Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
117 Cards in this Set
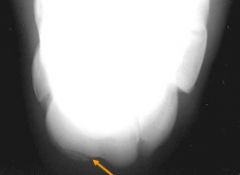
- Front
- Back

|
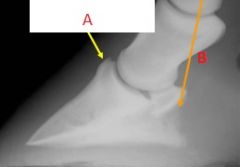
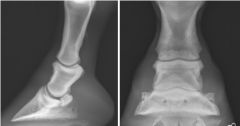
-A: Vascular channels
-B: Palmar process |
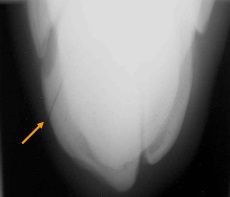
|
|
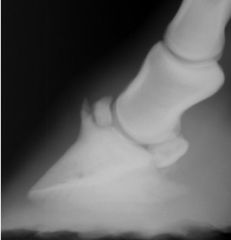
-A: Extensor process
-B: Palmar process |
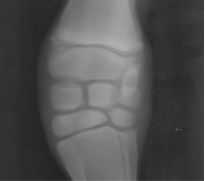
|
|
Diseases of the Pedal Bone
|
-Fractures
-Laminitis -Pedal Osteitis (infectious/non-infectious) |
|
|
Pedal Bone
-Type I Fracture |
-non-articular palmar process
|
|
|
Pedal Bone
-Type II Fracture |
-axially located
-intra-articular |
|
|
Pedal bone
-Type III Fracture |
-midline sagittal fracture
|
|
|
Pedal Bone
-Type IV Fracture |
-Extensor Process
|
|
|
Pedal Bone
-Type V Fracture |
-Comminuted Fracture
|
|
|
Pedal Bone
-Type VI Fracture |
-Solar Margin Fracture
|
|
|
Pedal Bone
-Type VII Fracture |
-Palmar process fractures in foals
|
|

Name the Fractures
|
-A: Type I
-B: Type II -C: Type III -D: Type IV |
|
|
Why might Type VI fractures of P3 be missed on a radiograph?
|
-if the radiograph is overexposed the solar margin may be burned out
|
|
|
Type VI P3 Fractures
-Common Causes |
-Pedal Osteitis
-Laminitis |
|
Name the Fracture Type
|
-Type IV
|
|

Name the Fracture Type
-presenting condition |
-Type VII
-Foal Bilateral Forelimb lameness |
|
|
What may an osseous fragment at the extensor process of P3 represent?
|
-acute or chronic fracture (Type IV)
-a separate center of ossification -mineralization within the extensor tendon -normal variation |
|
|
Why is radiographic followup of a P3 fracture challenging?
|
-most often heals by fibrous union
-if fracture line is evident by 6-9 months then bony union will probably not occur |
|
|
What should you consider laminitis to be if radiographic signs are visible?
|
-chronic
|
|
|
Radiographic signs of laminitis
|
-thickening of the dorsal hoof wall (> 20 mm)
-Palmar rotation of P3 -Indistinct dorsal surface of P3 -Increased number of vascular channels directed to the dorsal surface of P3 -Remodeling and/or pathologic fracture of the toe -Sinking of P3 -Increased founder distance (>1 cm between proximal hoof wall and proximal extensor process) -Linear lucency in the soft tissues of the dorsal hoof wall -Opaque soft tissue band at the level of the coronary band, followed by a depression in the soft tissues just proximal to the coronary band |
|
|
Non-Infectious Pedal Osteitis
-cause |
-response of the P3 to inflammation
-diffuse or focal demineralization |
|
|
Non-infectious Pedal Osteitis
-radiographic changes |
-irregularity of the solar margin
-Increased number and size of the vascular channels in P3 -Generalized loss in bone density -remodeling of the toe -tiny vascular channels radiating through the dorsal cortex of P3 -Bony response on the dorsal surface of P3 |
|
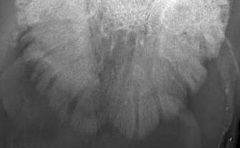
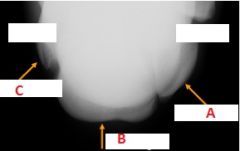
Name the condition
-why |
-non-infectious pedal osteitis
-abnormal widening of the vascular channels in P3 |
|

Name the condition
-why |
-non-infectious pedal osteitis
-yellow: remodeling of the toe -orange: vascular channels in the dorsal cortex of P3 and a faint bony response |
|
|
Why is infection of the P3 termed osteitis and not osteomyelitis?
|
-P3 does not have a medullary cavity
|
|
|
Infectious pedal osteitis
-cause |
-penetrating wounds
-sub-solar abcess formation |
|
|
Infectious Pedal Osteitis
-radiographic findings |
-focal areas of bone lysis
-sequestrum formation -possible gas in soft tissues |
|
|
How do you know if the presence of gas on a radiograph is due to a sub-solar abcess?
|
-if you know that packing of the hoof was completed correctly
|
|
|
Normal nutrient foramen locations of P1
|
-mid-diaphyseal dorsal cortex (lateral)
-distal 1/3 of palmar cortex (lateral) -circular; mid-diaphyseal (doral-palmar) |
|

Name these normal structures of P1
|
-yellow: oblique sesamoidean ligament attachment
-orange: collateral ligament for digital interphalangeal joint |
|
|
Degenerative Joint Disease
-aka |
-Osteoarthrosis
|
|
|
Degenerative Joint Disease is secondary to what diseases?
|
-trauma
-joint instability -poor confirmation -infection -developmental orthopedic disease |
|
|
Degenerative Joint Disease
-Radiographic findings |
-periarticular osteophyte formation
-enthesophytes -joint space width changes -subchondral bone lysis or sclerosis -soft tissue swelling |
|
|
Enthesophyte
-definition |
-new bone formation at the site of soft tissue attachment
|
|
Classify the condition
|
-Severe Degenerative Joint Disease
|
|
Classify the Condition
|
-Moderate Degenerative Joint Disease
|
|
|
Most common fractures of P1 and P2
|
-chip fracture of the proximal, dorsomedial ridge of P1
-spiral/longitudinal sagittal fracture of P1 -comminuted fracture of P2 |
|

Classify the condition
|
-Chip fracture of P1
|
|
|
What are chip fractures of P1 most commonly due to?
|
-overextension injuries
|
|

Classify the condition
|
-comminuted fracture of P2
|
|
|
Flexural defomities
-location |
-most common at distal interphalangeal joint
-can occur at proximal interphalangeal joint |
|
|
Flexural deformities
-cause |
-congenital
-acquired |
|
|
Deformity of the distal interphalangeal joint
-due to |
-contracture (or decreased length relative to bone growth) of the deep digital flexor tendon and/or the inferior check ligament
|
|
|
Flexural deformities
-radiographic findings |
-vertical orientation of the hoof wall relative to the ground
|
|

Classify the condition
|
-flexural deformity of the distal interphalangeal joint
|
|

Classify the condition
-due to |
-luxation
-due to deep digital flexor tendon disruption |
|
|
Navicular degeneration vs. Navicular Disease
|
-Navicular degeneration: radiographic change
-Navicular disease: clinical disease |
|
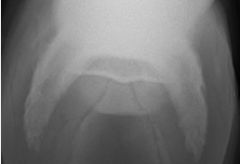
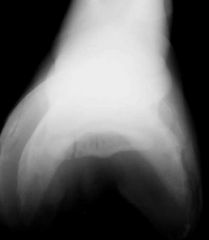
Name the radiographic view
|
-skyline view
|
|
|
Navicular degeneration
-radiographic findings |
-erosive lesions of the flexor cortex
-cystic lesions within the body of the navicular bone -sclerosis of the medullary cavity, with loss of corticomedullary definition -increase in the number, size, shape of synovial invaginations -fractures/avulsions of the distal flexor border of the navicular bone (impar ligament) -osteophyte/enthesophyte production and remodeling at the proximal border and extremities of the bone -mineralization of the distal sesamoidian (impar) ligament |
|
|
Navicular bone
-ligament attached to the distal flexor border |
-distal sesamoidean ligament (impar ligament)
|
|
|
Navicular bone infection
-name of condition |
-osteomyelitis
|
|
|
Navicular bone osteomyelitis
-secondary disease to |
-penetrating wound
|
|
|
How to determine if the navicular bone or bursa was involved in a penetrating wound
|
-Fistulography
|
|
|
Fistulography
-definition |
-intraduction of positive contrast in a wound or drainage tract
|
|
|
Osteomyelitis of the navicular bone
-radiographic findings |
-sclerosis or lysis of the bone (flexor cortex)
|
|
|
Navicular Bone Fracture
-reason for a false positive diagnosis |
-improper packing leading to overlying sulcus artifact
|
|
|
Where should fractures of the navicular bone be confined to?
|
-margins of the navicular bone
|
|
|
What can be done helpful for cases where a navicular bone fracture is expected but cannot be confirmed on the initial radiograph examination?
|
-re-evaluation in 10-14 days
|
|
|
Navicular bone fracture
-method of healing |
-fibrous union
|
|
|
Multipartite
-definition |
-multiple areas of ossification
|
|
|
Osseous fragments at the distal border of the navicular bone
-causes |
-chip fracture (avulsion of impar ligament)
-separate centers of ossification within the impar ligament -mineralization of synovium |
|
Classify the condition
|
-fracture of the navicular bone
|
|
|
Soft tissue swelling over the dorsal surface of the Metacarpus, or Metatarsus
-reason |
-periostitis
|
|
|
Soft tissue swelling on the palmaroplantar surface of the Metacarpal, or Metatarsal bone/joint
-reason |
-flexor tendon abnormality
-suspensory desmitis |
|
|
Soft tissue swelling of the Metacarpus, or Metatarsus
-causes |
-trauma
-infection |
|
|
Most common form of soft tissue mineralization of the Metacarpal, or Metatarsal region
|
-Dystrophic mineralization
|
|
|
Reason for periosteal reastion on the dorsal surface of MCIII
|
-response to microfractures
|
|
|
Why might periosteal reaction occur between MCII and MCIII or between MCIII and MCIV?
|
-interosseous ligament damage
|
|

Classify the condition
|
-periosteal reaction
|
|
|
Most common location for metacarpal/metatarsal fractures
|
-distal half of the splint bones
|
|
|
Most common location for incomplete/stress fractures of Metacarpals/Metatarsals
|
MCIII or MTIII:
-distal condyle of MCIII -Dorsal cortex -Palmaroplantar cortex |
|
|
Sesamoid fracture types
|
-apical
-mid-body -basilar |
|
|
Abaxial sesamoid fracture
-cause |
-avulsion fracture from suspensory ligament
|
|

Classify the condition
|
-apical fracture of the sesamoid
|
|
|
Differential for mineralization of soft tissue around the Metacarpal/Metatarsal joints
|
-cortisone arthropothy (injection of steroids)
|
|
|
Osteocondrosis of Metacrapals/Metatarsals
-common cause |
-abnormal endocondral ossification
|
|
|
Why should images of the contralateral limb always be taken with suspected osteocondrosis of the metacarpals/metatarsals?
|
-commonly occurs bilaterally
|
|
|
Osteochondrosis of metacarpals/metatarsals
-radiographic findings |
-subchondral bone lucency
-flattening with adjacent sclerosis -defect/irregularity in subchondral bone -osseous fragment possibly present -osseous cyst-like lesion |
|
|
Common locations of osteochondrosis in the metacarpophalangeal joint
|
-sagittal ridge of MCIII/MTIII
-distal condyle of MCIII/MTIII -proximal phalynx -palmar eminence of the proximal phalanx |
|

Classify the condition
|
-Subchondral cysts
|
|
|
Sesmoiditis
-location of normal association with degenerative change |
-suspensory ligament
|
|
|
Sesmoiditis
-radiographic findings |
-bony proliferations on the non-articular margins of the proximal sesamoids
-linear or cystic lesions in the abaxial surface -lysis in the axial margins associated with disease of the intersesamoidean ligament |
|

Classify the condition
|
-Sesmoiditis
|
|
|
Sequestra
-Most common location |
-distal extremities
-areas where little soft tissue is covering bone |
|
|
When does a sequestra form?
|
-when a portion of the bone becomes avascular
|
|
|
Sequestra
-radiographic findings |
-sharply marginated, sclerotic fragment
-fragment separated by the parent bone by a zone of lucency and outer rim of sclerotic bone -draining tract (cloaca) may be present |
|

Classify the condition
|
-sequestra
|
|

Classify the Structure
|
-chestnut
|
|
|
Carpus
-Intra-capsular swelling differentials |
-synovitis
-osteoarthrosis -fracture -sepsis |
|
|
Carpus
-Extra-capsular swelling differentials |
-hygroma
-tendon disease -abscess -cellulitis |
|
|
Hygroma
-definition |
-subcutaneous synovial bursa that forms as a result of trauma
|
|
|
If a swelling is centered around 1 joint margin, what kind of swelling is it most likely?
|
-intra-capsular
|
|
|
Carpus fracture
-concurrent condition that is usually present |
-soft tissue swelling
|
|
|
Carpus fracture
-types |
-chip
-corner (large chip) -slab |
|
|
Carpus fracture
-common locations of chip fractures |
-dorsodistal surface of the radium
-dorsodistal margin of the radial carpal and intermediate carpal bones -proximal 3rd carpal bone -dorsoproximal intermediate and radial carpal bones |
|
|
Carpus fracture
-most useful views for chip fractures |
-flexed lateral
-oblique |
|
|
Carpus fracture
-most common slab fracture |
-3rd carpal bone
|
|
|
-A: 4th carpal
-B: 3rd Carpal -C: 2nd carpal |
|
Classify the condition
|
-dorsal slab fracture
|
|
Classify the condition
|
-parasaggital slab fracture
|
|
|
Effect of stress from training on the carpal bones
|
-sclerosis of the 3rd carpal bone
|
|
|
3rd Carpal bone Sclerosis
-view necessary to detect -other findings |
-skyline view of the distal row of carpal bones
-lose normal trabecular pattern of bone -lose distinction between cortical and medullary bone |
|

Classify the condition
-why |
-Degenerative Joint Disease of the carpus
-heterogenous opacity -periarticular osteophytes |
|
|
Angular limb deformity
-radiographic findings |
-physitis
-wedging of the distal radial epiphysis -incomplete cuboidal bone ossification or malformation |
|
|
Physitis
-defintion |
-irregularity with asymmetrical widening of the distal radial physis, metaphyseal and epiphyseal flaring, and cortical thickening)
|
|
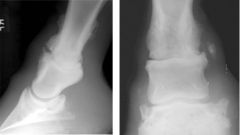
Classify the condition
|
-angular limb deformity
|
|
|
Osteochondrosis of the Tarsus
-common locations |
-Distal Intermediate Ridge of the Tibia (DIRT)
-Medial and Lateral Trochlear Ridges |
|

Radiographic view
|
-DMPLO
|
|

Classify the Condition
|
-DIRT lesion (arrow)
-osteochondrosis of the Tarsus |
|
|
View where it is easiest to view a DIRT lesion
|
-DMPLO
|
|

Radiographic View
|
-DLPMO
|
|
|
If a fracture of the Tarsus is difficult to detect, what should be done?
-why? |
-radiographic reassessment in 7-14 days
-allows time for bony remodeling to occur at the fracture site |
|

Classify the Condition
|
-Slab fracture of the tarsus
|
|

Classify the condition
|
-ankylosis from osteoarthrosis (DJD)
|
|
|
Cause of septic arthritis in foals
|
-hematogenous spread
|
|
|
Cause of osteomyelitis in adult horses
|
-penetrating wounds
|
|
|
Septic Arthritis
-radiographic findings |
-joint effusion
-subchondral bone lysis -collapse of the joint |
|

Classify the condition
|
-Septic arthritis with osteomyelitis
|