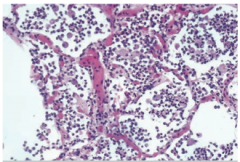
Lung Biopsy |
Bronchopneumonia -notice the neutrophils in the alveolar spaces |
|
|
What is it? Where is it? Presentation? |
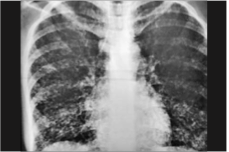
Interstitial Pneumonia = Atypical Pneumonia -diffuse interstitial infiltrates involving ≥ 1 lobe; alveolar spaces free of exudates -presents with mild UR symptoms: cough, mild fever, minimal sputum- can be apparent respiratory distress that doesn't match severity of symptoms (but CXR can look worse than pt.) -bacterial and viral causes |
|
|
|
Causes of Interstitial Pneumonia |
1. Mycoplasma pneumoniae - most common; affects young adults & children (military recruits/college students in dorm); Complications - autoimmune hemolytic anemia (IgM to I antigen on RBCs > cold hemolytic anemia) and erythema multiforme (nosocomial) 2. Chlamydia pneumoniae - 2nd most common; young adults (sim to MP); can also see chlamydia psittaci (from bird) - causes interstitial pneumonia with BAL showing intracellular organisms 3. RSV - most common cause in infants 4. CMV - due to posttransplant immunosuppressive therapy 5. Influenza - elderly, immunocompromized, and those w/ preexisiting lung disease; increases risk for superimposed S aureua or H flu 6. Coxiella burnetti - high (Q) fever; seen in farmers & veterinarians (spores on cattle from ticks or in cattle placenta); rickettsial but distinct from others because it (1) causes pneumonia, (2) doesn't require arthropod vector (heat resistant endospore) (3) no rash -Legionella also a cause |
|
|
|
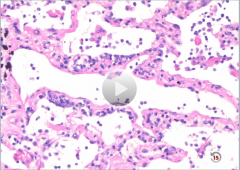
Interstitial Pneumonia
-air sacs predominantly empty -inflammatory cells in wall of interstitium |
|
|
|
Aspiration Pneumonia
Seen in? Causes? Clinical Features? |
seen in alcoholics and comatose patients
most often due to anaerobic bacteria in orpharynx (Bacteroides, Fusebacterium, Peptococcus)
Classic: right lower lobe abscess - right main stem bronchus branches at less acute angle |
|
|
|
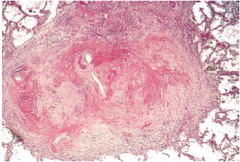
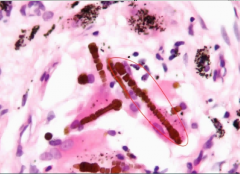
Histoplasmosis
Where is it seen? Who gets it? Presentation? Pathology? |
-Midwest (Ohio/Tennessee valley) - Carried by dung of starlings and bats – often seen in cave explorers, spelunkers, chicken farmers. -Presentation: non-productive cough; can simulate TB: coin lesions, consolidations, miliary spread, and cavitation >> marked dystrophic calcification of granulomas (most common cause of calcifications in the spleen) -Pathology: granulomatous inflammation with caseous necrosis; yeast form in macrophages -Treatment: usually self-limiting; amphotericin B or itraconazole |
|
|
|
Cryptococcus neoformans
Describe it. Found where? Presentation? Treatment? |
-Budding yeast w/ narrow-based buds surrounded by thick capsule -Found in pigeon excreta -Primary lung disease (40%): granulomatous inflammation with caseation -Treatment: fluconazole |
|
|
|
Blastomyces dermatitidis
Describe it. Seen where? in who? Presentation? Pathology? Treatment |
-Yeast have broad-based buds and nuclei -Occurs in Great Lakes region, central, & southeastern US -Most often associated with fishing, hunting, gardening, exposure to beaver dams; male dominant -produces skin and lung disease: skin lesions simulate squamous cell carcinoma -Granulomatous inflammation with caseous necrosis -Treatment: liposomal amphotericin B |
|
|
|
Cocciodioidomycosis
Describe it. Where do you see it? how do you get it? Presentation? Pathology? Treatment? |
-spherules with endospores in tissues -Contracted by inhaling arthrospores in dust (increased after earthquakes) in the southwest (valley fever) -Flu-like symptoms and erythema nodosum (painful nodules on lower legs; inflammation of subcutaneous fat) -Granulomatous inflamation with caseous necrosis -Treatment: self limited; if severe, itracoazole or fluconazole |
|
|
|
Asperigillus fumigatus
Describe it. Presentations/ Pathogenesis? Treatment? |
-Fruiting body and narrow-angled (<45 degrees), branching septate hyphae -Aspergilloma: fungus ball (CXR) develops in preexisting cavity (TB) in the lung >> massive hemoptysis -Allergic bronchopulmonary asperigillus: type I and type III hypersensitivities; IgE increased, eosinophilia; intense inflammation of airways and mucus plugs in terminal bronchioles >> repeated attacks >> bronchiectasis and interstitial lung disease >> treat w/ corticosteroids -Vessel invader with hemorrhagic infarctions and necrotizing bronchopneumonia -Treatment: voriconazole |
|
|
|
Pneumocystis jiroveci |
-no ergosterol in plasma membrane -cysts and trophozoites: cysts attach to type I pneumocytes -primarily an OI with CD4 count< 200 (AIDS defining) -Predominantly produces pulmonary disease >> fever, dyspnea, sever hypoxemia, diffuse intra-alveolar foamy exudates with cup-shaped cysts in silver or Giesma stains; CXR shows diffuse alveolar and insterstitial infiltrates -Treatment: TMP-SMX |
|
|
|
Primary TB
Pathogenesis? Features? |
-from initial exposure (aerosolized MT) -results in focal caseating necrosis in lower lung and hilar lymph nodes -foci undergo fibrosis and calcification >> Ghon complex *subpleural -asymptomatic +PPD -Pathogenesis: 1st 3 weeks = bacteremia, no symptoms; > 3 weeks = cell mediated immunity (IFN-y from Th1 cells crucial for macrophage activation >> TNF release >> epithelioid histiocytes) |
|
|
|
Progressive Primary TB |
-Polymorphisms in NRAMP1 may not develop effective immune response -also seen in immunocompromised hosts, malnourished children, elderly |
|
|
|
Secondary TB
Pathogenesis? Features? Presentation? |
-reactivation of Ghon complex, most commonly seen in AIDs, but can be due to aging -occurs at apex of lung (O2 highest here; poor lymph drainage) -forms cavitary foci of caseous necrosis, or miliary TB (regions of TB across lung), or TB bronchopneumonia -Presents: fever, night sweats, cough w/ hemoptysis, weight loss -Biopsy: caseating granulmoas; AFB = acid-fast bacilli |
|
|
|
Most common systemic spread of TB |
meninges (meningitis) *at base of brain, cervical lymph nodes, kidneys (sterile pyuria), lumbar vertebrae (Pott disease) |
|
|
|
caseating granuloma - TB -necrosis in center, epithilioid histiocytes at edge |
|
|
|
Obstructive Disease Spirometry |
Airway Obstruction
-decreased FVC -very decreased FEV1 -decreased FEV1/FVC -TLC increased (air trapping) (normal lung capcity = 7L; COPD = 8L) |
|
|
|
Chronic Bronchitis definition |
Obstructive Lung Disease
-chronic (extremely) productive cough lasting 3 months a year over a minimum of 2 consecutive years -highly associated with smoking; can be seen in city dwellers |
|
|
|
What characterizes chronic bronchitis? |
hypertrophy of bronchial mucinous glands>> hypersecretion of mucus
-increased thickness of mucus glands relative to bronchial wall thickness (Reid index increases to >>50%; normal = 40%) - b/c smokers bringing in tons of foreign particles >> more mucus needed to clear >> hypertrophy |
|
|
|
Pathogenesis of Chronic Bronchitis |
-irritants >> hypertrophy of mucous glands in trachea & bronchi >> induces increased goblet cells in smaller bronchi & bronchioles -primarily large bronchiole involvement, but morphologically, obstruction is due to small airway disease w/ goblet cell metaplasia causing mucous plugging in terminal bronchioles; coexisting emphysema --CD8 mediated - so can see lymphocytic infiltrate -can also see fibrosis, and sqaumous metaplasia on biopsy |
|
|
|
Clinical Features of chronic bronchitis |
-symptoms start after 20 pack years -productive cough due to excessive mucus production -cyanosis (blue bloaters) - mucus plugs trap CO2 >> increased PACO2 >> increased PaCO2 and decreased PaO2 -increased risk of infection & cor pulmonale (pulmonary HTN) -wheezing (due to terminal bronchiole involvement), crackles, cyanosis (early onset hypoxemia due to shunting), late-onset dyspnea |
|
|
|
chronic bronchitis w/ > 50% thickness of mucus glands |
|
|
|
chronic bronchitis (pic from USMLE Rx) -along with hypertrophy of the mucus glands and globlet cells, you will see lymphocytic (predominantly) infilatrate, squamous metaplasia, and fibrosis |
|
|
|
Emphysema definition & mechanism
|
obstructive lung disease
air space enlargement & destruction: destruction of alveolar air sacs >> loss of elastic recoil, increased compliance, and collapse of airways due to exhalation >> obstruction and air trapping w/ decreased tendency of the lung as a whole to collapse from chest wall >> barrel chest (bronchioles don't have cartilage and sacs are supposed to keep tube open w/ their elastic recoil, but when air causes drag along bronchioles now, they collapse) |
|
|
|
Pathogenesis of Emphysema |
imbalance of proteases and antiproteases -inflammation normally >> release of proteases by neutrophils & macrophages >> alpha1-antitrypsin neutralizes proteases -excessive inflammation or lack of A1AT (smoking actually denatures A1AT also) or TGFB1 polymorphism >> increase elastase activity >> loss of elasticity >> increased compliance >> emphysema -Key cells involved: inflammatory cells, necrosis of epithelial cells, destruction/ LOF of mesenchymal cells (so no ECM replacement, loss of elasticity & thus no fibrosis) [-CD8 mediated] |
|
|
|
Most common cause of emphysema |
smoking
pollutants >> excessive inflammation & protease-mediate damage >> centriacinar (smoke in central airway >> destroys respiratory bronchiole first) emphysema most severe in upper lobes |
|
|
|
AIAT deficiency
Pathogenesis? Complications? Genetics? |
-lack of antiprotease >> panacinar (antire acinus destroyed) emphysema most severe in the lower lobes -liver cirrhosis - misfolded protein accumulates in ER of hepatocytes >> liver damage; biopsy: pink, PAS + globules in hepatocytes -severity based on degree of deficiency -PiM - normal allele -PiZ - most common mutation >> misfolding >> accumulation in ER -PiMZ - heterozygotes = asymptomatic w/ decreased circulating levels of A1AT, but risk of emphysema w/ smoking -PiZZ - homozygous = panacinar emphysema + cirrhosis |
|
|
liver biopsy |
AIAT deficiency
PAS + pink globules in hepatocytes
|
|
|
|
Clinical Features of Emphysema |
-dyspnea and cough w/ minimal sputum -prolong expiration w/ pursed lips (pink puffer) to increase the back pressure and force walls open; sitting hunched over -weight loss (thin patients) -increased anterior-posterior diameter of chest ('barrel-chest') - increased FRC >> flattened diaphragm on CXR; distant heart and breath sounds -hypoxemia due to destruction of capillaries in the alveolar sac >> pulmonary HTN & cor pulmonale are late complications -decreased DLCO due to destruction of alveolar walls |
|
|
|
Mediastinal Emphysema |
-interstitial emphysema- air enters stroma of mediastinum, lung, or subQ tissue -due to vomiting, violent coughing (whooping cough), perforation, pts on respiratorys w/ obstruction -swelling of head & neck with crackling over chest -air often absorbed spontaneously |
|
|
|
Another cause of panacinar emphysema (genetic susceptibility) |
TGF-B1 polymorphisms |
|
|
|
Bullous Emphysema |
-can be caused by any form of emphysema -forms large subpleural blebs that can burst causing pneumothorax |
|
|
|
[Prognosis of COPD w/ BODE Index] |
-BMI -Airflow Obstruction (FEV1) -Dyspnea -Exercise capacity (6 min. walk test) |
|
|
|
[Treatment of COPD] |
-Smoking cessation -Bronchodilators - <10% increase in FEV1 ---B2 agonists, anticholinergics (most successful) -Inhaled glucocorticoids in those with <60% FEV1 (most effective when combined with bronchodilator) -Influenza & Pneumovax vaccines -O2 therapy, Rehab, Ventilatory Support, Surgery |
|
|
|
Asthma definition/hallmarks |
-obstructive pulmonary diseasereversible airway bronchocontsriction, most often due to allergic stimuli >> T1HS rxn [-syndrome of chronic airway inflammation w/ variant & recurring symptoms, pathophysiolgically defined as airflow obstruciton and hyperresponsiveness; aberrant & repeated episodes >> airway remodeling] -hallmarks: intermittent, reversible obstruction, chronic bronchial inflammation w/ eosinophils, smooth muscle hypertorphy & hyperreactivity, excess mucous secretion |
|
|
|
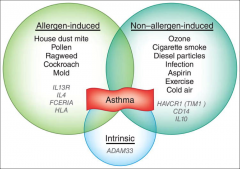
Genetic association w/ asthma |
-variable expression in family -loci on 5q: regulation of IgE synthesis, mast cell and eosinophil produciton -polymorphisms: IL-13, CD14, class II HLA, B2 receptors, & IL-4 receptors -20q: ADAM33 regulates smooth muscle cell and fibroblast proliferation |
|
|
|
Asthma causes/associations & test |
-presents in childhood -often associated w/ allergic rhinitis, eczema, and a family hx of atopy (genetically susceptible) -can arise from nonallergic causes like exercise, viral infection, aspirin, and occupational exposures (viral infection early in childhood increases risk - RSV < 6 months old esp.) -test w/ methacholine challenge [respond w/ FEV1 drop of ≥ 20% at ≥8 mg/dL to ≤ 16 mg/dL; high NPV] [-significant response to bronchodilator on PFT: >12% increase on FEV1 & 200 ml increase in FEV1] |
|
|
|
Pathogenesis of Asthma |
type 1 hypersensitivity -Allergens induce Th2 CD4+ T cells in genetically susceptible individuals >> Th2 secretes IL-4, Il-5, IL-13 >> re-exposure >> IgE-mediated activation of mast cells >> release of preformed histamine granules & generation of leukotrienes C4, D4, E4 >> bronchial hyperreactivity, bronchoconstriction, inflammation, edema (early phase) >> inflammation, esp. major basic protein derived from eosinophils, damages cells & perpetuates bronchoconstriction (late phase >4 hrs) >> repeated bouts >> hypertrophy and hyperplasia of SM >> airway remodeling (hypertrophy of SM & mucous glands >> increase BM thickness, increased vascularity & deposition of subepithelial collagen) [-chronic, severe asthma associated with Th17 response] |
|
|
|
Atopic Asthma |
-type I IgE mediated - allergen induced -hypersensitivity often w/ family history of atopy [-present younger: peak in 2nd decade] [-seasonal] |
|
|
|
Non-Atopic Asthma |
-no evidence of allergen sensitization or family hx of atopy -viral or occupation exposure thought to be trigger -viral inflammation to mucosa lowers the subepithelial threshold to irritants [-older presentation - 30s or 50s] [-normal IgE levels so neg. allergen testing] |
|
|
|
Drug-Induced Asthma |
-most common is aspirin sensitivity -patients present with recurrent rhinitis, nasal polyps, urticaria, and bronchospasms -thought to be due to aspirin inhibiting COX pathway w/o affecting leukotriene route >> asthmatics very sensitive to leukotriene C4, D4, E4 |
|
|
|
Clinical Features of Asthma |
-Episodic & related to allergen exposure; worse in morning & night --presents w/ cough, tachypnea, hypoxemia, pulsus paradoxus, severe dyspnea & wheezing >> largest difficulty is expiration (decreased I/E ratio) -progressive hyperinflation w/ air trapping -productive cough, classically w/ spiral-shaped mucus plugs (Curschmann spirals), and eosinophil-derived crystals (Charcot-Leyden crystals) -severe, unrelenting attack can result in status asthmaticus and death -CXR often normal, can show hyperinflation |
|
|
|
Cytokines & their Function in Asthma [lecture] |
IL-3 - differentiation of myeloid cells IL-4 - IgE class switch IL-5 - eosinophil chemoattractant IL-13 - eosinophil survival GM-CSF - increased production of eosinophils |
|
|
|
[Triggers of Asthma] |
-In Western countries, dust mites most common trigger |
|
|
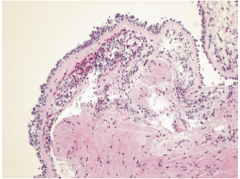
Lung Biopsy
Describe the airway changes seen in this disease |
Asthma -Thick mucous plugs in Curschmann spirals; sub-basement fibrosis; eosinophilic inflammation; SM hyperplasia -Overall airway changes seen in asthma: thickening of alveoli septa, SM hyperplasia, sub-basement membrane fibrosis, mucosal gland hypertrophy, goblet cell metaplasia, [denuded airway epithelium] |
|
|
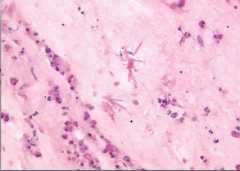
sputum smear |
asthmatic
Charcot-Leyden crystals from galectin-10 protein from eosinophils |
|
|
|
Asthma Treatment |
Bronchoconstriction is mediated by inflammation and parasympathetic tone, so treatment is based on this -B2 agonists (albuterol = SABA >> use for attacks; salmeterol/formoterol = LABA >> use with ICSs for prevention) -corticosteroids for chronic -avoidance of allergens [Allergen avoidance, Beta agonists, Corticosteroids, Drugs (other), Education, Functional Assessment] - 1) SABA, 2) low-dose ICS 3) LABA + low dose ICS or medium ICS 4) medium ICS + LABA 5) just increase dose |
|
|
|
Bronchiectasis definition |
-obstructive pulmonary disease -permanent dilation of bronchioles and bronchi; loss of airway tone via destruction of SM & elastic tissue results in air trapping -on gross examination, you will see dilated bronchioles in the periphery of the lung where they don't belong |
|
|
|
Bronchiectasis Causes |
Secondary disease due to necrotizing inflammation with damage to airway walls. Causes: -Cystic fibrosis: mucus plugging >> chronic infection -Kartagener syndrome - inherited defect in the dynein arm (primary ciliar dyskinesia), which is necessary for ciliary movement. Associated w/ sinusitis, infertility, and situs inversus -tumor or foreign body (obstruction) - localized to obstucted segment -necrotizing infection - S. aureus, Klebsiella, TB, MAC -allergic bronchopulmonary aspergillosis - hypersensitivity rxn due to aspergillus >> CI damage; seen in pts w/ asthma and CF -poor ciliary motility (smoking) |
|
|
|
Bronchiectasis pathogenesis |
Chronic & persistent infection -obstruction >> infection >> chronic inflammation -infection>> obstruction & inflammation
These result in damage to bronchial walls >> widening |
|
|
|
Clinical Features of bronchiectasis & histological morphology |
Clinical Features -cough -dyspnea -foul-smelling sputum >> TONS of puss being coughed up [-hemoptysis] [-crackles & wheezing] -complications: secondary (AA) amyloidosis hypoxemia, clubbing, & pulmonary HTN >> cor pulmonale Morphology -affects lower lobes bilaterally -dilated bronchioles -acute & chronic inflammation w/ exudate within the walls of bronchi and bronchioles -fibrosis of bronchial & bronchiolar walls >> chronic >> peribronchial fibrosis |
|
|
|
Restrictive Lung Disease Spirometry |
restricted filling of the lung >> decreased TLC, decreased FEV1, very decreased FVC, increased or normal FEV1/FVC (≥80%)
most commonly due to interstitial disease of the lung or with chest wall abnormalities (massive obesity) >> decreased compliance and increased elasticity |
|
|
|
Types of Restrictive Lung Diseases |
-Poor breathing mechanics: poor muscle effort (MG, polio), structural apparatus (scoliosis, obesity) -Interstitial Lung Disease (decreased diffusion capacity and increaesed A-a gradient)
|
|
|
|
Drugs that Cause Interstitial Lung Disease |
bleomycin, amiodarone, nitrofurantoin, busulfan, methotrexate, aspirin |
|
|
|
Hallmarks of Interstitial Lung Disease |
-reduced compliance & increased elasticity (more pressure to expand stuff lungs) >> increased RR & work of breathing >> dyspnea -decreased TLC, vital capacity, and residual volume; narrow/ small flow-volume loop -V/Q abnormalities due to damage to alveolar epithlium & interstitial capillaries >> hypoxia/ hypoxemia @ rest or w/ exercise -chest xrays show ground-glass, diffuse irregular lines, or nodules -progresses to pulmonary HTN >> cor pulmonale >> respiratory failure & honeycombing on CT |
|
|
|
Idiopathic Pulmonary Fibrosis
What is it? Pathogenesis? |
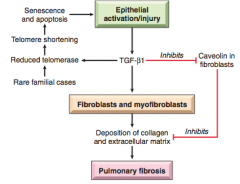
-fibrosis of lung interstium >> increased elasticity -likely related to cyclical lung injury >> TGF-B (for healing) from injured type I pneumocytes induces fibrosis -eosinophils, mast cells, TH2 cell, IL-4, & IL-13 -referred to as UIP on radiograph -Exclude secondary causes: drugs like bleomycin and amiodarone and radiation therapy |
|
|
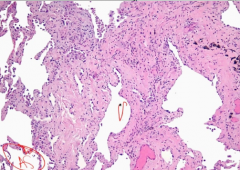
Lung Biopsy of dyspneic, hypoxic patient w/ ground glass consolidation on chest xray
Morphological progression of this disease? |
idiopathic pulmonary fibrosis - early cellular stage
-UIP: hallmark = patchy interstitial fibrosis -fibroblastic foci >> less cellular & more collagenous >> honeycombing |
|
|
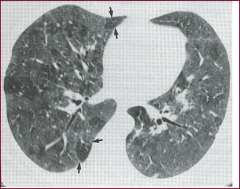
HRCT of chest |
-Ground Glass appearance: cellular stage of interstitial lung disease (centrilobar opacities/nodules) -UIP pattern: basilar, subpleural dominant, diffuse |
|
|
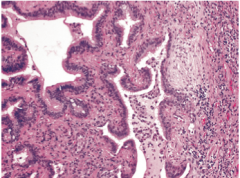
Lung biopsy of dyspneic, hypoxic patient |
idiopathic interstitial fibrosis - advanced stage with honeycombing seen on the left (late fibrotic stage) |
|
|

|
-Honeycombing: fibrotic stage of interstitial lung disease -UIP pattern: basilar, subpleural dominance, diffuse -no biopsy needed if definite UIP pattern found |
|
|
|
Clinical Features, Treatment & Prognosis of Idiopathic Pulmonary Fibrosis |
-progressive dyspnea & cough, exercise desat, reduced DCLO -PE: dry, velcro-like crackles during inspiration -later stages: clubbing, edema, cor pulmonale -bilateral mid-lower lobe infiltrate of chest xray -fibrosis on lung CT; initially seen in subpleural patches, but eventually results in diffuse fibrosis with end-stage honeycomb lung -treatment: lung transplant; corticosteroids help 10% of patients -Prognosis: 3-5 years |
|
|
|
Nonspecific Interstitial Pneumonia
what do you see? most common in who? |
-chronic & bilateral interstitial lung disease -cellular pattern: mild to moderate interstitial inflammation (lymphocytes & mast cells) with diffuse homogenous or patchy distribution -fibrosing patter: diffuse or patchy homogenous fibrosis -fibroblastic foci & honeycombing absent -commonly seen in RA |
|
|
|
Bronchiolitis Obliterans Organizing Pneumonitis
presentation? histology? treatment? |
-chronic interstitial lung disease -Presentation: cough & dyspnea; patchy consolidation on xray -Histology: polypoid plugs of loose organizing connective tissue in alveoli, alveolar ducts, & bronchioles -Treatment: oral steroids for 6 months |
|
|
Lung Biopsy of patient w/ cough & dyspnea & patchy consolidation on xray |
BOOP! -alveolar spaces filled wth balls of fibroblasts (Masson bodies) |
|
|
|
Pneumoconioses
What? Pathogenesis? |
restrictive lung disease -interstitial fibrosis due to occupational exposure -requires chronic exposure to small particles that are fibrogenic (1-5 um most dangerous size b/c get lodged @ bifurcation) -alveolar macrophages engulf foreign particles trapped in mucus and induce fibrosis |
|
|
|
Coal Workers' Pneumoconiosis |
-Exposure: Carbon dust -Path: diffuse fibrosis (black lung)>> shrunken lung (centrilobular emphysema can occur); associated with RA (Caplan syndrome) -mild exposure results in anthracosis (collections of carbon-laden macrophages) -no increased risk of cancer, but can develop pulmonary HTN & cor pulmonale rarely |
|
|
|
Silicosis
Exposure? Cause? Path? Pathogenesis? |
-Exposure: silica (sandblasters, foundries, & silica miners) -Most prevalent occupation disease in the world -Quartz is most toxic & fibrogenic -Path: Fibrotic nodules in upper lobes of the lung -Increased risk of TB (not cancer); "eggshell" calcification of hilar lymph nodes -Silica impairs phagolysosome formation by macrophages -Macrophages ingest particles >> release TNF & fibrogenic cytokines |
|
|
Lung Biopsy |
silicosis - whorled hyalinized collagen fibers with amorphous center |
|
|
|
Berylliosis |
-Exposure: Beryllium (beryllium miners & aerospace industry) -Path: nocaseating granulomas in the lung, hilar lymph nodes, and systemic organs (similar to sarcoidosis but driven by Be) -increased risk of lung cancer |
|
|
|
Asbestosis
Exposure? Associated Disease? |
Chronic interstitial lung disease -Exposure: asbestos fibers (construction workers, roofers, plumbers, and shipyard workers) -Associated w/: (1) parenchymal interstitial fibrosis (asbestosis) (2) local fibrous plaques (most common), or diffuse fibrosis of pleura (3) pleural effusions (4) lung (bronchogenic) carcinomas (more common) (5) pleural & peritoneal mesotheliomas (6) laryngeal carcinomas -asbestos x6 risk for cancer; asbestos + smoking = 49x risk |
|
|
|
Asbestos Pathogenesis & Manifestations |
Begins in lower lobes & subpleurally, then moves to middle & upper lobes -Fibrosis of lung and "ivory white" pleural plaques >> honeycombing (enlarged air spaces w/ thickened walls) & adhesions to chest wall & pleura >> scarring can lead to pulmonary HTN & cor pulmonale -pleural plaques=common manifestation: well-circumscribed collagen w/ calcification = "ivory white pleural plaques" pathogonominc for expsure but not precancerous -develop over parietal pleural & over domes of diaphragm -Manifestations are same as other chronic interstitial lung disease (dyspnea, lung crackles, clubbing) |
|
|
lung biopsy |
Asbestos (ferrunginous) bodies -lesions may contain long, gold-brown fusiform robs resembing dumb bells; these are fibers w/ associated iron form phagocyte ferritin (asbestos bodies), which confirm exposure |
|
|
|
Caplan Syndrome |
Rheumatoid arthritis and pneumoconiosis with intrapulmonary nodules |
|
|
|
Sarcoidosis definition & epidemiology |
restrictive lung disease
-systemic disease characterized by noncaseating granulomas in multiple organs -classically seen in African American females, Swedish & Danish -higher prevalence in nonsmokers |
|
|
|
Sarcoidosis Pathogensis & involved tissues |
-Due to CD4+ Th1 cell response to unknown antigen (IL-8, TNF, IL-2, IFN-y & macrophrage recruitment) -granulomas involve hilar lymph nodes & lung (mid-upper lobes) leading to restrictive lung disease - 90% of cases involved the lung -other commonly involved tissue: uvea (uveitis >> blurry vision), skin in 25% (cutaneous nodules - erythema nodosum), salivary & lacrimal glands (mimics Sjogren syndrome, but will see noncaseating granulomas) |
|
|
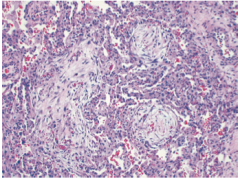
lung biopsy |
sarcoidosis - noncaseating epithelioid granulomas that are compact & surrounded by CD4 + lymphocytes |
|
|
lung biopsy |
Astroid body configuration of giant cells seen in sarcoidosis
Schaumann bodies, concentrations of calcium & protein, can also be seen in Sarcoidosis |
|
|
|
Clinical Features & Treatment of Sarcoidosis |
-dyspnea or cough - lungs involved in 90% of cases -hilar & paratracheal enlargement -fever, fatigue, weight loss, night sweats, hepatomegaly, splenomegaly -elevated serum ACE -hypercalcemia (1-alpha hydroxylase activity of epithelioid histiocytes converts vit D to active form >> hypervitamatosis D) -anergy to PPD due to reduction of peripheral Th1 cells -hypergammagloblinemia -diagnosis of exclusion -Genetic Predisposition: HLA-A1 & HLA-A8 -Treatment is steroids; 2/3 of cases resolve spontaneously; 1/3 get chronic disease & 10-15% develop diffuse interstitial fibrosis |
|
|
|
Lofgren's Syndrome |
-acute sarcoidosis -bilateral hilar lymphadenopathy of CXR -erythema nodosum (esp. on shins) -fever, polyarthritis -more common in women |
|
|
|
Hyerpsensitivity Pneumonitis
What? Who? |
-chronic interstitial (restrictive) disease -granulomatous (w/ eosinophils b/c hypersensitivity) reaction to inhaled organic antigens (pigeon's breeder's lung, farmer's lung) -silofiller lung: put things in silos, closed space, fermentation >> NO2 >> inhale >> react -Farmer's lung:on tractor, dust being blown up in the air and thermophilic actinomyces (which is a mold) is inhaled; leading to hypersensitivity -Bysinosis: worker in textile industry, and they get dyspnea (Monday disease) -Goodpasture Syndrome: starts in lungs (cough, hemoptysis), moves to kidneys |
|
|
|
Hypersensitivity Pneumonitis Pathogenesis |
Type III (immunecomplex mediated) & IV Hypersensitivity (CD8) reactions >> damage at the level of the alveoli (interstitial noncaseating granulomas) |
|
|
|
Hypersensitivity Pneumonitis Presentation |
-Acute: fever, cough, chest tightness, headache and dyspnea hours after exposure & resolves w/ removal of exposure (episodic) -Chronic disease presents w/ cough, dyspnea, malaise, weight loss -Chronic exposure leads to interstitial fibrosis (restrictive lung disease) |
|
|
Lung Biopsy of patient w/ fever, cough & dyspnea who is a farmer |
Hypersensitivity Pneumonitis
loosely associated non-caseating granulomas |
|
|
|
Pulmonary Eosinophilia |
chronic interstitial (restrictive) lung disease
-seen in a variety of diseases: acute eosinophilic pneumonia (rapid fever, dyspnea, hypoxia, diffuse infiltrates; BAL 25% eos), Loeffler Syndrome (transient lesions, benign), tropic eosinophilia, secondary eosinophilia (from asthma, allergies), & idiopathic chronic eosinophilic pneumonia (lymphs & eos in alveolar septal walls; fever, night sweats, dyspnea) |
|
|
|
Desquamative Interstitial Pneumonia
Who? Histology? Presentation? Similar Disease? |
-smokers -accumulation of macrophages w/ dusty brown pigment in air spaces, thickened alveolar septa, limited inflammatory infiltrate, mild interstitial fibrosis -PFTs show mild restrictive disease -Presentation: dyspnea and dry cough that stop w/ smoking cessation -Respiratory bronchiolitis is similar, but has bronchiolocentric distribution |
|
|
|
Idiopathic Pulmonary Hemosiderosis
Presentation? Pathogenesis? |
-primary (immune-mediated) diffuse alveolar hemorrhage syndrome -triad: hemoptysis, anemia, diffuse pulmonary infiltrates -similar to Good Pasture Syndrome, but no renal involvement or anti-basement membrane antibodies -immunosuppressive therapy works, so thought to be immune-mediated |
|
|
|
Good Pasture Syndrome
Presentation? Pathogenesis? Treatment? |
-primary (immune-mediated) diffuse alveolar hemorrhage syndrome -triad: hemoptysis, anemia, diffuse pulmonary infiltrates -proliferative, rapidly progressive glomerulonephritis & hemorrhage interstitial pneumonitis cause by antibodies to the alpha3 chain of collagen IV (basement membrane) -usually IgG, can be IgA or IgM -Treatment: plasmaphoresis or immunosuppressive therapy |
|
|
|
Wegner Granulomatosis
Histology? Manifestations? |
Pulmonary Angiitis -Lung lesions: necrotizing vasculitis & parenchymal necrotizing granulomatous inflammation -Manifestations: chronic sinusitis, epistaxis, nasal perforations, cough, hemoptysis, chest pain -PR3-ANCAs in 95% of cases |
|
|
|
Pulmonary Hypertension definition |
high pressure in the pulmonary circuit (MAP ≥ 25 mmHg at rest; normal 10-14 mmHg) |
|
|
|
Pulmonary Hypertension Pathologic Changes
|
-atherosclerosis of pulmonary trunk, medial smooth muscle hypertrophy of pulmonary arteries w/ some intimal fibrosis
-plexiform lesions in long-standing disease |
|
|
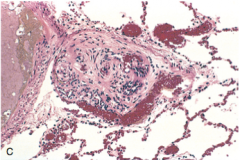
lung biopsy of dyspneic patient w/ a history of hypertension & atherosclerosis |
tuft of capillaries from long-standing pulmonary hypertension = plexiform lesions
-you see thickened capillary walls |
|
|
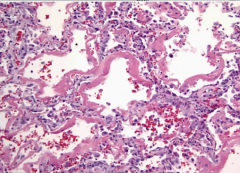
Lung biopsy of young woman with dyspnea |
-pulmonary hypertension (primary) -medial arterial thickening
-can be seen in secondary |
|
|
Lung biopsy of a 65 yo male w/ history of HF |
-pumonary hypertension (secondary -Plexiform complex
-can be seen in primary |
|
|
|
Complications/ Presentation of Pulmonary Hypertension |
-leads to RV hypertrophy w/ eventual cor pulmonale -presents w/ exertional dyspnea or right-sided heart failure
|
|
|
|
Primary Pulmonary Hypertension
Seen in? Presentation? Pathogenesis? Prognosis? |
-seen in young adult females -Presentation: fatigue, syncope, dyspnea on exertion, chest pain -familial form related to inactivating mutations of BMPR2 (TGF-B signalling path) >> excess proliferation of vascular smooth muscle (monoclonal endothelial proliferation) -sporadic forms may be associated with 5HTT (serotonin transporter protein) - increased protein in vascular smooth muscle >> increased proliferation -Prognosis: 2-5 years |
|
|
|
Secondary Pulmonary Hypertension
Causes & Course |
-COPD or interstitial lung disease b/c of destruction of lung parenchyma -mitral stenosis b/c increased resistance >> increased pressure -recurrent thromboemboli b/c of the decreased cross-sectional area of pulmonary vascular bed -autoimmune disease (scleroderma) or inflammation >> intimal fibrosis >> medial hypertrophy -left to right shunt: increased shear stress >> endothelial injury -sleep apnea or living at high altitude: hypoxic vasoconstriction -course: severe respiratory distress >> RVH >> decompensated cor pulmonale >> death |
|
|
|
ARDS Pathogenesis |
acute insult >> neutrophil accumulation >> release of Il-1 & TNF, FR, coagulation cascade >> endothelial activation>> more pro-inflammatory than anti- >> diffuse damage to the alveolar-capillary interface (diffuse alveolar damage) >> increased alveolar capillary permeability (from neutrophils getting in) >> leaking of protein rich fluid into air sac >> noncardiogenic pulmonary edema (normal PCWP) & congestion that combines with necrotic epithelial cells >> which is reorganized forming hyaline membranes in alveloli >> type II pneumocytes attempt to regenerate, but intra-alveolar fibrosis occurs -overall results in intrapulmonary shunting |
|
|
lung biopsy of a hypoxic, cyanotic patient w/ sudden onset |
-air sacs lined by dense hyaline membrane = ARDS |
|
|
|
Clinical Features of ARDS |
-hypoxemia w/ cyanosis w/ respiratory distress - due to thicken diffused barrier of air sacs (increased surface tension >> collapse of air sacs) ---collapsing pressure = surface tension/radius of the airway
|
|
|

|
-ARDS w/ diffuse white out |
|
|
|
Symptoms of Acute Respiratory Failure |
-hypoxic: anxiety, agitation, dyspnea, tachypnea, cyanosis, tachycardia -ventilatory: somnolence |
|
|
|
Etiology of ARDS
Causes, common mechanism, 2 types? |
-sepsis (most common cause), infection, shock, trauma, aspiration, pancreatitis, DIC, hypersensitivity rxns, amniotic fluid embolism, gastric aspiration, uremia, and drugs [-Hypoxemic Failure due to: shunt, V/Q mismatch, diffusion impairment, hypoventilation, low SvO2 (shock, hypovolemia)] - w/o hypercapnia [-Ventilatory Failure due to: decreased respiratory drive (neuromusc. disorder or CVA), increased mechanical load (pleural effusion, pulmonary fibrosis), excessive dead space (COPD), increased CO2 production (sepsis)] - w/ hypercapnia -common theme: activation of neutrophils induces protease- and free radical- mediated damage of type I and type II pneumocytes |
|
|
|
Stages of Respiratory Distress Syndrome |
-3 pathological stages of RDS: exudative stage in which intralveolar hyaline membrane formation occurs, a proliferative stage in which type II pneumocytes and fibrobasts proliferate, and a fibrotic stage characterized by lung remodeling and fibrosis
|
|
|
|
ARDS Treatment |
-address underlying cause -ventilation w/ PEEP (to keep air sacs from collapsing) -recovery may be complicated by interstitial fibrosis; damage and loss of type II pneumocytes leads to scarring and fibrosis -rule out cardiogenic edema w/ PCWP < 18 mmHg |
|
|
|
Neonatal Respiratory Distress Pathogenesis |
Inadequate surfactant levels: <1.5 lecithin:sphingomyelin ratio indicative of NRDS -surfactant made by type II pneumocytes -phosphatidylcholine (lecithin) is major component -Surfactant decreases surface tension in the lung, preventing collapse of alveolar air sacs after expiration -lack of surfactant leads to collapse of air sacs & formation of hyaline membranes |
|
|
|
Causes Neonatal Respiratory Distress Syndrome |
-Prematurity - surfactant production begins at 26 weeks, adequate levels @ 34 weeks -amniotic fluid lecithin:sphingomyelin >2:1 = mature (lecithin increases as surfactant produced) -C section- due to lack of stress-induced steroids (cortisol, ACTH) to increase synthesis of surfactant -Maternal diabetes - hyperglycemic mom >> baby hyperglycemic >> baby produces insulin >> insulin decreases surfactant production |
|
|
|
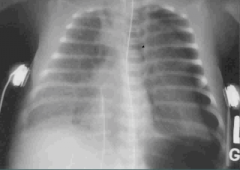
Ground-glass appearance = Neonatal Respiratory Distress |
|
|
|
Clinical Features & Treatment of Neonatal Respiratory Distress |
-increased respiratory effort after birth; tachypnea w/ use of accessory muscles & grunting -hypoxemia & cyanosis -diffuse granularity of the lung (ground-glass appearance) on xray -Treatment: steroids before birth & artificial surfactant at birth; PEEP to help with mass intrapulmonary shunting (due to atelectasis) (note: thyroxine can also stimulate surfactant production, but don't treat with this) |
|
|
|
Complications of Neonatal Respiratory Distress Syndrome |
-hypoxemia increases the risk for persistance of patent ductus arteriosus and necrotizing enterocolitis -supplemental oxygen increases the risk for free radical injury. Retinal injury >> blindness; lung damage leads to bronchopulmonary dysplasia |
|
|
|
Most common cause of cancer mortality |
Lung Cancer |
|
|
|
Key Risk factors of Lung Cancer |
-Cigarette smoke (85% of of lung cancer cause); 20x increase w/ 40ppy hx -polycyclic hydrocarbons & arsenic (squamous carcinoma) -risk directly related to duration & amount of smoking -radon - from radioactive decay of uranium (in soil) ---accumulates in closed spaces like basements ---responsible for public exposure to IR (2nd most common cause of LC) ---uranium miners have increased risk -Asbestos - more likely to develop LC than mesothelioma; 6[-11x ]increase -COPD/pulmonary fibrosis - 1-2x increase |
|
|
|
Average age of presentation of lung cancer |
60 years |
|
|
|
Lung Cancer Presentation & Next Steps |
-cough [new of change in cough] -wheezing -weight loss (adverse prognostic indicator b/c cancer usually advanced) -dyspnea -hemoptysis [endobronchial lesion likely] -chest pain -post-obstructive pneumonia -Next Steps: xray >> shows solitary "coin lesion" nodule (or uncalcified nodule) >> compare against prior xray >> present & unchanged = benign; new or growing >>biopsy |
|
|
|
Screening for Lung Cancer [lecture]
Who? What? |
-low dose CT recommended -30 year pack history -55-88 yrs of age -active smoker -someone who quit in the last 15 years |
|
|
|
Benign Lung Lesions |
-often occur in younger patients -can produce coin lesion -granuloma- often due to TB or fungus (esp. Histo in the Midwest) -Bronchial hamartoma- benign tumor made of lung tissue & cartilage (belongs there but is unorganized); often calcified |
|
|
|
Division of Lung Cancer |
Small-cell carcinoma (15%) - not amenable to surgical resection & treated w/ chemo
Non-small cell carcinoma (85%) - treated w/ surgical resection & doesn't respond to chemo |
|
|
|
Types of Non-Small Cell Carcinoma |
Squamous cell carcinoma (20%) Adenocarcinoma (38%) Large cell carcinoma (5%) Bronchioalveolar carcinoma Carcinoid tumor Metastasis to the lung |
|
|
|
Small Cell Carcinoma
Arise from? Histology? Seen in? Location? Complications? Mutations? |
-Histology: poorly differentiated small cells; arises from neuroendocrine (Kulchitsky cells = dark blue) -+TTF-1, napsin, synaptophysin, chromogranin on IHC -Association: Male smokers (>60 yo mostly) -Location: Central -Rapid growth and early metastasis (presents w/i few months) >> aggressive & inoperable >> treat w/ chemoradiation -Paraneoplastic syndromes common: ADH or ACTH or antibodies against Ca channels (Eaton-Lambert syndrome) -high propensity for brain & bone metastasis & visceral disease -Amplification of myc genes common |
Pneumonic: A's
ADH, ACHT, antibodies, amplificaiton |
|
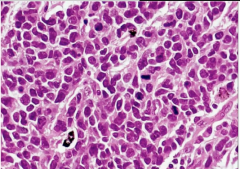
Lung Biopsy of a smoker |
Small Cell Carcinoma
-small cells mimic lymphocytes and degree of mitotic activity -nuclear molding pattern - cells round, oval, smooth and smushed up against each other |
|
|
|
Squamous Cell Carcinoma
Arise from? Histology? Associated mutations? Seen in? Location? Complications? |
-Arise from epithelial lining of bronchi -Histology: keratin pearls or intercellular bridges -p63+ & CK5/6 + on IHC -Mutations: highest p53 of all lung cancers, also RB and p16 -Association: most common tumor of male smokers -Location: Central -Complications: may produce PTHrP [can cavitate & cause hypercalcemia & hyponatremia]; poor prognosis; mets more common, esp. to adrenals |
Pneumonic: C's - central, cavitation, cigarettes, hyperCalcemia |
|
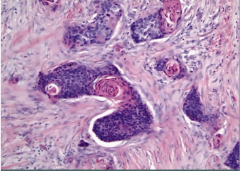
Lung Biopsy of a male smoker |
Squamous cell carcinoma
pink keratin pearls |
|
|
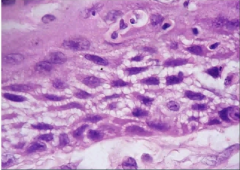
Lung Biopsy of a male smoker |
Squamous cell carcinoma
intercellular bridges - desmosomal connections between squamous cells >> being pulled apart from one another |
|
|
|
Adenocarcinoma
Arise from? Histology? Seen in? Location? Complications? Genetics? |
-Arise from mucus glands -Histology: glands or mucin; Ck7, TTF-1 + on IHC -Association: most common tumor in non smokers and female smokers (and overall) -Location: Peripheral -Complications: present with mets, often to the brain; paraneoplastics: Trousseau's, clubbing -Associated w/ EGFR mutations & EML-ALK4 fusion is specific to adenocarcinoma & aren't smoking dependent (KRas is a driver mutation) |
|
|
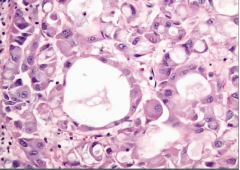
Lung Biopsy of a nonsmoker |
Adenocarcinoma
-tumor cells forming glandular space w/ mucin inside |
|
|
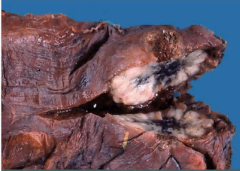
Lung |
Adenocarcinoma
tumor peripherally located up against the pleura |
|
|
|
Large Cell Carcinoma
Histology? Seen In? Location? |
-Histology: poorly differentiated large cells; pleomorphic -Association: smoking -Location: central or peripheral -Poor prognosis -Larger than SCLC, high mitotic rate, necrosis common |
|
|
|
Bronchioloalveolar Carcinoma
Arise from? Histology? Seen In? Location? Presentation? Prognosis? |
-Subtype of adenocarcinoma (minimally invasive) -Arise from: columnar cells that grow along preexisting bronchioles and alveoli & arises from Clara cells -Histology: picket fence arrangement over alveoli -Association: younger, women, nonsmokers -Location: Peripheral -May present with pneumonia-like consolidation (hazy infiltrates) on imaging -Excellent prognosis - may not need treatment |
|
|
Lung Biopsy |
Bronchioloalveolar Carcinoma
-normal alveolar air sacs on right -left: walls are replaced by tall columnar cells |
|
|
|
Common Sites of Lung Mets
Which cancers have the highest propensity? |
-adrenals, brain, bone (pathologic fracture), liver (hepatomegaly, jaundice) -Adenocarcinoma (80%) -Small Cell (95%) -Large Cell (80%) -Squamous Cell (>50%) |
|
|
|
Complications of Lung Cancer (Syndromes) |
-Superior vena cava syndrome (common in SCLC) -Pancoast tumor -Horner's Syndrome -Endocrine (paraneoplastic syndromes) -Recurrent laryngeal symptoms (hoarsness) -Effusions (pleural or pericardial) |
SPHERE of complications |
|
|
Carcinoid Tumor
Histology? Seen In? Location? Complications? |
-Histology: well-differentiated neuroendocrine cells (have granules) and are chromogranin A positive -bronchial carcinoid -Association: not related to smoking; most common in children/ young adult -Location: polyp like mass in bronchus (can be central or peripheral) -low-grade malignancy -can rarely cause carcinoid syndrome (5HT release >> flushing, diarrhea, wheezing) |
|
|
Lung |
Carcinoid Tumor
Polyp-like mass in bronchus |
|
|
Lung Biopsy |
Carcinoid Tumor
Nests of cells (characteristic of neuroendocrine cells); no mitosis, no necrosis |
|
|
Lung Biopsy w/ Special Stain |
Carcinoid Tumor
positive stain for chromogranin |
|
|
|
Metastasis to the Lung
Most common sources? Location? Commonality? What kind of tumor? |
-most common sources are breast, colon, bladder & prostate carcinoma -multiple cannon ball nodules on imaging; bilateral, peripheral -more common than primary tumors -Sarcoma |
|
|
|
Lung Cancer Staging, associated symptoms w/ spread & Survival |
-T - tumor size & local extension -Pleural involvement w/ adenocarcinoma [>>effusion] -SVC syndrome (distended head & neck veins w/ edema & blue discoloration of arms & face) -involvement of recurrent laryngeal (hoarseness) & phrenic (diaphragmatic paralysis) nerves -Compression of sympathetic chain >> Horner Syndrome (ptosis, miosis, anhidrosis); due to apical Pancoast tumor -N- spread to regional lymph nodes (1)hilar 2)mediastinal 3)contralateral) -M- unique site of metastasis = adrenal gland -survival: 15% 5 years survival rate due to late presentation b/c absence of screening |
|
|
|
Diagnosis Methods for Lung Cancer |
-sputum cytology - useless -CXR - PA & lateral; compare to previous -CT scan - more sensitive to CXR -PET scan - mets; useless in brain -MRI - for brain mets -Biopsy ---Bronchoscopy for dx and staging; central lesions ---CT guided biopsy for more invasive or peripheral lesions ---Mediastinoscopy for nodal staging ---VATs for excision of wedge ---open lung biopsy - invasive
|
|
|
|
Pneumothorax definition & presentation |
-accumulation of air in pleural space (between parietal and visceral pleural which are lined by mesothelial cells that produce fluid to lubricate) -presents w/ unilateral chest pain & dyspnea, unilateral chest expansion, decreased tactile fremitus, hyperresonance, and diminished breath on the affected side |
|
|
|
Spontaneous Pneumothorax |
-due to rupture of subpleural emphysematous bleb -seen in young adults (tall, thin males) -results in collapse of portion of the lung & trachea shift to side of collapse & diaphragm is up |
|
|
|
spontaneous pneumothorax
R lung collapsed |
|
|
|
Spontaneous pneumothorax Lung-physical findings |
-decreased breath sounds -hyperresonant to percussion -decreased tactile fremitus |
|
|
|
Tension Pneumothorax
What happens? How to treat? |
-arises w/ penetrating chest wall injury -air enters pleural space, but cannot exit >> positive pressure >> atelectasis due to compression -trachea is pushed to the opposite side of injury -MEDICAL EMERGENCY>> insert chest tube |
|
|
|
Tension pneumothorax Lung-physical findings |
-decreased breath sounds -hyperresonant to percussion -decreased tactile fremitus -tracheal deviation away from side of lesion |
|
|

|
Tension pneumothorax -hyperlucent left lung with low left hemidiaphragm and rightward mediastinal shift |
|
|
|
Mesothelioma
What is it? Histology? Associated with? Presntation? |
-malignant neoplasm of mesothelial cells -Psamomma bodies on histo; Ck 5/6 and calretinin + -highly associated with asbestos -presents w/ recurrent hemorrhagic pleural effusions, pleural thickening, dyspnea, chest pain -tumor encases the lung -median survival <12 mos |
|
|
Lung |
Mesothelioma
tumor encasing the lung |
|
|
What is it? Where is it? Complications? |
Pancoast Tumor -Carcinoma in the apex of the lung -Can affect cervical plexus >> Horner's Syndrome (ipsilateral ptosis, miosis, anhidrosis), SVC syndrome, hoarseness, and sensorimotor deficits |
|
|
|
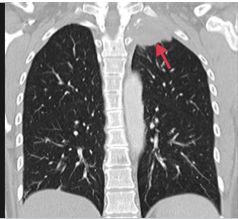
Resorption Atelectasis |
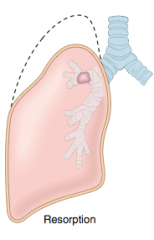
-obstruction prevents air from reaching distal airways >> air is trapped & slowly diffuses out of airways >> alveolar collapse |
|
|
|
Compression Atelectasis |
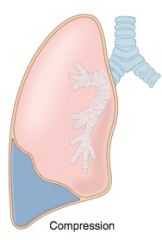
-accumulation of fluid, blood, or air in pleural cavity collapses adjacent lung -seen in pleural effusions -leakage of air can >> pneumothorax |
|
|
|
Contraction Atelectasis |
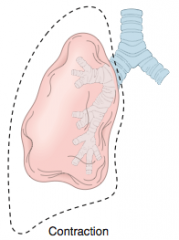
local/generalized fibrosis increases elastic recoil of the lung hampering expansion |
|
|
|
Patients w/ pneumonia (consolidation) and those w/ pneumothorax & pleural effusion all have decreased breath sounds... how do you distinguish them? |
Tactile fremitus -increased in consolidation of the long b/c sound is transmitted w/ less decay in fluid (fluid in alveloi helping to transmit sound) -Decreased in pleural effusion in pneumothorax b/c space between the alveoli & chest wall is diminshed (fluid outside alveoli blocking sound) |
|
|
|
TMN Staging [lecture] |
Tumor -T1: ≤ 3 cm -T2: >3cm -T3: locally advance >7 cm; sep. tumor nodules; same lobe -T4: mediastinal invasion; sep nodules; different lobes, same lung Nodal Involvement -N1: ipsilateral hilar -N2: ipsilateral mediastinal or subcarinal -N3: contralateral mediastinal/hilar or supraclavicuar/ scalen Metastases -M0- no mets -M1a- pleural or pericardial effusion and/or contralateral lung nodules -M1b - distant visceral disease |
|
|
|
Treatment of NSCLC [lecture] |
-Early Stage: surgery +/- adjuvant chemotherapy -Locally advancee: surgery + chemo; inoperable - chemoradiation -Distant Metastasis: palliative care |
|
|
|
Sequence of Lung Carcinoma Development
|
-3p mutation >> KRas >> TP53
-KRas + EGFR go hand in hand when EGFR found -EMK-ALK4 also seen |
|
|
|
anatomic dead space |
conducting zone: nose, pharynx, larynx, trachea, bronchi (large airways), bronchioles & terminal bronchioles (small airways) |
|
|
|
Role of conducting zones |
warms, humidifies, & filters air
do NOT participate in gas exchange |
|
|
|
Where are are cartilage & goblet cells located? |
extend to end of bronchi |
|
|
|
Histology & role of cells in conducting airways |
pseudostratified columnar cells (beat mucus up) extend to the beginning of the terminal bronchioles >> transition to cuboidal cells |
|
|
|
Where dos airway smooth muscle extend to? |
the end of the terminal bronchioles |
|
|
|
Lung parenchyma consists of and has what role? |
consists of respiratory bronchioles, alveolar ducts & alveoli
participates in gas exchange |
|
|
|
Histology of respiratory zone |
mostly cuboidal cells in respiratory bronchioles >> transitions to simple squamous up to alveoli
no cilia - debris removed by macrophages |
|
|
|
Type I pneumocytes |
-97% of of alveolar surfaces -line the alveoli -thin, squamous to participate in gas exchange |
|
|
|
Type II pneumocytes |
-secrete surfactant to decrease alveolar surface tension and prevent atelectasis -precursor (stem) cells to type I pneumocytes -involved in regeneration after lung damage -cuboidal and clustered -have lamellar bodies that produce the surfactant (on EM, look like onions) |
|
|
|
Club (Clara) cells |
-nonciliated -low columnar/cuboidal w/ secretory granules -secrete component of surfactant -degrade toxins -serve as reserve cells |
|
|
|
Law of Laplace? applies to what? |
Collapsing Pressure (P) = 2 surface tension (T)/ radius
alveoli have an increased tendency to collapse on expiration as radius decreases |
|
|
|
Surfactant made of? produced when? mature lungs when? how to test for mature lungs? |
-surfactant is a mix of lecithins; most imporitant is dipalmitoylphosphatidylcohline -synthesis begins in 26th week of gestation -lungs mature by week 35 -lecithin:sphingomyelin ratio > 2:1 in amniotic fluid = mature lungs |
|
|
|
Lobes? |
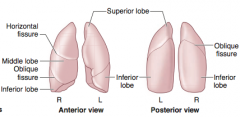
-Right has 3 lobes -left has 2 & lingula |
Left has Less Lobes |
|
|
More common site for Aspiration of a Foreign Body Why? Upright vs. Supine |
-R lung is more common site for foreign body aspiration b/c R main stem bronchus is wider & more vertical -Aspiration of a Peanut: Upright = lower portion of R inferior lobe; Supine - superior portion of R superior lobe |
|
|
|
Relationship of pulmonary artery to bronchi at each hilum |
Right - anterior Left- superior |
RALS |
|
|
Structures perforating diaphragm and where |
T8: IVC T10: esophagus, vagus (CN10) T12: aortic hiatus (aorta, thoracic duct, azygous vein) |
I ate 10 eggs at 12
at T-1-2 it's red white & blue |
|
|
Diaphragm innervation referred pain? |
-Phrenic nerve (C3,4,5) -pain referred to shounder (C5) & trapezius ridge (C3 & 4) |
C3,4,5 keeps the diaphragm alive |
|
|
Inspiratory Reserve Volume |
-IRV -amount of air that can be inspired after a normal inspiration -about 3 L |
|
|
|
Tidal Volume |
-TV -air that moves into the lung in normal inspiration -500 mL |
|
|
|
Expiratory Reserve Volume |
-ERV -air that can be expired after normal expiration -about 1 L |
|
|
|
Residual Volume |
-RV -air in lung after maximal expiration -cannot be measure with spirometry -1.2 L |
|
|
|
Inspiratory capacity |
-IC -IRV + TV |
|
|
|
Functional Residual Capacity |
-FRC -ERV + RV -volume in lungs after normal expiration |
|
|
|
Vital Capacity |
-TV + IRV + ERV -maximum volume of gas that can be expired after maximal expiration |
birthday breath |
|
|
Total Lung Capacity |
-TLC -RV + ERV + TV + IRV -volume of gas in lungs after maximal inspriation |
|
|
|
Determining Physiological Dead Space |
Vd = Vt x (PaCO2 - PeCO2/PaCO2) |
|
|
|
What is physiological dead space? |
-anatomic dead space + physiological dead space in alveoli -volume of inspired air that doesn't participate in gas exchange |
|
|
|
Largest contributor to physiological dead space? |
apex of the lung |
|
|
|
Minute ventilation |
-Ve -total volume of gas entering the lungs per minute -Ve = Vt x RR |
|
|
|
Alveolar Ventilation |
-VA -volume of gas per unit time that reaches the alveoli -VA = (Vt - Vd) x RR |
|
|
|
When is the lung & chest wall system at atmospheric pressure? |
-@ FRC -chest wall tendency to spring out = lung tendency to collapse |
|
|
|
[Indication for O2 Therapy - Medicare] |
-PaO2 ≤ 55 mmHg -SaO2 ≤ 88% -PaO2 55-60 mmHg or SaO2 89% w/ evidence of pulmonary HTN, peripheral edema suggesting CHF, or polycythemia (Hct 55%) |
|
|
|
What determines lung/chest wall volume? |
elasticity |
|
|
|
At FRC, what is the pressure? |
-0 cmH2O -intrapleural pressure is negative (preventing pneumothorax) -PVR is at a minimum |
|
|
|
What prevents pneumothorax? |
negative intrapleural pressure |
|
|
|
What is compliance & what causes it to change? |
-change in lung volume for a given change in pressure (change in volume/change in pressure) -decreased in pulmonary fibrosis, pnuemonia, pulmonary edema -increased in emphysema and normal aging |
|
|
|
Hemoglobin is composed of what & exists in what forms? |
-composed of 2 alpha & 2 beta subunits -exists in T (taut) form which has low affinity for O2 & in R (relaxed) form which has high (300x) affinity for O2 -Hb exhibits positive cooperativity & negative allostery
|
Taut in Tissues Relaxed in Respiratory Tract |
|
|
Fetal Hemoglobin Composed of? Affinities? |
-composed of 2 alpha and 2 gamma subunits -lower affinity for 2,3 BPG >> higher affinity for O2 >> shifts dissociation curve left |
|
|
|
What shifts O2 association curve & where? |
-increased H+, 2,3-BPG, CO2, temperature, altitude, Cl causes, exercise, transition from relaxed to taut >> curve shifts right >> facilitates unloading of oxygen to tissues |
BAT ACE |
|
|
Problems with Hb cause what? |
tissue hypoxia from decreased O2 saturation and content |
|
|
|
What is methemoglobin & how does it differ from the normal? |
-Methemoglobin = oxidized for of Hb (ferric, Fe3+) that does not bind oxygen as readily & has increased affinity for cyanide -Hb normally must be reduced (ferrous, Fe2+) to bind O2 |
|
|
|
Treatment of Methemoglobinemia |
methylene blue |
|
|
|
How do nitrites affect us? |
-poison by oxidizing Fe2+ in Hb to Fe3+ |
|
|
|
Presentation of Methemoglobinemia |
cyanosis & chocolate-colored blood |
|
|
|
Treatment of cyanide poisoning? |
Use nitrites to to oxidize Hb to methemoglobin to bind cyanide.
Then use thiosulfate to bind this cyanide production thiocyanide that is excreted in the urine |
|
|
|
Carboxyhemoglobin What does it cause? |
-form of Hb bound to CO in place of O2 -CO has 200x affinity for Hb -causes decreased O2 binding capacity with a left shift in the O2 dissociation curve >> decreased unloading of O2 to tissues |
|
|
|
What causes the sigmoidal shape of the O2-Hb dissociation curve? |
-positive cooperativity - Hb has higher affinity for O2 for each subsequent O2 molecule bound (up to 4) |
|
|
|
O2 content of blood |
=(O2 binding capacity x saturation) + dissolved O2 |
|
|
|
Normally __ g Hb can bind ___ mL O2 |
1g Hb can bind 1.34 mL of O2 |
|
|
|
Normal amount of Hg in the blood
At what value are what affects seen? |
15 g/dL
>5 g/dL of deoxygenated Hb >> cyanosis |
|
|
|
Normal O2 binding capacity |
20.1 mL O2/dL |
|
|
|
What occurs when Hb falls? |
O2 content of blood falls, but O2 saturation & PO2 don't |
|
|
|
Oxygen delivery |
cardiac output x O2 content |
equation |
|
|
CO poisoning - describe lab values that would be seen |
Normal Hb decreased O2 saturation normal dissolved O2 (PaO2) decreased total O2 content |
|
|
|
Anemia - describe lab values seen |
decreased Hb normal O2 saturation normal dissolved O2 (PaO2) decreased total O2 content |
|
|
|
Polycythemia |
increased Hb normal O2 content normal dissolved O2 (PaO2) increased total O2 content |
|
|
|
Pulmonary circulation is usually a ___ resistance ____ compliance system. |
-low resistance, high compliance |
|
|
|
PO2 & PCO2 exert ___ effects on pulmonary & systemic circulation. What are they? |
-PO2 & PCO2 exert opposit effects on pulmonary & systemic ciculation -In pulmonary, a decrease in PAO2 >> hypoxic vasocontriction to divert blood from poorly ventilated regions to well-ventilated regions |
|
|
|
Perfusion Limited |
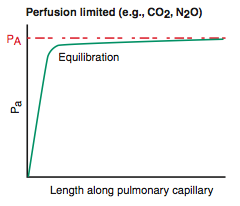
-O2 (normal health), CO2, N2O -gas equilibrates early along the length of the capillary -diffusion can only be increased if perfusion is increased |
|
|
|
Diffusion Limited
|
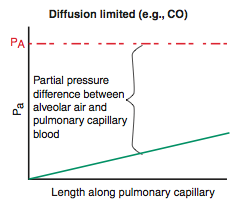
-O2 (emphysema & fibrosis), CO
-gas does not equilibrate by the time blood reaches the end of the capillary |
|
|
|
Pulmonary Vascular Resistance
(equations) |
PVR = (Ppulm art - P left atrium) / CO
P left atrium = PCWP
b/c delta P = Q x R, so R = delta P/Q
R = 8nl/pi r^4 |
|
|
|
Alveolar Gas Equation |
PAO2 = PIO2 - (PaCO2 / R)
R = respiratory quotient = CO2 produced / O2 consumed
PAO2 = 150 - (PaCO2 / 0.8) |
|
|
|
A-a gradient
What does an abnormal gradient mean & what causes it? |
PAO2 - PaO2 = 10-15 mmHg
an increased A-a gradient can be seen in hypoxemia
causes include V/Q mismatch, shunting, fibrosis (impairs diffusion) |
|
|
|
A-a gradient [broken down form lecture]
equations and values |
PAO2 = PIO2 - PaCO2/0.8 PAO2 = (PB - PH2O) x FiO2 - PaCO2/0.8 PAO2 = (760 - 47) x 0.21 - PaCO2/0.8 PAO2 = 150 - PaCO2/0.8 |
|
|
|
Normal AaDO2 according to age [lecture] |
normal A-a gradient = (age/4) + 4 |
|
|
|
AaDO2 equation [lecture] |
AaDO2 = 150 - PaCO2/0.8 - PaO2 (sea level) |
|
|
|
Hypoxemia
Definition? Causes & A-a gradient seen |
Def: decreased PaO2
Normal A-a gradient in high altitude and hypoventilation
Increased A-a gradient: V/Q mismatch, diffusion limitations, R >> L shunt, shunt (not corrected with O2), decreased SVO2 (hypermetabolism, anemia, decreased CO) |
|
|
|
Examining Low PaO2 |
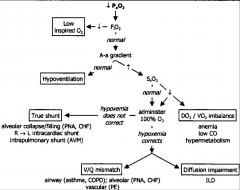
-if A-a > 30 mmHg (or just high), the problem is in the lungs (problem in V, Q or or diffusion) -if A-a normal, then something outside the lungs is causing hypoxemia; respiratory acidosis will also be present |
|
|
|
What are causes of respiratory acidosis? |
COPD, depression of respiratory center (obstruction like epiglottis, larygotracheobronchitis, cafe coronary (paralyzed resp. muscles), ALS, GBS, paralysis of the diaphragm, barbituates)
normal A-a gradient |
|
|
|
Hypoxia
causes? |
Def: decreased O2 delivery to tissue
Causes hypoxemia, decreased cardiac output, anemia, carbon monoxide poisoning |
|
|
|
Ischemia |
loss of blood flow caused by impeded arterial flow or decreased venous drainage |
|
|
|
Lung Zones V/Q |
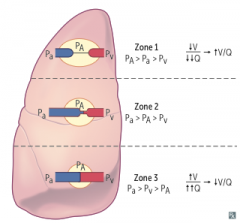
-Apex: V/Q = 3 (wasted ventilation); intraplerual pressure most negative -Base: V/Q = 0.6 (wasted perfusion); intrapleural pressure least negative -Both ventilation & perfusion are greater at the base of the lung than the apex |
|
|
|
V/Q in exercise & why |
-approaches 1 b/c increased cardiac output >> vasodilation of apical capillaries |
|
|
|
V/Q >> 0 |
airway obstruction = shunt
O2 will not help |
|
|
|
V/Q >> infinity |
blood flow obstruction (physiologic dead space)
<100% dead space >> O2 supplementation will help |
|
|
|
CO2 is transported in what forms |
-HCO3- (90%) -Carbaminohemoglobin/HbCO2 (5%): bound to N-terminus of globin (NOT heme) >> T configuarion >> unloading of O2 -Dissolved CO2 (5%)
|
|
|
|
Haldene Effect |
In the lungs, oxygenation of Hb promotes dissociation of H+ from Hb >> CO2 formation & release from RBCs |
|
|
|
Bohr Effect |
In tissues, increased H+ shifts the curve right >> unloading of O2 |
|
|
|
CO2 transport/HCO3- formation |
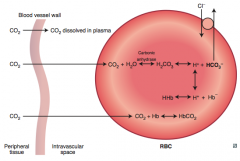
CO2 diffuse out of vessel into RBC >> combines with H2O >> carbonic anhydrase forms H2CO3 >> dissociaties to H+ & HCO3- >> HCO3- exchanged for Cl- & H+ combines w/ Hb forming HHb |
|
|
|
Response to High Altitude |
-decreased atomspheric O2 >> decreased PaO2 >> increased ventilation >> decreased PaCO2 -chronic increased ventilation -increased RPO >> increased Hct & Hb (chronic hypoxia) -increased 2,3 BPG >> binds Hb to release more O2 -cellular changes (increased mitochondria) -increased renal excretion of HCO3- due to respiratory alkalosis (can augment w/ acetazolamide) -chronic hypoxic vasoconstriction >> RV hypertrophy
|
|
|
|
Response to exercise |
-increased CO2 production -increased O2 consumption -increased ventilation rate to meet O2 demand -more uniform V/Q throughout lung -increased pulmonary blood flow due to increased cardiac output -decreased pH (secondary lactic acidosis) -No change in PaO2 or PaCO2, but an increase venous CO2 and decrease in venous O2 |
|
|
|
Rhinosinusitis
What is it? Cause? |
-obstruction of sinus drainage into nasal cavity >> inflammation & pain over affected area (most commonly maxiallary sinus pain in adults) -Most common cause is viral URI; can cause secondary bacterial infection (S. aureuas, H. flu, M. catarrhalis) |
|
|
|
Deep Venous Thrombosis
Risk? Presentation? Complication? Treatment? |
-Predisposed by Virchow's Triad: stasis, hypercoagulability (Factor V Leiden), endothelial damage -95% of PEs from DVTs -Homan sign: dorsiflexion of foot >> calf pain -Treatment: Heparin for prevention & acute management; Warfarin for long term prevention of DVT recurrence
|
|
|
|
Most common site from which embolization to the lungs comes from? |
Femoral vein |
|
|
|
Pulmonary Emboli Causes/Types & Complications |
-Fat, Air, Thrombus, Bacteria, Amniotic Fluid, Tumor -Fat embolus associated with long bone fractures and liposuction; triad: hypoxemia, neurological abnormalities, petechial rash -Amniotic embolus - can cause DIC; postpartum -Gas: nitrogen bubbles precipitate ascending divers; treat w/ hyperbaric oxygen |
Embolus moves like a FAT BAT |
|
|
Clinical Features of Pulmonary Embolism
what types of thromboembolism (size) and their associated complication/prentation? |
-most are silent b/c they are small -5% - when >60% of pulmonary vasculature is occluded >> acute cor pulmonale, sudden death, CV shock -10-15% - when small to medium sized arteries are blocked but underlying arterial insufficiency >> infarction >> present w/ dyspnea -chronic small emboli >> pulmonary HTN >> chronic cor pulmonale >> pulmonary vascular sclerosis >> worsening edema -patients who have had 1 PE have a 30% chance of having another |
|
|
|
Pulmonary Embolus Pathogenesis, Presentation, Work-Up |
-Pathogenesis: V/Q mismatch >> hypoxemia >> respiratory alkolosis -Presentation: sudden onset of dyspnea, chest pain, tachypnea; possibly sudden death -V/Q scan first; CT pulmonary angiography perfered imaging method (confirmatory)
|
|
|
|
Lines of Zahn are interdigitating arease of pink (platelets, fibrin) and red (RBCs) found only in thrombi formed before death. Helps distinguish pre- and postmoretem thrombi |
|
|
|
Consequences of Embolic Pulmonary Embolism (Sequelae) |
(1) increase in pulmonary artery pressure (blockage of flow or vasospasm) (2) ischemia of downstream parenchyma >> infarction/coagulative necrosis (usually occurs w/ underlying CV disease like HF) -these lead to increase pulmonary artery pressure >> decreased CO >> R sided HF >> hypoxemia due to -perfusion of atelecatic lung zones -low CO widen arterial-venous O2 sat dif. -R>>L cardiac shunting (congenital) |
|
|
|
Sleep Apnea
Features? Manifestations? Treatment? |
-Repeated cessation of breathing for >10 sec. during sleep >> daytime somnolence -Normal PaO2 during the day -Nocturnal hypoxia >> pulmonary/systemic hypertension, arrhythmias (atrial fibrillation/ flutter), and sudden death -Hypoxia >> EPO release >> increased erythropoiesis -Treatment: weight loss, CPAP, surgery |
|
|
|
Types of Sleep Apnea (3) |
-Central sleep apnea - no respiratory effort -Obstructive sleep apnea - respiratory effort against airway obstruction; associated with obesity & loud snoring -Obesity hypoventilation syndrome: obesity (BMI≥30) >> hypoventilation >> decreased PaO2 & increased PaCO2 during waking hours |
|
|
|
Pleural effusion Lung-physical findings |
-decreased breaths sounds -dull to percussion -decreased tactile fremitus |
|
|
|
Atelectasis (bronchial obstruction) Lung-physical findings |
-decreased breath sounds -dull to percussion -decreased tactile fremitus -tracheal deviation towards side of lesion |
|
|
|
Consolidation Lung-physical findings & causes |
-Causes: lobar pneumonia, pulmonary edema -bronchial breath sounds & late inspiratory crackles -dull to percussion -increased tactile fremitus |
|
|
|
Horner's Syndrome |
ipsilateral ptosis, miosis, & anhydrosis due to compression of the cervical sympathetic chain |
|
|
|
Superior Vena Cava Syndrome
What is it? Symptoms? Causes? Complications? |
-obstruction of SVC impairs drainage from head ("facial plethora"), neck (JVD), and upper extremities (edema) -commonly caused by malignancy and thrombosis of indwelling catheters -MEDICAL EMERGENCY -can raise ICP if obtsruction severe >> dizziness, headaches, and increased risk of aneurysm/rupture of intracranial arteries |
|
|
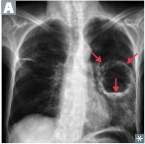
What is it? Mechanism? Seen in? Causes
|
Lung abscess - air-fluid levels on CXR -localized collection of puss in the parenchyma -Caused by bronchial obstruction (cancer), or aspiration or oropharyngeal contents (seen in alcoholics, epileptics, diabetics due to DKA) -Often due to S. aureus or anaerobes (Bacteroides, Fusobacterium, Peptostreptococcus) |
|
|
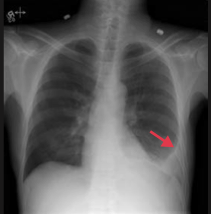
Definition and Complication |
Pleural Effusion - blunting of costophrenic angle -excess fluid accumulation between parietal and visceral pleura -causes restricted lung expansion during inspiration |
|
|
|
Transudate pleural effusion
definition? Causes? |
-decreased protein content (<0.5 of serum protein) -<0.6 serum LDH -<2/3 upper limit of normal serum LDH -Due to CHF, nephrotic syndrome, or hepatic cirrhosis |
|
|
|
Exudate pleural effusion
definition? Causes? Treatment |
-increased protein content (>0.5 of serum protein) ->0.6 of serum LDH ->2/3 upper limit of normal serum LDH -Due to malignancy, pneumonia, collagen vascular disease, trauma (states of increased vascular permeability) -very low glucose seen - think RA -Must be drained due to risk of infection |
|
|
|
Chylothorax |
-due to thoracic duct injury from trauma or malignancy -milky-appearing fluid high in triglycerides |
|
|
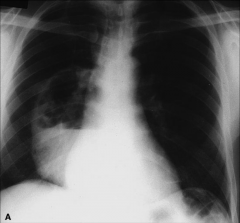
What is it?
Most likely cause? |
Lung abscess - notice the air fluid level (seen if communicates with bronchus)
Most likely due to Staph aureus |
|
|
|
Diphenhydramine, dimenhydrinate, chlorpheniramine |
-1st generation H1 blocker: contain -en/-ine or -en/-ate -reversible inhibitors of H1 receptors -Use: motion sickness, allergy, sleep aid -Toxicity: Sedation, anticholinergic, anti-alpha-adrenergic
|
|
|
|
Loratadine, Fexofenadine, Desloratadine, Cetirizine |
-2nd generation H1 blocker: end in -adine -reversible inhibitors of H1 receptors -Use: allergy -Toxicity: Far less sedation than 1st generation due to decreased entry to CNS |
|
|
|
Guaifenesin |
-Expectorant - thins respiratory secretions; does not suppress cough reflex |
|
|
|
N-acetylcysteine |
-Expectorant -Mucolytic - can looks mucus plugs in CF patients -Used as antidote for acetominophen overdose |
|
|
|
Dextromethorphan |
-Expectorant -Antitussive (antagonizes NMDA glutamate receptors) -Synthetic codeine analog - has mild opioid effect when used in excess -Nalozone can be given for overdose -Mild abuse potential |
|
|
|
Pseudophedrine, phenylephrine |
-MOA: Sympathomimetic alpha-agonistic non-prescription nasal decongestants -Use: Reduce hyperemia, edema, and nasal congestion; open obstructed eustachian tubes -Can be used illicitly to make methamphetamines -Toxicity: HTN; can cause CNS stimulation/anxiety (pseudophedrine) |
|
|
|
Asthma drugs
Focus on? |
Bronchocontriction is mediated by inflammation and parasympathetic tone: drugs aimed at this |
|
|
|
Albuterol |
-B2 agonist -Use: asthma - acute exacerbation -MOA: Relaxes bronchial smooth muscle by binding B2 receptors [Adverse Effects: tachycardia, tremor, arryhthmia, hypokalemia] |
|
|
|
Salmeterol, Formoterol |
-B2 agonist -Use: asthma - long-acting for prophylaxis -Adverse Effects: tremor and arrhythmia |
|
|
|
Methylxanthines |
-Theophylline - likely causes bronchodilation by inhibiting phosphodiesterases >> increased cAMP levels b/c of decreased hydrolysis -Usage limited b/c of narrow therapeutic index (cardiotoxicity, neurotoxicity) -Metabolized by CYP-450 -Blocks effects of adenosine |
|
|
|
Ipratropium |
-Muscarinic antagonist -Use: asthma & COPD -competitively blocks muscarinic receptors preventing bronchoconstriction [-blocks cough reflex] |
|
|
|
Tiotropium |
-Muscarinic antagonist -long acting -competitively blocks muscarinic receptors preventing bronchoconstriction -Used for COPD (& asthma) [-blocks cough reflex] |
|
|
|
Beclothemasone, Fluticasone |
-corticosteroids -Use: 1st line therapy for chronic asthma -MOA: inhibits the synthesis of virtually all cytokines; inactivates NFkB, the transcription factor that induces the production of TNF-alpha and other inflammatory agents [-Adverse Effects: pneumonia, oral candidiasis, hoarseness, HPA-axis supression, easy bruising, osteoporosis, growth suppression] |
|
|
|
Omalizumab |
-Use: allergic asthma resistant to steroids and long-acting B2 agonists -MOA: monoclonal anti-IgE antibody; binds mostly unbound serum IgE & blocks binding to FcERI |
|
|
|
Methacholine |
-muscarinic receptor agonist -Use: bronchial provocation challenge for diagnosis of asthma |
|
|
|
Bosentan |
-Use: pulmonary arterial hypertension -MOA: competitively antagonizes endothelin-1 receptors >> decreases pulmonary vascular resistance |
|
|
|
Goodpasture Syndrome |
-Type II hypersensitivity antibodies to GBM and alveolar BM >> linear IF -Present with hemoptysis and hematura (due to necrotizing glomerulernephritis) |
|
|
|
Diagnosis of Inhaled Anthrax |
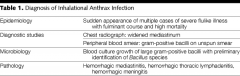
|
|
|
|
Aspiration of foreign objective
Where does it go? |
Sitting/standing = posterobasal segment of right lower lobe Back: superior segment of right lower lobe |
|
|
|
Most common cause of lung abscess? |
MCC abscess = aspiration of oropharyngeal material |
|