Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
44 Cards in this Set
- Front
- Back
|
How can you distinguish respiratory vs metabolic disorders?
|

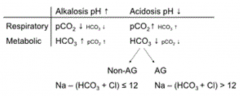
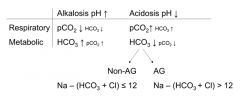
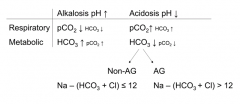
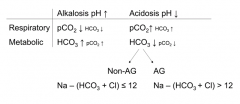
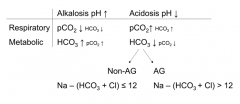
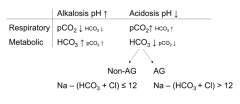
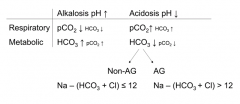
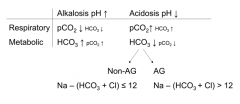
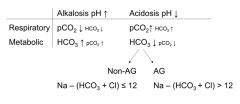
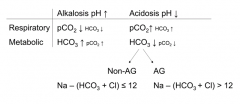
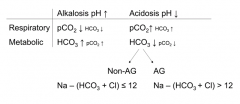
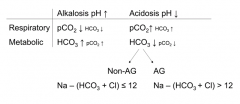
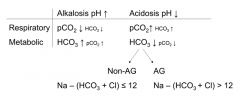
- Respiratory: first a change in pCO2 (later a compensation by HCO3), arrows opposite direction as pH
- Metabolic: first a change in HCO3 (later a compensation by pCO2), arrows same direction as pH |
|
|
What are the features of respiratory alkalosis?
|

pH ↑
pCO2 ↓ → (HCO3 ↓) |
|
|
What are the features of respiratory acidosis?
|

pH ↓
pCO2 ↑ → (HCO3 ↑) |
|
|
What are the features of metabolic alkalosis?
|

pH ↑
HCO3 ↑ → (pCO2 ↑) |
|
|
What are the features of metabolic acidosis?
|

pH ↓
HCO3 ↓ → (pCO2 ↓) |
|
|
Which of the major acid-base disorders is associated with an anion gap?
|
Metabolic Acidosis
pH ↓ HCO3 ↓ → (pCO2 ↓) |
|
|
How do you determine the anion gap?
|
Na - (HCO3 + Cl)
Non-Anion Gap: ≤ 12 Anion Gap: > 12 |
|
|
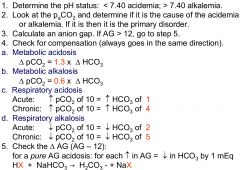
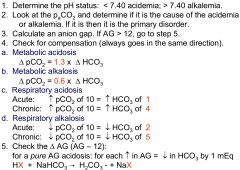
How should you approach determining the acid-base disorder?
|
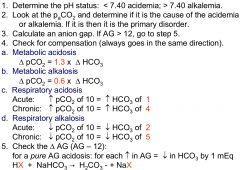
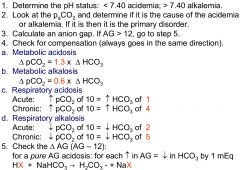
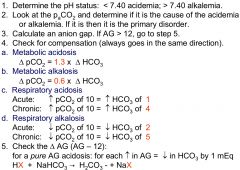
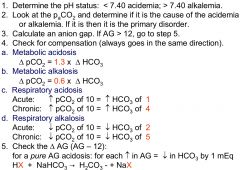
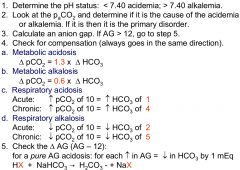
1. Determine pH
2. Look at pCO2 to determine if it cause of disorder 3. Calculate anion gap (if AG > 12, go to step 5 4. Check for compensation (goes in same direction) 5. Check ΔAG (AG - 12) |
|
|
How can you check for compensation in Metabolic Acidosis?
|
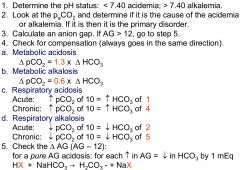
ΔpCO2 = 1.3 x ΔHCO3
|
|
|
How can you check for compensation in Metabolic Alkalosis?
|
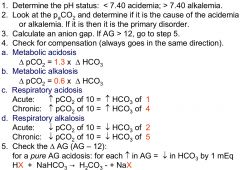
ΔpCO2 = 0.6 x ΔHCO3
|
|
|
How can you check for compensation in Respiratory Acidosis?
|
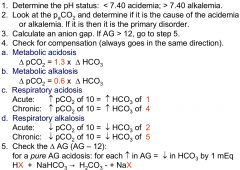
- Acute: ↑ pCO2 of 10 = ↑ HCO3 of 1
- Chronic: ↑ pCO2 of 10 = ↑ HCO3 of 4 |
|
|
How can you check for compensation in Respiratory Alkalosis?
|
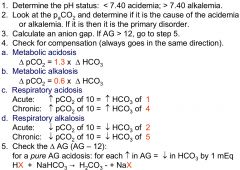
- Acute: ↓ pCO2 of 10 = ↓ HCO3 of 2
- Chronic: ↓ pCO2 of 10 = ↓ HCO3 of 5 |
|
|
How do you assess for a pure AG metabolic acidosis?
|
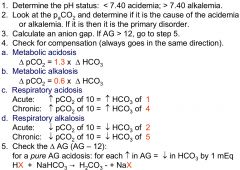
For each ↑ in AG = ↓ HCO3 by 1 mEq
HX + NaHCO3 → H2CO3 + NaX |
|
|
When assessing for compensation, what should you compare to?
|
Compare to the expected value, not the normal values
|
|
|
How many Arterial Blood Gas (ABG) measurements do you need?
|
Need serial measurements (one is only a snapshot in time)
|
|
|
In what direction does respiratory compensation go for a primary metabolic disorder?
|
Same direction
|
|
|
In what direction does metabolic compensation go for a primary respiratory disorder?
|
Same direction
|
|
|
What does compensation mean for pH?
|
pH comes closer towards normal than without compensation, but pH NEVER quite reaches 7.40
|
|
|
What does it tell if you pCO2 and HCO3 are deranged but the pH is normal?
|
There are at least two simultaneous disorders (that are making pCO2 and HCO3 off, but averaging to normal pH)
|
|
|
How long does it take for respiratory compensation?
|
Almost instantaneous
|
|
|
How long does it take for metabolic compensation?
|
Takes several hours
|
|
|
What do you always need when doing an Arterial Blood Gas (ABG) analysis?
|
Basic Metabolic Panel (BMP)
|
|
|
What use is a BMP for assessing an acid base disorder?
|
It may reveal an acid base disorder without an ABG
|
|
|
In the case of a pure (i.e. no other acid-base disorder) compensated metabolic alkalosis, what changes in pH, pCO2, and HCO3 do you expect?
|
- pH: ↑
- pCO2: ↑ - HCO3: ↑ |
|
|
What are the normal values for HCO3 and pCO2?
|
- HCO3: ~24 (22-26 mEq/L)
- pCO2: ~40 (35-45 mmHg) |
|
|
Your patient has the following arterial blood gas results; what is your diagnosis?
pH: 7.62 pCO2: 20 HCO3: 20 |
Respiratory Alkalosis
|
|
|
A 38 kg 85-yo demented woman is intubated. The ventilaor is set at a rate of 12, tidal volume of 200 cc, FiO2 is reduced to 30%. What is your diagnosis based on the following ABG results?
pH: 7.40 pCO2: 60 pO2: 52 HCO3: 36 |
Respiratory Acidosis &
Metabolic Alkalosis (know there are 2 disorders because the pH is normal but there is an elevation of both pCO2 and HCO3) |
|
|
31 yo woman undergoes an uneventful open cholecystectomy under general anesthesia. In recovery room she appears to be taking fast and shallow breaths. Her ABG shows:
pH: 7.32 pCO2: 50 HCO3: 25 Diagnosis? How do you check for compensation? |
Respiratory Acidosis
(**acute compensation: ↑pCO2 of 10 = ↑HCO3 of 1) (chronic compensation: ↑pCO2 of 10 = ↑HCO3 of 4) |
|
|
31 yo woman undergoes an uneventful open cholecystectomy under general anesthesia. In recovery room she appears to be taking fast and shallow breaths. Her ABG shows:
pH: 7.32 pCO2: 50 HCO3: 25 What is the most likely reason for her disturbance? |
Hypoventilation (trying to breath but not getting much O2 exchange in lungs since they are shallow) →
Respiratory Acidosis (acute compensation) |
|
|
Patient is a smoker of 15-pack years and diagnosed w/ COPD and her pre-opeartive ABG is
pH: 7.37 pCO2: 50 HCO3: 28 What is your diagnosis? |
Respiratory Acidosis
(acute compensation: ↑pCO2 of 10 = ↑HCO3 of 1) (**chronic compensation: ↑pCO2 of 10 = ↑HCO3 of 4) |
|
|
31 yo woman undergoes an uneventful open cholecystectomy under general anesthesia. In recovery room she appears to be taking fast and shallow breaths. What if NOW her ABG shows:
pH: 7.40 pCO2: 50 HCO3: 30 What is the most likely reason for her disturbance? |
Respiratory Acidosis &
Metabolic Alkalosis |
|
|
What combination of disorders do you have if pH is 7.4 and pCO2 and HCO3 are elevated?
|
Respiratory Acidosis &
Metabolic Alkalosis |
|
|
What combination of disorders do you have if pH is 7.4 and pCO2 and HCO3 are depressed?
|
Respiratory Alkalosis &
Metabolic Acidosis |
|
|
A 49 yo man is diagnosed w/ a perforated ulcer and has been vomiting (ie losing HCL) for 2 days.
What is his most likely acid-base disturbance, purely based on clinical picture? |
Metabolic Alkalosis
(he is vomiting up H+, which makes it an alkalosis and it is not caused by his breathing, so it is a metabolic problem) |
|
|
A 49 yo man is diagnosed w/ a perforated ulcer and has been vomiting (ie losing HCL) for 2 days.
His arterial HCO3 is 36, pH 7.40. What kind of acid-base disturbance? |
Metabolic Acidosis &
Respiratory Alkalosis |
|
|
A 49 yo man is diagnosed w/ a perforated ulcer and has been vomiting (ie losing HCL) for 2 days.
His arterial HCO3 is 36, pH 7.40. What is his expected pCO2 in mmHg? |
HCO3 increased factor of 1.5 (24 → 36)
pCO2 should increase by 1.5 (40 → 60 mmHg) |
|
|
A 49 yo man is diagnosed w/ a perforated ulcer and has been vomiting (ie losing HCL) for 2 days.
If the Metabolic Alkalosis is fully compensated, what would his ABG look like? |
pH: ↑
pCO2: ↑ HCO3: ↑ (remember: ΔpCO2 = 0.6 * ΔHCO3) |
|
|
A 49 yo man is diagnosed w/ a perforated ulcer and has been vomiting (ie losing HCL) for 2 days.
What IV crystalloid fluid would you give this patient peri-operatively? - Normal saline (Cl- 154) - Ringer's lactate (Cl- 109) - 5% dextrose in water - 8.4% sodium bicarbonate - Plasmalyte (Cl- 98) |
Normal Saline (Cl- 154) because you want to replace all of the lost Cl- (vomiting up HCl)
|
|
|
A 40 yo male comes to ED w/ a 1-day hx of diarrhea after having had dinner in a local fast food restaurant.
What is his most likely ABG disturbance if he is otherwise healthy? |
Metabolic Acidosis
|
|
|
A 40 yo male comes to ED w/ a 1-day hx of diarrhea after having had dinner in a local fast food restaurant.
His HCO3 is 10. What do you expect his pH and pCO2 to be if he is fully compensated? |
Metabolic Acidosis
pH: ↓ ΔpCO2 = 1.3 * ΔHCO3 = 1.3 * (10 - 24) = 1.3 * -14 ΔpCO2 = -18.2 pCO2 - 40 = -18.2 pCO2 = 21.8 |
|
|
A 40 yo male comes to ED w/ a 1-day hx of diarrhea after having had dinner in a local fast food restaurant.
What IV crystalloid fluid would you give this patient? - Normal saline (Cl- 154) - Ringer's lactate (Cl- 109) - 5% dextrose in water - 8.4% sodium bicarbonate - Plasmalyte (Cl- 98) |
Ringer's Lactate (Cl- 109)
(isotonic loss of Cl- in diarrhea, so just need to restore fluids) |
|
|
An unconscious 20 yo female, 70 kg, is brought to ED. To protect her airway she is intubated and mechanically ventilated w/ tidal volume 500 cc, rate 14, FiO2 50%.
Lab results: pH: 7.40 pCO2: 40 HCO3: 24 Na 146 Cl 105 What is her acid-base disturbance? |
AG: Na - (HCO3 + Cl)
= 146 - 24 - 105 = 17 AG > 12 = AG Metabolic Acidosis |
|
|
An unconscious 20 yo female, 70 kg, is brought to ED. To protect her airway she is intubated and mechanically ventilated w/ tidal volume 500 cc, rate 14, FiO2 50%.
Lab results: pH: 7.30 pCO2: 40 HCO3: 19 Na 146 Cl 110 What acid-base disturbances does this patient have? |
- First AG Metabolic Acidosis (AG = 17)
- In addition, Respiratory Acidosis |
|
|
An unconscious 20 yo female, 70 kg, is brought to ED. To protect her airway she is intubated and mechanically ventilated w/ tidal volume 500 cc, rate 14, FiO2 50%.
Lab results: pH: 7.30 pCO2: 40 HCO3: 19 Na 146 Cl 110 Glucose 392 Based on these lab results, what medical problem does this patient likely have? |
Diabetic Ketoacidosis
|