![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
1304 Cards in this Set
- Front
- Back
|
Which blood vessels branch FIRST from the aorta? A) Pulmonary arteries B) Renal arteries C) Femoral arteries D) Coronary arteries |
D) |
|
|
Which of the following relates to rhythmic pacemaker cells? A) Have organized sarcomeres B) Action potentials are generated through the funny current C) Have plateaus in the action potential D) Contribute to the force of contraction |
B) |
|
|
The importance of the plateau phase of the action potential of myocardial cells is in:
A) Enhancing the efficiency of oxygen use by the cells
B) Regulating Ca2+ availability of the cells
C) Preventing over-stretching of the cells
D) Preventing tetanus |
D) |
|
|
At what point in the cardiac cycle does ventricular relaxation occur? A) Begins during the first part of the P wave B) Begins just after the Q wave C) Begins just before the T wave D) Begins just after the T wave |
C) |
|
|
Which of the following paracrines does NOT cause vasodilation?
A) CO2
B) Ca2+
C) H+ ions from metabolic acids
D) Nitric oxide |
B) |
|
|
What are the main functions of the circulatory system? |
Transport and distribute essential substances to the tissues (where oxygen is the main one) Remove metabolic byproducts Adjustment of oxygen and nutrient supply in different physiologic states Regulation of body temperature Humoral communication |
|
|
In the transportation of materials entering the body in the cardiovascular system, where does oxygen come from and go to? |
From lungs To all cells |
|
|
In the transportation of materials entering the body in the cardiovascular system, where does nutrients and waste come from and go to? |
From intestinal tract
To all cells |
|
|
In the transportation of materials from cell to cell in the cardiovascular system, where does waste come from and go to? |
From some cells To liver for processing |
|
|
In the transportation of materials from cell to cell in the cardiovascular system, where does immune cells, antibodies and clotting proteins come from and go to? |
From being present in blood continuously To being available to any cell that needs them Immune cells go to specific and certain areas where immune reaction is happening and are removed by the spleen |
|
|
In the transportation of materials from cell to cell in the cardiovascular system, where does hormones come from and go to? |
From endocrine cells To target cells |
|
|
In the transportation of materials from cell to cell in the cardiovascular system, where does stored nutrients come from and go to? |
From liver and adipose tissue To all cells |
|
|
In the transportation of materials leaving the body in the cardiovascular system, where does metabolic waste come from and go to? |
From all cells To kidneys |
|
|
In the transportation of materials from cell to cell in the cardiovascular system, where does heat come from and go to? |
From all cells To skin |
|
|
In the transportation of materials from cell to cell in the cardiovascular system, where does carbon dioxide come from and go to? |
From all cells To lungs |
|
|
Why is a steady supply of oxygen for the cells particularly important? |
Cells deprived of oxygen can become irreparably damaged within a short period of time If oxygen delivery stops to the brain for 5 to 10 minutes, permanent brain damage results |
|
|
What happens if the brain is deprived of oxygen? |
If oxygen delivery stops to the brain for 5 to 10 minutes, permanent brain damage results Because of brain's sensitivity to hypoxia (low oxygen), homeostatic controls do everything possible to maintain cerebral blood flow even if it means depriving other cells of oxygen |
|
|
What is hypoxia? |
Low oxygen supply to tissue/cells |
|
|
Arteries take blood away or to the heart? |
Away from the heart |
|
|
Veins take blood away or to the heart? |
To the heart |
|
|
What do pulmonary veins do? |
Return O2-rich blood to the left atrium |
|
|
What does the aorta do? |
Carry O2-rich blood from the left ventricle and branches with an artery to go to specific organs Generally, an artery divides into arterioles and capillaries which then lead to venules |
|
|
What is the septum? |
The central wall of the heart divided it into two halves (right and left) |
|
|
What is the atrium? |
Part of the heart Receives blood returning to the heart from blood vessels |
|
|
What is the ventricle? |
Part of the heart Pump blood out into blood vessels |
|
|
What type of blood does the right side of the heart receive? |
Blood from tissues and sends it to lungs for oxygenation
NOTE: Deoxygenated blood is not completely devoid of oxygen, simply has less oxygen than blood going from lungs to the tissues |
|
|
What type of blood does the left side of the heart receive? |
Newly oxygenated blood from the lungs and pumps it to the tissues throughout the body |
|
|
What is cyanosis? |
Low-oxygen blood which impart a bluish colour to certain areas of the skin |
|
|
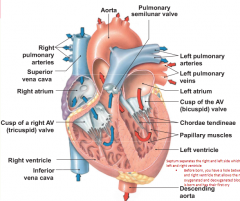
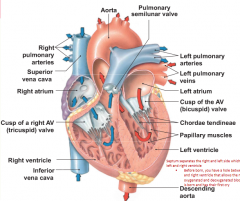
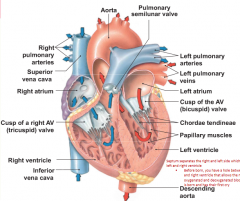
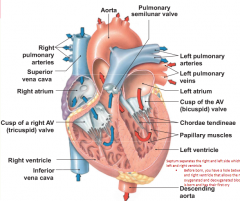
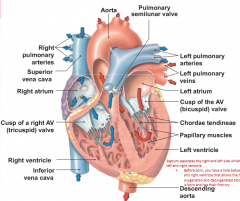
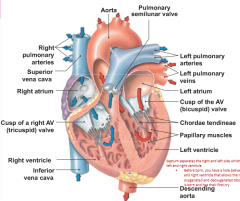
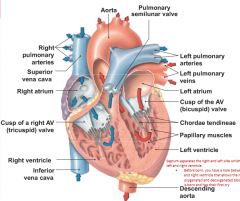
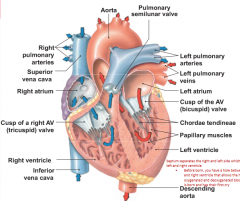
Generalize the pathway of blood flow in the heart? |
Superior and inferior vena cava Enters right atrium Blood flows through tricuspid valve into right ventricle Pumped through pulmonary semilunar valve to pulmonary trunk and arteries to the lungs to pulmonary veins leaving the lungs Blood from lungs enter heart at left atrium and passes through bicuspid valve into left ventricle Goes through aortic semilunar valve to aorta to the body |
|
|
What is the superior vena cava? |
Formed from the joining of the veins from the upper part of the body Empties into the right atrium |
|
|
What is the inferior vena cava? |
Formed from the joining of the veins from lower part of the body
Empties into the right atrium |
|
|
What are the coronary arteries? |
First branch/division of aorta after it leaves the left ventricle Nourish the heart muscle itself Blood from these arteries flow into capillaries then into coronary veins which empty directly into right atrium at the coronary sinus |
|
|
What does the abdominal aorta supply blood to? |
Supplies blood to the trunk, legs, andinternal organs such as liver (hepatic artery), digestive tract and kidney (renal arteries) |
|
|
What are hepatic portal veins? |
Blood leaving the digestive tract goes directly to the liver by hepatic portal veins |
|
|
What is the hypothalamic-hypohyseal portal system? |
Connects the hypothalamus and anterior pituitary |
|
|
What is the pericardium? |
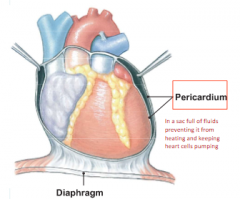
A sac full of fluids preventing it from heating and keeping heart cells pumping
A tough membrane sac that consists of a thin layer of pericardial fluid that lubricates external surface of the heart as it beats
Inflammation of the pericardium (pericarditis) may reduce the lubrication to the point that the heart rubs against the pericardium, creating sound known as friction rub |
|
|
What is pericarditis? |
Inflammation of the pericardium May reduce the lubrication in the pericardium to the point that the heart rubs against the pericardium, creating sound known as a friction rub |
|
|
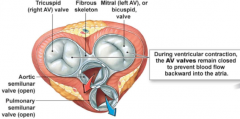
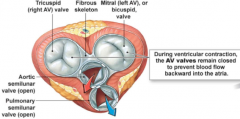
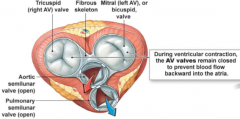
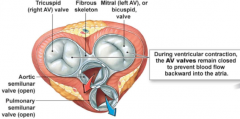
What is the atrioventricular (AV) valves? |
Occur between the atria and ventricles Valves are re-enforced by chordae tendinae attached to muscular projections within the ventricles Two types of non-identical AV valves: 1) Tricuspid valve 2) Bicuspid valve |
|
|
What are the twp types of non-identical AV valves? |
Tricuspid valve Bicuspid valve |
|
|
What is the tricuspid valve? |
An AV valve Separates the right atrium and ventricle (right AV junction) Has three flaps |
|
|
What is the bicuspid valve? |
An AV valve AKA Mitral valve Between left atrium and left ventricle (left AV junction) Has two flaps As you get older, it gets more stiff and can cause problems |
|
|
What is valve prolapse in the heart? |
It is when the valves cannot close |
|
|
What is the semilunar valves? |
Between ventricle and arteries Separate ventricle from major arteries Each have three cuplike leaflets that snap close when blood attempting Two types: 1) Aortic valve 2) Pulmonary valve Semilunar valves prevent blood that has entered the arteries from flowing back into the ventricles during ventricular relaxation |
|
|
What is the aortic valve? |
A semilunar valve Between left ventricle and aorta |
|
|
What is the pulmonary valve? |
A semilunar valve Between right ventricle and pulmonary trunk |
|
|
Where does the right atrium receive blood from and send to? |
Receive from venae cavae Send to right ventricle |
|
|
Where does the right ventricle receive blood from and send to? |
Receive from right atrium Send to right lungs |
|
|
Where does the left atrium receive blood from and send to? |
Receive from pulmonary veins Send to left ventricle |
|
|
Where does the left ventricle receive blood from and send to? |
Receive from left atrium Send to the body except for lungs |
|
|
Where does the venae cavae receive blood from and send to? |
Receive from systemic veins Send to right atrium |
|
|
Where does the pulmonary trunk (artery) receive blood from and send to? |
Receive from systemic veins Send to right atrium |
|
|
Where does the pulmonary vein receive blood from and send to? |
Receive from veins of the lungs Send to left atrium |
|
|
Where does the aorta receive blood from and send to? |
Receive from left ventricle Send to systemic arteries |
|
|
How does the blood in the atrium get pushed into the ventricle? |
Two ways: 1) Contraction of heart would push blood from atrium to the ventricle 2) Gravitational pull of blood will cause it go from atrium to ventricle |
|
|
What is systemic circulation? |
Flow of blood between the heart and the cells of the body |
|
|
What is pulmonary circulation? |
Flow of blood between the heart and lungs |
|
|
What is coronary circulation? |
Circulation of blood within the heart |
|
|
A red blood cell is just leaving the foot. Arrange the following structures in the order that the red blood cell will encounter them on its path if it travels once around the body back to the foot: A) Inferior vena cava B) Mitral valve C) Pulmonary artery D) Aorta E) Pulmonary semilunar valve |
AECBD |
|
|
Describe myocardial muscle cells? |
Branched Single nucleus Attach to each other by specialized junctions known as intercalated disks |
|
|
What are intercalated disks? |
Specialized junctions that attach myocardial muscle cells together
Consist of interdigitated membrane
Contains desmosomes (allows force created in one cell to be transferred to adjacent cells) and gap junctions (allows waves of depolarization to spread rapidly from cell to cell)
Help make cells act and work together as if they are one cell |
|
|
What are T-Tubule in the heart muscle? |
Network of calcium signaling to spread throughout the cell |
|
|
Explain the different of cardiac muscles verses skeletal muscle appearance under light microscope: |
Both are striated |
|
|
Explain the difference of cardiac muscles verses skeletal muscle in location: |
Skeletal are attached to bones and a few sphincters close off hollow organs
Cardiac muscles are found heart muscles |
|
|
Explain the difference between cardiac muscles verses skeletal muscle tissue morphology |
Skeletal: mutinucleate, large, cylindrical fibers
Cardiac: uninucleate, shorter, branching fibers |
|
|
Explain the different of cardiac muscles verses skeletal muscle in control |
Skeletal: Ca++ and troponin, fibers independent of one another Cardiac: Ca++ and troponin, fibers electrically linked via gap junctions |
|
|
Explain the different of cardiac muscles verses skeletal muscle in contraction speed |
Skeletal: fastest Cardiac: intermediate |
|
|
Explain the different of cardiac muscles verses skeletal muscle initiation of contraction |
Skeletal: Requires ACh from motor neuron Cardiac: Authorhytmic |
|
|
Explain the difference of cardiac muscles verses skeletal muscle hormonal influence on contraction: |
Skeletal: None
Cardiac: Epineprhine |
|
|
What are autorhytmic cells? |
Initiation the contraction of cardiac muscle Signal for myocardial contraction comes Smaller from contractile cells and contain few contractile fibers Do not have organized sarcromeres Do not contribute to contractile force of the heart |
|
|
What are the steps to excitation-contraction coupling of cardiac muscle which lead to contraction? |
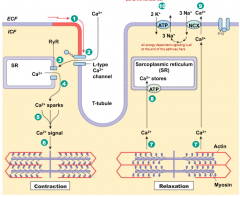
1) Action potential enters from adjacent cell
2) Voltage-gated Ca++ channels open and Ca++ enters cell
3) Ca++ induces Ca++ release through ryanodine receptor-channels (RyR)
4) Local release causes Ca++ spark
5) Summed Ca++ Sparks create a Ca++ signal
6) Ca++ ions bind to troponin to initiate contraction
7) Relaxation occurs when Ca++ unbinds from troponin
8) Ca++ is pumped back into sacroplasmic reticulum for storage
9) Ca++ is exchanged with Na+ by the NCX antiporter
10) Na+ gradient is maintained by Na+-K+-ATPase |
|
|
How much ATP is being used in the excitation-contraction coupling of cardiac muscle and when? |
2 ATP used minimally
One when Ca++ is pumped back into sacroplasmic reticulum for storage
At least one when Na+ gradient is maintained by Na+-K+-ATPase |
|
|
Do cardiac muscles have the ability to execute graded contractions? |
Yes in which fibers varies the amount of force it can generate |
|
|
How strong is the contraction force if cytosolic Ca++ concentrations are low? |
Small |
|
|
What happens to the SR, crossbridges and contraction force if additional Ca++ enters cell from extracellular fuid? |
More Ca++ released from sacroplasmic reticulum
Additional Ca++ binds to troponin, enhancing ability to form crossbridges with actin
Additional force |
|
|
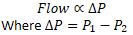
What are the phases of myocardial contractile cell action potential? |
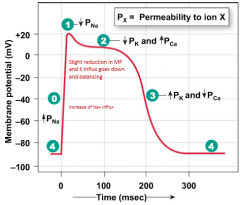
0) Na+ channels open 1) Na+ channels close 2) Ca++ channels open, fast K+ channels close 3) Ca++ channels close, slow K+ channels open 4) Resting potential |
|
|
What is phase 0 of the myocardial contractile cell action potential? |
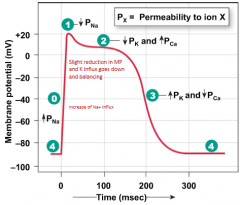
Depolarization
MP becomes more positive
Voltage-gated Na+ channels open, allowing Na+ to enter cell and rapidly depolarize it
Membrane potential reaches about +20mV before Na+ channels close |
|
|
What is phase 1 of the myocardial contractile cell action potential? |
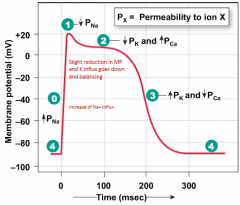
Initial repolarization Na+ close Begins repolarization as K+ leaves through open K+ channels |
|
|
What is phase 2 of the myocardial contractile cell action potential? |
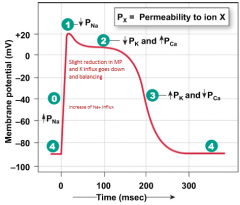
Plateau
Initial repolarization is very brief AP flattens into a plateau as result of two events 1) Decrease in K+ permeability 2) Increase in Ca2+ permeability Voltage-gated Ca2+ activated by depolarization. When open, Ca2+ enters cell "fast" K+ channels close This combination of Ca2+ influx and decreased K+ efflux causes AP to flatten out into a plateau The influx of Ca2+ lengthens the total duration of myocardial action potential The longer myocardial AP helps prevent sustained contraction called tetanus Prevention of tetanus in heart is important because cardiac muscle must relax between contraction so ventricles can filled with blood |
|
|
What is phase 3 of the myocardial contractile cell action potential? |
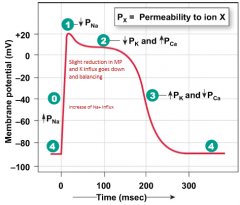
Rapid repolarization Plateau ends when Ca2+ channels close and K+ permeability increases once more "Slow" K+ channels responsible for this phase Activated by depolarization but are slow to open When this opens, K+ exits rapidly, returning cell to resting potential |
|
|
What is phase 4 of the myocardial contractile cell action potential? |
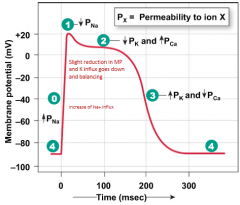
Resting membrane potential Myocardial contractile cells have stable resting potential of about -90mV |
|
|
What is the stable resting potential of myocardial contractile cells? |
-90mV |
|
|
Why is the refractory period of contractile myocardium long? |
Resetting of Na+ channels gates delayed until end of action potential |
|
|
Which of the following statements regarding contractile cells is true? A) Contractile cell action potentials have a plateau due to an increase in K+ permeability B) Contractile cell resting membrane potential is -60mV C) Depolarization due to influx of Na+ is very fast D) Depolarization is due to ion binding to cation channels |
C)
|
|
|
As blood moves through the cardiovascular system, how is pressure lost? |
Lost because of friction between fluid and blood vessel walls Pressure falls continuously as blood moves farther from the heart |
|
|
What is hydrostatic pressure? |
If fluid is not moving, the pressure it exerts is called the hydrostatic pressure Force exerted equally in all directions |
|
|
If the walls of a fluid-filled container contract, what happens to the pressure exerted on the fluids? |
Increases |
|
|
If the walls of a fluid-filled container expand/dilate, what happens to the pressure exerted on the fluids? |
Decreases |
|
|
What is the flow through a tube proportional to? |
Pressure gradient Higher pressure gradient, greater fluid flow Directly proportional to the pressure gradient Inversely proportional to resistance to flow Flow depends on pressure gradient NOT absolute pressure |
|
|
What is the system resistance to flow in the cardiovascular system? |

Tendency of cardiovascular system to oppose blood flow
An increase in resistance of blood vessel results in a decrease in low through the vessels |
|
|
In system resistance to flow in cardiovascular system, what happens if resistance increases? |
Flow decreases |
|
|
In system resistance to flow in cardiovascular system, what happens if resistance decreases? |
Flow increases |
|
|
What is Poiseuille's law? |

Resistance to fluid offered by a tube increases as the length of the tube increases Resistance increases as viscosity of fluid increases Resistance decreases as the tube's radius increases |
|
|
What is the main variable that affects resistance in the systemic circulation and why? |
Changes in the radius of blood vessels Because of Poiseuille's law |
|
|
What is vasoconstriction? |
Decrease in blood vessel diameter Decreases blood flow through a vessel |
|
|
What is vasodilation? |
Increases in blood vessel diameter Increases blood flow through a vessel |
|
|
What is Mean Arterial Pressure (MAP)? |

Maintained when arteries act as a pressure reservoir during heart's relaxation phase
Primary driving force for blood flow
Influenced by two parameters: 1) Cardiac output (volume of blood that heart pumps per minute) 2) Peripheral resistance (resistance of blood vessels to blood flow through them)
Closer to diastolic pressure than systolic pressure because diastole lasts twice as long as systole |
|
|
What are pacemaker cells? |
They generate spontaneous action potentials
"Slow response" action potentials where they have slower rate of depolarization Found in the sinoatrial and atrioventricular nodes of the heart The SA node is the fastest pacemaker and normally sets the heart rate. If this is damaged and cannot function, a slower pacemaker will take over |
|
|
What cells in heart have rapid depolarization? |
Non-pacemaker cells |
|
|
What is the underlying reason that heart cells contract? |
Pacemakers/initiator cells Unstable resting membrane potentials (called a pacemaker potential) -55 to -62mV Due to presence of funny current Have the ability to generate action potential spontaneously in absence of input from nervous system |
|
|
What are If channels? |
Funny current
The reason myocardial autorhytmic cells (pacemaker cells) can contract the heart spontaneously
Permeable to both K+ and Na+ (If belongs to a family of HCN [Hyperpolarization-activated Cyclic Nucleotide-gated] channels which is energy dependent)
When open at negative membrane potential, Na+ influx exceeds K+ efflux
As membrane potential becomes more positive, If channels gradually close and one set of Ca++ channels open |
|
|
How do depolarization of autorhythmic cells rapidly spread to adjacent contractile cells? |
Through gap junctions of intercalated disks |
|
|
What is the role of Na+ and Ca++ ions in depolarization of nerve and muscle cells? |
Depolarization phase caused by opening of sodium channels |
|
|
What is the role of Na+ and Ca++ ions in depolarization of cardiac pacemaker cells? |
Ca++ ions are involved in the initial depolarization phase of the action potential |
|
|
What is the role of Na+ and Ca++ ions in depolarization of cardiac non-pacemaker cells? |
Ca++ influx prolongs the duration of the action potential and produces a characteristic plateau phase |
|
|
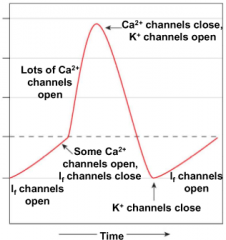
What are the 5 steps in electrical conduction in the heart? |
1) SA node depolarizes 2) Electrical activity goes rapidly to AV node via internodal pathways 3) Depolarization spreads more slowly across atria. Conduction slows through AV node 4) Depolarization moves rapidly through ventricular conducting system to the apex of the heart 5) Depolarization wave spreads upward from the apex through Purkinje fibers causing contractile cells to contract simultaneously |
|
|
In electrical conduction in the heart, why does depolarization spread slowly across the atria? |
The action potential encounters fibrous skeleton of the heart at the junction of atria and ventricles which will act as a barricade This prevents transfer of electrical signals from atria to ventricles |
|
|
What is the SA node? |
Set of pace of the heartbeat at ~70bpm AV node (50 bpm) and Purkinje fibers (25-40 bpm) can act as pacemakers under some conditions Slower pacemaker activity Depolarization begins here |
|
|
What is AV node? |
Routes the direction of electrical signals Delays the transmission of action potentials |
|
|
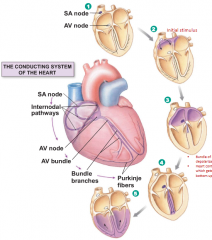
What is the vagus nerve? |
Activation of this can innervate the SA node At rest, significant vagal tone on SA node cause resting heart rate between 60 and 80 beats per min Can cause decreased heart rate Part of parasympathetic system These parasympathetic fibers CANNOT change the force of contraction because they only innervate the SA node and AV node |
|
|
What is atropine? |
A muscarinic receptor antagonist, leads to a 20-40 beat per minute increase in heart rate |
|
|
What can cause the heart rate to increase? |
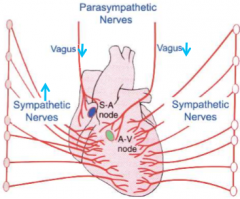
A withdrawal (decrease) of vagal tone Activation of sympathetic nerves innervating SA node Circulating catecholamines acting via beta-1-andrenoceptors located on SA nodal cells |
|
|
How does beta-1-receptors cause increase heart rate? |
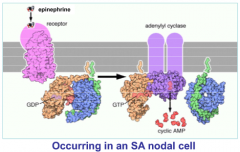
B1 receptor activation via EPI binding cause cyclic AMP production within the cell
Funny current channels are HCN which are cyclic nucleotide gated channels
cAMP increases which directly increase funny current resulting in Na+ entering the cell more quickly
More cAMP also makes more PKA which phosphorylates numerous calcium channels (DHPR, RyR and SERCA) further increasing calcium conductance into the cell
Action potential generated more frequently |
|
|
How does the parasympathetic system decrease the heart rate? |
Pacemaker cells have muscarinic M2 Gi-protein coupled receptors ACh acts on beta-gamma subunits of G-proteins, activates K+ channels Once opens, cause K+ to leak out and cell becomes hyperpolarized Funny current also reduced by ACh where lower cAMP decreases activity of ion channel, decreasing sodium influx which means takes longer for cell to reach threshold Therefore, heart rate slows |
|
|
How does ACh reduce funny currents? |
Causes decreased amounts of cAMP which decreases activity of ion channels, decreasing sodium influx Therefore longer for cell to reach threshold |
|
|
Which of the following statements regarding autorhythmic cells is true? A) The depolarization phase requires the movement of K+ out of the cell B) Are found throughout the heart C) The membrane potential is unstable, floating between -55mV to -90mV D) Increasing the concentration of cAMP will increase the rate of depolarization |
D) |
|
|
What is Einthoven's triangle? |
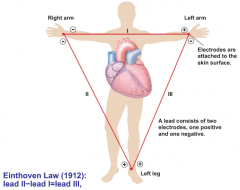
ECG electrodes attach to both arms and left leg form a triangle. Each two-electrode pair constitutes one lead (pronounced "leed"), which one positive and one negative electrode. An ECG is recorded from one lead at a time |
|
|
What is Electrocardiogram (ECGs)? |
Show summed electrical activity generated by all cells of heart Contains multiple leads, positive, negative and inactive Two major components of waves (deflections above and below baseline of P, QRS, and T) and segments (sections of baseline between two waves) Different waves of ECG reflect depolarization or repolarization of atria and ventricle |
|
|
How is it possible to use surface electrodes to record internal electrical activity? |
Salt solutions (such as NaCl-basedextracellular fluid) are good conductors of electricity |
|
|
What are the three major waves of the ECG? |
P wave QRS complex T wave |
|
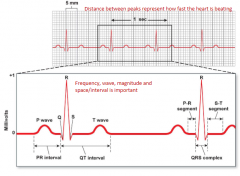
Label this ECG with its waves, intervals and segments: |
|
|
|
What is the P wave of an ECG? |
Atrial depolarization Initiation of heart beat |
|
|
What is the P-R segment of an ECG? |
Conduction through AV node and AV bundle Depolarization travels down to atrium |
|
|
What is the QRS complex of an ECG? |
Ventricular depolarization |
|
|
What is the T wave of an ECG? |
Ventricular repolarization |
|
|
What is an interval of an ECG? |
Combination of waves and segments |
|
|
What is the electrical events of the cardiac cycle? |
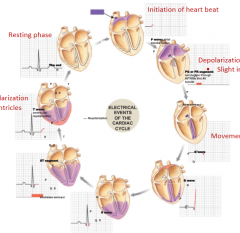
1) P wave: initiation of the heart beat, atrial depolarization 2) PQ or PR segment: conduction through AV node and AV bundle, depolarization travels down atrium, slight increase in P wave 3) Q wave: movement of electrical down sternum 4) R wave 5) S wave: depolarization back up heart, repolarization of ventricle also happen but you do not see it 6) ST segment: ventricles contract 7) T waves: Ventricular repolarize 8) End: resting phase |
|
|
What is the Q wave of an ECG? |
Movement of electrical down sternum |
|
|
What is the S wave of an ECG? |
Depolarization back up heart Repolarization of ventricle also happen but you do not see it |
|
|
What is the ST segment of an ECG? |
Ventricles contract |
|
|
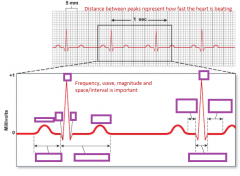
What does the distance between peaks represent in the heart on an ECG? |
How fast the heart is beating |
|

Is this a normal or abnormal ECG? If abnormal, how so? |
Normal |
|

Is this a normal or abnormal ECG? If abnormal, how so? |
Third-degree block
Normal P, wide QRS
Not severe but not good as you are getting depolarization of atrium more frequently than of ventricle |
|

Is this a normal or abnormal ECG? If abnormal, how so? |
Atrial fibrillation No P, irregular QRS |
|

Is this a normal or abnormal ECG? If abnormal, how so? |
Ventricular fibrillation No P, no QRS |
|

Is this a normal or abnormal ECG? If abnormal, how so? |
Second degree heart block P not triggering QRS |
|
|
Which of the following statements regarding an ECG tracing is true? A) The atria depolarize during PR segment B) Ventricles contract during ST segment C) The T wave indicates atrial and ventricular repolarization D) The QRS complex indicates ventricular contraction |
B) |
|
|
What is complete heart block? |
Conduction of electrical signals from atria to ventricles through AV node is disrupted SA node fires at rate of 70 beats per minute but those signals never reach ventricle Ventricles coordinate with fastest pacemaker Rate at which ventricles contract is much slower than rate at which atria contract If ventricular contraction is too slow to maintain adequate blood flow, it may be necessary for heart's rhythm to be set artificially by a surgically implanted mechanical pacemaker |
|
|
What are cardiac arrhythmias? |
Family of cardiac pathologies that range from benign to those with potentially fatal consequences Electrical problems that arise during the generation or conduction of action potentials through the heart Usually can be seen on ECG Some can be "dropped beats" that result when ventricles do not get their usual signal to contract Some at PVCs (premature ventricular contractions) Extra beats that occur when an autorhytmic cell other than an SA node jumps in and fires an action potential out of sequence |
|
|
What is Long QT syndrome (LQTS)? |
Heart condition that can be observed with an ECG Has several forms: Some are inherited channelopathies which mutations occur in myocardial Na+ and K+ channels Another form, ion channels are normal but protein ankyrin-B that anchors that channel to cell membrane is defective |
|
|
What is iatrogenic? |
Form of LQTS Physician-caused Occur as a side effect of taking certain medication Can be caused when patient takes a non-sedating antihistamine called terfenadine (Seldane) that binds to K+ repolarization channel Can be lethal |
|
|
What are the two phases of cardiac cycle? |
Diastole Systole |
|
|
What is diastole? |
Time during which cardiac muscle relaxes Ventricles are relaxed Heart spends 2/3 in diastole |
|
|
What is systole? |
Time during which muscle contracts Ventricles contract |
|
|
In general, which side of the heart will have lower pressure? |
Right |
|
|
What are the 5 mechanical events/phases of the cardiac/heart cycle between contraction and relaxation? |
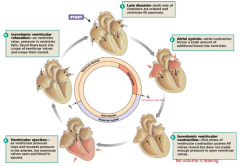
1) Late atrial and ventricular diastole where heart is at rest 2) Atrial systole and completion of ventricular filling 3) Isovolumic ventricle contraction 4) Ventricular ejection and heart pump 5) Isovolumic ventricle relaxation |
|
|
What happens during the late atrial and ventricular diastole event/phase of the cardiac/heart cycle between contraction and relaxation? |
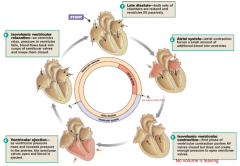
Event/phase 1
Both sets of chambers are relaxed and ventricles fill passively
As the ventricles relax, AV valves between atria and ventricles open
Relaxing ventricles expand to accommodate the entering blood |
|
|
What happens during atrial systole and completion of ventricular filling event/phase of the cardiac/heart cycle between contraction and relaxation? |
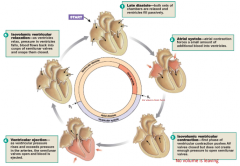
Event/phase 2 Atrial contraction forces a small amount of additional blood into ventricles It begins following a wave of depolarization that sweeps across the atria Pressure increases that accompanies contraction pushes blood into ventricle Small amount of blood forced backwards into veins |
|
|
What happens during the isovolumic ventricular contraction event/phase of the cardiac/heart cycle between contraction and relaxation? |
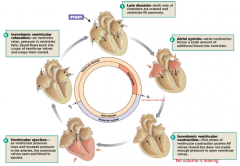
Event/phase 3 First heart beat sound First phase of ventricular contraction pushes AV valve closed but does not create enough pressure to open semilunar valves Here high pressure will develop but no movement happens While ventricles begin to contract, atrial muscle fibers are repolarizing and relaxing |
|
|
What happens during ventricular ejection and heart pump event/phase of the cardiac/heart cycle between contraction and relaxation? |
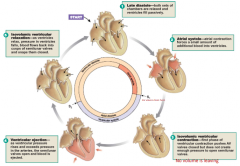
Event/phase 4 As ventricular pressure rises and exceeds pressure in arteries, semilunar valves open and blood is ejected High-pressure blood is forced into arteries, displacing low-pressure blood that fills them and pushing it farther into vascular AV valves remain closed |
|
|
What happens during isovolumic ventricular relaxation event/phase of the cardiac/heart cycle between contraction and relaxation? |
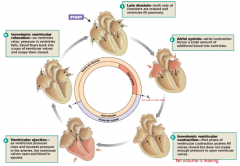
Event/phase 5 (final) Second heart beat As ventricles relax, pressure in ventricles falls, blood flows back into cusps of semilunar valves and snaps them closed At end of ventricular ejection, ventricles begin to repolarize in arteries and blood starts to flow backward into heart |
|
|
During which events/phases of the cardiac/heart cycle between contraction and relaxation would you hear heart beats? |
During isovolumic ventricular contraction (3rd) and relaxation (5th)
Lub, dub |
|
|
During which events/phases of the cardiac/heart cycle between contraction and relaxation would have the highest pressure? |

During ventricular ejection (4th) |
|
|
During which events/phases of the cardiac/heart cycle between contraction and relaxation would you find the QRS complex? |

During atrial systole and completion of ventricular filling (2nd, Q) and isovolumic ventricle contraction (3rd, RS) |
|
|
During which events/phases of the cardiac/heart cycle between contraction and relaxation would the left ventricle volume be lowered? |

During the ventricular ejection (4th) |
|
|
Which of the following statements regarding the cardiac cycle is true? A) Isovolumetric ventricular contraction is seen as a flat horizontal line (not volume) B) Blood is ejected when ventricular pressure exceeds the aortic pressure C) The QRS complex occurs just after the rise in ventricular pressure D) Atrial systole is needed for most of the ventricular filling |
B) |
|
|
What causes the vibrations of the first heart beat? |
Closure of AV valves |
|
|
What causes vibrations of the second heart beat? |
Closing of semilunar valve |
|
|
What are the steps in left ventricular press-volume changes during one cardiac cycle? |
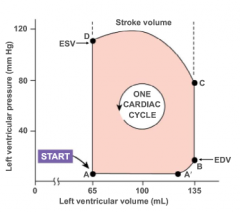
A) Venticular filling where pressure at minimum and mitral valves open
B) End diastolic volume where most volume at the heart at one time where atrium pushes last bit of blood C) Start of systole and isovolumetric contraction D) Blood ejected from heart and isovolumetric relaxation (end-systolic volume) |
|
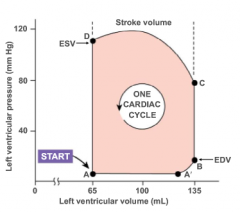
Match the following events to points A-D A) Aortic Valve opens B) Mitral Valve Opens C) Aortic Valve closes D) Mitral Valve closes |
A) C B) A C) D D) B |
|
|
What is stroke volume? |
SV = EVS - ESV
Amount of blood pumped by 1 ventricle in 1 contraction
Volume of blood before contraction subtracted by volume of blood after contraction is equal to stroke volume
Average for person at rest is 70mL
Stroke volume is not constant and can increase to as much as 100mL during exercise |
|
|
What is cardiac output? |
CO = HR * SV Amount of blood pumped ver ventricle per unit time Indicator of total blood flow through body Average is 5040mL |
|
|
If one side of heart begins to fail and unable to pump efficiently, what happens to cardiac output? |
CO becomes mismatched
Here blood pools in the circulation behind the weaker side of heart |
|
|
What is cardiac reserve? |
Difference between resting and maximal CO |
|
|
Which of the following statements regarding pressure-volume (PV) loops is true? A) Pressure is shown on X-axis and volume on Y-axis B) Blocked aortic semilunar valve would cause PV loop to be taller and shift to the right C) Decreasing heart rate will cause PV loop to be flatter and longer horizontally D) In aortic regurgitation, PV loop is wider and shifted to the left |
B) |
|
|
What is the critical factor controlling stroke volume of a heart? |
Preload of cardiac muscle cells |
|
|
What can you do increase stroke volume? |
Slow heart beat and exercise to increase venous return to the heart |
|
|
What can you do to decrease stroke volume? |
Blood loss and extremely rapid heartbeat |
|
|
In striated muscles, force created by a muscle fiber is directly related to what? |
Length of sarcomere Longer the muscle fiber and sarcomere when contraction begins, greater tension developed |
|
|
What happens to stroke volume when ventricular walls increase? |
Stroke volume increases If additional blood flows into ventricles, muscle fibers stretch then contract more forcefully, ejecting more blood |
|
|
What does the Frank-Starling law state? |
Stroke volume increases as EDV increases (which is affected by venous return) |
|
|
What is venous return affected by? |
Skeletal muscle pump
Respiratory pump
Sympathetic innervation |
|
|
What is force of contraction of heart affected by? |
Stroke volume Length of muscle fiber and contractility of heart |
|
|
How does skeletal muscle pumps affect venous return? |
Contraction or compression of veins returning blood to the heart Skeletal muscle contractions that squeeze veins (particularly in legs), compressing them and pushing blood toward the heart Helps return blood to heart when exercising and does not assist venous return when individual is resting |
|
|
How does respiratory pump affect venous return? |
Pressure changes in abdomen and thorax during breathing Created by movement of thorax during inspiration (breathing in) As chest expands and diaphragm moves towards abdomen, thoracic cavity enlarges and develops a subatmospheric pressure The lower pressure decreases pressure in inferior vena cava as it passes through thorax which helps draw more blood into vena cava from veins in abdomen |
|
|
How does sympathetic innervation affect venous return? |
Sympathetic innervation of veins When veins constrict, their volume decreases, squeezing more blood out of them and into heart With larger ventricular volume at beginning of next contraction, ventricle contracts more forcefully, sending blood out into arterial side of circulation Sympathetic innervation of veins allow body to redistribute some venous blood to arterial side of circulation |
|
|
What are some extrinsic factors influencing stroke volume separate from Frank-Starling? |
Contractility is the increase in contractile strength (independent of stretch and EDV)
Increase in contractility comes from: 1) Increase sympathetic stimuli 2) Certain hormones 3) Ca++ and some drugs |
|
|
How does a decrease in parasympathetic activity increase heart rate? |

Parasympathetic influence is withdrawn from autorhythmic cells They resume intrinsic rate of depolarization and heart rate increases to 90-100 bpm |
|
|
How does sympathetic input increase heart rate? |

Increase heart rate above intrinsic rate
Norepinephrine (or epinephrine) on beta-1-receptors speed up depolarization rate of autorhythmic cells and increase heart rate |
|
|
How does sympathetic neurons (NE) affect heart rate? |
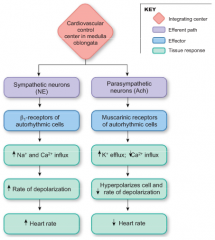
Catechoalmines bind and activate beta-1-adrenergic receptors on autorhythmic cells
Cause an increase of Na+ and Ca++ influx (Catecholamines norepinephrine and epinephrine increase ion flowthrough both If and Ca++ channels)
Increase rate of depolarization
Increase rate of heart rate (stimulation of pacemaker cells) |
|
|
What can speed up depolarization and heart rate during pacemaker potential phase? |
Increased permeability to Na+ and Ca++ |
|
|
How does parasympathetic neurons (ACh) affect heart rate? |
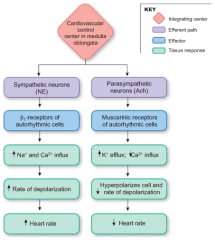
ACh activates muscarinic cholinergic receptors of autorhythmic cells
Increase K+ efflux and decrease Ca++ influx
Potassium permeability increases to hyperpolarize the cell so that pacemaker potential beings at a more negative value Also decreases rate of depolarization
Decreases heart rate |
|
|
What is the steps/events of the phospholamban as a regulatory protein that alters sacroplasmic reticulum Ca++-ATPase activity? |
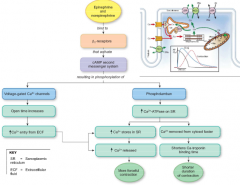
1) Signal molecule binds to and active beta-1-adrenergic recetors on contractile myocardial cell membrane
2) Activated beta-1-receptors use a cyclic AMP second messenger system to phosphorylate specific intracellular proteins
3) Phosphorylation of voltage-gated Ca2+ channels increase probability that they will open and stay open longer
More open channels allow more Ca2+ to enter cell
4) Catecholamines increase Ca2+ storage through use of regulatory protein called phospholamban
5) Phosphorylation of phospholamban enhanced Ca2+-ATPase activity in sarcoplasmic reticulum
Making more Ca2+ available for calcium-induced calcium release
6) More active crossbridges
Net result of catecholamine simulation is stronger contraction
Can also shorten duration of contraction |
|
|
What are inotropic agents? |
Any chemical that affects contractility is an 'iontropic' agent Epinephrine, norepineprine, have positive inotropic effects Chemicals with negative inotropic effects decrease contractility |
|
|
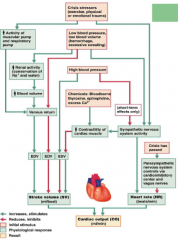
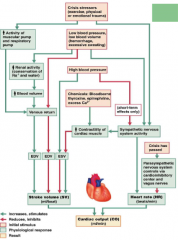
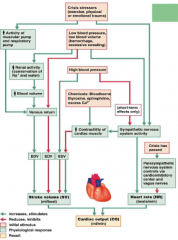
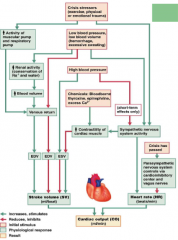
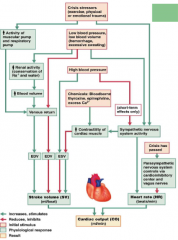
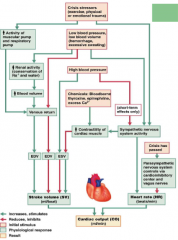
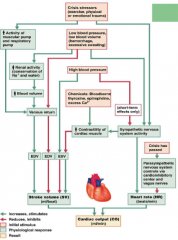
What does a crisis stressors (exercise, physical or emotional trauma) do to activity of muscular pump and respiratory pump? |
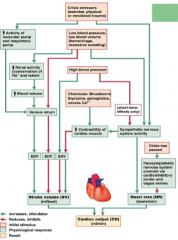
Increase/stimulate activity |
|
|
What does a crisis stressors (exercise, physical or emotional trauma) do to venous return? |
Increases/stimulates |
|
|
What does a crisis stressors (exercise, physical or emotional trauma) do to EDV? |
Increases/stimualtes |
|
|
What does a crisis stressors (exercise, physical or emotional trauma) do to stroke volume (SV)? |
Increases/stimulates |
|
|
What does a crisis stressors (exercise, physical or emotional trauma) do to cardiac output (CO)? |
Increases/stimulates |
|
|
What does a crisis stressors (exercise, physical or emotional trauma) do to sympathetic nervous system activity? |
Increases/stimualtes |
|
|
What does a crisis stressors (exercise, physical or emotional trauma) do to contractility of cardiac muscle? |
Increases/stimulates |
|
|
What does a crisis stressors (exercise, physical or emotional trauma) do to ESV? |
Decreases/inhibits |
|
|
What does a crisis stressors (exercise, physical or emotional trauma) do to heart rate (HR)? |
Increases/stimulates |
|
|
What does a low blood pressure and low blood volume (hemorrhage, excessive sweating) do to renal activity (conservation of Na+ and water)? |
Increases/stimulates |
|
|
What does a low blood pressure and low blood volume (hemorrhage, excessive sweating) do to blood volume? |
Increases/stimulates |
|
|
What does a low blood pressure and low blood volume (hemorrhage, excessive sweating) do to venuos return? |
With increased/stimulated blood volume, increase/stimulates Directly: decreases/inhibits |
|
|
What does a low blood pressure and low blood volume (hemorrhage, excessive sweating) do to EDV? |
When directly inhibiting venous return, inhibits/decreases Else words increases/stimulates |
|
|
What does a low blood pressure and low blood volume (hemorrhage, excessive sweating) do to stroke volume (SV)? |
When directly inhibiting venous return, inhibits/decreases
Else words increases/stimulates |
|
|
What does a low blood pressure and low blood volume (hemorrhage, excessive sweating) do to cardiac output (CO)? |
At first/directly: inhibit/decrease Elsewords/want to: Increases/stimulates |
|
|
What does a low blood pressure and low blood volume (hemorrhage, excessive sweating) do to sympathetic nervous system activity? |
Increases/stimulates |
|
|
What does a low blood pressure and low blood volume (hemorrhage, excessive sweating) do to contractility of cardiac muscle? |
Increases/stimulates |
|
|
What does a low blood pressure and low blood volume (hemorrhage, excessive sweating) do to ESV? |
Decreases/inhibits |
|
|
What does a low blood pressure and low blood volume (hemorrhage, excessive sweating) do to heart rate (HR)? |
Increases/stimulates
|
|
|
What does a high blood pressure do to ESV? |
Increase/stimulate |
|
|
What does a high blood pressure do to stroke volume (SV)? |
Decrease/inhibit |
|
|
What does a high blood pressure do to cardiac output (CO)? |
Decrease/inhibit |
|
|
What does a high blood pressure do to sympathetic nervous system activity? |
Short term only: Decrease/inhibit |
|
|
What does a high blood pressure do to contractility of cardiac muscle? |
Short term only: Increase/stimulate |
|
|
What does a high blood pressure do to heart rate (HR)? |
Short term only: Decrease/Inhibit |
|
|
What does a chemicals such as bloodborne, thyroxine, epinephrine and excess Ca++ do to contractility of cardiac muscle? |
Increase/stimulate |
|
|
What does a chemicals such as bloodborne, thyroxine, epinephrine and excess Ca++ do to ESV? |
Decrease/inhibit |
|
|
What does a chemicals such as bloodborne, thyroxine, epinephrine and excess Ca++ do to stroke volume (SV)? |
Increase/stimulate |
|
|
What inhibits stroke volume in cardiac output? |
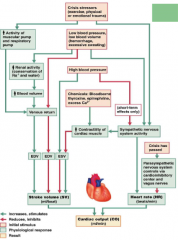
High blood pressure
Direct inhibition of venuous return from low blood pressure/volume |
|
|
Which of the following statements regarding Frank-Sterling law of the heart are true? B) Increased afterload promotes increased stroke volume C) A fast heart rate during aerobic exercise cause an increase in stroke volume D) Increasing cardiac muscle fibre length always causes stroke volume to increase |
A) |
|
|
What are the three types of blood vessels in the cardiovascular system? |
Arteries Capillaries Veins |
|
|
What is endothelium? |
Inner lining of all blood vessels
Type of epithelium
Secrete many paracrine and play important roles in regulation of blood pressure, blood vessels growth and absorption of materials |
|
|
What is tunica intima? |
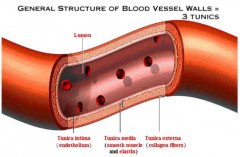
Endothelium and its adjacent elastic connective tissue together Simply called the intima Thickness of smooth muscle-connective tissue layers surrounding the intima varies in different vessels |
|
|
What is vascular smooth muscle? |
Smooth muscle of blood vessels |
|
|
What are veins? |
Venules drain blood from capillaries
Much less smooth muscle and connective tissue than arteries Have valves preventing backflow Carry about 70% of body's blood Can act as a reservoir during hemorrhage Closer to surface of body than arteries Carry blood to heart |
|
|
What are the two types of vessels in capillary beds? |
Vascular shunt
True capillaries |
|
|
What are vascular shunt? |
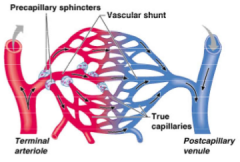
A capillary bed Directly connects an arteriole to a venule |
|
|
What are true capillaries? |
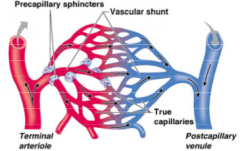
Capillary beds
Exchange vessels
Oxygen and nutrients cross to cells Carbon dioxide and metabolic waste products cross into blood |
|
|
What do precapillary sphincters do? |

If relaxed, blood flowing into metarteriole is directed into adjoining capillary beds If constricted, metarteriole blood bypasses the capillaries and goes directly to venous circulation |
|
|
Which of the following components of blood vessel walls come into direct contact with blood cells? A) Elastin B) Smooth muscle C) Collagen D) Endothelium |
D) |
|
|
What is the average resting heart rate in adults? |
~70bpm |
|
|
What is tonic control for heart rate? |
Tonic control of heart is dominated by parasympathetic branch When all sympathetic and parasympathetic input is blocked, the spontaneous depolarization rate of SA node is 90-100 times per minute To achieve resting heart rate of 70bpm, tonic parasympathetic activity must slow the intrinsic rate down from 90 bpm ACh slows conduction of action potentials through AV node, thereby increasing AV node delay Catecholamines epinephrine and norepinephrine enhance conduction of action potentials through AV node and through conduction system |
|
|
In an isolated heart, what are the two parameters that affect the force of ventricular contraction? |
Length of muscle fibers at beginning of contraction Contractility of heart |
|
|
What is contractility of the heart? |
Is the intrinsic ability of cardiac muscle fiber to contract at any given fiber length and is a function of Ca++ interaction with contractile filaments |
|
|
What are cardiac glycosides? |
Include digitoxin and related compound ouabain A molecule used to inhibit sodium transport Increase contractility by slowing Ca2+ removal from cytosol Remedy for heart failure When in drug form: -Depress Na+-K+-ATPase activity in all cells -This cause Na+ build up in cytosol and contraction gradient for Na+ across cell membrane diminishes -Decreases potential energy available for indirect active transport |
|
|
What are metartioles? |
Arterioles branch into vessels Partially surrounded by smooth muscle Allow white blood cells to go directly from arterial to venous circulation |
|
|
What are pericytes? |
Secrete factors that influence capillary growth and they can differentiate to become new endothelial or smooth muscle cells Loss of pericytes around capillaries of the retina is a hallmark of disease diabetic retinopathy, a leading cause of blindness |
|
|
What is angiogensis? |
Process by which new blood vessels develop |
|
|
What are the controls of angiogenesis? |
Controlled by balancing angiogenic and antiangiogenic cytokines A number of related growth factors promote angiogenesis including: -Vascular endothelial growth factor (VEGF) -Fibroblast growth factor (FGF) These growth factors are mitogens Meaning they promote mitosis or cell division Normally produced by smooth muscle cells and pericytes Cytokines that inhibit angiogenesis include: -Angiostatin (made from blood protein plasminogen) -Endostatin |
|
|
What growth factors promote angiogenesis? |
Vascular endothelial growth factor (VEGF) Fibroblast growth factor (FGF) |
|
|
What are some cytokines that inhibit angiognesis? |
Angiostatin Endostatin |
|
|
What is a pulse in relation to blood? |
Rapid pressure increase that occurs when left ventricle pushes blood into aorta Also known as pressure wave Amplitude of pressure wave decreases over distance because of friction and wave disappears at capillaries |
|
|
What is pulse pressure? |
Measure of strength of pressure wave Defined as systolic pressure minus diastolic pressure Systolic pressure - Diastolic pressure = Pulse pressure |
|
|
What is hypotension? |
Blood pressure falls to low |
|
|
What happens if blood pressure falls to low? |
Hypotension Driving force for blood flow is unable to overcome opposition by gravity Blood flow and oxygen supply to brain are impaired Person may become dizzy or faint |
|
|
What is hypertension? |
Blood pressure is chronically elevated |
|
|
What happens if blood pressure is chronically elevated? |
High pressure on wall of blood vessel may cause weakened areas to rupture and bleed into tissues |
|
|
What is cerebral hemorrhage? |
Rupture occurs in brain May cause loss of neurological function |
|
|
Where is blood pressure the greatest and lowest? |
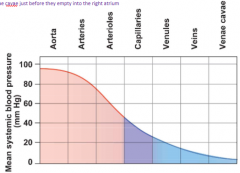
Greatest in aorta Lowest in venae cavae As blood moves through the system, pressureis lost because friction between the fluid and blood vessel walls |
|
|
Why does the heart need to create pressure and how does it do it? |
Needed for blood in order to generate blood flow (needs to generate a pressure difference)
Done with a cardiac contraction |
|
|
What is flow rate? |
Volume of blood that passes a given point in the system per unit time In circulation, flow is expressed in either liters per min or milliliters per minutes (mL/min) |
|
|
What is velocity of flow? |
Distance a fixed volume of blood travels in a given period of time Measure of how fast blood flows past a point Depends on total cross-sectional area of ALL the vessels |
|
|
What is the relationship between velocity of flow, flow rate and cross-sectional area of a tube? |

Relationship between velocity of flow (v), flow rate (Q) and cross-sectional area of a tube (A)
Velocity of flow through tube equals the flow rate divided by the tube's cross-sectional area
In a tube of a fixed diameter, velocity is directly related to flow rate
In a tube of variable diameter, if flow rate is constant, velocity varies inversely with the diameter |
|
|
Blood flow through an individual blood vessel is determined by what? |

Vessel's resistance to flow |
|
|
If a radius of a blood vessel is decreased by a factor of 2, and the length of the vessel is decreased by a factor of 4, how will the flow rate through the vessel change? |
Decreased by a factor of 4 |
|
|
What is active hyperemia? |
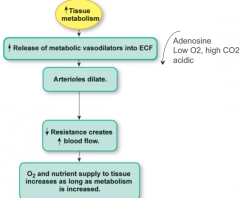
Process in which an increase in blood flow accompanies an increase in metabolic activity Locally mediated increase in blood flow |
|
|
What is reactive hypermeia? |
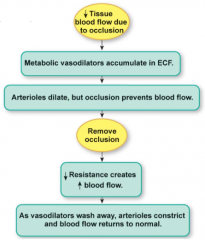
Increase in tissue blood flow following a period of low perfusion (blood flow) Locally mediated increase in blood flow |
|
|
How is there tonic control of arteriolar diameter using norepinephrine? |

Tonic discharge of norepinephrine from sympathetic neurons help maintain myogenic tone of arterioles Norepinephrine binding to alpha-receptors con vascular smooth muscle cause vasoconstriction |
|
|
Which of the following statements regarding hyperemia is true? A) Active hyperemia occurs due to a decrease in tissue metabolism B) Active hyperemia leads to a release of metabolic vasodilators to tissue C) Reactive hyperemia occurs due to an initial increase in tissue blood flow D) Reactive hyperemia occurs at the time an occlusion is present |
B) |
|
|
What is Poiseullie's Law in aspects of resistance to blood flow? |
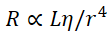
Resistance to blood flow (R) is directly proportional to length of the tube through which fluids flow (L) and the viscosity (eta) of the fluid and inversely proportional to the fourth power of the tubing radius (r) Normally length of systemic circulation and blood viscosity is relatively constant |
|
|
What local and systemic control mechanisms influence arteriolar resistance? |
Local control of arteriolar resistance Sympathetic reflexes Hormones |
|
|
What is the physiological role of norepinephrine? |
Mediates vasoconstriction Baroreceptor reflex Binds to alpha-receptors |
|
|
What is the physiological role of serotonin? |
Mediates vasoconstriction Platelet aggregation Smooth muscle contraction |
|
|
What is the physiological role of endothelin? |
Mediates vasoconstriction Local control of blood flow |
|
|
What is the physiological role of vasopressin? |
Mediates vasoconstriction Increases blood pressure in hemorrhage |
|
|
What is the physiological role of angiotensin 2? |
Mediates vasoconstriction Increases blood pressure |
|
|
What is the physiological role of epinephrine? |
Mediates vasodilation Increase blood flow to skeletal muscles, heart and liver Binds to beta-2-receptors |
|
|
What is the physiological role of acetylcholine? |
Mediates vasodilation
Many functions such as erection reflex (indirectly through NO production) |
|
|
What is the physiological role of nitric oxide (NO)? |
Mediates vasodilation Local control of blood flow |
|
|
What is the physiological role of bradykinin (via NO)? |
Mediates vasodilation
Increases blood flow Stimulates pain receptors |
|
|
What is the physiological role of adenosine? |
Mediates vasodilation Increases blood flow to match metabolism |
|
|
What is the physiological role of decreases oxygen, increased carbon dioxide, increase hydrogen and increased potassium? |
Mediates vasodilation Increased blood flow to match metabolism |
|
|
What is the physiological role of histamine? |
Mediates vasodilation Increased blood flow |
|
|
What is the physiological role of natriuretic peptides? |
Mediates vasodilation Reduces blood pressure |
|
|
What is the physiological role of vasoactive intestinal peptide? |
Mediates vasodilation Digestive secretion and relax smooth muscle |
|
|
What is myogenic autoregulation? |
Vascular smooth muscle has the ability to regulate its own state of contraction |
|
|
How is myogenic autoregulation work at the cellular level? |
When vascular smooth muscle cells in arterioles are stretched, mechanically gated channels in muscle membrane open Cation entry depolarizes the cell Depolarization open voltage-gated Ca++ channels and Ca++ flows into cell down its electrochemical gradient Ca entering cell combine with calomodulin and activates myosin light chain kinase MLCK in turn increases myosin ATPase activity and crossbridge activity resulting in contraction |
|
|
What happens when precapillary sphincters constrict? |
Restrict blood flow into capillaries |
|
|
What happens when precapillary sphincters dilate?
|
Blood flow into capillaries increase |
|
|
What happens if blood flow to a tissue is occluded? |
O2 levels fall and metabolic paracrines suchas CO2 and H+ accumulate in interstitial fluid |
|
|
What does local hypoxia cause? |
Causes endothelial cells to synthesize the vasodilator nitric oxide |
|
|
Most systemic arterioles are innervated by sympathetic neurons. What is an exception? |
Arterioles involved in erection reflex of penis and clitoris (controlled indirectly by parasympathetic innervation) |
|
|
What are the five "Korotkoff" sounds? |
1) Snapping sound first heart at the systolic pressure. Repetitive sounds for at least two consecutive beats is considered systolic pressure 2) Murmurs heard for most of the area between systolic and diastolic pressure 3) Loud, crisp, tapping sound 4) Sounds at pressures ~10mmHg above diastolic (described as thumping and muting) 5) Silence as cuff pressure drops below diastolic blood pressure. Disappearance of sound is considered diastolic blood pressure |
|
|
What is a sphygmomanometer? |
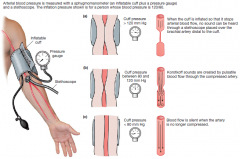
Can estimate arterial blood pressure in radial artery of arm Consisting of an inflatable cuff and a pressure gage Cuff encircles upper arm and is inflated until it exerts pressure higher than systolic pressure driving arterial blood When cuff pressure exceeds arterial pressure and blood flow into lower arm stops Then cuff pressure gradually released and when cuff pressure falls below systolic arterial blood pressure, blood pressure begins to fall again As blood squeezes through a still-compressed artery, a thumping noise called a Korotkoff sound can be heard with each pressure wave The pressure which first heard represents the highest pressure in the artery and is recorded as systolic pressure Point at which sound disappears is the lowest pressure in the artery and recorded as diastolic pressure |
|
|
What is considered normal blood pressure? |
120/80 mmHg Systolic: Less than 120 Diastolic: Less than 80 |
|
|
What is considered prehypertension blood pressure? |
(120-139) / (80-89) |
|
|
What is considered hypertension stage 1? |
(140-159) / (90-99) |
|
|
What is considered hypertension stage 2? |
(160+) / (100+) |
|
|
What is hypertensive crisis? |
Systolic over 180 and diastolic over 110 Emergency care needed Can be caused by heat stroke or head injury |
|
|
When measuring pulse, what digit should you not use and why? |
Thumb as has own pulse |
|
|
During the measurement of blood pressure, a thumping noise is heard when pressure in the cuff is: A) Higher than systolic pressure B) Lower than systolic and diastolic pressure C) Lower than systolic pressure and higher than diastolic pressure D) Higher than systolic pressure and lower than diastolic pressure |
C) |
|
|
What are four main factors that influence/determine mean arterial pressure? |
Blood volume Effectiveness of heart as pump (cardiac output) Resistance of system to blood flow Relative distribution of blood between arterial and venous blood vessels |
|
|
If flow in exceeds flow out, what happens the blood and MAP? |
Blood collects in arteries MAP increases |
|
|
In flow out exceed flow in, what happens to MAP? |
MAP decreases |
|
|
What is peripheral resistance? |
Resistance to flow offered by arterioles |
|
|
What happens to heart pump if cardiac output is increased? |
Heart pumps more blood into arteries per unit time |
|
|
If resistance to blood flow out of arteries does not change, what happens to flow, blood volume and blood pressure? |
Flow into arteries is greater than flow out Blood volume in arteries increases Arterial blood pressure increases |
|
|
If cardiac output remains unchanged but peripheral resistance increases, what happens to flow in and out, blood and arterial pressure? |
Flow into arteries is unchanged Flow out is decreased Blood accumulates in arteries Arterial pressure increases |
|
|
What factors influence arterial blood pressure? |
Distribution of blood in systemic circulation Total blood volume |
|
|
What is the rapid response in blood pressure control? |

Increase blood volume leads to increased blood pressure Triggers compensation by cardiovascular system causes vasodilation and decreased cardiac output Decrease blood pressure to normal |
|
|
What is the slow response in blood pressure control? |

Increase blood volume leads to increased blood pressure Triggers compensation by kidneys Excretion of fluid in urine to decrease blood volume Decrease blood pressure to normal |
|
|
How does the sympahetic output by alpha receptor decrease blood pressure when blood pressure is high? |

High blood pressure Increase firing of baroreceptors in carotid arteries and aorta Sensory neurons would have the cardiovascular control center in medulla oblongata cause a decrease of sympathetic output Less NE released which means less binding to alpha-receptor Anterior smooth muscle causes vasodilation Decrease peripheral resistance Decrease blood pressure Inhibits (negative feedback) of firing of baroreceptors in carotid arteries and aorta |
|
|
How does the sympahetic output by beta-1 receptor decrease blood pressure when blood pressure is high? |

High blood pressure
Increase firing of baroreceptors in carotid arteries and aorta
Sensory neurons would have the cardiovascular control center in medulla oblongata cause a decrease of sympathetic output
Less NE released which means less binding to beta-1 receptors
Ventricular myocardium would cause decrease force of contraction
Decrease cardiac output
Decrease blood pressure
Inhibits (negative feedback) of firing of baroreceptors in carotid arteries and aorta |
|
|
How does the sympahetic output by beta-2 receptor decrease blood pressure when blood pressure is high? |

High blood pressure Increase firing of baroreceptors in carotid arteries and aorta Sensory neurons would have the cardiovascular control center in medulla oblongata cause a decrease of sympathetic output Less NE released which means less binding to beta-2 receptors SA node would cause decrease heart rate Decrease cardiac output Decrease blood pressure Inhibits (negative feedback) of firing of baroreceptors in carotid arteries and aorta |
|
|
How does the parasympathetic output by ACh on muscarnic receptor decrease blood pressure when blood pressure is high? |

High blood pressure Increase firing of baroreceptors in carotid arteries and aorta Sensory neurons would have the cardiovascular control center in medulla oblongata cause a increase of parasympathetic output More ACh on muscarnic receptors SA node would cause decrease heart rate Decrease cardiac output Decrease blood pressure Inhibits (negative feedback) of firing of baroreceptors in carotid arteries and aorta |
|
|
What is the heart's response to orthostatic hypotension by sympathetic output using alpha receptors? |

Decrease mean arterial blood pressure upon standing causes a decrease of firing of carotid and aortic baroreceptors Causes cardiovascular control center in medulla to increase sympathetic output having more NE released These bind to alpha-receptors of arterioles and veins causing vasoconstriction Increase peripheral resistance Increase blood pressure to normal Negative feedback to inhibit decreased firing of carotid and aortic baroreceptors |
|
|
What is the heart's response to orthostatic hypotension by sympathetic output using beta-1 receptors? |

Decrease mean arterial blood pressure upon standing causes a decrease of firing of carotid and aortic baroreceptors
Causes cardiovascular control center in medulla to increase sympathetic output having more NE released
These bind to beta-1-receptors of ventricles causing increase force of contraction
Increase cardiac output
Increase blood pressure to normal
Negative feedback to inhibit decreased firing of carotid and aortic baroreceptors |
|
|
What is the heart's response to orthostatic hypotension by sympathetic output using beta-2 receptors? |

Decrease mean arterial blood pressure upon standing causes a decrease of firing of carotid and aortic baroreceptors Causes cardiovascular control center in medulla to increase sympathetic output having more NE released These bind to beta-2-receptors of SA node causing increase heart rate Increase cardiac output Increase blood pressure to normal Negative feedback to inhibit decreased firing of carotid and aortic baroreceptors |
|
|
What is the heart's response to orthostatic hypotension by parasymapethic output using muscarinic receptors? |

Decrease mean arterial blood pressure upon standing causes a decrease of firing of carotid and aortic baroreceptors Causes cardiovascular control center in medulla to decrease parasympathetic output having less ACh released Less to bind to muscarinic of SA node causing increase heart rate Increase cardiac output Increase blood pressure to normal Negative feedback to inhibit decreased firing of carotid and aortic baroreceptors |
|
|
What is the renal response of the renin-angiotensin aldosterone system to increase blood volume? |
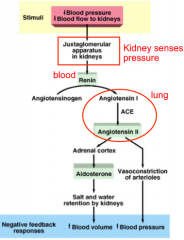
Decreased blood pressure and blood flow to kidneys
Juxtaglomerular apparatus in kidneys senses pressure
Blood renin would convert angiotensinogen into angiotensis I in lung
ACE convert angiotensin I into angiotensin II
Goes to adrenal cortex which converted into aldosterone
Causes salt and water retention by kidneys
Increase blood volume |
|
|
What is the renal response of the renin-angiotensin aldosterone system to increase blood pressure? |
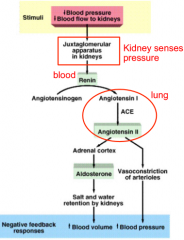
Decreased blood pressure and blood flow to kidneys
Juxtaglomerular apparatus in kidneys senses pressure
Blood renin would convert angiotensinogen into angiotensis I in lung
ACE convert angiotensin I into angiotensin II
Causes vasoconstriction of arterioles
Increase blood pressure |
|
|
If blood volume increases, what happens to blood pressure and kidney? |
Blood pressure increases Kidneys restore normal volume by excreting excess water in urine |
|
|
If blood volume decreases, what happens to blood pressure and kidney? |
Blood pressure decreases Kidneys cannot restore lost fluid, only conserve blood volume thereby prevent further decrease in blood pressure |
|
|
Artral natriuretic peptide released in response to high or low blood pressure and what does it do? |
High Produced by atria and regulates blood flow Promotes water and salt excretion Antagonizes affects of AngII Can cause vasodilation, decreased blood pressure, decreased blood volume and natriuresis diuresis |
|
|
Which of the following statements regarding the control of blood pressure is true? A) Baroreceptors in large veins increase their rate of firing due to an increase in blood pressure B) An increase in baroreceptor firing increases norepinephrine release onto arterioles C) Increased released of norepinephrine onto arterioles causes an increase in blood pressure D) An increase in parasympathetic output will cause a decrease in norepinephrine release |
C) |
|
|
What are continuous capillaries? |
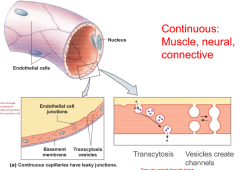
Most common capillaries
Endothelial cells joined to one another with leaky junctions
Found in muscle, connective tissue and neural tissue
Fluids move through junctions between endothelial cell junctions when they separate a bit |
|
|
What are fenestrated capillaries? |
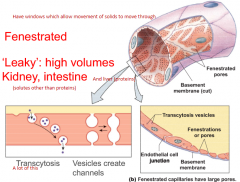
Have pores that allow high volume of fluid to pass rapidly between plasma and interstitial fluid Found primarily in kidney and intestine where associated with absorptive transporting epithelia Have 'windows' which allow movement of solids to move through A lot of transytosis |
|
|
What are the two types of capillaries? |
Continuous Fenestrated |
|
|
How do substances exchange in capillaries? |
Through capillary exchange
Exchange between plasma and interstitial fluid occurs through paracellular pathway (between endothelial cells) or endothelial transport (movement through cells)
Small dissolved solutes and gases move by diffusion or through cells depending on their lipid solubility
Larger solutes and proteins move by vasicular transport (which is active requiring ATP, example would be transcytosis) |
|
|
What is transcytosis? |
Transports large molecules (like proteins) across endothelium layer
In most capillaries |
|
|
What is interstitium? |
Space between cells |
|
|
What is interstitial fluid? |
Fluid in the interstitum Almost all are gel or gel like Very little "free fluid" under normal conditions |
|
|
What are the two major types of solid structures in the interstitium? |
Collagen fibers Proteoglycan filaments |
|
|
What are proteoglycan filaments? |
Coiled molecules composed of hyaluronic acid |
|
|
What is bulk flow? |
Mass movement of fluid as a result of hydrostatic or osmotic pressure gradients Two forces regulate bulk flow in capillaries 1) Hydrostatic pressure 2) Osmotic pressure |
|
|
What is absorption in capillaries? |
Fluid movement into capillaries |
|
|
What is filtration of capillaries? |
Fluid movement out of capillaries |
|
|
What is hydrostatic pressure of bulk flow? |
Lateral pressure compound of blood flow that pushes fluid out through capillary pores
Forces fluid out of capillary |
|
|
What is osmotic pressure of bulk flow? |
Determined by solute concentration of a compartment
Main solute different between plasma and interstitial fluid is due to proteins
Which are present in plasma but mostly absent from interstitial fluid
Created by presence of proteins known as colloid osmotic pressure (aka oncotic pressure) |
|
|
What is colloid osmotic pressure? |
AKA Oncotic pressure Creates osmotic pressure These are not equivalent to total osmotic pressure in capillary Simply a measure of osmotic pressure created by proteins Higher in plasma than interstitial fluid Osmotic gradient favours water movement by osmosis from interstitial fluid into plasma Colloid osmotic pressure of proteins within capillary pulls fluid into capillary |
|
|
What is hydrostatic pressure of interstitial fluids? |
Very low that is can be considered zero This means that water movement by hydrostatic pressure is directed out of capillary |
|
|
What determines net pressure driving fluid flow across capillaries? |

Net pressure driving fluid flow across capillary is determined by difference between hydrostatic pressure and colloid osmotic pressure |
|
|
What does a positive value for net pressure indicate? |
Net filtration |
|
|
What does a negative value for net pressure indicate? |
Net absorption |
|
|
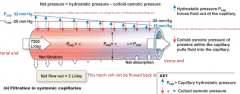
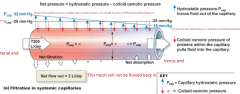
What is capillary hydrostatic pressure? |
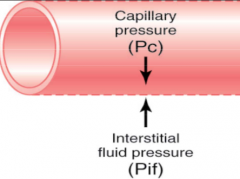
Pc Forces fluid outward through capillary membrane |
|
|
What is interstitial fluid pressure? |
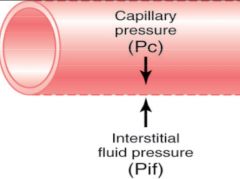
Pif Opposes filtration when value is positive Counteract Pc where it is negative |
|
|
What is plasma colloid osmotic pressure? |
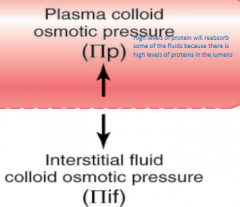
pi p/c
Opposes filtration causing osmosis of water inward through the membrane
High levels of protein will reabsorb some of the fluids because there is high levels of proteins in the lumens block |
|
|
What is interstitial fluid colloid osmotic pressure |
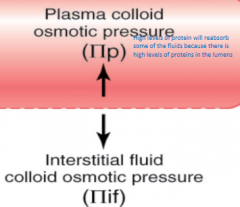
pi if Promotes filtration by causing osmosis of fluid outward through membrane Provided by interstitial fluid where proteins are found in it flowing out |
|
|
Why is interstitial fluid pressure typically negative? |
Due to removal of fluid by lymphatic system General gradient pressure dropped |
|
|
How is interstitial fluid colloid pressure kept small/low? |
By pumping of fluid into lymphatic system |
|
|
What causes plasma colloid osmotic pressure to be large? |
Presence of large proteins (osmotic pressure to favour diluting proteins) |
|
|
How do you calculate net fluid pressure? |

|
|
|
Most capillaries show transition from net filtration at the arterial end to net absorption at venous end. What are exception(s)? |
Capillaries in part of kidney filter fluid along entire length
Capillaries in intestine are only absorptive, picking up digested nutrients that have been transported into interstitial fluid form lumen of intestine |
|
|
Utilizing the data below, calculate the rate of net fluid movement across capillary wall? Pressure in mmHg: Plasma colloid osmotic pressure = 20 Capillary hydrostatic = 20 Venous hydrostatic = 5 Arterial = 80 Interstitial hydrostatic = 5 Interstitial colloid osmotic = 5 Filtration coefficient = 10 ml/min/mmHg |
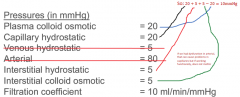
100 ml/min (filtration) |
|
|
What are lymph vessels? |
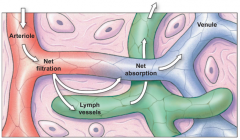
Walls that are anchored to surrounding connective tissue by fibers that hold thin-walled vessels open
In tissues, they join one another to form larger lymphatic vessels that progressively increase in size
These vessels have system of semilunar valves Largest lymph ducts empty in venous circulation just under collarbones |
|
|
What are the functions of the lymphatic system? |
Returning fluid and proteins filtered out of capillaries to circulatory system Picking up fat absorbed at small intestine and transferring it to circulatory system Serving as a filter to help capture and destroy foreign pathogens |
|
|
What is the lymphatic system? |
A route by which fluid and protein can flow from interstitial spaces to the blood
Prevent edema
Lymph is derived from interstitial fluid
Plays important role in immune system
Eventually drain into subclavin veins into heart |
|
|
What is edema? |
Unnecessary and build up on the wrong side of the membrane If there is edema, it can cause increase of pressure and cause dysfunction of tissue/organ It causes disruption of balance between filtration and absorption Increase hydrostatic pressure Decrease plasma protein concentration Increase interstitial proteins |
|
|
What are the determinants of lymph flow for degree of activity of lymphatic pump? |
Smooth muscle filaments in lymph vessel cause them to contract External compression also contributes to lymphatic pumping |
|
|
What is the determinant of lymph flow? |
Interstitial fluid hydrostatic pressure |
|
|
What happens to the lymph flow when you increase interstitial fluid hydrostatic pressure? |
Increased lymph flow |
|
|
What can cause edema? |
Inadequate drainage of lymph When filtration is a lot higher than absorption |
|
|
What is elephantiasis? |

Type of edema Abnormal enlargement of any part of the body due to obstruction of lymphatic channels in the area Caused by a small parasite roundworm, transmitted by mosquito which sides in your lymph channels |
|
|
What is ascites? |
Type of edema Fluid in the peritoneal cavity of the abdomen Caused by liver cirrhosis |
|
|
What is liver cirrhosis? |
Type of edema that causes ascites Caused by alcoholism, hepatitis, fatty liver disease and/or acetaminophen Decreased function of the liver which is the main site for plasma potential |
|
|
What is sinusoids and what does it do in the liver? |
Five times wider than capillaries Found in bone marrow, liver and spleen Sinusoid endothelium has fenestrations and there may be gaps between cells as well In liver; sinusoidal endothelium lack basal lamina which allow even more free exchange between plasma and interstitial fluid |
|
|
What causes capillary filtration? |
Caused by hydrostatic pressure that forced fluid out of capillary through leaky cell junctions |
|
|
What is the leading cause of deaths worldwide? |
Dying... well besides that cardiovascular disease 1/3 Canadian die of it 1/5 Canadian succumb to heart failure |
|
|
Which is worse when you have a higher level of: HLD or LDL? |
LDL |
|
|
What are some risk factors of cardiovascular diseases? |
Problems in circulation of lipids (too much fat in system caused by lack of exercise, diet, or uncontrollable genetics) Sex Age Family history Smoking Sedentary lifestyle Untreated hypertension Stress |
|
|
What is diabetes mellitus? |
Metabolic disorder contributes to development of atherosclerosis |
|
|
What are non-controllable risk factors for cardiovascular disease? |
Sex Age Family history |
|
|
What are controllable risk factors for cardiovascular disease? |
Smoking Obesity Sedentary lifestyle Untreated hypertension Untreated cholesterol Stress |
|
|
What is artherosclerosis? |
Build-up of fatty material (mainly cholesterol under the inner lining of arteries) called plaque Plaque can cause a thrombus (blood clot) to form This can dislodge and circulate as a large clot (thromboembolism) |
|
|
What are the steps in developing artherosclerosis of LDL and plaque? |
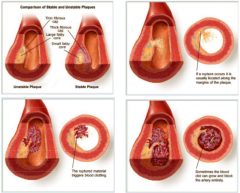
1) LDL-cholesterol accumulates between the endothelium and connective tissue and is oxidized 2) Marcophages ingest cholesterol and become foam cells 3) Smooth muscle cells, attracted by macrophage cytokines, begin to divide and take up cholesterol 4) Lipid core accumulates beneath endothelium 5) Fibrous scar tissue forms to wall off lipid core 6) Smooth muscle cells divide and contribute to thickening of intima 7) Calcification are deposited within plaque 8) Macrophages may release enzymes that dissolve collagen and convert stable plaques to unstable plaques 9) Platelets that are exposed to collagen activate and initiate a blood clot |
|
|
What is ischemic heart disease? |
An imbalance between supply of oxygen and myocardial demand resulting in "myocardial ischemia" |
|
|
What is arrhythmia? |
Poor rhythms in the heart which can cause inappropriate contractions and increased clots |
|
|
What are the diagnosis for acute myocardial infarction? |
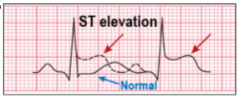
Typical chest pain
Electrocardiographic changes of ST elevation (whole heart function has change and heart struggling to function properly) Myocardial enzyme elevation of creatine kinase (CK-MG) and troponin |
|
|
What are some medical treatments for acute myocardial infarction? |
Rest, oxygen, analgesia (pain killer) and aspirin
Thrombolysis
Primary angioplasty
Beta blockers
ACE inhibits (blocking formation of angiotensin) |
|
|
What is primary angioplasty? |
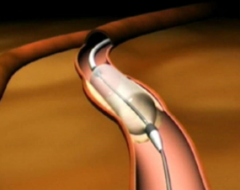
Balloon to open up blood vessel which push walls of arteries back |
|
|
What do beta-blockers do? |
Reduced sympathetic outflow Causes heart to rest a little fraction more and recover from heart attack Does not allow heart rate to go up |
|
|
Why is doing a coronary artery stent or coronary artery bypass graft dangerous? |
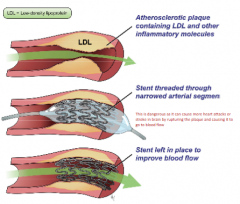
This is dangerous as it can cause more heart attacks or stroke inbrain by rupturing the plaque and causing it to go to blood flow |
|
|
What are the causes the myocardial infraction? |
Heart disease Hypertension Electrolyte imbalance |
|
|
What is hypertension? |
Sustained elevated arterial pressure of 140/90 or higher Transient elevations are normal and can be caused by fever, physical exertion and emotional upset Chronic elevation is a major cause of heart failure, vascular disease, renal failure and stroke Can cause damage to cerebral blood vessels and lead to stroke (clot/ischemia or hemorrhage), increased cardiac load leading to hypertrophy, contributes to atherosclerosis and pressure imbalances |
|
|
What is hypotension? |
Low BP in which systolic pressure is below 100mmHg |
|
|
What are the consequences of hypertension? |
Damage to cerebral blood vessels and lead to stroke (clot/ischemia or hemorrhage) Increased cardiac load leading to hypertrophy Contributes to atherosclerosis Pressure imbalances |
|
|
How do you treat hypertension? |
Calcium channel blockers Diuretics Beta-blocker ACE inhibitors |
|
|
What is orthostatic hypotension? |
Temporary low BP and dizziness when suddenly rising from a sitting or reclining position |
|
|
What is chronic hypotension? |
Can be caused by poor nutrition Warning sign for Addison's disease (a adrenal cortex defect) |
|
|
What is acute hypotension? |
Important sign of circulatory shock Threat to patients undergoing surgery and those in intensive care units |
|
|
What is circulatory shock? |
Too little blood in vessels to supply organs |
|
|
What is hypovolemic shock? |
Type of circulatory shock Blood loss |
|
|
What is anaphylaxis? |
Type of vascular shock which is a type of circulatory shock Histamine-based allergies |
|
|
What is septicemia? |
Type of vascular shock which is a type of circulatory shock
Systemic infection |
|
|
What is cardiogenic? |
Type of circulatory shock Infarcted heart |
|
|
What are the signs and symptoms of circulatory shock? |
Systolic BP below 90 Resting tachycardia Weakpulse Cool, pale, clammy skin Altered mental state, confused Reduce urine formation Thirsty Acidosis (lactic acid build-up) Nausea (reduced blood flow to digestive tract) |
|
|
What are the functions of blood? |
Regulates body temperature by absorbing and redistributing heat out of body Transports gases, nutrients, hormones and metabolic waste Regulates composition of interstitial fluid Restricts fluid loss at injury sites via blood clotting Defends against toxins and pathogens |
|
|
What does plasma mostly consist of? |
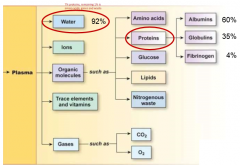
92% water |
|
|
What protein is mostly found in plasma? |
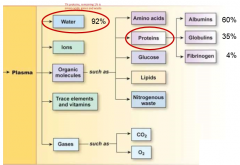
Albumins
|
|
|
What are the functions of plasma proteins? |
Generate colloid osmotic pressure Buffer pH Transport/carriers |
|
|
What is the function of albumins? |
Colloid osmotic pressure Carriers |
|
|
What is the function of alpha and beta globulins as a plasma protein? |
Clotting factors Enzymes Carriers |
|
|
What is the function of gamma globulins as a plasma protein? |
Antibodies |
|
|
What is the function of fibrinogen as a plasma protein? |
Forms fibrin for blood clotting |
|
|
What is the function of transferring as a plasma protein? |
Iron transport |
|
|
What type of dye does neutrophils take up? |
Neutral dye |
|
|
What type of dye does eosinophils take up? |
Acidic dye |
|
|
What type of dye does basophils take up? |
Basic dye |
|
|
What is the most common type of white blood cell? |
Neutrophils |
|
|
Where do white blood cells come from? |
Prenatal: Yolk sac, liver, spleen and bone marrow Postnatal: Bone marrow Adults: Pelvis, spine, ribs, cranium proximal end long bones |
|
|
What is haematopoiesis? |
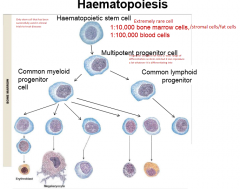
Blood formation
|
|
|
What is a haematopoietic stem cell? |
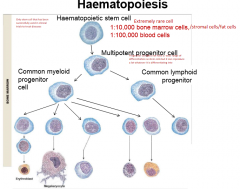
Extremely rare cell First cell in haematopoiesis Only stem cell that has been successfully used in clinical trials to treat disease |
|
|
What are multipotentent progenitor cells? |
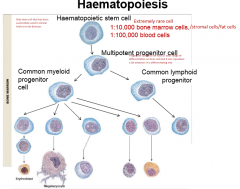
Progenitor cell does not have a wide range of differentiation as stem cells but it can reproduce a lot whatever it is differentiating into |
|
|
What regulates haematopoiesis? |
Cytokines such as CSFs and IL Hormones such as EPO and TPO |
|
|
What are colony stimulating factors (CSFs)? |
Stimulating formation of colonies from one homeostatic stem cell From endothelial cells and white blood cells |
|
|
Where are interleukin (ILs) released from? |
White blood cells |
|
|
Where are erthropoietin (EPO) released from?
|
Kidneys |
|
|
Where are thrombopoietin (TPO) released from? |
Liver |
|
|
What do the hormones EPO and TPO do? |
Support the differentiation along lineages to increase numbers of cells for proliferation |
|
|
What does erthyropoietin cause differentiation of? |
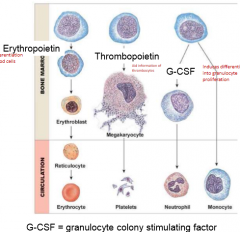
Common myeloid progenitor cell into erythroblasts into erhyrocytes (red blood cells) |
|
|
What does thrombopoietin cause differentiation of? |
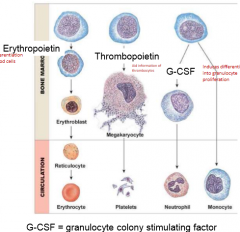
Common myeloid pregenitor cell into megakaryocytes to platelets |
|
|
What does ganulocyte colony stimulating factor cause differentiation of? |
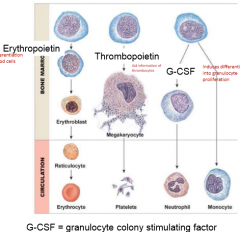
Common myeloid pregenitor cell into neutrophils (and other ganulocytes) |
|
|
Which protein is most abundant in plasma? B) Albumins C) Antibodies D) Fibrinogens |
B) |
|
|
List all of the types of formed elements that are found in blood |
Erythrocytes, neutrophils, monocytes, platelets, basophils,eosinophils, T lymphocytes, B-lymphocytes, NK cells |
|
|
What are red blood cells (RBCs)? |
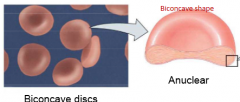
Anuclear (in mammalanian) sac of hemoglobin and enzymes Essentially bags filled with haemoglobin and enzymes No mitochondria = anaerobic metabolism No nucleus = no new trasncription |
|
|
What does band 3 tetramer of red blood cells to? |

Link onto ankyrin which is a nexus for a long spectrin filamentswhich form a meshwork on the inside of the membrane which are linked togetherby actin This allows them to move through tighter and tighter places (flexible) No nucleus so any damage to them cannot be fixed and they have a short life span |
|
|
What is haemoglobin (Hb)? |
Protein made up of globin protein Most adult haemoglobin is HbA (2 alpha chains, 2 beta) Has iron in the middle in it that exchanges the oxygen for you |
|
|
What causes sickle cell anemia (relating to blood cells, not parasite)? |
Due to sickle cell haemoglobin (HbS)
Made up of the two alpha chains but there is a mutation at the betachain at one gene
Whenever HbS release oxygen, it causes changes/polymerizes at the abnormal chain and gives itself the sickle shape
When sickle goes through small capillaries, they start to rip andtear itself and tissue causing bleeding, pain and other results |
|
|
What causes the spikes of hypertonic solution red blood cell? |
Cytoskeleton |
|
|
What is erythropoiesis? |

Regulated by erythropoietin Erhyropoietin synthesized and released from kidney in response to low oxygen Nucleus ejected, mitochondria and endoplasmic reticulum breakdown |
|
|
What are the steps of erythropoiesis? |

Day 1) Proerythroblast (a blast is an immature form of a cell) Day 2) Basophilic erythroblasts Day 3) Polychromatophilic erythroblast Day 4) Normoblast (last stage has nucleus) Day 5-7) Ejection of nucleus and becomes a reticulocyte (looks like it has a meshwork or lattice to it which is the end ofthe RNA making the last of the proteins it can make) Enters circulation as a mature red blood cell |
|
|
What is jaundice? |
Hyperbilirubinemia High levels of yellow (bilirubin) in you High turnover of red blood cell Liver disease Bile duct obstruction |
|

Jessica is a newborn baby who has yellow skin and sclera What condition does she have? |
Neonatal jaundice |
|

Jessica is a newborn baby who has yellow skin and sclera How can she be treated? |

Can be treated with blue light (420-470) in a lamp or blanket form (phototherapy) |
|
|
What is anemia? |
Reduced quality or quantity of red blood cells Decreased production, increased removal |
|
|
What are the symptoms of anemia? |
Irritability Fatigue Dizziness, light-headedness, rapid heartbeat |
|
|
What can cause low production of red blood cells? |
Destruction of stem cells via drugs and radiation (aplastic anemia) Inadequate nutrients: iron, folic acid, vitamin B12 (iron deficiency anemia, folate deficiency anemia, pernicious anemia) Low erythropoietin (renal anemia) |
|
|
What causes hemolytic anemia? |
Genetics (defects in RBC proteins)
Parasitic infection Drugs Autoimmune reactions (antibodies being made in response in low temperature which attackyour red blood cells) |
|
|
What causes hemorrhagic anemia?
|
Excessive blood loss |
|
|
What is polycythemia? |
High numbers of RBCs High blood viscosity Increased production of RBCs |
|
|
What causes polycythemia vera? |
Primary polycythemia: abnormal erythrocyte precursors Secondary polycythemia: low oxygen delivery to tissue |
|
|
What causes relative polycythemia? |
No pathology, due to reduced plasma volume
Dehydration |
|
|
What are the components of the immune system and what do they do? |
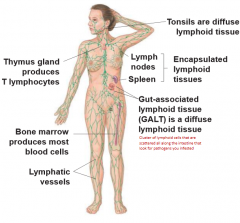
Thymus gland: produces T lymphocytes Bone marrow: produces most blood cells Lymphatic vessels Tonsils: diffuse lymphoid tissue Lymph nodes and spleen: Encapsulated lymphoid tissues Gut-associated lymphoid tissue (GALT): diffuse lymphoid tissue |
|
|
What do secondary lymphoid tissue contain? |
Mature immune cells that interact with pathogens and initiate an immune response |
|
|
Which white blood cell is specialized for fighting against parasitic worms? |
Eosinophils |
|
|
What do natural killer (NK) cells generally do? |
Destroy cells by releasing factors |
|
|
What does antimicrobial proteins generally do? |
Punch holes in bacteria |
|
|
What do inflammation generally do in an innate immune response? |
Wall of an area where infection might occur |
|
|
What does a fever generally do in a innate immune response? |
Make environment more hostile to pathogens |
|
|
What is diapedesis? |
Immune cell would flatten out and squeeze through cells |
|
|
How do pathogens detect infectious/bacterial cells? |

By using pattern recognition receptors (PRP) such as Toll-like receptors to detect PAMPs on pathogens |
|
|
What is opsonization? |

Using Fc receptors on a phagocytosis immune cell, it would created a bridge like formation with the antibodies that attached itself to a polysaccharide capsule of a pathogen |
|
|
What are opsonins? |
Molecules that coat a pathogen and act as a physical bridge betweenpathogen and phagocyte |
|
|
How does a macrophage and dendritic cell display antigen fragments? |
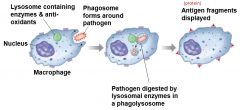
Phagosome form around pathogen Pathogen digested by lysosomal enzymes in phagolysosome Antigen fragments displayed |
|
|
What is the function of opsonins? A) Digest invading cells B) Mark pathogens for phagocytosis C) Bind to Toll-like receptors D) Promote diapedesis |
B)
|
|
|
How do natural killer (NK) cells detect virally-infected or cancerous cells? |
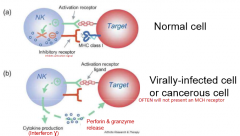
If a target cell presents an activation receptor ligand but not an MHC class ligand, the NK cell would have cytokin production and release of interferon gamma (signals for more lymphocytes into area) as well as perforin and granzyme to kill cell |
|
|
What does interferon gamma do? |
Signals for more lymphycocytes into area Released by NK cells |
|
|
What are antimicrobial proteins? |
Interferons Released by host cells in response to presence of pathogens (IFN alpha, beta and gamma) Enchance phagocytosis Attract phagocytes Stimulate inflammation Destroy target cell membranes |
|
|
What do IFN alpha and beta do? |
Prevent viral replication in cells |
|
|
What do IFN gamma do? |
Activate macrophages and other immune cells |
|
|
What is the classical pathway of complement? |
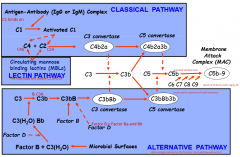
Anti-gen antibody (IgG or IgM) complex C1 binds on which will be activated Turn C4 and C2 into C4b and C2a which combines to create C3 convertase (C4b2a) This will turn C3 into C3b which will combine with C3 convertase into C5 convertase (C4b2a3b) which will turn C5 into C5b C5b will activate and bind to C6, C7 (inserts itself into cell wall/membrane), C8 and C9 (bunch of C9 which will form a ring by C8) to created membrane attack complex, MAC (C5b-9) |
|
|
What is the lectin pathway of complement? |
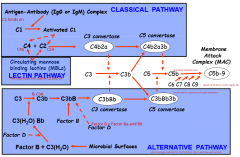
Circulating mannose binding lectins (MBLs) will convert C4 and C2 into C4b and C2a which combines to create C3 convertase (C4b2a) This will turn C3 into C3b which will combine with C3 convertase into C5 convertase (C4b2a3b) which will turn C5 into C5b C5b will activate and bind to C6, C7 (inserts itself into cell wall/membrane), C8 and C9 (bunch of C9 which will form a ring by C8) to created membrane attack complex, MAC (C5b-9) |
|
|
What is the alternative pathway of complement? |
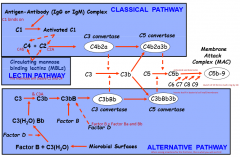
When seeing a bacteria for the first time, this is what happens Microbial surfaces will activate Factor B + C3(H2O) Factor D will convert this into C3(H2O) Bb which converts C3 into C3b and C3a where C3b will turn into C3bB C3bB with Factor B and Factor D will turn into C3 convertase (C3bBb) C3 convertase will turn C3 into C3b which will bind with C3b to turn into C5 convertase (C3bBb3b) This will convert C5 into C5b C5b will activate and bind to C6, C7 (inserts itself into cell wall/membrane), C8 and C9 (bunch of C9 which will form a ring by C8) to created membrane attack complex, MAC (C5b-9) |
|
|
Which of the following is NOT a role for complement proteins? B) Cause inflammation C) Form part of the membrane attack complex D) Activate apoptosis in host cells |
D) |
|
|
What is inflammation? |
Localized tissue response to injury producing Causes swelling, redness, heat and pain Roles are slowing the spread of pathogens, mobilization of local, regional and systemic defenses and sets the stage for repair |
|
|
How does the inflammatory response work? |
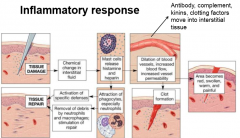
When there is tissue damage, there will be a chemical change in interstitial fluid This causes mast cells to release histamine and heparin. This does two things 1) Attraction of phagocytes (activation of specific defenses), especially neutrophils (removal of debris by neutrophils and macrophages; stimulation of repair) This causes tissue repair 2) Dilation of blood vessels, increased blood flow, and increased vessel permeability This causes area to become red, swollen, warm and painful as well as clot formation |
|
|
What is a fever? |
Body temperature above 37.2 C |
|
|
What causes fever? |
Pyrogens change the thermoregulatory set point in the hypothalamus |
|
|
What are the roles of a fever? |
Speeds up metabolic activity of host Inhibits some pathogens |
|
|
Which is the first cell to exit the bloodstream during inflammation? A) Macrophage B) Neutrophil C) Dendritic cell D) Mast cell |
B) |
|
|
How is specificity of acquired immunity achieved? |
Responds to a specific antigen
Both B and T cells have receptors that recognize specific antigen |
|
|
How is memory of acquired immunity achieved? |
"Remembers" any antigen it has encountered (identifies a substance) Some activated B and T cells are long lasting |
|
|
How is tolerance of acquired immunity achieved? |
Responds to foreign substances but ignores normal tissue B and T cells with receptors that recognize self are deleted or not activated |
|
|
What is humoral immunity? |
B cell receptors bind to extracellular antigen |
|
|
What is cell-mediated immunity? |
T cell receptors bind to antigens (which must have MHCs) displayed on surface of cells |
|
|
What are MHCs and are they found in humans? |
Major histocompatbility complex No, humans have human leukocyte antigens (HLA) |
|
|
What is clonal selection and expansion of B- and T-cells? |
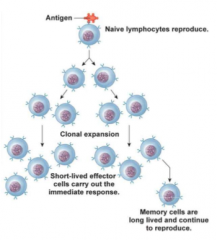
Antigen binds to B- and/or T-cell (selection) and it starts producing naive lymphocytes (expansion) |
|
|
What are memory cells? |
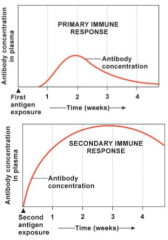
Memory comes in where some of these cells become effector cells andbe able to come in and destroy pathogen while others become memory cells wherethey leave the cell cycle and are long lasting They are long lived and continue to reproduce |
|
|
Where do B- and T- lymphocytes originate from? |
Bone marrow |
|
|
What is tolerance of B cells? |
Undergo negative selection in bone marrow Process of negative selection where theypresent antigens to B cells where if the B cells bind, it will initiateapoptosis and cell death |
|
|
What is tolerance of T cells? |
T cells undergo positive and negative selection in the thymus For T cells, they undergo both positive and negative selection wherethey will present only MHC to one with functional receptors and if T cellsbind, that good Then second test, if they cannot pull off the second MHC, it will be marked for apoptosis |
|
|
What identifies the class of an antibody? |
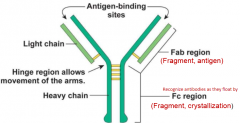
Heavy chain |
|
|
How is antibody diversity generated? |
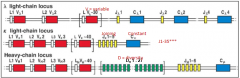
Variable region makes up antigen binding site which is made up of anumber of gene segments that is a combination of VJC (or VDJC for heavy) |
|
|
What are the steps of somatic recombination for light and heavy chain? |
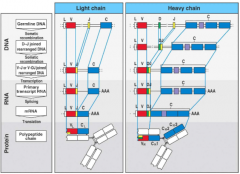
DNA: 1) Germline DNA 2) D-J joined rearranged DNA 3) V-J or V-DJ joined rearrange DNA RNA: 4) Primary transcript RNA 5) mRNA Protein: 6) Polypeptide chain |
|
|
How are B-cells activated and then what happens? |

B cells start to become activated when they encounter antigen
Antigen is internalized, combined with MHC II and then transported to cell surface
Helper T cell recognizes antigen and MHC II
After binding to MHC, it express the CD40L (ligand) which will then bind to CD40 which causes the release of cytokines (IL 4,5,6)
Activated B cells divide and some become plasma cells and secrete antibodies, others become memory B cells |
|
|
What are plasma cells? |
Secrete antibodies |
|
|
The following are steps in activation of B cells. Put the steps in correct order: 1) Some B cells differentiate into plasma cells 2) Plasma cells secrete antibody 3) T cell secrete cytokines 4) Antigen is internalized by B cell 5) Antigen is presented on MHC molecule on B cells 6) Antigen binds to B cell receptor 7) T cell recognizes antigen on B cells |
6,4,5,7,3,1,2 |
|
|
What is IgG? |

A class of antibodies Most common type of circulating antibody Transferred across placenta from mother to baby Whenever IgM is present, IgG will not be produced |
|
|
What is IgM? |

Class of antibodies First type of antibody to be secreted in response to a new antigen Good at causing antigen clumping for removal Activates complement |
|
|
What is IgA? |
Class of antibodies Crosses epithelial cells Protects epithelial surfaces and present in breast milk First antibody introduced into a new born |
|
|
What is IgE? |

Fights parasites Eosinophils have receptors for the IgE Release histamine from mast cells |
|
|
What is IgD? |
Role unclear |
|
|
In a routine examination, some blood is taken and analyzed. The results show a high IgM level for the mumps antigen. What does this indicate about the person? A) Has just recovered from mumps B) Is just coming down with mumps C) Is allergic to mumps D) Has being exposed to mumps for second time |
B) |
|
|
What are acute phase proteins? |
Plasma proteins always in the blood and isresponse to invasion |
|
|
What are c-reactive peptides? |
Opsins |
|
|
What are hepcidin? |
Hormone that produce that limits iron available into body (which bacteria need to live) |
|
|
In exercising muscles, an increase in blood flow allows appropriate oxygen and nutrients to sustainactivity. This event is called ___________ and is caused by local artery ___________ to___________________ generated from ___________________. A ) active hyperemia; vasodilation; high carbon dioxide; tissue metabolism B ) active hyperemia; vasodilation; low oxygen; an occlusion C ) reactive hyperemia; vasodilation; high carbon dioxide; an occlusion D ) reactive hyperemia; vasoconstriction; high oxygen; tissue metabolism |
A) |
|
|
Which of the following is not a protein found in plasma? A ) Albumin B ) Globulins C ) Carbonic anhydrase D ) Fibrinogen |
C) |
|
|
Which ONE of the following statements is FALSE about hypertension? A ) Hypertension is a risk factor for many other cardiovascular diseases B ) The cause of essential hypertension is well known C ) The baroreceptors reset to accept elevated blood pressures D ) Blood pressure gets progressively higher with age. |
B) |
|
|
Which ONE of the following statements about capillary fluid exchange across the length of acapillary is true? A ) Capillary hydrostatic pressure forces fluid into the capillary, plasma colloid osmotic pressureforces fluid out B ) At the centre of the capillary, capillary hydrostatic pressure is equal to plasma colloid osmoticpressure C ) At the arterial end, absorption exceeds filtration D ) Capillary hydrostatic pressure stays the same, but plasma colloid osmotic pressure decreases |
B) |
|
|
What cell is NOT found in the bone marrow during normal haematopoiesis? A ) Dendritic cells B ) Reticulocytes C ) Normoblasts D ) Megakaryocytes |
A) |
|
|
The specificity of an antibody is determined by: A ) The antibody binding sites B ) The antibody class C ) The Fc region D ) The variable region |
D) |
|
|
Identify the correct statement about the heart valves: A ) During ventricular contraction, the mitral valve remains open B ) The valves in the heart ensure that blood moves in one direction C ) The heart has two semilunar valves and two bicuspid valves D ) The aortic valve is attached to the chordae tendinae |
B) |
|
|
Which ONE of the following properties contribute to the decrease in blood pressure from~93mmHg in the aorta to ~40mmHg in the capillaries? A ) The increase in resistance provided by the arterioles B ) The ability of arterioles to vasodilate C ) The number of endothelial cells that line the capillaries D ) The smaller cross sectional area of capillaries |
A) |
|
|
In the cardiac cycle, the ________ initiates _____________ in the left ventricle that results in_________________ ventricle pressure and ___________ ventricular volume A ) QRS complex; isovolumetric contraction; increased; unchanged B ) P wave; diastole; reduced; reduced C ) T wave; isovolumetric relaxation; increased; unchanged D ) QRS complex; ventricular systole; decreased; increased |
A) |
|
|
Which parameter CANNOT be calculated based on knowing the value of the following factors:end diastolic volume, end systolic volume, heart rate, and peripheral resistance? A ) Mean arterial pressure B ) Cardiac output C ) Diastolic blood pressure D ) Stroke volume |
C) |
|
|
Identify the correct statement regarding the immune response to extracellular bacteria: A ) The complement system can be activated by IgM, IgG, and IgA B ) Macrophages release bradykinin during inflammation, causing the sensation of pain C ) Clonal selection of B cells generally results in the production of two types of clones: plasmacells and memory cells D ) C-reactive protein is an acute phase protein released from neutrophils that acts as an opsoninwhen bound to bacteria |
C) |
|
|
Aortic stenosis is characterized by stiffening of the aorta, causing it to become less flexible. WhichONE of the following events DOES NOT occur in a patient with aortic stenosis? A ) Shifting of the pressure-volume relationship to greater left ventricular pressures B ) Impairment of the Windkessel effect resulting in greater cardiac afterload C ) Reduced contribution of the aorta to the movement of blood during ventricular relaxation D ) Increased venous return causing greater stroke volume |
D) |
|
|
Identify the correct statement about the relationship between pressure, resistance, and blood flow inthe body: A ) Vessel radius is the only determinant of vascular resistance B ) In large straight arteries, blood flow is essentially silent C ) Mean arterial pressure is the same throughout the body and it does not matter which artery ismeasured D ) The maximal pressure developed by the heart is the only parameter that determines thedriving force of blood through the circulation |
B) |
|
|
For leukocytes to battle an infection, adhesion molecules are necessary including ______, whichloosely binds leukocytes to the blood vessel wall to slow down their movement, and ________which tightly attaches leukocytes to the vessel wall in preparation for diapedesis. A ) Integrin; spectrin B ) Spectrin; integrin C ) Selectin; integrin D ) Integrin; selectin |
C) |
|
|
Which statement is true in regards to the anatomical organization of the cardiovascular system? A ) Arteries only carry oxygenated blood B ) Veins only carry de-oxygenated blood C ) Once blood passes through one organ, it travels directly to the heart D ) Blood from the coronary veins feed into the right atrium |
D) |
|
|
Identify the statement that is NOT TRUE about the left atrium in the cardiac cycle: A ) When the left atrium contracts left ventricular volume increases B ) The P wave occurs just prior to contraction of the left atrium C ) Atrial diastole occurs just prior to ventricular systole D ) Contraction of the left atrium occurs just prior to closing of the mitral valve. |
C) |
|
|
You and your friends decide to go camping in Algonquin park over the weekend. One evening, yougo for a walk and on the way back to your campsite, you notice a black bear lurking around yourtent. Being frightened, your cardiac system responds by: A ) Closing voltage-gated calcium channels and reducing calcium entry B ) Reducing phosphorylation of phospholamban and inactivating calcium ATPase on thesarcoplasmic reticulum C ) Releasing epinephrine/norepinephrine to bind alpha1 receptors on the heart D ) Increasing calcium release from the sarcoplasmic reticulum and shortening calcium-troponinbinding time |
D) |
|
|
In the left ventricular pressure-volume relationship (the pressure-volume loop), which statement is FALSE? (Hint: Drawing the pressure-volume graph may help).
A ) A perfectly horizontal line represents passive ventricular filling
B ) Isovolumetric events occur when the mitral valve is open
C ) Ejection of blood into the aorta is shown by reduced ventricular volume
D ) Vertical lines represent isovolumetric ventricular events |
B) |
|
|
Which statement is INCORRECT with respect to red blood cells? A ) Glycolysis is their primary source of ATP B ) They migrate into infected regions of tissue in response to cytokines C ) Erythropoietin regulates their differentiation from common myeloid progenitor cells D ) Ankyrin links the cytoskeleton to the plasma membrane |
B) |
|
|
Many elderly people get light-headed and dizzy upon standing up after prolonged sitting. Thiscondition is termed orthostatic hypotension. Which of the following responses may contribute tothis condition? A ) Reduced activation of the muscarinic receptors in the SA node B ) An increased sympathetic output leading to norepinephrine release C ) Increased activation of the parasympathetic system D ) Increased B1- receptor activation in the ventricles |
C) |
|
|
Identify the INCORRECT sequence of blood flow through the heart: A ) Aorta, right atrium, left atrium B ) Superior vena cava, tricuspid valve, pulmonary semilunar valve C ) Pulmonary veins, left atrium, aortic semilunar valve D ) Inferior vena cava, left ventricle, bicuspid valve |
D) |
|
|
As a medical resident, you are asked to assess a patient who has edema. You are given a catheterand a manometer, allowing you to assess pressure in various tissue compartments. What results areyou likely to find that supports the diagnosis of edema? A ) Decreased plasma colloid osmotic pressure B ) Increased arterial and venous pressures C ) Plasma colloid osmotic pressure exceeds hydrostatic pressure D ) Capillary fluid absorption exceeds capillary fluid filtration |
A) |
|
|
How do natural killer cells specifically target virally-infected cells? A ) Kill cells that present viral antigens in combination with MHC class I B ) Kill cells that secrete interferon C ) Kill cells that present viral antigens in combination with MHC class II D ) Kill cells that lack MHC class I |
D) |
|
|
Identify the true statement about movement of blood through arteries: A ) Resistance increases as radius increases B ) Resistance increases as radius decreases C ) Resistance decreases as length increases D ) Resistance increases as viscosity decreases |
B) |
|
|
When relaxing at the beach after your exam, you notice that a fellow swimmer has stepped on apiece of broken glass and is bleeding heavily from their foot. Although this is a serious injury, theinjured swimmer is fully conscious and able to place a phone call to emergency services. Youcorrectly reason that, despite the loss of blood volume, they still have adequate blood pressure tomaintain brain function. What compensatory mechanisms contribute to this relatively normal bloodpressure? A ) Decreased heart rate, increased baroreceptor firing B ) Decreased sympathetic nerve activation, decreased breathing rate C ) Aldosterone release, anti-diuretic hormone release D ) Increased kidney blood flow, increased urine output |
C) |
|
|
Which statement is FALSE about cardiac contractile cells? A ) Calcium entry through L-type channels initiate calcium-induced calcium release B ) Cardiac contractile cells have a graded contraction to stimulation C ) The sodium/calcium exchanger and the sodium/potassium ATPase work together to restoreion gradients D ) The short cardiac contractile cell refractory period is short to allow tetanus to occur |
D) |
|
|
As an emergency physician, you routinely use an electrocardiogram (ECG) to check the heart function of your patients. One evening, you identify a patient with atrial fibrillation. Which of the following ECG parameters would identify this condition?
A ) Multiple P waves
B ) Absence of a P wave
C ) Absence of a QRS complex
D ) Absence of a T wave |
B) |
|
|
You have had a sore tooth for several days and decide to visit your physician. She orders adifferential white cell count to be done on your blood and from that, determines you have anabscessed tooth due to a bacterial infection. What type of white blood cell would be expected to beelevated in this analysis? A ) Monocytes B ) Eosinophils C ) Neutrophils D ) Lymphocytes |
C) |
|
|
Individuals taking a particular anticoagulant must ensure that their daily consumption of vitamin K remains relatively constant. What is the name of the anticoagulant?
A) Protein C
B) Coumadin
C) Heparin
D) Aspirin |
B) |
|
|
Asa child, Lucia who is Rh negative was mistakenly transfused with Rhpositive blood. She is now expecting her first child with an Rh positivepartner. Should her doctors be worried about her pregnancy? A) Yes, because if she is injected with anti-D antibodies they will attack the antibodies that she already has in her blood. B) No, because there is no risk of the fetal blood mixing with the maternal blood C) No, because the gene encoding for the D antigen is recessive so there is no chance that her fetus is Rh positive D) Yes, because she developed immunological memory to the D antigen as a child |
D) |
|
|
What percentage of resting cardiac output do the kidneys receive? 1) 16% B) Less than 1% C) 35% D) 20% |
D) |
|
|
The primary function of the kidneys involves regulating the _______ andthe _______ of plasma and interstitial fluid. A) Temperature; composition B) Volume; composition C) Pressure; volume D) Composition; osmolarity |
B) |
|
|
In order to enter Bowman's space, plasma is filtered as it moves acrossthe endothelial cell, through the _______ and eventually across the _________. A) Podocyte; basement membrane B) Basal lamina; macula densa C) Basal lamina; podocyte D) Podocyte; granular cell |
C) |
|
|
What are T-cell receptors? |
Inserted into cell membranes of immature precursor T-lymphocyte cells Not antibodies like receptors on B-lymphocytes Can bind only to MHC-antigen complexes on surface of an antigen-presenting cell |
|
|
What are MHC proteins? |
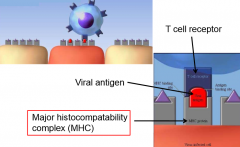
Family of membrane protein complexes encoded by a specific set of genes
Every nucleated cell of body has MHC proteins on its membrane
MHC proteins combine with fragments of antigen that have digested within the cell
MHC-antigen complex is then inserted into cell membrane so that antigen is visible on extracellular surface
Free antigen in extracellular fluid cannot bind to unoccupied MHC receptors on cell surface
Two classes: MHC 1 and 2 |
|
|
What are Cytotoxic T cells? |
TC cells CD8 which bind to TCR onto MHC-1 and antigen on an infected cell Kill infected/cancerous cells It prevent reproduction of intracellular invaders such as viruses, some parasites and some bacteria when cells infected by these pathogens are targeted for destruction Two way to kill their targets: 1) Release cytotoxic pore-forming molecules called perforin and granzymes These enzymes related to digestive enzymes trypsin and chymotrypsin When granzymes enter target cell through perforin channels, they active an enzyme cascade that induces cell to commit suicide (apoptosis) 2) Instruct target cells to undergo apoptosis Activating Fas (death receptor protein) on target cell membrane |
|
|
What are Helper T cells? |
CD4 (can use flow cytometry and an antibody bounded to it to analyze helper T cells)
Bind to MHC-2 and antigen
Release cytokines (interferon-gamma, interleukins, colony-stimulating factors)
Activate T and B cells
Can bind to B cells and promote their differentiation into plasma cells and memory B cells |
|
|
What does interferon-gamma generally do? |

Activate macrophages Causes polarization of Naive TH cells into TH1 effector cells |
|
|
What do interleukin generally do? |
Activate antibody production and cytotoxic T lymphocytes Support actions of mass cell and eosinophils |
|
|
What are MHC class 1 (MHC-I)? |
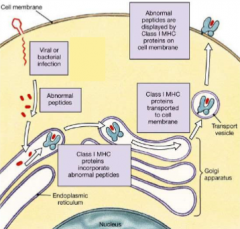
Binds to an intercellular antigen that is located in the cytosol ofthe cells such as abnormal protein that cancerous cell produce or the protein capsule of viruses
Located on all nucleated cells
Present endogenuous antigen
When viruses and bacteria invade cell, they are digested into peptide fragments and loaded onto MHC-I "platforms" Activate TC cells where TC cell recognizes the target as either a virus-infected cell or as a tumor cell and kills it to prevent it from reproducing |
|
|
How does activation of TC cells happen? |
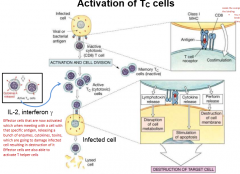
Infected cell will present viral or bacterial antigen Inactive cytotoxic T cell with a CD8 would recognize the infected cell by MHC-1 with antigen (binds to T cell receptor Causes activation and cell division of cytotoxic T cell of active and memory (inactive) TC cells. These cells can activate activate T helper cells Active TC cells bind to infected cell by MHC-1 with antigen to T-cell receptor, causing release of lymphotoxin, cytokine and perforin Cause cell to be lysed/destroyed |
|
|
In the activation of Tc cells, what does the CD8 do? |
Holds the complex in place to stabilize the binding |
|
|
In the activation of Tc cells, when is lymphotoxin released and what does it do? |
Released when activate Tc cells bind to infected cell Causes disruption of cell membrane |
|
|
In the activation of Tc cells, when is perforin released and what does it do? |
Released when activate Tc cells bind to infected cell Causes destruction of cell membrane |
|
|
What is MHC class 2 (MHC-II)? |
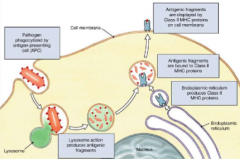
Located on dendritic cells, macrophages and B cells (antigen-presenting cells)
Present exogenous antigen
When immune cell engulfs and digests antigen, fragments return to immune cell membrane combined with MHC-2 proteins
Activate TH cells |
|
|
What is the helper T cell response when encountering an APC with foreign antigen fragment on its MHC-2? |
THcell responds by secreting cytokines that enhance immune response |
|
|
How are helper T cells activated? |
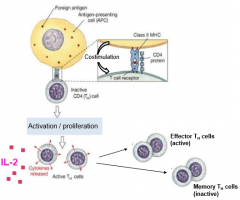
An inactive TH cell with an CD4 binds to a infected cell presenting an MHC-2 with an antigen and costimulation Causes activation and proliferation of effector (active) and memory (inactive) TH cell Effector/active TH cells release the cytokine IL-2 THs then coordinate activity of TH, TC and B cells (does not destroying pathogen itself) |
|
|
What does IL-12 do? |

Causes polarization of naive TH cells into TH1 effector cells |
|
|
What does IL-4 do? |

Causes polarization of naive TH cells into TH2 and/or TH9 effector cells |
|
|
What does IL-6 do? |

Causes polarization of naive TH cells into TH17 cells |
|
|
What does TGF-beta do?
|

Causes polarization of TH9, TH17 and T-regulatory effector cells
|
|
|
What does IL-2 do? |

Causes polarization of T-regulatory cells |
|
|
What causes polarization of TH1 effector cells? |

Triggered by intracellular pathogens Polarization by IFN-gamma and/or IL-12 |
|
|
What causes polarization of TH2 effector cells? |

Triggered by extracellular parasites Polarization by IL-4 |
|
|
What causes polarization of TH9 effector cells? |

Triggered by extracellular parasites and/or allergic inflammation
Polarization by TGF-beta or IL-4 |
|
|
What causes polarization of TH17 effector cells? |

Triggered by extracellular bacteria/fungus
Polarization by TGF-beta and/or IL-6 |
|
|
What does T-reg cells do? |

Regulates activity of TH cells |
|
|
What happens to a T cell when you have a co-simulatory signal and a specific signal? |
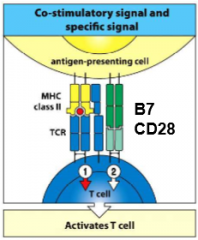
Activates T-cell |
|
|
What happens to a T cell when you have a specific signal alone? |
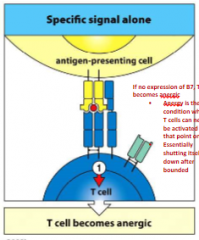
T cell becomes anergic
If no expression of B7 (a co-stimulatory), T cell becomes anergic |
|
|
What does it mean when a cell becomes anergic? |
Anergy is the condition where T cells can never be activated from that point on Essentially shutting itself down after bounded |
|
|
What happens to a T-cell when it has a co-stimulatory signal alone? |
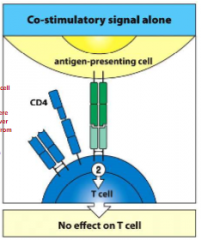
No effect on T cell |
|
|
TH cells bind to MHC class 2 and antigen. What co-receptor is used to strengthen this binding? A) CD40 B) B7 C) CD28 D) CD4 |
D) |
|
|
How does the immune system respond to a virus? |
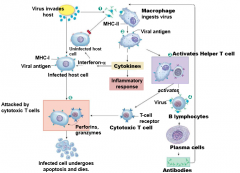
1) Antibodies act as opsonins 2) Macrophages ingest viruses and insert fragments of viral antigen into MHC-2 on their membrane 3) Helper T cells bind to viral antigen on macrophage MHC-2 molecules 4) Prevent exposure to virus by creating memory B lymphocytes with viral antibody on their surface 5) Cytotoxic T cell uses viral antigen-MHC-1 complexes to recognize infected host cell |
|
|
In the immune system's response to a virally infected cell, what does antibodies acting as opsonins on an infected cell do? |
Coating viral particles to make them batter targets for antigen-presenting cells Bind to virus particles, preventing them from entering their target cells No longer effective when virus inside host cell |
|
|
What does interferon-alpha do? |
Causes host cell (of infected cells) to make antiviral proteins, preventing replication of viruses |
|
|
What does granzymes do when inside of an infeted/target cell? |
Induce apoptosis |
|
|
Which of the following is needed to mount an immune response but does not directly rid the body of extracellular pathogens? A) Antibodes B) Helper T cells C) B cells D) Cytotoxic T cells |
B) |
|
|
What is the effect of immune and deficient response to an antigen against infectious agents? |
Immune: Protective immunity Deficient: Recurrent infection |
|
|
What is the effect of immune and deficient response to an antigen against innocuous substance? |
Immune: Allergy Deficient: No response |
|
|
What is the effect of immune and deficient response to an antigen against grafted organ or unmatched blood? |
Immune: Rejection Deficient: Acceptance |
|
|
What is the effect of immune and deficient response to an antigen against self organ? |
Immune: Autoimmunity Deficient: Self tolerance |
|
|
What is the effect of immune and deficient response to an antigen against a tumour? |
Immune: Tumor immunity Deficient: Cancer |
|
|
What happens during a first exposure of an allergic response (immediate hypersensitivity)? |
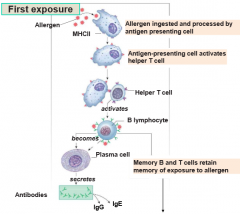
1) Allergen ingested and processed by antigen presenting cell 2) Antigen-presenting cell activates helper T cells 3) Activates B-lymphocytes 4) Becomes plasma cells (or memory B and T cells to retain memory of exposure to allergen) 5) Secretes antibodies (IgG and IgE) |
|
|
What happens during a reexposure of an allergic response with IgE? |
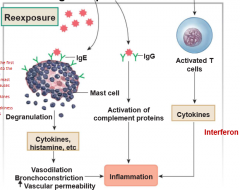
1) Bind to Fc receptors on mass cells (created from crystallization zone) 2) Cause degranulation and release of cytokines and histamines (and etc) 3) Cause vasodilation, bronchoconstriction and increased vascular permeability 4) Inflammation |
|
|
What happens during a reexposure of an allergic response with IgG? |
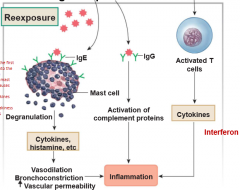
1) Binds to receptors 2) Cause activation of complement proteins 3) Inflammation |
|
|
What happens during a reexposure of an allergic response with activated T cells? |
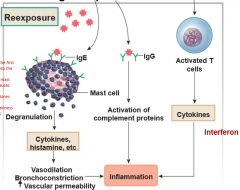
1) Cause release of cytokines such as interferon
2) Inflammation |
|
|
Individuals at risk of developing anaphylactic shock carry a needle with epinephrine. Why? A) Increase heart rate B) Increase vasoconstriction C) Block histamine receptors D) A and B E) All of the above |
D) It is the immediate response that drops blood pressure soepinephrine would increase heart rate to up the flow of blood throughout thebody and cause vasoconstriction to counteract vasodilators |
|
|
What is the most frequent and least frequent blood type? |
Most: Type O Least: Type AB |
|
|
What is more common, Rh+ or Rh-? |
Rh+ |
|
|
What surface antigens and antibodies does blood type A have? |

Surface antigen: A Antibodies: Anti-B |
|
|
What surface antigens and antibodies does blood type B have? |

Surface antigen: B
Antibodies: Anti-A |
|
|
What surface antigens and antibodies does blood type AB have? |

Surface antigen: A and B
Antibodies: Neither anti-A or anti-B |
|
|
What surface antigens and antibodies does blood type O have? |

Surface antigen: Neither A or B Antibodies: Anti-A and Anti-B |
|
|
What happens when an anti-B antibody binds to an B antigen? |
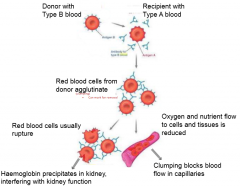
It would bind to B antigen Cause red blood cells to agglutinate (clump) to mark for removal Cause either: 1) Rupture leading to haemoglobin precipitating in kidney, interfering with kidney function 2) Oxygen and nutrient flow in cells and tissue to be reduced as clumping caused a blocked capillary |
|
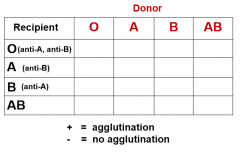
Predict what would happen if the follow combinations of donors and recipients: |
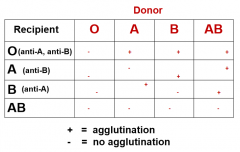
|
|
|
Why is Rh factor status important? |
Unlike the ABO blood group, Rh- individuals can develop antibodies by: 1)Transfusion of Rh- individuals (no D antigen) with Rh+ (D antigen) blood 2) When an Rh- mother becomes pregnant with Rh+ baby |
|
|
How do doctors prevent hemolytic diseases of the newborn? |
Inject D antigen antibodies into Rh- mother during and following her pregnancy Antibodies bind to and remove fetal red blood cells in mother's bloodstream before they can trigger an immune response in the mother Thus, B cells are not activated in mother and no immunological memory of the D antigen is acquired Therefore in subsequent pregnancy with an Rh+ fetus, mother does not produce D antigen antibodies upon exposure to fetal red blood cells with D antigen |
|
|
What are the primary functions of basophils and mast cells? |
Release chemicals that mediate inflammation and allergic responses |
|
|
What are the primary functions of neutrophils? |
Ingest and destroy invaders |
|
|
What are the primary functions of eosinophils? |
Destroy invaders, particularly antibody-coated parasites |
|
|
What are the primary functions of monocytes and macrophages? |
Ingest and destroy invaders Antigen presentation |
|
|
What are the primary functions of lymphocytes and plasma cells? |
Specific responses to invaders, including antibody production |
|
|
What are the primary function of dendritic cells? |
Recognize pathogens and activate other immune cells by antigen presentation |
|
|
What is the thymus gland? |
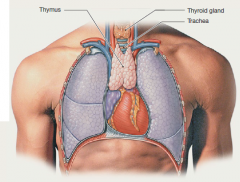
Two-lobed organ located in thorax, just above heart Reaches greatest size during adolescence Shrinks and largely replaced by adipose tissue as person ages |
|
|
What is HIV? |
Virus that causes acquired immunodeficiency syndrome (AIDS) Infects cells of immune system, particularly T lymphocytes, monocytes and macrophages Wipes out helper T cells, cell-mediated immunity against the virus is lost |
|
|
Why is there no guarantee that antibodies produced during one infection will be effective against next invasion by same virus? |
Many viruses mutate constantly, and protein coat forming the primary antigen may change significantly over time If protein coat changes, antibody may no longer recognize it |
|
|
What are platelets? |
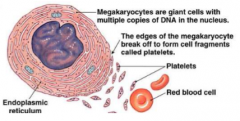
They are needed for blood clotting Half life is about 10 days Thrombopoietin increases platelet numbers It has no nucleus where its cytoplasm contains mitochondria, endoplasmic reticulum and granules Produced from megakaryocytes |
|
|
What are megakaryocytes? |
Develop their formidable size by undergoing mitosis up to seven times without undergoing nuclear or cytoplasmic division Outer edge of marrow megakaryocytes extend through the endothelium into lumen of marrow blood sinuses |
|
|
What are the three phases to regulate blood clotting? |
Vascular Platelet Coagulation |
|
|
What is hemostasis? |
Process of keeping blood within a damaged blood vessel |
|
|
What is vascular phase of blood clotting regulation? |
Neurogenic and myogenic control Immediate constriction of damaged vessels caused by vasconstrictive paracrine released by endothelium Prolonged by sertonin, endothelin-1 and thromoboxane A2 |
|
|
What is platelet phase of blood clotting regulation? |
Temporary blockage of a break by a platelet plug Plug formation begins with platelet adhesion When platelets adhere or stick to exposed collagen in damaged area Adhere platelets activate, releasing cytokines into area around injury Reinforce local vasoconstriction and activate more platelets which aggregate or stick to one another to form a loose platelet plug |
|
|
How are platelet plugs formed? |
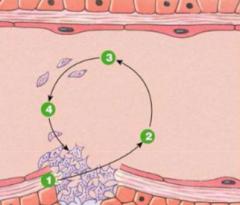
1) Exposed collagen binds and activates platelets via von Willebrand factor 2) Factors (ADP, PAF, sertonin, thromboxane A2) released from platelet 3) Factors attract more platelets 4) Platelets aggregate to form plug |
|
|
What is another name for 5-hydroxytryptamine? |
Serotonin |
|
|
What is PAF factor? |
Platelet-activating factor Sets up positive feedback loop by activating more platelets Initiates pathways that convert platelets membrane phospholipids into thromboxane A2 (a vasoconstrictor) Contribute to platelet aggregation |
|
|
What factors/chemicals can prevent platelet adhesion and cause vasodilation? |
Postacyclin (prostaglandin I2, PGI2) AND Nitric oxide (NO) |
|
|
What is the coagulation phase of blood clotting regulation? |
Formation of a clot that seals the hole until tissue A fibrin protein mesh that stabilizes the platelet plug to form a clot Initiated by exposed collagen and tissue factor (a protein-phospholipid mixture) Coagulation cascade consists of two pathways which converge to one: - Fibrin as an end project of a series of enzymes reactions - Some chemical factors involved in coagulation cascade also promote platelet adhesion and aggregation in damaged region |
|
|
What does the contact activation pathway (intrinsic pathway) start with? |
Collagens and proteins already present in plasma |
|
|
What does tissue factor pathway (extrinsic pathway) start with? |
Damaged tissue exposes tissue thromboplastin |
|
|
What does calcium chelators (EDTA) inhibit? |
Coagulation |
|
|
What is thrombin? |
An enzyme that converts fibrinogen into soluble fibrin polymers |
|
|
Why are there several positive feedback loops in coagulation cascade? |
To sustain thecascade until one or more of the participating plasma proteins are completelyconsumed |
|
|
What is the common pathway of the coagulation cascade? |
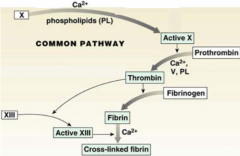
1)Factor X, using phospholipids (PL), factor VIII and Ca++ will be converted into Active X 2) Active X converts Prothrombin (II) using Ca++, V and PL into Thrombin (IIa) 3) Thrombin will convert Fibrinogen into Fibrin and Factor XIII into Active XIII 4) Active XIII will convert Fibrin using Ca++ into Cross-linked Fibrin |
|
|
What is the intrinsic (contact activation) pathway of the coagulation cascade? |
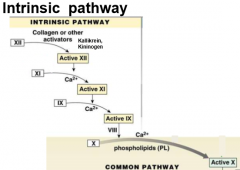
Begins when damage to the tissue exposes collagen
1) Uses collagen or other activators to convert XII into Active XII
2) Active XII converts Factor XI using Ca++ into Active XI
3) Active XI will convert Factor IX using Ca++ into Active IX
4) Active IX will convert X into Active X using factor VIII, Ca++ and phospholipids (PL). Begins common pathway |
|
|
What does anticoagulant coumadin (warfarin) do? |
Blocks action of Vitamin K |
|
|
What regulates levels of factor VIII? |
von Willebrand factors |
|
|
What is needed for the synthesis of factor IX? |
Vitamin K |
|
|
What is the extrinsic (tissue factor) pathway of the coagulation cascade? |
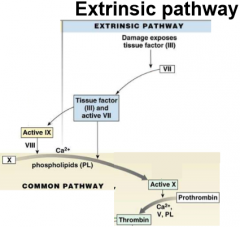
Starts when damaged tissues expose tissue factor (tissue thromboplastic or factor III)
1) Factor VII is converted into Tissue factor (III) and active VII by a damage exposes tissue factor (III)
2) This will cause Active IX to convert Factor X into Active X using Factor VIII, Ca++ and phospholipids (PL) or directly beginning common pathway |
|
|
What is needed for the synthesis of factor X? |
Vitamin K |
|
|
What is needed for the synthesis of thrombin? |
Vitamin K |
|
|
What is needed for the synthesis of factor VII? |
Vitamin K |
|
|
Which factor links platelets to collagen during haemostasis? A) Factor VIIa B) Sertonin C) Thrombin D) von Willebrand factor |
D) |
|
|
What happens when you have a deficiency of factor VIII? |
In mild forms, can cause reduced amounts of active X Severe forms essentially eliminate activity of common pathway Suffer internal and external bleeds |
|
|
Haemophilia B is due to the deficiency of what factor? |
Factor IX |
|
|
What is fibrinolysis? |
Breakdown of formed clot Uses thrombin, plasminogen and tPA (tissue plasminogen activator) as plasmin to breakdown fibrin polymer into fibrin fragments |
|
|
How is the clot removed after healing has taken place? |
Clot disintegrates when fibrin is broken into fragments by enzyme plasmin An inactive form of plasmin, plasminogen, is part of clot After coagulation, thrombin works with second factor called tissue plasminogen activator (tPa) to convert inactive plasminogen into plasmin Plasmin breaks down fibrin by process of fibrinolysis |
|
|
What does the anticoagulant Active Protein C do? |
Inhibit conversion of Factor V into Active V Inhibit conversion of Factor VIII into Active VIII |
|
|
How is Active Protein C formed? |
Protein C and thrombomodulin is converted into Active Protein C using Protein S |
|
|
What does the anticoagulant TFPI do? |
Inhibit conversion of Factor VII into Active VII |
|
|
What does the anticoagulant Antithrombin do? |
Inhibit conversion of Factor X into Active X Inhibit activity of Thrombin |
|
|
Where is plasminogen/plasmin released from? |
Liver |
|
|
What is plasminogen/plasmin activated by? |
tPA and thrombin |
|
|
What is the function of plasminogen/plasmin? |
Breaks down fibrin |
|
|
Where is tPA released from? |
Many tissues |
|
|
What is the function of tPA? |
Activates plasminogen |
|
|
Where is TFPI (tissue factor pathway inhibitor) released from? |
Endothelium |
|
|
What does TFPI do? |
Inhibits tissue factor VII and active VII complex |
|
|
Where is antithrombin III released from? |
Liver |
|
|
What is antithrombin III activated by? |
Heparin |
|
|
What is the function of antithrombin III? |
Block IX, X, XI, XII and thrombin |
|
|
Where is Protein C released from? |
Liver |
|
|
What activates Protein C? |
Thrombin |
|
|
What is the function of Protein C? |
Degrades Activate V and VIII |
|
|
What is thrombus? |
Blood clot (or fatty deposit) attached to a vessel wall |
|
|
What is embolus? |
Floating blood clot (or fatty deposit) |
|
|
Jason just had an ischemic stroke, resulting from obstruction within blood vessels leading to brain. What should you do? |
Immediate transport to hospital (preferably a primary stroke center) Do brain imaging (CT scan or MRI) Administration of tissue plasminogen activator (tPA) Must ensure stroke not cause by hemorrhage |
|
|
Jason just had an ischemic stroke, resulting from obstruction within blood vessels leading to brain. Why would you use tPA to help in this case? |
tPA helps to break up clot, thus reducing tissue damage tPA must be administrated within 4.5-6 hours following first signs of stroke Slight risk of brain haemorrhage secondary to tPA effects |
|
|
What are the signs of stroke? |
Sudden weakness or numbness Trouble speaking/understanding or confusion Vision problems Sudden severe and unusual headache Dizziness |
|
|
What happens when you have too little hemostasis? |
Excessive bleeding |
|
|
What happens when you have too much hemostasis? |
Thrombus |
|
|
What is intracellular space? |
ICF 2/3 of cell Higher solute concentration than water |
|
|
What is extracellular space? |
ECF 1/3 of cell Water from ECF will move to ICF Made of plasma and ISF |
|
|
What happens to ECF and ICF volumes if we eat salt (NaCL)? |
Increase in ECF sodium content and concentration
Sodium will be retained in ECF, thus the concentration of Na+ in ECF will increase
This leads to an increase in ECF osmolality
Function of number of solute in fluid
Osmolality rises
Water moves from ICF to ECF
There is a decrease in ICF volume and increase in ECF volume and cell shrinks
Raise osmolality in EC space, the water in the cells will move out
When eat chip, the concentration of solute in ECF will increase
Remember, cell membrane cannot tolerate the differences in osmolality
Therefore you raise the osmolality, water goes into the EC space
Osmolality moves from inside of the cell to outside of the cell |
|
|
Where is water loss?
|
Skin Lungs Urine Feces |
|
|
What is hyperkalemia? |
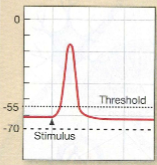
Potassium abnormalities Increase concentration of potassium in ECF Less diffusion of potassium out of cells Increase resting membrane potential Increased cell excitability |
|
|
What is hypokalemia? |
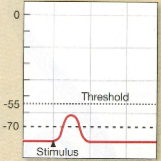
Potassium abnormalities Decreased potassium concentration in ECF More diffusion of potassium out of cells Decreased resting membrane potential Less cell firing |
|
|
What is the cause of hyperkalemia? |
Diabetic ketoacidosis Tissue damage such as burns and hemolysis |
|
|
What are the consequences of hyperkalemia? |
Arrhythmias (which leads to) Atrial fibrillations (which leads to) Heart attack (which leads to) Death |
|
|
How many particles are in a mole of one substance? |
6*10^23 |
|
|
What is the normal osmolarity of the human body? |
280-296 mOsm/L |
|
|
What factors cause exchange between compartments of capillaries? |
Osmolarity (fluid move from low to high osmolairty) Plasma proteins (draws fluids in) |
|
|
What happens to content of blood/renal in extreme starvation and/or low protein diet? |
Low plasma protein which leads to low osmotic pressure
Less water is reabsorbed back into capillaries Increased water retention in ECF and abdominal distention |
|
|
How do you measure the concentration in g/L of body fluids? |

|
|
|
How do you calculate measurements of body fluids in volume? |

|
|
|
What is total body water (TBW)? |
Add substance and distribute to all comparments Markers are 3H2O and 14C-Antipyrene Plasma vs interstitial volume depends onbalance of oncotic pressure and hydrostatic pressure |
|
|
What are some markers to measure ECF? |
Inulin (free filterable, not reabsorbed, not secreted) Mannitol and sulfate 22Na |
|
|
What are some markers to measure plasma volume? |
125I-Albumin Evan's Blue |
|
|
How do you measure ICF? |
TBW - ECF |
|
|
How do you measure ISF? |
ECF - plasma volume |
|
|
What happens to water between compartments of ICF and ECF when you add isotonic NaCl? |
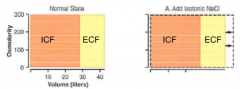
Increase in volume in liters |
|
|
What happens to water between compartments of ICF and ECF when you add hypotonic NaCl? |

Decreased osmolarity Increase volume of ECF and ICF |
|
|
What happens to water between compartment of ICF and ECF when you add hypertonic NaCl? |
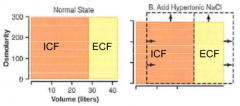
Increase osmolarity Decrease ICF and increase ECF volume |
|
|
What is the hormone EPO? |

Erythropoietin
Kidney senses low oxygen and secretes EPO which binds to EPO receptors on bone marrow
Causes increased erythrocyte production
Glycoprotein synthesized by pericytes at border of medulla and cortex where O2 levels are low
Increase secretion of EPO with anemia or hypoxemia EPO increases red blood cell production in bone marrow |
|
|
What is Vitamin D? |
Functions is to increase absorption of dietary calcium from gut If you don't have vitamin D, you will have difficulty reabsorbing Ca2+ from diet Vitamin D in diet or from skin (sunlight) must be activated by two hydroxylation steps: 25-hydroxylation in liver 1-hydroxylation in kidney Final active hormone is 1,25-dihydroxyvatmin D (calcitriol) |
|
|
How does vitamin D increase plasma calcium? |
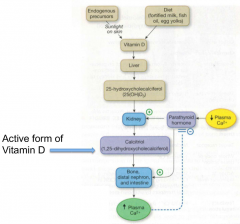
1) Vitamin D either consumed by diet or by sunlight on skin (endogenuous precursors) 2) Vitamin D goes to liver 3) Turned into 25-hydroxycholecalciferol (25(OH)D3) 4) Goes to Kidney (which detects parathyroid hormone released caused by low calcium) and turned into Calcitriol (1,25-dihydroxycholecalciferol, active form of Vitamin D) 5) Goes to bone, distal nephron and intestine 6) Increases plasma calcium Inhibits parathyroid hormone |
|
|
What type of organ are kidneys? |
Retroperitoneal |
|
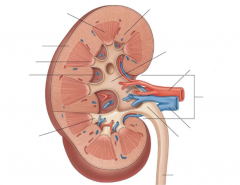
Label the kidney |
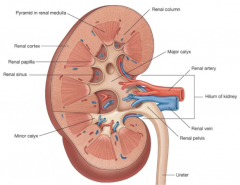
|
|
|
Kidney receives how much cardiac output? |
~20% |
|
|
How much (in percentage) how the kidney weight? |
Less than 1% of the body weight |
|
|
How much ATP does the kidney utilize (in percentage)? |
~16% |
|
|
Where does the kidney receive cardiac output from? |
Renal arteries |
|
|
What are the two arterioles and set of capillaries does the nephron have? |
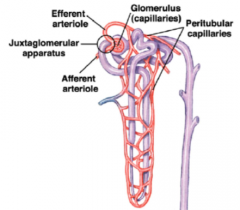
Efferent and afferent arteriole Glomerulus and peritubular capillaries |
|
|
Give an overview of formation of urine: |
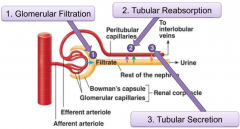
Blood is filtered through glomerulus and various components are secreted into urine or reabsorbed along nephron Urine leaves nephron via collecting ducts Urine is removed from kidney by traveling from ureter to bladder (stored until voiding) |
|
|
How do you calculate Amount of Solutes Excreted? |
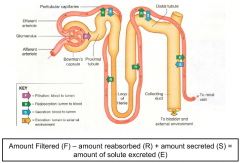
|
|
|
What is the glomerulus? |
A small capillary network that functions as afilter When capillaries are leaky to water and requires small starling force to move water across |
|
|
What are the functions of the glomerulus? |
Transfers fluid from blood into kidney tubule by filtration Nonspecific Filtrate ISF or plasma (contains water and dissolved solutes) No plasma proteins or blood cells enter the tubule |
|
|
What is the renal corpuscle? |
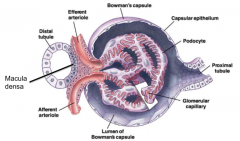
Blood enters through the afferent arteriole and exits through the efferent arteriole Capillaries loop's structure plays role in functions of the tuft: Uses starling forces to move water from the capillaries and into the bowman's space Ultra filter, takes advantage of starling forces, moves water from capillary lumen into the bowman's space Where the filtrate then moves to the tubules where it will be processed Starling forces are not large, but capillaries are very leaky Capillaries in the glomerulus is more leaky than elsewhere in body For small starling forces, a large volume of water is moving across There are one million of these capillary tufts in kidneys Collectively, it forms 150L filtrate everyday Kidneys reabsorbs 95% of the filtrate, thus left with 1.5L of urine Ultra filtrate leads to final form of urine |
|
|
What do the podocytes in the renal corpuscle? |
Leads to ability of the kidney to absorb water and to filtrate it |
|
|
What are the capillary pores in the renal corpuscle? |
Endothelial cells are fenestrated (large pores) Do not let blood cells and plasma proteins pass Albuminuria (protein in urine) |
|
|
What are the basement membrane for in the renal corpuscle? |
Basal lamina separates vessel endothelium and epithelial layer of Bowman's capsule Composed of collagen and glycoproteins |
|
|
What are filtration slits for in the renal corpuscle? |
Specialized cells that are podocytes with narrow slits between them Size of filtration slit can vary with contraction of messangial cells in basal lamina Allows water to move across (via starling forces) but holds back macromolecules |
|
|
What are the three forms of filtration pressure in the glomerulus? |
1) Glomerular capillary blood pressure/hydraulic pressure of blood 2) Plasma colloid osmotic pressure (pi) 3) Bowman's capsule hydrostatic pressure |
|
|
What is glomerular capillary blood pressure/hydraulic pressure of blood in the glomerulus? |
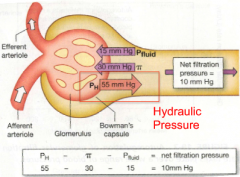
Pressure exerted by blood in glomerular capillaries Favours filtration On average about ~55mmHg |
|
|
What is plasma colloid osmotic pressure (pi) in the glomerulus? |
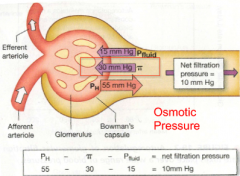
Beacuse proteins are only found in plasma, pressure draws fluid back Opposes filtration On average, about ~30mmHg |
|
|
What is Bowman's capsule hydrostatic pressure in the glomerulus? |
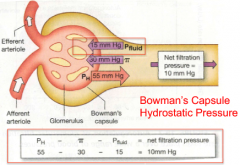
Bowmna's capsule is an enclosed space so pressure of fluid with the capsule creates a fluid pressure Opposes filtration On average about ~15mmHg |
|
|
How does glomerular capillary blood pressure regulate glomerular filtration rate (GFR)? |
Depends on the contraction of the heart and resistance offered by the afferent and efferent arterioles |
|
|
How does autoregulation regulate glomerular filtration rate (GFR)? |
Local control process in which kidney maintains a relatively constant GFR despite a range of fluctuating blood pressure
Kidney autoregulates in response to blood pressure that is driving the renal blood flow
If BP falls, afferent arterioles dilates (higher pressured driving fluid is met with higher resistance)
If BP rises, afferent arteriole constrict |
|
|
What happens to starling force, water and GFR when you raise glomerulus pressure? |
Alter starling force
Move water from capillary to bowman's space
Increase in GFR |
|
|
What is myogenic? |
Intrinsic ability of vascular smooth muscle to respond to pressure changes Blood pressure provides the hydrostatic pressure that drives the glomerular filtration |
|
|
What is tonic state of the glomerulus? |
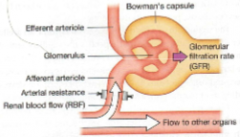
Renal blood flow and GFR change if resistance in arterioles changes |
|
|
What happens if there is vasconstriction of the afferent arteriole of the glomerulus? |
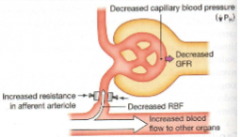
Increase resistance and decrease renal blood flow, capillary blood pressure and GFR |
|
|
What happens if there is vasoconstriction of efferent arteriole of the glomerulus? |
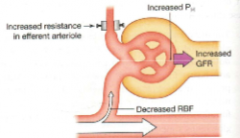
Increase resistance in efferent arteriole and decrease renal blood flow but increase capillary blood pressure and GFR |
|
|
What is tubuloglomerular feedback? |

1) GFR increase 2) Flow through tubule increases 3) Flow past macula densa increases 4) Paracrine from macula densa to afferent arteriole 5) Afferent arteriole constricts This causes resistance in arteriole to increase, hydrostatic pressure in glomerulus and GFR to decrease |
|
|
How are the afferent and efferent arterioles innervated in reflex control of GFR? |
Sympathetic neurons that terminate on alpha-receptors Activation causes vasoconstriction which regulates GFR |
|
|
What is kidney failure? |
Kidney cannot adequately filter wastes products from blood Can be caused by an acute kidney injury or chronic kidney disease Determined by decrease in GFR |
|
|
What can be an outcome of decreased GFR in kidney? |
Decreased or no urine production Accumulation of waste products in blood Blood in urine (hematuria) Protein loss in urine (proteinuria) |
|
|
What is hematuria? |
Blood in urine |
|
|
What is proteinuria? |
Protein loss in urine |
|
|
What are the functions of secretion of the kidney? |
Waste removal (urea, uric acid, bile salts, ammonia, catecholamines and creatinine) Removal of foreign substances (drugs, food additives) Acid base balance (secretion of H and HCO3 regulates pH of body fluids) |
|
|
Explain H+ secretion from kidneys: |
H+ can be added to filtered fluid through secretion in proximal tubule, distal tubule and collecting ducts |
|
|
If body fluids are too acidic, what happens to H+ secretion? |
Increases |
|
|
If body fluids are too basic or alkaline, what happens to H+ secretion? |
Decreases |
|
|
Explain K+ secretion: |
K+ is selectively moved in opposite directions in different parts of the tubule Proximal tubule actively reabsorbed K+ Distal tubule and collecting duct actively secreted K+ if needed Almost all K+ filtrated is reabsorbed Most of the K+ in urine is derived from controlled secretion |
|
|
What are the two ways that substances can be removed/secreted from kidney? |
1) Filtration through glomerular capillaries 2) Secretion into filtrate Both excrete via urine |
|
|
How is excretion calculated? |
Filtration - Reabsorption + Secretion |
|
|
How do you calculate GFR? |
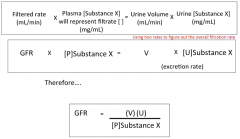
|
|
|
What is inulin? |
Unique because 100% filtered is excreted, not reabsorbed or secreted Filtered load = P[inulin] * GFR Filtered load is equal to excretion rate of inulin Therefore GFR is equal to clearance of inulin |
|
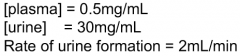
Calculate clearance of inulin |
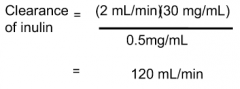
|
|
Calculate clearance of urea |
|
|
|
How is glucose and amino acids cleared from the kidney? |
Filtered by glomerulus into renal tubule Not normally present in urine Can assume they are completely reabsorbed (secondary active transport) Clearance should equal 0mL/min |
|
|
Why should the clearance of glucose and amino acids be 0mL/min in a healthy person? |
Should be 0 in a healthy person because in a healthy person, there should be no amino acids and proteins in your excretion |
|
|
What is plasma creatinine? |
Can be used as a natural marker Metabolite of phosphocreatine Secreted slightly by tubules but for clinical purpose assume that GFR is equal to excretion An abnormal decrease in GFR causes an increase in plasma creatinine concentration Blood concentration of creatinine provides measure of kidney function |
|
|
How much of inulin is excreted? |
100% |
|
|
For urine to become more concentrated, what must happen to the tubule epithelium? |
It must become permeable to water so that water can move by osmosis out of the lumen to the more concentrated interstitial fluid |
|
|
What is antidiuretic hormone? |
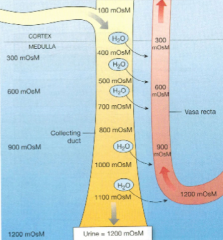
ADH Also known as Arginine vasopressin (AVP) or vasopressin ADH regulates permeability of water of the distal tubule and collecting duct Does this by inserting pores that allow water to be reabsorbed (thus, not having diuresis - urine production) |
|
|
What is the function of ADH on kidney? |
Increases water reabsorption from DCT and collecting ducts Increases plasma volume |
|
|
What are the functions of ADH on blood vessels? |
Acts to constrict them
Increases peripheral vascular resistance
Increases arterial blood pressure |
|
|
What happens in the absence of ADH? |
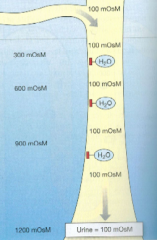
Without ADH, apical membrane of distal tubule and collecting duct are impermeable to water |
|
|
What is the mechanisms of action of ADH? |

1) ADH binds to its V2 membrane receptor 2) Receptor binding activates G-protein/cAMP secondary messenger signaling 3) Aquaporin-2 (AP2) water pores become inserted into the apical membrane via phosphorylation of intracellular proteins 4) Water is transported by AP2 on the apical surface and by osmosis across basal membrane into blood. Water pores are present on basolateral membrane but not regulated by ADH |
|
|
What happens if ADH levels fall? |
Water pores are removed from apical membrane by endocytosis Of vesicles containing aquaporin into cell for available use fornext time interact with ADH |
|
|
What is membrane recycling? |
In the process of ADH levels decreasing, the process of endocytotic vesicles containing water pores are stored in cytoplasm until another signal from ADH causes them to be reinserted into membrane In which parts of cell membrane are alternatively added and withdrawn |
|
|
How is ADH produced? |

1) Hypothalamic neurons synthesize ADH 2) ADH transported along hypothalamic-hypophyseal tract to posterior pituitary 3) ADH stored in axon terminals in posterior pituitary 4) ADH released into blood when hypothalamic neurons fire and travels to kidney |
|
|
In the renal reflex (osmolarity of ECF), what happens if ECF osmolarity decreases? |
This means less solutes and more water Causes water move into cells Cells then would swell causing ion channel disruption and brain cell swelling |
|
|
In the renal reflex (osmolarity of ECF), what happens if ECF osmolarity increases? |
Cause osmoreceptors to release ADH to stimulate third and increase water reabsorption Water moves out of cells Causing cells to shrink and depoalrization and ion channels to open |
|
|
What happens to your kidneys and vasopressins when you ingest salt (NaCl)? |
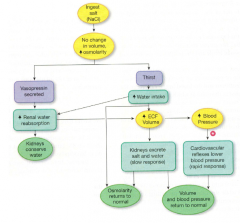
Once ingested, no change in volume would happen, increasing osmolarity Vasopressin secreted Increase renal water reabsorption Kidneys conserve water |
|
|
What happens to your kidneys and water intake when you ingest salt (NaCl)? |
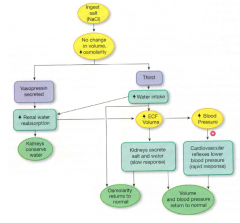
Once ingested, no change in volume would happen, increasing osmolarity
Cause thirst to increase water intake Increase renal water reabsorption Kidneys conserve more water |
|
|
How does ECF volume effect osmolarity after ingestion of salt (NaCl)? |
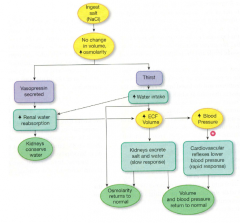
Once water intake or renal water reabsoprtion increases, ECF volume increases This causes kidneys to excrete salt and water (a slow response) Increasing osmolarity return to normal OR the increase in water intake can directly increase osmolarity to return to normal |
|
|
How does ECF volume effect volume and blood pressure after ingestion of salt (NaCl)? |
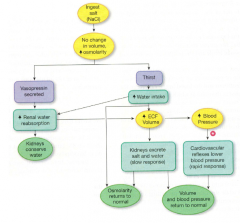
Once water intake or renal water reabsoprtion increases, ECF volume increases There can either be a slow response (kidneys excrete salt and water) to cause volume and blood pressure to return to normal Or a rapid response (cardiovascular reflexes lower blood pressure) by increasing blood pressure to cause volume and blood pressure to return to normal |
|
|
How does blood pressure effect volume and pressure after ingestion of salt (NaCl)? |
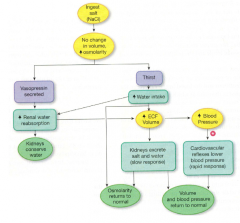
Once water intake or renal water reabsoprtion increases, ECF volume increases There is a rapid response (cardiovascular reflexes lower blood pressure) by increasing blood pressure to cause volume and blood pressure to return to normal |
|
|
In response to decrease blood volume, how do volume receptors in atria, carotid and aortic baroreceptors increase blood pressure by cardiovascular system? |

Decreased blood volume leading to decreased blood pressure Detected by volume receptors in atria and carotid and aortic baroreceptors Trigger homeostatic reflexes Cardiovascular system cause increase cardiac output and vasoconstriction |
|
|
In response to decrease blood volume, how do volume receptors in atria, carotid and aortic baroreceptors increase blood pressure by behaviour? |

Decreased blood volume leading to decreased blood pressure Detected by volume receptors in atria and carotid and aortic baroreceptors Trigger homeostatic reflexes Behaviour causes thirst to increase water intake Increasing ECF and ICF volume Increasing blood pressure |
|
|
In response to decrease blood volume, how do volume receptors in atria, carotid and aortic baroreceptors conserve water? |

Decreased blood volume leading to decreased blood pressure Detected by volume receptors in atria and carotid and aortic baroreceptors Trigger homeostatic reflexes Causes kidneys to conserve water to minimize further volume loss |
|
|
In response to increase blood volume, how do volume receptors in atria, endocrine cells in atria, carotid and aortic baroreceptors decrease blood pressure by cardiovascular system? |

Increase blood volume and pressure detected by volume receptors in atria, endocrine cells in atria and carotid and aortic baroreceptors Trigger homeostatic reflexes Cardiovascular system would decrease cardiac output and cause vasodilation Decrease blood pressure |
|
|
In response to increase blood volume, how do volume receptors in atria, endocrine cells in atria, carotid and aortic baroreceptors decrease blood pressure by kidneys? |
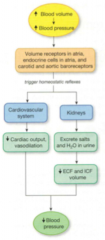
Increase blood volume and pressure detected by volume receptors in atria, endocrine cells in atria and carotid and aortic baroreceptors Trigger homeostatic reflexes Kidneys would cause excretion of salt and water into urine Decrease ECF and ICF volume Decrease blood pressure |
|
|
What causes bedwetting of children? |
In normal children: ADH levels increase at night causing increase reabsorption of water causing decrease noctornal production concentration of urine In enuretic children: ADH level do not increase at night causing decrease reabsorption of water causing increase noctornal production of urine |
|
|
What drug can treat enuretic children? |
Desmopresin |
|
|
What is the extent of controlled reabsorption of sodium in the kidney inversely proportion to? |
Inversely proportional to the magnitude of sodium load in the body |
|
|
What happens if there is too much sodium in the body? |
Decreased controlled sodium reabsorption Causes an increase of sodium loss via urine |
|
|
What happens if there is too little or depletion of sodium in the body? |
Increased controlled reabsorption Causes a decrease sodium loss via urine |
|
|
Expansion of plasma volume does what to blood pressure? |
Increases |
|
|
Contraction of plasma volume does what to blood pressure? |
Lower/decrease |
|
|
How does an increase in sodium load increase blood pressure? |
Increases ECF osmolarity Extra sodium holding extra water Expansion of ECF volume Increase blood pressure |
|
|
How does a decrease in sodium load decrease blood pressure? |
Decrease ECF's osmolarity Less water than normal held by ECF ECF volume reduction Decreased blood pressure |
|
|
What hormone does the juxtaglomerular apparatus secret in relation to blood pressure? |
Renin |
|
|
How do the kidneys sense a drop in blood pressure? |
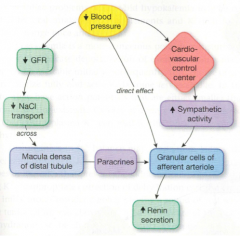
By the juxtaglomerular apparatus Three pathways: 1) Decreased blood pressure directly effect granular cells of afferent arteriole causes an increase of renin secretion 2) Decrease blood pressure causes cardiovascular control center to increase sympathetic activity causing granular cells of afferent arteriole to increase renin secretion 3) Decrease blood pressure causes decrease GFR causing decrease NaCl transport across macula densa of distal tubules. Causing paracrines to effect granular cells of afferent arteriole to incraese renin secretion |
|
|
What is aldosterone? |
A steroid hormone
Synthesized in adrenal cortex (the outer portion of the gland that sits on top of each kidney) Secreted into the blood and transported on a protein carrier to its target |
|
|
What are the mode of actions for aldosterone? |
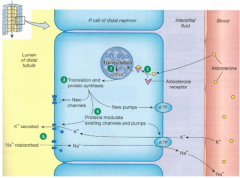
Primary target of aldosterone is last 1/3 of DT and CT Target cells are the principal cell or P cell P cell look like other polarized transporting cell with Na+/K+-ATPase pumps on basolateral membrane Various channels and transporters on the apical membrane Aldosterone enters cell by simple diffusion In target cells, aldosterone combines with cytoplasmic receptor Hormone-receptor complex moves in to the nucleus and binds to DNA, initiating the synthesis of new protein channels and Na+/K+-ATPase pumps New protein must be inserted into cell membrane before their effect can be noticed Entire process takes 1-2 hours, a slow response for hormone to increase ECF fluid volume In the distal nephron, Na+ and water reabsorption are separately regulated where water does not automatically follow Na+ reabsorption and ADH must be present In the proximal tube, Na+ reabsorption is automatically followed by water reabsorption because proximal tubule epithelium is always freely permeable to water |
|
|
What stimulatory factors affect aldosterone release? |
Direct at adrenal cortex by an increased extra cellular potassium concentration Indirect through RAAS pathway |
|
|
How is an increased extra cellular potassium concentration at adrenal cortex stimulate aldosterone release? |
An increase in potassium concentration stimulates aldosterone production and results in secretion by the nephron This reflex protects the blood from hyperkalemia (elevated blood potassium) |
|
|
How does the RAAS pathway stimulate aldosterone release? |
Decreased blood pressure Decreased flow past macula densa |
|
|
What inhibitory factors affect aldosterone release? |
Direct at adrenal cortex by increased osmolarity |
|
|
How does an increased osmolarity at the adrenal cortex inhibit aldosterone release? |
An increase in ECF osmolarity inhibits aldosterone secretion Less aldosterone means increased sodium excretion which helps decrease osmolarity |
|
|
What is atrial naturetic peptide? |
ANP
It is secreted when atrial cells stretch more than in normal, as would occur with increase in blood volume At systemic level, ANP enhances sodium excretion and urinary water loss Has short half-life |
|
|
Using natriuretic peptides and less vasopressins, how does an increased blood volume cause increased NaCl and water excretion? |
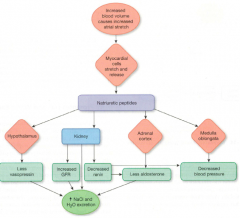
Increased blood volume causes increased atrial stretch
Myocardial cells stretch and released natriuretic peptides
Causes the hypothalamus to release less vasopressin
Causes an increased NaCl and water excretion |
|
|
Using natriuretic peptides and increased GFR, how does an increased blood volume cause increased NaCl and water excretion? |
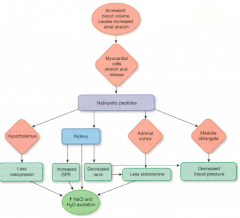
Increased blood volume causes increased atrial stretch Myocardial cells stretch and released natriuretic peptides Causes kidney to increase GFR Causing increased NaCl and water excretion |
|
|
Using natriuretic peptides and decreased renin, how does an increased blood volume cause increased NaCl and water excretion? |
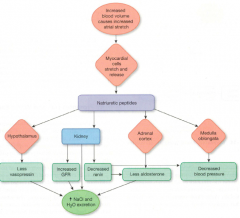
Increased blood volume causes increased atrial stretch Myocardial cells stretch and released natriuretic peptides Causes kidney to decrease renin Causes less aldosterone Causes increased NaCl and water excretion |
|
|
Using natriuretic peptides and kidney directly, how does an increased blood volume cause increased NaCl and water excretion? |
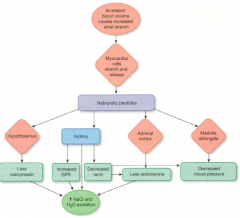
Increased blood volume causes increased atrial stretch Myocardial cells stretch and released natriuretic peptides Causes kidney to directly increase NaCl and water excretion |
|
|
Using natriuretic peptides and less aldosterone from adrenal cortex, how does an increased blood volume cause increased NaCl and water excretion? |
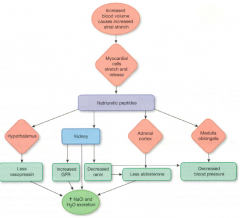
Increased blood volume causes increased atrial stretch Myocardial cells stretch and released natriuretic peptides Causes the adrenal cortex to release less aldosterone Causes an increase in NaCl and water excretion |
|
|
Using natriuretic peptides and decreased renin, how does an increased blood volume cause decreased blood pressure? |
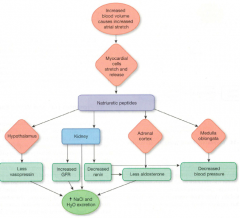
Increased blood volume causes increased atrial stretch Myocardial cells stretch and released natriuretic peptides Causes kidney to release less renin Causes decreased blood pressure |
|
|
Using natriuretic peptides and medulla oblongata, how does an increased blood volume cause decreased blood pressure? |
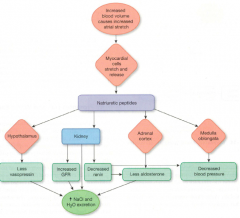
Increased blood volume causes increased atrial stretch Myocardial cells stretch and released natriuretic peptides Causes the medulla oblongata to decrease blood pressure |
|
|
What are the known functions of ANP? |
Increases GFR, apparently by relaxing the contractile surrounding the filtration slits Decreases sodium and water reabsorption in the collection ducts Inhibits release of renin, aldosterone and ADH ANP and like peptides are secreted by neurons in brain which lowers blood pressure |
|
|
What is the micturition reflex? |
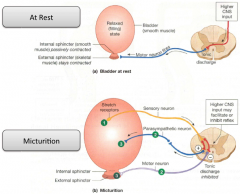
When there is high CNS input, it may facilitate or inhibit reflex The reflex itself causes the bladder to stretch |
|
|
The pH of a solution if a measure of its what? |
[H+] |
|
|
What pH is considered acidic? |
Below 7.0 |
|
|
When pH is below 7.0, what does that mean has happened to its [H+]? |
Increased |
|
|
What pH is considered basic? |
Above 7.0 |
|
|
When the pH is above 7.0, what does that mean has happened to its [H+]? |
Decreased |
|
|
What is the normal range of pH in plasma in the body? |
7.35 to 7.45 |
|
|
What is pH relevance to cell function? |
Membrane channels are proteins sensitive to pH because function is dependent on their 3D shape Changes in [H+] alters the tertiary structure of protein |
|
|
What is pH relevance to enzymes (proteins)? |
Acid where is capable of donating a proton to a solution, where as a base accepts H+
H+ binding may change the charge, shape and therefore change function |
|
|
What is pH relevance to the nervous system? |
Neuronal firing affected: Less excitable causing CNS depression which can lead to COMA and/or death Hyper-excitable causing muscle twitches and sustained muscle contraction of tetanus which can lead to paralysis of respiratory muscles and/or irregular cardiac contractions |
|
|
What does a less excitable neuronal firing cause? |
CNS depression which can lead to COMA and/or death |
|
|
What does a hyper excitable neuronal firing cause? |
Muscle twitches and sustained muscle contraction of tetanus which can lead to paralysis of respiratory muscles and/or irregular cardiac contractions |
|
|
What is pH relevance to potassium imbalances? |
Can lead to disturbances in function of excitable tissues, especially the heart Renal regulation of H+ is closely linked to K+ balance owing to a renal transporter (antiport) |
|
|
What does an intracellular acidosis do? |
Can develop during hypokalemia Renal production of NH3 is increased Resulting in an increased in renal acid excretion |
|
|
What does an intracellular alkalosis do? |
Can develop during hyperkalemia Renal production of NH3 decreased in hyperkalemia Resulting in decrease in renal acid excretion |
|
|
What are buffers? |
A buffer is a molecule that prevents wide swings in pH by combing with or releasing H+ |
|
|
What happens to body in absence of buffers? |
Addition of acid to a solution will cause a sharp change in pH |
|
|
What happens to body in presence of a buffer? |
The pH change will be moderated or may even be unnoticeable |
|
|
Where can buffers be found in the body? |
Within the cell and in the plasma |
|
|
What are intracellular body buffers? |
Cellular proteins Phosphate ions (HPO4-2) Hemoglobin |
|
|
What is a extracellular body buffer? |
Bicarbonate |
|
|
What is the intracellular buffer cellular proteins? |
When pH rises, proteins with carboxyl side groups release H+
-COOH -> -COO- + H+
When pH falls, amino (NH2) side groups behind H+
-NH2 + H+ -> -NH3+ |
|
|
What is the equation for the intracellular buffer phosphate ions (HPO4-2)? |

|
|
|
What is the equation for the intracellular buffer hemoglobin? |
|
|
|
What is the extracellular buffer bicarbonate? |
Works by the Bicarbonate Buffer System (BBS) Produced from metabolic CO2 Most important extracellular buffer system of the body In equilibrium in any aqueous solution H+ reacts with bicarbonate, which reacts with CO2 As H+ concentration increases, it shift the equilibrium to the right H2O + CO2 -> H2CO3 -> HCO3- + H+ Increasing bicarbonate decreases [H+] and increases pH (alkalosis) Increasing PCO2 increases H+ + HCO3- |
|
|
Why is Bicarbonate Buffer System (BBS) so efficient?
|
Because both sides of equilibrium can independent regulated Bicarbonate can be increased or decreased by kidney CO2 can be increased or decreased by lungs (alveolar ventilation) Depending on how much you breathe If a disorder causes a fall in bicarbonate (and acidosis) the lungs can lower CO2 and bring pH toward normal compensation) So that concentration of H+ does not rise to much to cause acidosis If CO2 is too high, equilibrium will shift to left thus making more |
|
|
What are some sources of H+ for the body? |
Diet
Lactic acid
Ketoacids
Toxins
CO2 from tissue mtabolism
Proteins (they contain sulfur-containing amino acids cysteine and methionine which are metabolized to sulphuric acid) |
|
|
How do you obtain H+ for the body by diet? |
Many metabolic intermediates and foods are organic acids that ionize and contribute to H+ to the body fluids Protein with sulfur containing amino acids Metabolism (H2SO4 - you need to get rid of this) |
|
|
How does glucose and/or lactic acid get converted and used for Krebs' cycle? |
By lactic acidosis 1) Glucose converted into pyruvic acid (which can converted lactic acid and reverse back to pyruvic acid) 2) Pyruvic acid gets converted into Acetyl-CoA (can be blocked by insufficient O2) 3) Gets used in Krebs' cycle |
|
|
What are ketoacids? |
Abnormal fat and amino acid metabolism in the disease diabetes mellitus creates strong acids known as ketoacids (beta-hydroxybutyric acid and acetoacetic acid) |
|
|
What can cause a deficiency of insulin? |
Starvation Diabetes mellitus |
|
|
What can low insulin levels lead to? |
Fat releases fatty acids
Liver converts free fatty acids into ketoacids |
|
|
How does CO2 come from tissue metabolism? |
The biggest sources of acid in a daily basis is the production of CO2 during aerobic respiration CO2 is not an acid because it does not contain any H+ However CO2 from respiration combines with water to form H2CO3 which disassociates into HCO3- + H+ |
|
|
How does the respiratory compenstate for increased plasma H+ to decrease it? |
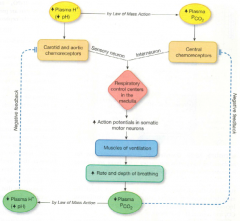
An increase in plasma H+ causes a decrease in pH and by Law of Mass Action, causes an increase in Plasma P(CO2) The increase plasma H+ causes carotid and aortic chemorecptors, by sensory neuron, causes the respiratory control centers in the medulla to increase action potentials in somatic motor neurons The central chemoreceptors (activated by the increase of plasma P(CO2)) does the same by interneurons This causes muscles of ventilation to increase rate and depth of breathing Decreases plasma P(CO2) (which inhibits the central chemoreceptors) which by Law of Mass Action decrease plasma H+ and increase pH (which inhibits carotid and aortic chemoreceptors) |
|
|
How does the kidney affect pH? |
Directly by retaining or excreting H+ Indirectly by changing the reabsorption |
|
|
How does the proximal tubule cause H+ secretion and reabsorption of filtered HCO3-? |
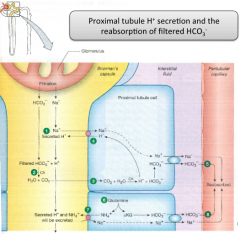
Want the bicarbonate to be in the interstitial space antiporter
Exchanges Na+ for H+ ion
Na+ moves in down its concentration gradient H+ interacts with bicarbonate to form H2CO3, which then breaks down into water and CO2
They move into the cell through aquaporin channel
When CO2 and water move back into the cell, a different enzyme will reverse the reaction to reform the bicarbonate and H+
H+ is recycled |
|
|
What is respiratory acidosis? |

Respiratory distress due to drugs or alcohol Increased airway resistance (asthma) Impaired gas exchange (fibrosis, pneumonia) Muscle weakness (muscular dystrophy) Inadequate gas exchange due to gas exchanging area (Emphysema) |
|
|
What is repiratory alkalosis? |
Excessive artificial ventilation (corrected by adjusting the ventilator) Hysterical hyperventilation (due to anxiety) |
|
|
What is metabolic acidosis? |

Lactic acidosis Ketoacidosis Ingested toxins Diarrhea |
|
|
What is metabolic alkalosis? |

Excessive vomiting (less of stomach acids) Excessive ingestion of bicarbonate (bicarbonate containing antacids) |
|
|
What are the functions of digestive system? |
Supply water, electrolytes and nutrients to the body Provide defenses to prevent both infection and autodigestion Remove waste |
|
|
What is the mouth of the human used for? |
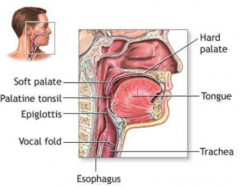
Receptable for food Tongue tastes/guides food Teeth grind food Mix food with saliva (from salivary glands) Minimal digestion of carbohydrates and lipids |
|
|
What is the salivary gland? |
These are accessory glands They also secrete enzymes initiating some digestive processes Depending on how long food stays in your mouth determines how well digestive system is Tongue is there to move the material, making it mix well with the saliva As you chew the food, it becomes a bolus of food |
|
|
What is the pharnyx of the human? |
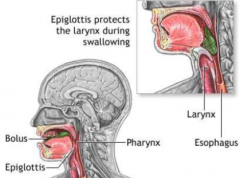
Swallowing reflex Pushes food into esophagus Area of where the materials enter Therefore it connects with the olfactory area The tongue push the ebolus back into the pharynx, presence of the ebolus causes it be pushed down |
|
|
What is the esophagus of the human? |
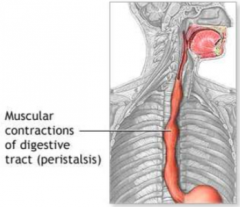
Moves food into the stomach (peristalsis)
No digestion
Muscular tube, no digestion taken place
Coordinated contraction of those muscles, helping pushing the ebolus of food down the tube
It is controlled by sphincters (muscular rigs of the esophagus) |
|
|
What is the stomach of the human used for? |
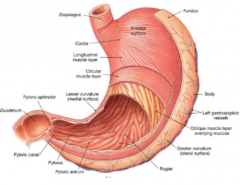
Temporarily stores ingested food Secretes acid/enzymes for digestion (mainly protein) Mechanically breaks down food/mix with secretion Slowly empties into small intestine |
|
|
What is the small intestine of the human? |
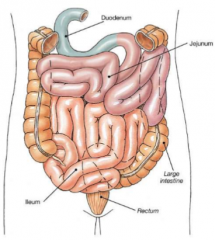
Segmentation and peristalsis Digestion of all types of nutrients Main site of absorption 20 ft in length It is small due to the diameter These areas are specialized in their activity, cells that line them but not specialized in the movement of the chyme Movement of chyme is facilitated due to: Increased in surface area of the small intestine, giving it more time for nutrients to be absorbed as it travels along Therefore nutrients are absorbed here Digestion aided by secretion of liver (via gall bladder) and pancreas |
|
|
What is bile salts? |
Comes from the liver Associated with the GI tract A number secretions enter into the main ducts coming from the liver Can go directly into the duodenum or stored into the gall bladder (a muscular sac to store bile and will release it in response to muscular contractions) This material will eventually be dropped into the duodenum The entrance of the material secreted by the pancreas and duct cells is controlled by sphincters orbed here |
|
|
What is the large intestine (colon) of the human? |
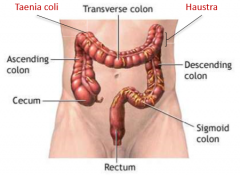
Segmentation and mass movement
Absorption of water/electrolytes
Storage of fecal material and expulsion
Large in diameter, but not long in length
Specialized regions of the large intestine because important processes are taken place
Have entrance of some of the chyme from small intestine (more soupy at this point) absorption of water from the chyme continues in the large intestine
It removes the last little bit of water
The material will become larger and more solid
Specialized motility patterns, to give the big material the ability to be expelled |
|
|
What is the mucosa of the GI tract wall? |
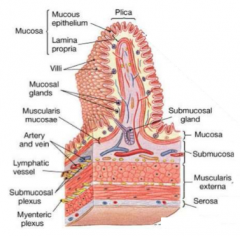
One of the four layers of the GI tract wall Includes epithelial cell layer, thin ECM, thin layer of muscle(musclaris mucosae) |
|
|
What is the submucosa of the GI tract wall? |
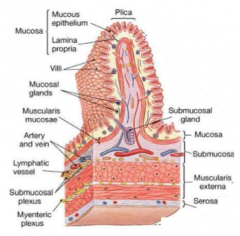
One of the four layers of the GI tract wall Thicker collection of ECM Some immune cells, glands, blood vessels Nerve system Network of nerve (submucosal plexus) |
|
|
What is the muscularis externa of the GI tract wall? |
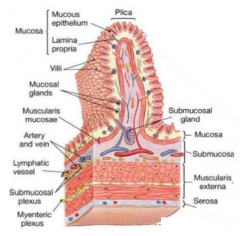
One of the four layers of the GI tract wall Layer of muscles Large intestine do not have continues later of longitudinal muscle Myenteric plexus another nerve network Made up two layers of muscles, longitudinal: Circular muscle and oblique muscle (layer of muscle for contraction of the stomach to break down food) |
|
|
What is the serosa of the GI tract wall? |
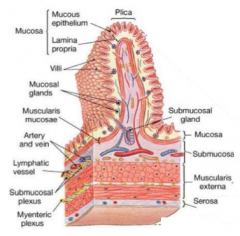
One of the four layers of the GI tract wall Facilitating movement over the GI tract Adhesions where there will be damage to the serosa, areas in the GI tract will stick to each other |
|
|
What is the gut-associated lymphoid tissues? |
GALT Open tube that is specialized to increase SA Toxins and pathogens will interface through the epithelial layer Under the epithelial layer you have loose collection of immune cells, specialized clusters attached to the illume of the small intestine |
|
|
What does the epithelial cell of the mucosa do? |
Secrete acid, bicarbonate, absorption of nutrients, water and vitamins |
|
|
What does the enteroendocrin cells of the mucosa do? |
Secrete hormones into blood stream |
|
|
What does the exocrine cells of the mucosa do? |
Secrete enzymes and mucus |
|
|
What does the goblet cells of the mucosa do? |
Secrete musuc |
|
|
What does the paneth cells of the mucosa do? |
Secrete antimicrobial compounds |
|
|
What is the myentric plexus? |
Part of the enteric nervous system (ENS) Regulates motility |
|
|
What is the submucosal plexus? |
Part of the enteric nervous system (ENS) Regulates secretion and absorption Immediately underlying the mucosal and epithelial cell |
|
|
What does the parasympathetic control generally do to digestive system? |
Increase gut muscle activity Relax sphincters Increase secretion |
|
|
What does the sympathetic control generally do to digestive system? |
Inhibit gut movement Constrict sphincters Reduce secretion |
|
|
What does GLP stand for and what does GLP-1 stimulate? |
Glucagon-like peptide Stimulate release of insulin |
|
|
What would expect to observe if you electrically stimulated the vagus nerve in an individual? A) Enhanced secretion of acid from stomach B) Reduced motility of the stomach C) Reduced levels of acetylcholine in the enteric nervous system D) Enhanced motility of the rectum |
A) |
|
|
What vessels bring blood to and from the digestive system? |
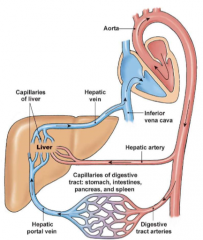
Splanchnic circulation
Blood leaving from the gut must pass through the liver
The portal system is the movement of blood from one capillary to another capillary bed |
|
|
What is the capillaries of the villi for? |
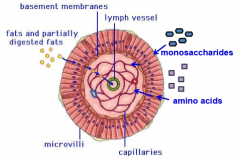
Gas exchange, transport soluble nutrients, water and electrolytes |
|
|
What are the central lacteal of the villi used for? |
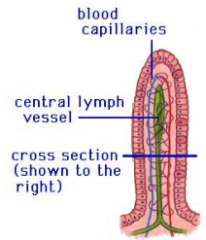
Fat absorption into lymphatic system |
|
|
What does hepatocytes do? |
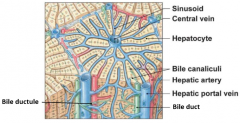
Remove potentially harmful agents Distinct arrangement Needs to face onto the sinusoid Secreting materials into the sinusoid It also secrete materials back into the GI tract through the bile ducts Others get secreted into the sinusoids The central vein connects to the hepatic vein |
|
|
In which blood vessel would you expect of observe the highest concentration of glucose following a meal? A) Hepatic vein B) Hepatic artery C) Hepatic portal vein D) Superior mesenteric artery |
C)
|
|
|
Which ONE of the following sequences correctly traces the flow of blood through the digestivesystem? A) celiac trunk, superior pancreatico-duodenal artery, inferior mesenteric vein B) celiac trunk, hepatic vein, liver sinusoid C) splenic vein, liver sinusoid, inferior vena cava D) inferior mesenteric vein, hepatic artery, central vein |
C) |
|
|
Which of the following is NOT a component in the intrinsic pathway of the coagulation cascade? A) Activation of factor XI in the presence of kallikrein B) Activation of factor IX by factor III and active factor VII C) Amplification of factor XI activation by thrombin D) Activation of factor IX in the presence of Ca2+ |
A) |
|
|
Which of the following is NOT a mechanism of how the kidneys sense a drop in blood pressure? A) By the smooth muscle cells around the arteriole B) By the macula densa cells of the distal collecting tubules C) By the juxtaglomerular cells D) By increased renin levels |
D) |
|
|
If the concentration of the filtrate entering the collecting duct is 500 mOsm and ADH is present, what would be the concentration of the filtrate leaving the collecting duct?
A) 700 mOsm
B) 300 mOsm
C) 100 mOsm
D) 500 mOsm |
A) |
|
|
What trigger signals the brain to increase the output of ADH for water conservation? A) The juxtaglomerular apparatus B) Osmoreceptors in the hypothalamus C) Chemoreceptors in the posterior pituitary D) Sympathetic nervous system |
B) |
|
|
The pathway down the nephron is: A) Bowmans capsule - loop of Henle - distal tubule - proximal tubule - collecting duct B) Bowmans capsule - distal tubule - loop of Henle - proximal tubule - collecting duct C) Bowmans capsule - proximal tubule - loop of Henle - distal tubule - collecting duct D) Bowmans capsule - proximal tubule - loop of Henle - collecting duct - distal tubule |
C) |
|
|
Which one of the following statements about ADH is FALSE? A) ADH is made in the posterior pituitary and released from the hypothalamus. B) ADH acts both on the kidney to increase water reabsorption and on blood vessels as avasoconstrictor. C) ADH is released when ECF osmolarity is high - thus attempting to reabsorb water from thekidney. D) When ADH is present the urine produced is very concentrated |
A) |
|
|
The ________ is a layer of smooth muscle cells whose contraction moves the intestinal villi toalter luminal surface area for absorption. A) muscularis mucosae B) Auerbach's plexus C) serosa D) muscularis externae |
A) |
|

If 30g of solute A is filtered through the glomerulus and the following data is obtained , what is theamount of solute A that has been excreted? A) 12 g B) 46 g C) 44 g D) 14 g |
D) |
|
|
Which are contained in the hilum of the kidney? A) Pyramids, columns and medulla B) Renal cortex, renal medulla and renal pelvis C) Renal artery, renal vein and renal pelvis D) Minor calyx, major calyx and renal pelvis |
C) |
|
|
In order to increase the GFR due to myogenic autoregulation, the kidney: A) vasoconstricts the efferent arteriole B) vasodilates the efferent arteriole C) vasodilates the afferent arteriole D) vasoconstricts the afferent arteriole |
A) |
|
|
Active transport has each of the following properties except: A) Competition B) Reaches saturation C) Only occurs in the loop of Henle D) Specific |
C) |
|
|
If the glomerular capillary blood pressure is 45mmHg, the hydrostatic pressure of the Bowmanscapsule is 10mmHg and the pressure created by plasma proteins is 15mmHg, what is the finalfiltration pressure? A) 10mmHg B) 20mmHg C) 30mmHG D) 40mmHg |
B) |
|
|
Hay fever that occurs when people are exposed to pollen involves an excess release of ____ which________ and causes them to ________. A) IgG; binds to pollen particles; release histamine B) IgE; binds to MHCII on macrophages; present pollen antigens to B cells C) IgG; binds to MHCI on mast cells; stimulate the proliferation of cytotoxic T cells D) IgE; binds to Fc receptors on mast cells; degranulate |
D) |
|
|
Identify the correct statement regarding neural control of the digestive system: A) Postganglionic sympathetic neurons release noradrenaline. B) Sympathetic innervation is divided into cranial and sacral divisions. C) Parasympathetic activation inhibits gut muscle activity. D) The myenteric plexus controls secretion within the intestinal wall. |
A) |
|
|
A patient is administered an intravenous solution that is ~500 mOsm. What happens to thispatient's body compartments following administration? (Hint: Normal serum osmolarity~300mOsm) A) ICF osmolarity increases & ECF volume is reduced B) ICF osmolarity increases & ECF volume expands C) ICF osmolarity decreases & ECF volume is reduced D) ICF osmolarity remains isotonic & ECF volume increases |
B) |
|
|
Select the FALSE statement about aldosterone: A) Increased extracellular [K+] stimulates aldosterone release. B) Aldosterone is indirectly stimulated through the RAAS pathway. C) ACE converts renin to angiotensin, which stimulates aldosterone. D) Aldosterone release is inhibited by increased osmolarity |
C) |
|
|
Which of the following regarding glucose handling in the kidney is true?
A) Glucose found in the urine (glucosuria), can be found at transport rates both above and below the renal threshold transport maximum.
B) Glucose reabsorption rate is directly linear to all plasma concentrations of glucose.
C) Glucose is primarily transported by transcytosis, including both exocytosis and endocytosis transport.
D) Glucose uses a Na+ cotransporter to cross the apical membrane, and as such is dependent on the basal membrane Na+/K+ ATPase to help drive reabsorption |
D) |
|
|
Which of the following regarding reabsorption in the nephron is FALSE? A) Bulk flow takes place in the proximal tubule. B) Osmolarity of filtrate in lumen and ISF are approximately equal (~300mOsm). C) Only 1/3 of plasma filtered through the glomerulus gets reabsorbed back into the circulation. D) Regulated reabsorption takes place in the later segments of the nephron |
C) |
|
|
Low dosages of aspirin inhibit blood coagulation by blocking the formation of ______ from______. A) thromboxane A2; prostacyclin B) thrombin; thromboxane A2 C) thromboxane A2; prostaglandin H2 D) arachidonic acid; thromboxane A2 |
C) |
|
|
Which ONE of the following statements regarding renal clearance is INCORRECT? A) If the concentration of substance X is less than the concentration of inulin excreted at thesame filtration rate (steady GFR), this means that substance X must be secreted into the urinefiltrate. B) A rise in plasma creatinine concentrations over time is indicative of a decreasing GFR overtime. C) At healthy physiological plasma concentrations, the filtered load of creatinine = excretionrate of creatinine. D) At healthy physiological plasma concentrations, the clearance of glucose is 0 mL/min |
A) |
|
|
In regards to fluid distribution in the body, the majority of fluid is contained in the __________,while the remaining fluid is stored in the ___________ + ___________. A) ECF; ICF; ISF B) ICF; ECF; plasma C) ECF; plasma; ICF D) ICF; ISF; plasma |
D) |
|
|
Johnny has presented to the emergency department in distress. An arterial blood gas is drawn andhis CO2 is 50mmHg, pH is 7.1 and HCO3- is 12 mEq/L. Normal values: Partial pressure of carbon dioxide (PaCO2): 38 - 42 mmHg. Arterial blood pH: 7.38 - 7.42. Oxygen saturation (SaO2): 94 - 100% Bicarbonate (HCO3-): 22 - 28 mEq/L. Which best describes his condition? A) Respiratory alkalosis B) Metabolic alkalosis C) Respiratory acidosis D) Metabolic acidosis |
D) |
|
|
Which ONE of the following ions is not directly secreted into the filtrate in the nephron? A) HCO3- B) Na+ C) K+ D) H+ |
B) |
|
|
The goal of renin is to _________. A) increase blood pressure by increasing Na+ reabsorption B) cause ADH release to be inhibited, preventing further water loss C) cause vasodilation of vessels, allowing for increased plasma volume storage D) increase blood pressure by decreasing H20 reabsorption |
A) |
|
|
What marker(s) can be used to measure ISF volume? A) 3H2O - Inulin B) Inulin - 125I-Albumin C) Inulin D) 125I-Albumin |
B) |
|
|
Which of the following is NOT a direct function of thrombin? A) activating factor V B) activating factor X C) activating protein C D) activating factor XIII |
B) |
|
|
All are sources of acid (H+) in the body except: A) Ketoacids B) CO2 from tissue metabolism C) Albumin D) Lactic acid |
C) |
|
|
What is a feature of the major histocompatibility complex II? A) Binds with CD28 receptors on T cells B) Recognized by NK cells C) Presents antigens that are synthesized in the cell D) Interacts with CD4 proteins on T cells |
D) |
|
|
Which of the following is NOT a major intracellular buffer? A) Cellular proteins B) Bicarbonate C) Phosphate ion D) Hemoglobin |
B) |
|
|
What enzyme is responsible for activating trypsinogen? A) Pepsin B) Enterokinase C) Procarboxypeptidase D) Chymotrypsin |
B) |
|
|
In response to the presence of food in the duodenum, the increasedrelease of ________ will primarily stimulate an increase in enzyme secretionfrom the exocrine pancreas. A) Glucose-dependent insulinotropic peptide B) Insulin C) Cholecystokinin D) Secretin |
C) |
|
|
__________ ions are produced within parietal cells and transported across the apical membrane via an active transporter while, at the same time, _________ moves across the apical membrane through ion channels.
A) Bicarbonate; chloride
B) Bicarbonate; hydrogen
C) Hydrogen;chloride
D) Hydrogen; bicarbonate |
C) |
|
|
Which of the following is not a function of the liver? A) Synthesis of albumin B) Synthesis and modification of hormones C) Secretion of bile D) Secretion of enzymes for digestion |
D)
|
|
|
Digestion products of lipase readily interact in the lumen of the GItract with: A) Low-density lipoproteins B) Chylomicrons C) Micelles D) Cholesterol |
C) |
|
|
Explain the short reflex of the control of GI function: |
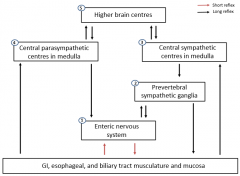
Uses ENS (enteric nervous system)
Local stimulus sensed by receptors (chemo orrestech) which is integrated in ENS and decided/act upon by ENS to facilitatesecretion or motility patterns |
|
|
Explain the long reflex of the control of GI function: |
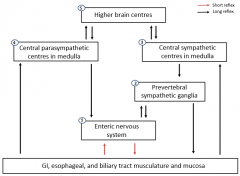
Cooperates CNS ENS signals out to CNS which then signals back to ENS The site or smell of food that tells body to get ready for food Also response to ENS action itself; maybe cause secretion of peptides which then move out further into the body to then tell the pancrease to secrete insulin OR GI peptides signal to the brain that you're hungry or full |
|
|
What is the function of GI motility? |
Moves food from mouth to anus Mechanical mixing of food Generally controlled by the ENS |
|
|
Describe the physiology of the GI smooth muscle and what is it? |
Cells connected by gap junctions to create a functional electrical syncytium Action potential travels in all directions The neurotransmitter are produced and released from varicosities and has broad release over broad region The receptors binding to neurotransmitters and propagate action potential |
|
|
What are the three general patterns of the muscle contraction in gastrointestinal tract? |
Between meals When tract is largely empty Series of contractions begin in stomach and passes slowly from section to sectional |
|
|
What are slow wave potentials? |
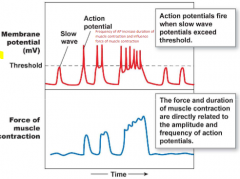
Slow undulating changes
Do not always reach threshold
Frequency of AP increase duration of muscle contraction and influence force of muscle contraction
Cycles of smooth muscle contraction and relaxation are associated with spontaneous cycle of depolarization and repolarization
Likelihood of slow wave firing an AP depends on input from enteric nervous system
When slow wave potential does reach threshold, voltage-gated Ca2+ channels in muscle fiber open Ca2+ enters and cell fires one or more action potentials
Depolarization phase of action potential, like that in myocardial autorythmic cell, is result of Ca2+ entry into the cell Ca2+ entry initiates muscle contraction
Contraction of smooth muscle is graded according to amount of Ca2+ that enter the fiber |
|
|
What happens when there is a longer duration of slow wave potentials? |
Longer the duration, more AP fire, greater contraction force, longer the contraction |
|
|
Are GI smooth muscle contractions spontaneous? |
Yes |
|
|
What are tonic contractions of the GI smooth muscle? |
Sustained for minutes or hours occur in somesmooth muscle sphincters and in anterior portion of stomach |
|
|
What are the phasic contractions of the GI smooth muscle? |
Contraction-relaxation cycles lasting only a few seconds Occur in posterior region of stomach |
|
|
What are the Interstitial cells of the Cajal (ICC)? |
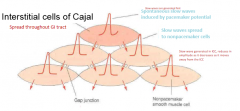
Slow waves originate in this network of cells
Lies between smooth muscle layers and intrinsic nerve plexues
Act as intermediary between the neurons and smooth muscles
Functions as the pacemakers for slow wave activity in different regions of GI tract
Slow waves that begin spontaneously in ICC spread to adjacent smooth muscle layers through gap junctions
Set pace for entire group
Slow wave generated in ICC, reduces in amplitude as it decreases asit moves away from the ICC |
|
|
What are the frequency difference between heart pacemaker cells and ICCs? |
Heart pacemaker cells: ~80/min ICC: Varies through GI tract (3/min to 12/min) |
|
|
What are the node differences between heart pacemaker cells and ICCs? |
Heart pacemaker cells: Point sources or nodes of activity ICC: No nodes/any region capable |
|
|
What is the depolarization of the ICC stimulated by? |
Stretch Parasympathetics (ACh) |
|
|
What is the hyperpolaization of the ICC stimulated by? |
Sympathetic (noradrenaline) Cholecystokinin |
|
|
What does the parasympathetic do to the modulation of the GI muscle? |
Increase gut muscle activity Relaxes sphincters Go into ENS |
|
|
What does the sympathetic do to the modulation of the GI muscle? |
Inhibit gut movements Constrict sphincters Go into ENS |
|
|
What is the migrating motor complex (MMC)? |
A "housekeeping" function that sweeps food remnants and bacteria out of the upper GI tract and into large intestine |
|
|
What are the three phases of the MMC? |
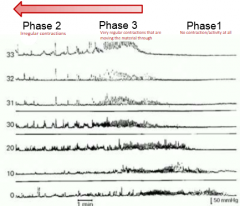
Phase 1: No contraction/activity at all Phase 2: Irregular contraction Phase 3: Vary regular contractions that are moving the material through. Rhythmic contraction of circular muscle that propagates along length of small intestine every 80-110 min |
|
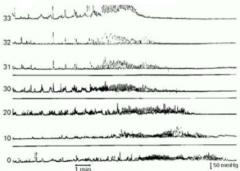
Explain what is going on here: |
This is a recording of intraluminal pressure activity from proximal small intestine in man Note the various components of the migrating motor complex which include phase 2, irregular phasic contractions (seen on the left of the figure), phase 3, a band of rhythmic phasic contractions that slowly migrates through gut (seen in center of figure), and phase 1, motor quiescence (on the right hand side of this figure) This cycle comprising phase 1-3 will continue to occur as long as individual remains fasted |
|
|
What is motilin? |
Secreted by endocrine M cells in crypts in duodenum and jejunum
Hormone released during interdigestive state
Acts on myenteric neurons and smooth muscle cells to regulate the MMC
Measureable at the same time at the MMC but we don't know which oneis first |
|
|
What is deglutition? |
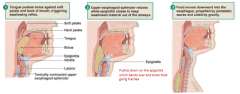
AKA Swallowing
Reflex action that pushes a bolus of food or liquid into esophagus
Stimulus for swallowing is pressure created when tongue pushes the bolus against soft palate and back of stomach
Pressure from bolus activates sensory afferents running through glossopharyngeal nerve (cranial nerve IX) to a swallowing center in medulla oblongata
Output from swallowing center consists of somatic motor neurons that control skeletal muscle of pharynx and upper esophagus as well as autonomic neurons that act on the lower portions of esophagus As reflex begins, soft palate elevates to close off nasopharynx Muscle contraction move larynx up and forward Which help close off trachea and open upper esophageal sphincter As bolus move down toward esophagus, epiglottis folds down This completes closure of upper airway and preventing food and liquid from entering the airways Respiration is briefly inhibited When bolus reaches esophagus, upper esophageal sphincter relaxes Waves of peristaltic contractions then push the bolus toward the stomach, aided by gravity Lower end of esophagus lies just below the diaphragm and is separated from stomach by lower esophageal sphincter |
|
|
What does the pressure from the bolus do in the esophagus cause? |
Activates sensory afferents running through glossopharyngeal nerve (cranial nerve IX) to a swallowing center in medulla oblongata |
|
|
What cranial nerve is the glossopharyngeal nerve? |
9 |
|
|
What is the process of deglutition like? |
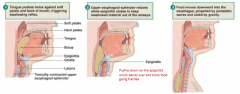
As reflex begins, soft palate elevates to close off nasopharynx Muscle contraction move larynx up and forward (which help close off trachea and open upper esophageal sphincter) As bolus move down toward esophagus, epiglottis folds down This completes closure of upper airway and preventing food and liquid from entering the airways Respiration is briefly inhibited When bolus reaches esophagus, upper esophageal sphincter relaxes Waves of peristaltic contractions then push the bolus toward the stomach, aided by gravity Lower end of esophagus lies just below the diaphragm and is separated from stomach by lower esophageal sphincter |
|
|
What is voluntary swallowing? |
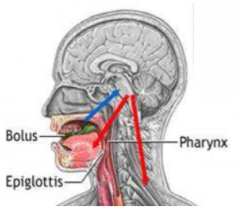
Chewing food and pushing bolus of food toward pharynx by having thetongue touching the hard palate (where tongue is crating smaller space forbolus) Tongue pulled upwards against hard palate Respiration inhibited |
|
|
What is the process of voluntary swallowing? |
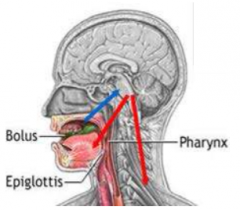
Food activates cranial nerve 9 and 10 Activates swallowing centre in medulla/lower pons Activates cranial nerve 5, 9, 10, and 12 |
|
|
What is another name for the cranial nerve IX? |
Glossopharyngeal nerve |
|
|
What is another name for the cranial nerve X? |
Vagus nerve |
|
|
What is another name for the cranial nerve V? |
Trigeminal nerve |
|
|
What is another name for the cranial nerve XII? |
Hypoglossal nerve |
|
|
What is another name for the cranial nerve VII? |
Facial nerve |
|
|
What is involuntary swallowing? |
Starts once bolus pushes back against soft palate Upward movement of soft palate Closing of epiglottis Base of tongue to push food into esophagus |
|
|
What is the process of involuntary swallowing? |
Food in pharynx causes activation of cranial nerve X Causes activation of swallowing center Causes activation of canial nerve V, VII, IX, X, and XII |
|
|
What is the esophagus? |
Leads to peristalsis and relaxation of lower esophageal sphincter |
|
|
What is the process of esophagus swallowing? |
Food causes activation of cranial nerve X Activation of swallowing center Activation of cranial nerve X Activation of myenteric plexus |
|
|
What what conditions is the esophagus unidirectional? |
Under perfect conditions |
|
|
What is the lower esophageal sphincter? |
Not a true sphincter but a region of relatively high muscle tension that act as a barrier between esophagus and stomach When food swallowed, tension relaxes, allowing bolus to pass into the stomach If does not stay contracted, gastric acid and pepsin can irritate the lining of esophagus, leading to pain and irritation of gastroesophageal reflux (heartburn) During inspiratory phase of breathing: When intrapleural pressure falls, walls of esophagus expand This expansion creates subatmospheric pressure in esophageal lumen and can suck acidic contents out of the stomach if the sphincter is relaxed |
|
|
What is peristalsis? |
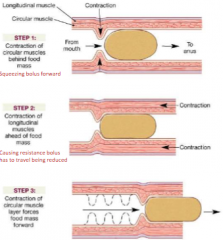
Main action to push bolus forward Progressive waves of contraction Propel food through GI tract (primary and secondary) Stimulated by distention and the bolus |
|
|
What is primary peristalsis? |
Movement of bolus but requires pharyngealstage (bolus being dropped in) |
|
|
What is secondary peristalsis? |
Doesn't have pharyngeal component stage Something stopped in esophagus (feels pain as there is still peristalsis happening/contraction) |
|
|
What are the steps in peristalsis? |
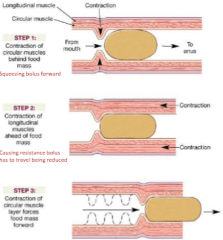
Step 1) Contraction of circular muscles behind food mass (squeezing bolus forward) Step 2) Contraction of longitudinal muscles ahead of food mass (causing resistance bolus has to travel being reduced) Step 3) Contraction of circular muscle layer forces food mass forward |
|
|
Explain the intrinsic regulation of peristalsis: |

Contraction by ACh and substance P via excavator motor neurons Relaxation via inhibitory neurons that release NO, vasoactive intestinal peptide and ATP Afferent neurons will signal through interneurons which is going to be relayed into circular muscle behind bolus causing contraction due to ACh from neurons Want to make sure there is no contraction of circular muscles in front There is usually inhibition of these muscles because of NO, vasoactive intestinal peptide and ATP |
|
|
What are the three general functions of the stomach? |
Storage (stomach stores food and regulates its passageinto small intestine) Digestion (stomach chemically and mechanically digestfood into soupy mixture of uniformly small particles called chyme) Protection (stomach protects the body by destroying manyof bacteria and other pathogens that are swallowed with food or trapped inairway mucus) |
|
|
What is the receptive relaxation of the stomach? |
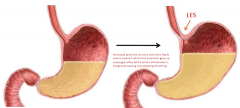
Increased presence as more and more foods enters stomach which thisextension goes up vasovagal reflex which where information is integratedcausing it to allowing stretching |
|
|
What is retropulsion of the stomach? |
Mechanical breakup of food where food is being jetted/slushed back as it goes back through a small diameter This breaks food into smaller pieces |
|
|
What is segmental contraction in the small intestine? |
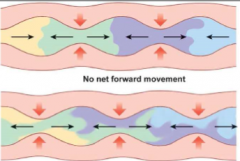
Localized concentric contractions at intervals along the intestine
Circular muscle contract/longitudinal relax
Where digestion (mixing of enzymes/chyme) and absorption (contact of chyme with intestinal wall) can happen
Short
Occur randomly
During contraction, digesting material propelled short distances |
|
|
What is the ileocecal valve? |
Controls emptying of small intestine and prevents back flow
Opened by distention of ileum and by the gastroileal reflex Closed by distension of the colon |
|
|
What causes the ileocecal valve to open? |
Distention of ileum Gastroileal reflex |
|
|
What causes the ileocecal valve to close? |
Distension of the colon |
|
|
What is mass movement in the large intestine |
1-3 per day - usually after a mean A gastrocolic reflex Waves of contraction moves content large distances Slow (5-10 cm/hour) Controlled by ENS< parasympathetic (+) and sympathetic (-) nervous system |
|

Lets say the picture on the left happened before the picture on the right and the person has yet to go to the washroom (defecate), how can this happened? |
Gets pushed into rectum but if the timing is not ready (socially acceptable, person holding it back, individual preventing it), it movesback and get out of the rectum |
|
|
What is defecation? |
Parasympathetic stimulation enhances mass movement in descending and sigmoid colon Relaxation of external sphincter Contraction of abdominal muscle, expulsion of feces |
|
|
What is the process of defecation? |
Rectal distension enhances ENS Causes paristalsis in rectum and relaxation of internal anal sphincter |
|
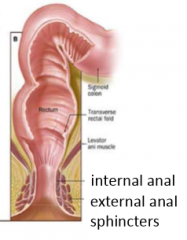
Of the internal and external anal sphincters, which one is voluntary and involuntary? |
Involuntary: Internal Voluntary: External |
|
|
What is an emetic? |
Chemical that causes you to vomit |
|
|
What is emesis? |
Vomiting Forceful expulsion of gastric and duodenal contents from mouth Protective reflex that removes toxic materials from GI tract before they can be absorbed |
|
|
What can excessive or prolonged vomitting cause? |
Excessive or prolonged vomiting, with its loss of gastric acid, can cause metabolic alkalosis |
|
|
What happens to the vagus during emesis? |
Enhances salivation Relaxes esophagus LES Body relaxes pylorus |
|
|
What happens to the spinal nerves during emesis? |
Inspiration Contract abdominal muscles |
|
|
What happens to the phrenic nerves during emesis? |
Diaphragm descends |
|
|
What happens to the stomach during emesis? |
Undergoes reverse peristalsis |
|
|
What are some stimulus for emesis? |
Chemicals in blood (such as cytokines and certain drugs) Pain Disturbed equilibrium (such as moving car or rocking boat) Tickling of back of pharynx |
|
|
Why is respiration inhibited during emesis? |
Done to prevent vomitus from behind inhaled If happens, can cause damage to respiratory system or aspiration pneumonia |
|
|
What is irritable bowel syndrome? |
Chronicfunctional disorder characterized by altered bowel habits and abdominal pain |
|
|
What is gastroparesis? |
Delayed gastric emptying More than a third of all diabetics Migrating motor complex is absent between meals and stomach empties very slowly after meals Patients suffer nausea and vomiting |
|
|
What is saliva? |
Water and mucus in saliva soften the lubricate food to make it easier to swallow a dry soda cracker without chewing it thoroughly Saliva also dissolves food so that can we taste it Chemical digestion begins with secretion of salivary amylase (amylase breaks starch into maltose after enzyme is activated by Cl- in saliva) Final function of saliva is protection |
|
|
How does saliva function as protection? |
Lysozyme is an antibacterial salivary enzyme Salivary immunoglobulins disable bacteria and viruses Saliva helps wash teeth and keep tongue free of food particles |
|
|
What is lactose? |
A disaccharide composed of glucose and galactose Ingested lactose must be digested before it can be absorbed (done by lactase) |
|
|
What is lactose intolerance? |
If a person with lactose intolerance drinks milk or eats dairy products, diarrhea may result Bacteria in large intestine ferment lactose to gas and organic acids, leading to bloating and flatulence Remedy is to remove milk products from diet, although milk predigested with lactase is available |
|
|
What is a remedy for lactose intolerance? |
Remove milk products from diet, although milk predigested with lactase is available |
|
|
What are M cells? |
M cells provide information about contents of lumen to immune cells of GALT Microvilli of M cells are fewer in number and more widely spaced than the typical intestinal cell Apical surface of M cells contain clathrin-coated pits with embedded membrane receptors M cell uses transcytosis to transport them to its basolateral membrane |
|
|
What is the rugae? |
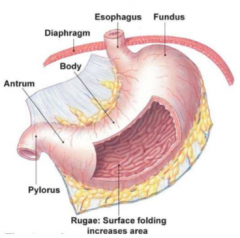
The rugae mainly needed so the stomach was withstand when you eat a meal It provides more volume |
|
|
What is the Haustra? |
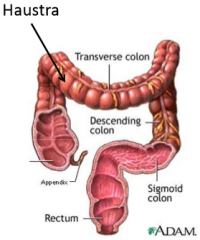
These increase SA, allowing for absorption It has pits that increases SA |
|
|
Where is saliva produced? |
Salivary glands |
|
|
What is the function of saliva? |
Protection Lubrication Taste Digestion |
|
|
Explain salivation under neural control under unconditioned response: |
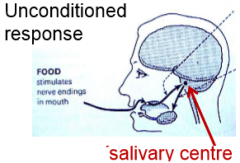
Taste of food, having stimulation of nerve endings in the mouth These trigger salivation |
|
|
Explain salivation under neural control of an conditioned response: |
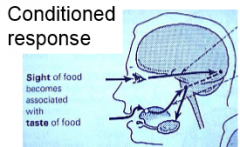
Site, smell or listening to food being cook can cause you to salivate Not direct nerve endings in the mouth |
|
|
What is secreted from mucous cells from the stomach? |
Mucus Bicarbonate |
|
|
What is secreted from parietal cells from the stomach? |
HCl Intrinsic factor |
|
|
What is secreted from chief cells from the stomach? |
Pepsinogen Gastric lipase |
|
|
What is secreted from enterochromaffin-like cells from the stomach? |
Histamine |
|
|
What is secreted from D cells from the stomach? |
Somatostatin |
|
|
What is secreted from G cells from the stomach? |
Gastrin |
|
|
What does mucous and bicarbonate protect? |
The stomach lining |
|
|
What are the gastric mucous cells? |
They secrete mucous to provide thick layer on top of cells and also secrete bicarbonate The mucous is protecting and forming physical barrier between stomach acid and the cells |
|
|
What is the parietal cell? |
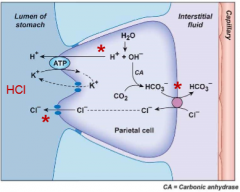
Secrete HCl (acid) and intrinsic factor into the lumen of the stomach Has proton/K+ ATPase where protons are pumped against its concentration gradient Deep in gastric glands Cytoplasmic pH of parietal cells is about 7.2 |
|
|
What does the acid (HCl) secreted from parietal cells do? |
Kill bacteria Denature proteins Activates pepsinogen |
|
|
What does the instrinsic factor secreted from parietal cells do? |
Binds to vitamin B12 (cobalamin)
Ensure absorption of vimtain B12 in ileum |
|
|
What is the parietal cell pathway for acid secretion? |
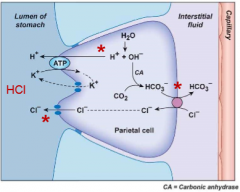
Begins with H+ from water inside parietal cell pumped into stomach lumen by H+-K+-ATPase in exchange for K+ into cell Cl- then follows H+ through open chloride channels, resulting in net secretion of HCl by cell |
|
|
What are chief cells? |
Secrete pepsinogen and gastric lipase |
|
|
What does pepsinogen go? |

Is cleaved to form active pepsin in lumen of stomach by action of H+ Pepsin is an endopeptidase that carries out the initial digestion of proteinsom |
|
|
What are G cells? |
Found deep in gastric glands Secrete the hormone, gastrin, into the blood |
|
|
What is gastrin? |
Binds to receptors on enterochromaffin-like cells Stimulates release of acid, histamine and pepsinogen Increases stomach motility and mass movements |
|
|
What can gastrin be stimulated by? |
Presence of amino acids and peptides in stomach By distension of stomach Neural reflexes mediated by gastrin-releasing peptide Coffee (even decaffeinated) |
|
|
What pancreatic secretions enter the small intestine? |
Pancreatic amylase, pancreatic lipase, nucleases, inactive proteases (trypsinogen, chrmotrpsinogen, procarboxypeptidase, proelastase); all secreted by Acinar cells Sodium, bicarbonate and water; all secreted by duct cells |
|
|
What does enterokinase (enteropeptidase) do? |
Breaks down proteins, specifically break down trypsinogen It is the substrate for the enteropeptidase |
|
|
What are brush order enzymes? |
Enzymes bound to membrane of microvilli Convert small carbohydrates into monosaccharides |
|
|
What is cystic fibrosis transmembrane regulator? |
CFTR CFTR is channel that functions For Cl- to leave the cell When Cl- leaves, it drags H2O and Na+ out with it End up making a watery secretion with lots of bicarb in it |
|
|
What is Acini? |
Lobulues that exocrine portion of pancreases consists of These open into ducts whose lumens are part of the body's external environment |
|
|
What does bicarbonate secretion into duodenum do/cause? |
Neutralize acid entering the stomach |
|
|
Explain the process of bicarboante production in pancreatic duct cell and/or duodenal cells: |
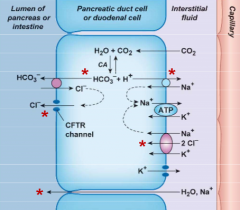
Produced from CO2 and water, secreted by apical Cl--HCO3- exchanger Chloride enters cell on basolateral NKCC cotransporter and leaves via apical CFTR channel Luminal Cl- then re-enters the cell in exchange for HCO3- entering lumen Hydrogen ions produced along bicarbonate leave cell on basolateral Na+-H+ exchangers H+ reabsorbed into intestinal circulation which helps balance HCO3- put into blood when partials cells secrete H+ into stomach |
|
|
Why do individuals with cystic fibrosis have to ingest pancreatic enzymes? |
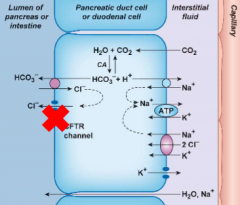
Thick mucus builds up in pancreatic ducts so enzyme scannot travel to small intestine |
|
|
What is secreted from the liver into small intestine via the gall bladder? |
Bile (bile salts, lecithin, cholesterol, bilirubin, bicarbonate)
|
|
|
What is bile? |
Nonenzyme solution secreted from hepatocytes(liver cells) Three key components: bile salts, bile pigments and cholesterol Secreted into hepatic ducts that lead to thegall bladder (stores and concentrates bile solution) |
|
|
What are bile salts? |
Facilitate enzymatic fat digestion Act as detergents to solubilize during digestion Made from steroid bile acids combined with amino acids |
|
|
What are bile pigments? |
Waste products of hemoblogin degradation |
|
|
What is bile salt recycling/enterohepatic circulation? |
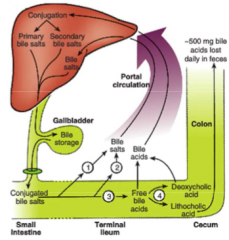
1 and 2 are passive or active transport, 3 and 4 are bacteria mediated absorption Secreted into small intestine Some converted by bacteria, most are being reabsorbed back to the blood (venus blood that takes blood away from the intestine), and then goes to the hepatic portal circulation which leads to the liver Bile salt is recycled and reabsorbed Lots glucose goes first into the liver before goes into the general circulation There is recycling of bile salt and being used over and over again before some are eliminated into the feces (not much though) |
|
|
Where is primary bile acid synthesized? |
Liver |
|
|
What is secondary bile acids created by? |
Bacterial conversion in intestine |
|
|
In one sentence, how is bile acid converted into bile salt? |
Conjugation with amino acid glycine or taurine |
|
|
What hormones are released from small intestines? |
Secretin Cholecystokinin (CCK) Glucose-dependent insulinotropic protein (GIP) Motilin Glucagon-like peptide-1 (GLP-1) |
|
|
What is secretin? |
Acid in small intestine trigger release of secretin Cause increase release of pancreatic bicarbonate to neutralize the acid Causes decrease gastric acid secretion and gastric emptying |
|
|
What is cholecystokinin (CCK)? |
Stimulated by fatty acids and amino acids in small intestine Cause increase release of pancreatic enzymes Causes decrease gastric acid secretion and gastric emptying |
|
|
What is glucagon-like peptide-1 (GLP-1)? |
Stimulated by fatty acids and carbohydrates in small intestine Creates feeling of satiety Increases insulin and beta cell growth Decreases glucagon and gastric acid secretion and gastric emptying |
|
|
What is the gallbladder? |
An organ that is not essential for normal digestion If duct becomes blocked by hard deposits (known as gallstones), gallbladder can be removed without creating long-term problems |
|
|
What is gastric acid? |
An organ that is not essential for normal digestion If duct becomes blocked by hard deposits (known as gallstones), gallbladder can be removed without creating long-term problems Example is HCl |
|
|
What does somatostatin (SS) do in/for the gastric phase of secretion? |
Primary negative feedback signal
Shuts down acid secretion directly and indirectly and also inhibits pepsinogen secretion |
|
|
What does maltase do? |
It is an enzyme that turns maltose into 2 glucose |
|
|
What does sucrase do? |
It is an enzyme that turns sucrose into 1 glucose and 1 fructose |
|
|
What does lactase do? |
Turns lactose into 1 glucose and 1 galactose |
|
|
What is a disccharidase? |
Brush-border enzymes Breakdowns disaccharides |
|
|
What is endopeptidase? |
Digests internal peptide bonds Commonly called proteases Attack peptide bonds in interior of amino acid chain and break long peptide chain into smaller fragments Secreted as inactive proenzymes from epithelial cells in stomach, intestine and pancreas Activated in GI tract lumen |
|
|
Give three examples of endopeptidase: |
Pepsin Trypsin chymotrypsin |
|
|
What is a exopeptidase? |
Digest terminal peptide bonds to release amino acids
Release single amino acids from peptides by chopping them off the ends, one at a time Two isozymes: carboxypeptidase and aminopeptidase |
|
|
Where are carboxypeptidase secreted by? |
Pancreas |
|
|
What does lipase do? |
Breaks down triglycerides into monoglycerides |
|
|
What does colipase do? |
Breaks down triglycerides into free fatty acids |
|
|
What does amylase do? |
Breaks long glucose polymers into smaller glucose chains and into disaccharide maltose Digestion continues in stomach until the amylase is exposed to low pH |
|
|
How much of the starch in the mouth is broken down into maltose? |
5% |
|
|
What is more potent, pancreatic or salivary amylase in small intestine? |
Pancreatic amylase |
|
|
Explain fructose absorption in the intestines: |
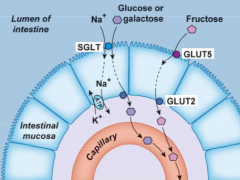
Not Na+ dependent Moves across apical membrane by facilitated diffusion on GLUT5 transporter and across basolateral membrane by GLUt2 |
|
|
Explain glucose absorption in the intestines: |
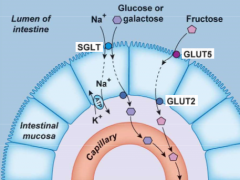
Glucose enters the cell with Na+ on the SGLT symporter and exits on the GLUT2 |
|
|
What is pepsinogen released from? |
Chief cells |
|
|
What does pepsin do? |
Cleaves proteins at aromatic amino acids such as phenylalanine, tryptophan and tyrosine Endopeptidase |
|
|
What is the process of activation of pancreatic enzymes? |
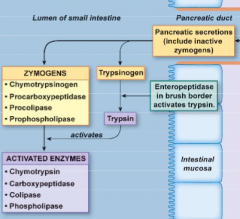
1) In pancreatic duct, there will be pancreatic secretions (include inactive zymogens) 2) Trypsinogen secreted and activated into Trypsin by enteropeptidase in brush border tyrpsin 3) Trypsin activates zymogens (chymotrypsinogen, procarboxypeptidase, procolipase, prophospholipase) into activated enzymes (chymotrypsin, carboxypeptidase, colipase, phospholipase) |
|
|
What is PepT1? |
An oligopeptide transporter Carries dipeptides and tripeptides into mucosal cells Uses H+ dependent cotransporter |
|
|
What does amphipathic mean? |
Have both hydrophobic region and hydrophilicregion |
|
|
What are bile salts? |
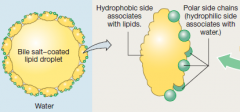
They increase surface area of fat for further digestion Is amphipathic They help form micelles |
|
|
Describe the hydrophobic regions of bile salts: |
Associate with surface of lipid dropletswhile polar side chains interact with water, creating stable emulsion of small,water-soluble fat droplets |
|
|
Explain fat absorption: |
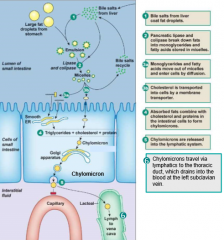
Micelles contact brush border Monoglycerides and free fatty acids diffuse into cell Re-esterify to triglycerides in smooth ER Cholesterol enters via an enery-dependent transporter (NPC1L1) Triglycerides to Golgi assemble with proteins to form chylmicrons Chylmicrons packaged into vesicles and secreted from cell via exocytosis Absorbed by lymphatic system |
|
|
What is ezetimibe? |
A drug that inhibits cholesterol absorption |
|
|
What are chylomicrons? |
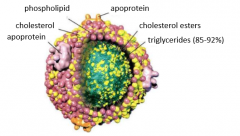
Used for energy or stored as triglycerides Chylmicron remnants taken up by liver Triglycerides joined with cholesterol and proteins to form large droplets Must be packaged into secretory vesicles and leave cell by exocytosis Large size of these prevent them from crossing basement membrane to enter capillaries Are absorbed into lacteals (lymph vessels of villi) Pass through lymphatic system and finally enter the venous blood just before it flows into heart |
|
|
How are fat soluble vitamins absorbed? |
Absorbed with fat |
|
|
How are water soluble vitamins absorbed? |
Absorbed via transporter |
|
|
Is Vitamin A a fat soluble or water soluble vitamin? |
Fat |
|
|
Is Vitamin B a fat soluble or water soluble vitamin? |
Most are water soluble |
|
|
Is Vitamin C a fat soluble or water soluble vitamin? |
Water |
|
|
Is Vitamin D a fat soluble or water soluble vitamin? |
Fat |
|
|
Is Vitamin E a fat soluble or water soluble vitamin? |
Fat |
|
|
Is Vitamin K a fat soluble or water soluble vitamin? |
Fat |
|
|
What is Vitamin B12? |
AKA Cobalamin Made by bacteria but also in seafood, meat and milk Intestinal transporter for B12 found only in ileum and recognizes B12 only when vitamin is complexed withprotein called intrinsic factor |
|
|
In an absence of intrinsic factors, what happens with vitamin B12? |
Will cause pernicious anemia Vitamin B12 deficiency which will severely diminish red blood cell synthesis |
|
|
What is pernicious anemia? |
Red blood cell synthesis is severely diminished |
|
|
What increases the levels of calbindin? |
Calcitriol/1,2-dihydroxyvitamin D3 |
|
|
What decreases ferroportin? |
Hepcidin |
|
|
Where is the hormone hepcidin released from? |
Liver |
|
|
What is ferroportin? |
An iron transporter for iron absorption |
|
|
What are the two ways water can be moved and/or be absorbed in the intestine? |
1) Osmosis (aid by transporters of solutes) 2) Co-transporters |
|
|
What is cellulose? |
Humans are unable to digest because we lack necessary enzymes Can be known as dietary fiber or roughage and is excreted undigested |
|
|
What is sucralose? |
AKA Splenda Artificial sweetener made from sucrose Cannot be digested because chlorine atoms substituted for three hydroxyl groups block enzymatic digestion of sugar derivative |
|
|
Why can sucralose not be digested in humans? |
Chlorine atoms substituted for three hydroxyl groups block enzymatic digestion of sugar derivative |
|
|
What does carboxypeptidase do? |
Removes single amino acids from COOH end of the protein |
|
|
How can lipase penetrate bile salts |
By using co-lipase to displace bile salts, allowing lipase access to fat inside bile salt coating |
|
|
What is swallowing? |
Cephalic phase ends here The anticipation of food, pushing the bolus of food to the back of the mouth to then initiate the swallowing reflex Delivering the food into the pharynx, going pass the esophageal sphincter It is pushing the bolus of food down the esophagus by peristalsis |
|
|
In detail, explain the process of swallowing? |

1) Tongue pushes bolus against soft palate and back of mouth, triggering swallowing reflex 2) Upper esophageal sphincter relaxes while epiglottis closes to keep swallowed material out of airways 3) Food moves downward into the esophagus, propelled by peristalsis waves and aided by gavity |
|
|
Very briefly, describe the process of swallowing? |
Food activates cranial nerve 9 and 10 Activates swallowing centre Activated cranial nerve 5,7,9,10,12 Causes individual to swallow |
|
|
What does vagus stimulation do to the stomach? |
Stomach secretion from different types of cells |
|
|
What is the cephalic phase control of small intestine? |
CN nerves to medulla
Vagus stimulates pancreatic secretion
The gastrin will signal to the pancreatic cells
The gastrin doesn't act locally
Gastrin is then signaling forward, causing secretion from the enzymes and the bicarb from duct cells in the pancreas
Also have vagus nerve to control the release of enzymes from duct cells |
|
|
Victor, a 55-year old male, has gone out with his wife to celebrate their 25th wedding anniversary. They order steak with a cream sauce, chcolate cake and a bottle of wine. When they get home, Victor goes to bed immediately. He awakens with a burning sensation in his lower chest that spreads toward his neck. The pain is alleviated with antacids. Are there any long-term risks if this condition persists? |
GERD (Gastroesophageal reflux disease) can cause Barret's esophagus - potential precursor to esophageal cancer The case where cells in the esophagus can change (mucous secreting cells) Cells are transforming, always running at the risk of cancer Abnormal cells can become cancerous What is changing these cells is the fact that they are being irritated due to the acidic chyme, the acid from the stomach that is splashing up into the lower esophagus |
|
|
What happens when there is no reflux in the stomach? |
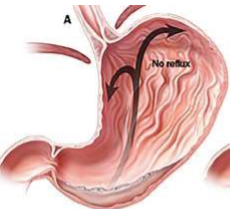
The LES (Lower esophageal sphincter) is tight The peristalsis taken place, allowing activities to take place in the stomach only |
|
|
What happens if there is reflux in the stomach? |
The sphincter is not tight, therefore contents from the stomach and go up If the stomach is full, then the chances of splash through the opening of LES is increased If you're lying down, there is even greater chance for the acidic contents to splash through the |
|
|
What are the causes of GERD? |
Fatty meals Alcohol Caffeine Chocolate Peppermint Any increase relaxation of LES |
|
|
How does fatty meals cause GERD? |
Decrease motility patterns, therefore staying in stomach longer |
|
|
How does caffeine and alcohol cause GERD? |
Increase acidity in stomach |
|
|
What are some treatments for GERD? |
Lifestyle changes: reduce weight, eat small meals, ear earlier in the evening, stop smoking Drugs: reduce acid secretion or enhance stomach emptying |
|
|
How does seeing or smell food cause effector cells to increase secretion and motility in stomach? |

This is a long reflex
1) Seeing food and smell food activates medulla
2) Send signals to stomach for gastric secretion by having medulla oblongata cause the preganglionic parasympathetic neurons in vagus nerve to activate enteric plexus
Now begins short reflex
3) Enteric plexus cause postganglionic parasympathetic and intrinsic enteric neurons to cause effector cells to increase secretion into stomach and motility in stomach to aid in mixing of contents in stomach |
|
|
What happens when pH is elevated in stomach? |
Anytime the pH is elevated (not acidic enough) it will trigger stretch receptors and chemoreceptors to local areas to trigger mucous cells, to secrete various secretions Gastrin also increases motility |
|
|
Explain regulation of stomach secretions: |
1) Food or cephalic reflexes initiate gastric secretion 2) Gastrin stimulates acid secretion by direction action on parietal cells or indirectly through histamine 3) Acid stimulates short reflex secretion of pepsinogen 4) Somatostatin release by H+ negative feedback signal that modulates acid and pepsin release |
|
|
What cells secretion somatostatin? |
D cells |
|
|
What are ulcers? |
Ulcers are the breakdown of the mucosa You start to lose mucosa surface, underneath the blood vessels will be exposed and leads to bleeding into the stomach Mainly caused by Helicobacter pylori (a bacteria) |
|
|
What are the causes of peptic ulcers? |
Mainly Helicobacter pylori Also by: drugs (NSAID), excessive acid (Zollinger Ellison, Pseudo-Zollinger Ellision, G cell hyperplasia), Stress ulcers (organ trauma, head injury) |
|
|
How does H. pylori survive in the stomach? |
They have urease The bicarb acts to buffer the protons The bacteria cause the bacteria to create the pedestals to protect the bacteria The bacterium release molecules to induce inflammatory response and cause damage to the cell Causes the cell to release IL-8 Release reactive oxygen species |
|
|
How is a breath test for H. pylori infection done? |
Drink urea containing 14C isotope then measure 14CO2 in breath If H. pylori found in stomach, the urease will convert the urea to bicarb The bicarb will be labelled That will travel into the blood stream main way for CO2 to be transported Carbonic anhydrase will convert these bicarb into CO2 If you have radioactivity, this indicates that you have H. pylori infection |
|
|
What are some treatments for H. pylori infection? |
H+/K+ pump inhibitors Antibiotics H2 antagonist |
|
|
What does secretin do and where released from? |
Released from S cells
Stimulates fluid and HCO3- secretion Can inhibit of chief and parietal cells Stimulated by decreased pH |
|
|
What does CCK do and where is it released from? |
Released from I cells Stimulates secretion of pancreatic enzymes Stimulated by presence of lipids and carbohydrates |
|
|
What are the two effects of the intestinal phase? |
Cause bicarb to be secreted to neutralize acid Enzymes are active when solution is neutral |
|
|
Johanna is a 4-year old Haitian girl who is living in Artibonite Departmente, approximately 50 miles north of Port-au-Prince She ate food contaminated with Vibrio cholerae and has developed cholera. Vibrio cholerae produces a toxin which permanently activates Gs(alpha) leading to excess production of cAMP in her intestinal epithelial cells. How do these changes influence water and electrolyte absorption? |
She is not getting proper water and sodium absorption
|
|
|
Johanna is a 4-year old Haitian girl who is living in Artibonite Departmente, approximately 50 miles north of Port-au-Prince She ate food contaminated with Vibrio cholerae and has developed cholera. Vibrio cholerae produces a toxin which permanently activates Gs(alpha) leading to excess production of cAMP in her intestinal epithelial cells. Oral rehydration therapy is used to treat this condition. How does it help? |
Needs to drink lots of water, including Na+ and K+ and glucose |
|
|
Who is William Harvey? |
1578 - 1657 First to figure out lungs were used for breathing, before him, theythought it was for cooling down the blood |
|
|
What is cellular respiration? |
Intracellular reaction of oxygen with organic molecules to produce CO2, water and energy in form of ATP Cell getting oxygen and releasing CO2 |
|
|
What is external respiration? |
Interchange of gases between environment and the body's cells and tissue |
|
|
What are the functions of the respiratory system? |
1) Gas exchange between air and cell (bringing air inside lungs, diffusing into blood stream and going totissuesmode) 2) Regulation of pH (more you breath, more created CO2, decrease pH) 3) Defence from inhaled pathogens/foreign particles (cilia that trap bacteria inside airways) 4) Vocalization (communication) |
|
|
Briefly, what is the larynx? |
Voice box Mkaes sound/voices |
|
|
What is the trachea made of? |
A rigid tube with rings of cartilage |
|
|
What does the upper respiratory tract consist of? |
Nasal cavity Tongue Larynx Pharynx (naso-, oro-, and eso-pharynx) Vocal chords Esophagus |
|
|
What does the lower respiratory tract consist of? |
Trachea Right and left lungs Right and left bronchus Diaphragm |
|
|
Of the respiratory muscles, what does the inspiratory muscles consist of? |
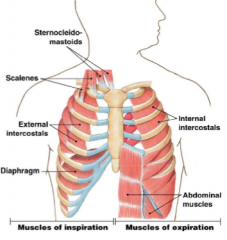
Diaphragm muscle Upper airway muscle Sternocleidomastoids Scalenes External intercostals |
|
|
What happens to lung volume when diaphragm moves down? |
It increases |
|
|
What are inspiratory muscles activated? |
In respiration |
|
|
Of the respiratory muscles, what does the expiratory muscles consist of? |
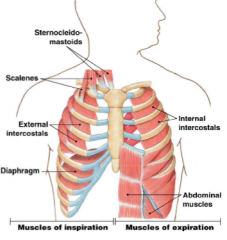
Abdominal muscles Internal intercostals |
|
|
What is congenital diaphragmatic hernias? |
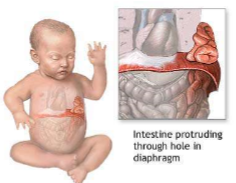
Congential diaphragmatic hernia (CDH) is a congential malformation (birth defect) of the diaphragm Usually an opening in the diaphragm |
|
|
What are the symptoms of congenital diaphragmatic hernias? |
Severe breathing difficulty, almost always develops shortly after baby is born because of ineffective movement of diaphragm and crowding of lung tissue which causes collapse This impacts development of lungs causing them to have smaller lungs |
|
|
What are the causes of congenital diaphragmatic hernias? |
Improper joining of structures during fetal development |
|
|
What is the treatment for congenital diaphragmatic hernias? |
Surgery is done to place the abdominal organs into proper position and repair the opening in diaphragm |
|
|
What is the function of the pleural fluid and sac? |
1) Creates a moist, slippery surface facilitating movements (lubrication so lung can move and slide inside) 2) Holds the lungs tight against the thoracic wall (suction/adherence) |
|
|
What happens when you do not have a negative pressure in the lungs (a positive pressure)? |
If you don’t have it, the lungs will collapse and won't be able to expand |
|
|
Of the parietal and visceral pleura, which one is attached to the lungs? |
Visceral |
|
|
What muscles does the airways of humans consist of? |
Pharynx Mouth Nasal cavity Larynx Trachea Bronchus Bronchiole Alveoli |
|
|
How many bronchi does the trachea branch into? |
2 (two) |
|
|
What is the function of the airways? |
Passage for air from mouth/nose to alveoli 1) Warm air to 37 degrees 2) Humidify air to 100% 3) Filter particles (through nose and respiratory cilia) 4) Vocalization |
|
|
Briefly, what happens if you have dry air coming into the airway? |
The air will not go through gas exchange |
|
|
What is an endotracheal tube in mechanically-ventilated patients? |
To bypass upper airways and give artificial ventilation |
|
|
What are the consequences of using a endotracheal tube in a mechanically-ventilated patients? |
Lower airways losing heat and water and secretions would thicken Secretions (mucus) may accumulate and block airways |
|
|
How do you get around the consequences of using a endotracheal tube in mechanically-ventilated patients? |
Heated tube and 100% humidity in inspired gas Make sure air is moist |
|
|
Which bifurcations have cartilage to maintain shape? |
1st (right and left main bronchi) 2nd to 4th (lobar bronchi) |
|
|
Which bifurcations have bronchiolar muscles? |
5th to 11th (segmental bronchi) 12th to 16th (terminal bronchioles) |
|
|
Briefly, what is the point of the cilia in the airways? |
Filtration Trap particles |
|
|
What does goblet cells secrete in the airways? |
Mucus |
|
|
What is cystic fibrosis? |
A genetic disease (that affect transport of sodium) that cause thick, sticky mucus to build up in the lungs and digestive tract |
|
|
What are the symptoms of cystic fibrosis? |
Delayed growth in newborns Failure to gain weight No bowel movements in first 2 days after birth Salty tasting skin Coughing and increased mucus in lungs Nasal congestion Pneumonia |
|
|
What causes the salty tasting skin of cystic fibrosis patients? |
Their bad transport of sodium |
|
|
What are the major pathological features of cystic fibrosis? |
Defective chloride ion transport across epithelial cell membrane Lower chloride and sodium levels into the airway lumen which reduce water secretion in airways |
|
|
What is the main mechanism/cause of cystic fibrosis? |
Defective cystic fibrosis transmembrane regulatory (CFTR) protein cause by a genetically mutated gene |
|
|
Where is gas exchanged taken place in the lungs? |
At the alveoli |
|
|
What are type 1 alveolar cells? |
Gas exchangers Big flat cells Oxygen and CO2 diffuse very well here |
|
|
What are type 2 alveolar cells? |
Synthesize and secrete surfactant |
|
|
What are alveolar macrophages? |
Remove foreign particles |
|
|
What happens to an alveoli without surfactant? |

Surface tension pulls molecules inward |
|
|
What happens to an alveoli when it has surfactant? |

Surfactant compensates for surface tension |
|
|
What is alveoli surfactant? |
Covers the side of alveoli It cancels the force of water |
|
|
What is surface tension? |
Molecules of water are attracted together by hydrogen bonds Inside the liquid, molecules are attracted in every direction At the surface, molecules are attracted only sideways and downward, not upward This phenomenon forces liquid to adopt the minimal surface possible |
|
|
What is infant respiratory distress syndrome (IRDS)? |
AKA Neonatal respiratory distress syndrome IRDS is a syndrome in premature infants caused by developmental insufficiency of surfactant production and structural immaturity in the lungs |
|
|
What are the symptoms of infant respiratory distress syndrome? |
Bluish colour of the skin and mucus membranes (cyanosis) because of low oxygen Grunting and nasal flaring Brief stop in breathing (apnea) Rapid breathing shallow breathing Shortness of breathing and grunting sounds while breathing |
|
|
What are the major pathological features of infant respiratory distress syndrome? |
Surfactant deficient lung is characterized by collapsed air-spaces alternating with hyper-expanded areas |
|
|
What are the causes of infant respiratory distress syndrome? |
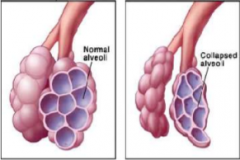
Genetic problem with the production of surfactant associated proteins IRDS affects about 1% of newborn infants and is leading cause of death in preterm infants |
|
|
What are some treatments for IRDS? |
Oxygen is given with small continuous position airway pressure (pure oxygen) Artificial or natural surfactants is administered through the endotracheal tube |
|
|
Is alveolar gas exchange of oxygen a passive or active process? |
Passive diffusion |
|
|
What is (are) the role(s) of the pleural fluid and sacs? A) To lubricate B) To hold lungs tight against thoracic wall C) To expand lungs when thoracic volume increases D) A, B, and C E) A and B |
D) |
|
|
What is (are) the role(s) of type 1 alveolar cells? A) Synthesize and secrete surfactant B) Keep alveoli in spheric shape C) Gas exchange D) B and C E) A and B |
C) |
|
|
Give an overview of a single breath: |
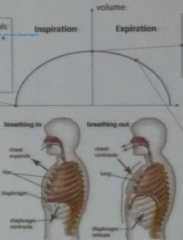
Inspiration: 1) Brainstem send signals to phrenic nerve to activate diaphragm 2) Inspiratory muscles contract 3) Lung expands 4) Air goes in At max lung volume 1) Lung at their peak volume 2) Activation of stretch receptors 3) Diaphragm stops Expiration 1) Diaphragm relaxes 2) Chest contract 3) Air goes out |
|
|
What is rate of breathing? |
Number of breathes per minute |
|
|
What is the diaphragm? |
Main muscle of breathing Controlled by phrenic nerve from spinal segments C3, C4 and C5 Inserted in the lower ribs Move downwards as it contracts |
|
|
What phrenic nerves control the diaphragm? |
C3
C4 C5 |
|
|
Which direction does the diaphragm move when it contracts? |
Downward |
|
|
Which muscles are innervated by intercostal nerves for inspiration? |
External intercostal Sternocleidomastoids Scalenes |
|
|
Which muscles lift ribs and expand thorax during inspiration? |
External intercostal Sternocleidomastoids Scalenes |
|
|
When are expiratory muscles used? |
Passive at rest Used during voluntary expiration or during environmental challenges |
|
|
Briefly, what do internal intercostal muscles do? |
Contract and force ribs inward |
|
|
Briefly, what do abdominal muscles do? |
Force ribs inward and decreases abdominal volume |
|
|
What two things happen to thoracic cavity during inspiration? |
1) Rib cage and thoracic cavity expand 2) Pressure in thoracic cavity decreases and lung expand |
|
|
What happens to respiration muscles when the rib cage and thoracic cavity expands? |
Sternocleidomastoids and scalenes contract Diaphragm muscle contracts and move down |
|
|
If you have lower pressure in the lungs, does air go in or out? |
In |
|
|
If you have higher pressure in the lungs, does air go in or out? |
Out |
|
|
What happens when the pressure in thoracic cavity decreases and lung expands? |
Pressure inside lungs decrease Air comes rushing in |
|
|
What is the intrapleural space? |
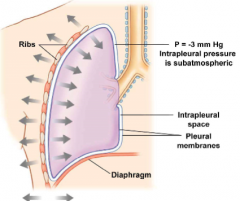
Filled with a few ml of fluid
Because liquid is non-expansible, lungs follow volume changes of the thorax
Pleural membranes are adherent to the lungs and to the thoracic wall by connective tissue
When you have expansion of ribs and negative pressure, it will expand the lungs |
|
|
What is pneumothorax? |
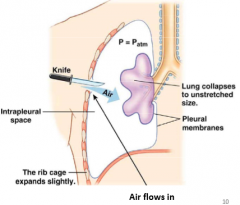
Air in pleural cavity breaks the fluid bond holding the lung to the chest wall Chest wall expands outward |
|
|
What is a first-aid remedy for pneumothorax? |
Apply a wet dressing on the wound to act as a one-way valve (out) and positive-pressure at the mouth to inflate lungs |
|
|
What is hydrothorax? |
Condition that results from blood accumulating in the pleural cavity |
|
|
What are the symptoms of hydrothorax? |
Tachypnea Dyspnea Cyanosis Decreased or absent breath sounds on affected side |
|
|
What is tachypnea? |
Faster and shallow breathing |
|
|
What is dyspnea? |
Difficulty breathing |
|
|
What are the causes of hydrothorax? |
Traumatic (from a blunt or penetrating injury to the thorax) |
|
|
What are the treatments for hydrothorax? |
Removing the source of bleeding and by draining the blood already in thoracic cacvity |
|
|
What is ventilation (of lungs)? |
Ventilation moves air between the environment and the alveoli Air flows into the lungs because of pressure gradients |
|
|
How do you calculate pulmonary ventilation? |
Rate * volume (L/min) |
|
|
How do you calculate Boyle's law? |
P1 * V1 = P2 * V2 |
|
|
What happens to pressure when you expand the lungs? |
It goes down |
|
|
What happens to pressure during inspiration? |
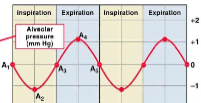
Inspiratory muscles contract Alveolar pressure drops by 1mmHg |
|
|
What happens to pressure at the end of inspiration? |
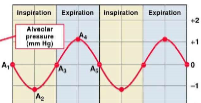
Volume of air is at its maximum Alveolar pressire is equal to atmospheric pressure |
|
|
What happens to intrapleural pressure during expiration? |
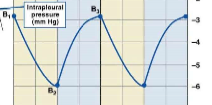
Inspiratory muscles cease Elastic recoil of lungs return to diaphragm and rib cage to original position Air pressure in lungs increase 1mmHg above atm pressure |
|
|
When is alveolar pressure at its lowest? |
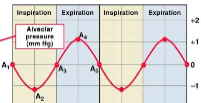
During inspiration |
|
|
When is alveolar pressure at its highest? |
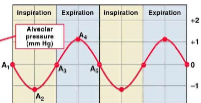
During expiration |
|
|
When is intrapleural pressure at its highest? |
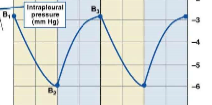
Beginning of inspiration, ending of expiration |
|
|
When is intrapleural pressure at its lowest? |
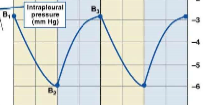
End of inspiration Beginning of expiration |
|
|
What is active expiration? |
Occurs when hyperventilation or CO2 increases Internal intercostal and abdominal muscles |
|
|
What happens during ventilation of dead space volume? |
Air remaining in trachea, bronchi and/or poorly perfused alveoli |
|
|
What is a spirometry? |

Measures volume of air inspired and expired by the lungs |
|
|
What is tidal volume? |
Normal volume of air going in and out of lungs at rest (breathingnormally) |
|
|
In a brief sentence, what is pulmonary ventilation? |
Volume of air moved into and out of the lungs each minute |
|
|
In a brief sentence, what is alveolar ventilation? |
Amount of fresh air that reaches the alveoli each minute |
|
|
In a brief sentence, what is eupnea? |
Normal quiet breathing
|
|
|
In a brief sentence, what is hyperpnea? |
Increased rate and volume in response to changes in metabolism (normal increase) |
|
|
In a brief sentence, what is hyperventilation? |
Increased rate and volume |
|
|
In a brief sentence, what is hypoventilation? |
Decreased (alveolar) ventilation |
|
|
In a brief sentence, what is tachypnea? |
Rapid breathing |
|
|
In a brief sentence, what is dyspnea? |
Difficulty of breathing (feeling) |
|
|
In a brief sentence, what is apnea? |
Cessation of breathing |
|
|
What is lung compliance? |
Degree the lungs will comply by changing their volume when subjected to a change in intrapleural pressure or the ability of the lung to stretch Compliance is a measure of distensibility Define as the change in lung volume produced by a unit of pressure change Degree the lungs will comply by changing their volume when subjected to a change in intrapleural pressure |
|
|
What is lung compliance influenced by? |
Elastic fibre network Surface tension in alveoli |
|
|
What happens when you have low lung compliance? |
Restrictive lung disease such as fibrotic lung disease |
|
|
How do you calculate lung compliance? |
Define as the change in lung volume produced by a unit of pressure change |
|
|
What are elastin fibers? |
In-between two 1 cells Creates sphere shape of alveoli It can stretch during inspiration |
|
|
What is pulmonary fibrosis? |
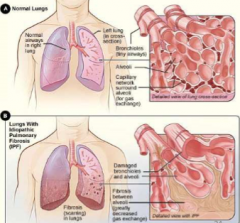
Formation or development of excess fibrous connective tissue (fibrosis) in lungs
"Scarring of the lungs"
Decreases compliance
Alveoli won't be in proper shape anymore and be either really large or small
Cannot be extend/expanded anymore
Won't have sphere anymore means less surface area Reducing exchange of gas |
|
|
What are the symptoms of pulmonary fibrosis? |
Shortness of breath Chronic dry, hacking coughing Fatigue and weakness Chest discomfort Loss of appetite and rapid weight loss |
|
|
What are the two types of flow of air in airways? |
Laminar flow Turbulent flow |
|
|
What is chronic obstructive pulmonary disease (COPD)? |
Is the occurrence of chronic bronchitis (secretion of mucus) and emphysema (destruction of lung tissue) |
|
|
What are the symptoms of chronic obstructive pulmonary disease (COPD)? |
History of cigarette smoking Chronic cought and sputum production (in chronic bronchitis) Dyspnea Decreased intensity of breath sounds and prolonged expiration on physical examination Airflow limitation on pulmonary function testing that is not fully reversible and most often progressive Low FEV1 |
|
|
What are the causes ofchronic obstructive pulmonary disease (COPD)? |
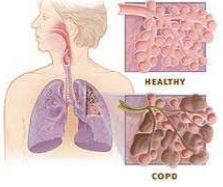
Noxious particles or gas (tobacco smoking) Abnormal inflammatory response in lung |
|
|
What happens during obstructive sleep apnea? |
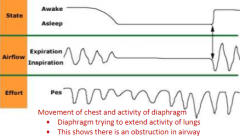
1) Reduction of upper airway muscle activity 2) Diaphragm activity but no flow 3) Rib cage and abdomen movements are opposite (rib cage expands, abdomen contracts) 4) Arousal and breathing resumes |
|
|
What is obstructive sleep apnea (OA) syndrome? |
Blockage of airways during sleep Apnea-hyponea index measures the number of apnea and hyponea Prevelance was estimated at 5% of general popularion having apnea Can lead to cardiovascular diseases with hypertension and stroke |
|
|
What are the symptoms ofobstructive sleep apnea (OA) syndrome? |
Daytime sleepiness Depression and hyperactive behaviours Repeated desaturation during night |
|
|
What are some treatments forobstructive sleep apnea (OA) syndrome? |
Losing weight Continuous positive airway pressure (CPAP) during night Stop drinking alcohol |
|
|
How does losing weight treatobstructive sleep apnea (OA) syndrome? |
Fat in upper airways reduces diameter and increases resistance |
|
|
How does stop drinking alcohol treat obstructive sleep apnea (OA) syndrome? |
Alcohol causes airways to relax which increases likelihood ofobstructive sleep apnea (OA) syndrome |
|
|
What causesobstructive sleep apnea (OA) syndrome? |
Collapse of the upper airways Sleep is reducing upper airway muscle activity Obesity is narrowing upper airway due to accumulation of fat Fluid shift from legs to neck during night |
|
|
In a brief sentence, what is congenital diaphragmatic hernia and what does it cause? |
Malformation of diaphragm Causes breathing difficulty and low tidal volume |
|
|
In a brief sentence, what is asthma and what does it cause? |
Inflammation of airways Causes increased resistance |
|
|
In a brief sentence, what is cystic fibrosis and what does it cause? |
Thick secretion Causes salty skin and delayed growth |
|
|
In a brief sentence, what is pulmonary fibrosis and what does it cause? |
Excess fibrous tissue Causes shrotness of breath, dry cough |
|
|
In a brief sentence, what is emphysema and what does it cause? |
Loss elasticity of alveolar tissue Causes high compliance |
|
|
What is Dalton's law of partial pressure (the equation)? |
Total atmospheric pressure = sum of partial pressures |
|
|
In the body, how you would calculate total atmospheric pressure? |
Patm = PO2 + PN2 + PCO2 + PH2O |
|
|
What is partial pressure equal to? |
Partial pressure = Fractional concentration * Total pressure |
|
|
In alveolus, will it gain/increase or lose/decrease partial pressure of oxygen and carbon dioxide? |
O2: Lose CO2: Gain |
|
|
If you lower CO2 levels, what happens to breathing? |
Slower |
|
|
If you increase CO2 levels, what happens to breathing? |
Faster |
|
|
Does CO2 dissolve well into blood stream? |
Very well yes |
|
|
What is Fick's law of diffusion? |
A passive process Gas transfer is equal to gas constant (k) * partial pressure gradient / wall thickness Increased wall thickness decreases gas transfer |
|
|
In Fick's law of diffusion, what is wall thickness: |
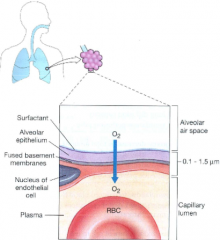
Wall thickness = surfactant + water +alveolar epithelium + fused basement membrane + capillary cells Disease can increase thickness |
|
|
What happens to gas transfer if you increase wall thickness?
|
Decreases gas transfer |
|
|
What is the gas constant (k) in Fick's law of diffusion? |
Solubility og as in alveolar membrane |
|
|
What are the symptoms for asthma? |
Dyspnea Confusion Diaphoresis Tachycardia Cyanosis |
|
|
What are the physiological effects of asthma? |
Inflammation of airways including bronchioles and alveoli Alveolar-capillary membrane changes Ventilation perfusion imbalance Reduced gas exchange |
|
|
What is emphysema? |
Destruction of alveoli means less surface area of gas exchange |
|
|
What happens to PO2 in alevoli and blood during emphysema? |
PO2 normal or low in alevoli PO2 low in blood |
|
|
What is a fibrotic lung disease? |
Thickened alveolar membrane slows gas exchange Loss of lung compliance may decrease alveolar ventilation |
|
|
What happens to PO2 in alevoli and blood during a fibrotic lung disease? |
PO2 normal or low in alveoli PO2 low in blood |
|
|
What is a pulmonary edema? |
Liquid in interstitial space increases diffusion distance Arterial PCO2 may be normal due to higher CO2 solubility Does not affect exchange surface |
|
|
What happens to PO2 in alevoli and blood during pulmonary edma? |
PO2 normal in alveoli PO2 low in blood |
|
|
What happens to PO2 in alevoli and blood during in asthma?? |
Bronchioles constricted so: PO2 low in alveoli and blood |
|
|
What is hematocrit? |
A blood test that measures the percentage of red blood cells in a volume of blood |
|
|
Why would you do a hematocrit test? |
If the patient has signs of anemia, diet deficiency or leukemia |
|
|
What are normal levels of hematocrit? |
Male: 40.7% to 50.3% Female: 36.1% to 44.3% |
|
|
What does it mean if a patient has a low hematocrit? |
Low RBC count in blood Anemia, bleeding, leukemia, malnutrition |
|
|
What does it mean if a patient has a high hematocrit? |
High RBC count in blood Congenital heart disease, dehydration, hypoxia, pulmonary fibrosis, decreased blood ventilation |
|
|
What does the heme group of a hemoglobin molecule do? |
Central iron atom that binds to O2 |
|
|
What happens when a hemoglobin releases its oxygen? |
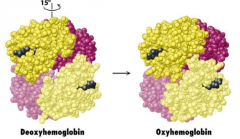
Goes through a conformational change from oxyhemoglobin to deoxyhemoglobin |
|
|
How much of the oxygen of hemoglobin is released in tissues? |
25% |
|
|
What is Bohr effect? |
A mechanism of how oxygen can move through tissue |
|
|
What is the relation between pH and Hb saturation? |
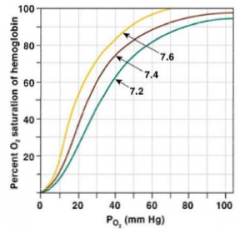
When you increase pH, you increase the the percentage of Hb being saturated by O2 |
|
|
What happens when you lower pH to Hb? |
More oxygen is being released by Hb |
|
|
What is the relation between temperature and Hb saturation? |
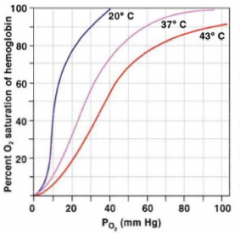
When you increase temperature, you decrease the amount of Hb being saturated by O2 |
|
|
When you decrease temperature, what happens to Hb? |
Less O2 being released by Hb |
|
|
What is the relation between PCO2 and Hb? |
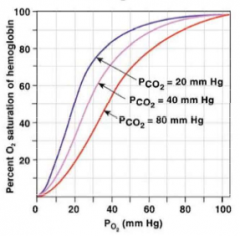
When you increase partial pressure of CO2, you decrease the amount of Hb being saturated by O2 |
|
|
When you decrease PCO2, what happens to Hb? |
Less O2 being released by Hb |
|
|
What causes carboxyhemoglobin? |
Combustion of organic materials produces carbon monoxide Carbon monoixde binds to a hemoglboin and is not being released It hampers the ability of hemoglobin to release oxygen to the tissues CO increases hemoglobin affinity for oxygen |
|
|
What are the treatments for carboxyhemoblogin? |
Air containing 100% oxygen or hyperbaric chamber |
|
|
What are the three forms of CO2 transport? |
1) Dissolved CO2 in the plasma 2) Plasma HCO3- (bicaronate) 3) Protein compounds (carbamino) |
|
|
What is carbonic anhydrase? |
Converts CO2 + water into a bicarbonate molecule |
|
|
What is another name for HbCO2? |
Carbaminohemoglobin |
|
|
What causes respiratory acidosis? |
PaCO2 is above normal but concentration of HCO3- is normal Hypoventilation Narcotic-induced respiratory depression Disease of airways Severe obesity which restrict how much lungs can expand |
|
|
What is a treatment for respiratory acidosis? |
Mechanically assisted ventilation and reversal of narcotic effect |
|
|
What is a pulse oximeter? |
Measures oxygen saturation and oxygen levels Detects two type of lights: infrared (IR) and red Uses ratio of absorption between red and Ir for results |
|
|
In a pulse oximeter, what does a low IR absorption mean? |
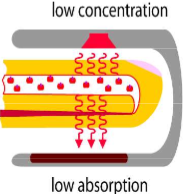
Low concentration of HbO |
|
|
In a pulse oximeter, what does a high IR absoprtion mean? |
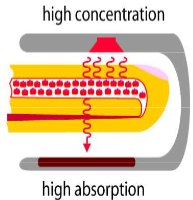
High concentration of HbO |
|
|
What happens to CO2 when you slow down breathing? |
CO2 rises |
|
|
If you have a pO2 of 37mmHg, what does that indicate? |
Severe hypoxia |
|
|
If you have pO2 of 47mmHg, what does that indicate? |
Mild hypoxia |
|
|
If you have a pO2 of 110mHg, what does that indicate? |
Normoxia |
|
|
What is the main stimulus for change in (respiratory) ventilation? |
CO2 |
|
|
Does O2 and pH have an impact on change of (respiratory) ventilation? |
Yes |
|
|
What are central chemoreceptors? |
Located in medulla and some other brain tissue Monitor H+ in cerebrospinal fluid and arterial circulation |
|
|
What are peripheral chemoreceptors? |
Carotid and aortic bodies Monitor arterial levels of oxygen and CO2/H+ Can detect proteins in the blood |
|
|
What happens when protons are detected in the cerebrospinal fluid? |
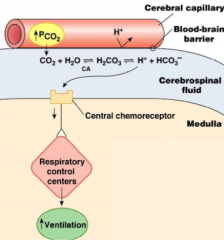
1) Central chemorecetpros would detect protons 2) Closure of K+ channels, causing depolarization of chemoreceptors, causing transmitter release 3) Signals respiratory control centers to increase ventilation |
|
|
What happens if you increase CO2 in the cerebral capillaries? |
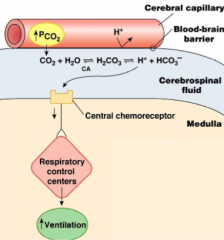
It will diffuse into the CSF Carbonic anhydrase (CA) will convert it into bicarbonates and protons (H+) Get detected by central chemoreceptors and increase ventilation |
|
|
Is the central chemoreceptor response fast or slow? |
"Too" slow |
|
|
What are retrotrapezoid nucleus? |

Cells that respond to change in CO2 Can cause breathing to increase and fire more |
|
|
What can increase the rate of retrotrapezoid nucleus firing? |
Hypercapnia Increase CO2 |
|
|
What are the medullary raphe? |

Located n the brain stem Serotoninergic neurons and are chemosensitive Surrounded by cells that detect change in CO2 and capillaries that go to the brain stem Quick to detect changes |
|
|
What is central sleep apnea? |
The cessation of airflow without respiratory effort Less than 1% of the general population 25-40% of these patients has/had heart failure |
|
|
What is Cheyne-Stokes breathing? |
AKA Periodic breathing Type of central sleep apnea Waxing and warning of breathing There will be saturation of O2 then start going down when patient is no longer breathing |
|
|
What can cause Cheyne-Stoke breathing? |
Heart failure Low sensitivity to CO2 Damage to respiratory centers |
|
|
What is congential central hypoventilation syndrome? |
AKA Ondine's curse Hypoventilation during sleep which may lead to respiratory arrest Patients exhibiting symptoms at birth or early infancy Marked reduction of ventilation and arousal response to CO2 |
|
|
What causes congential central hypoventilation syndrome? |
Mutation of Phox2B gene (a gene coding for transcription factor in autonomic nervous system development) |
|
|
What is the Phox2B gene? |
Agene coding for transcription factor in autonomic nervous system development Phox2B protein found at levels of the RTN |
|
|
What are some treatments for congential central hypoventilation syndrome? |
Patients with CCHS do not respond to pharmacological ventilatory stimulants Mechanical ventilation is required to ensure adequate ventilation, at least during sleep Bi-level positive airway pressure ventilation (BiPAP) Continuous negative extrathoracic pressure ventilation (CNEP) Diaphragm pacing During the first years of life, positive pressure ventialtion (PPV) via a tracheostomy is generally used |
|
|
How does a mutation of the Phox2B mutation effect breathing? |
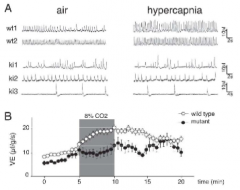
De novo mutations of transcription factor homeobox 2B (Phox2B) Phox2B is required for development of several neuron types in the central and peripheral nervous system Genetic elimination of the RTN severely abolishes CO2 sensitivity in constitutive and condition Phox2B mice |
|
|
The Phox2B gene is required for what? |
Several neuron types in the central and peripheral nervous system |
|
|
What does a pCO2 of 48.7 mmHg indicate? |
Hypercapnia |
|
|
What does a pCO2 of 43.7mmHg indicate? |
Normocapnia |
|
|
What does a pCO2 of 35.8mmHg indicate? |
Hypocania |
|
|
What are some central oxygen chemoreceptors? |
Locus coeruleus Thalamus preBotzinger Complex |
|
|
What are carotid bodies? |
Carotid bodies contain glomus cells Detect low oxygen (mainly), high CO2 and low pH Highest blood flow of all tissues in the body Afferent nerve fibers form the carotid sinus nerve (CSN) before entering the glossopharyngial nerve |
|
|
What do carotid bodies detect? |
Low oxygen (mainly) High CO2 Low pH |
|
|
What are the three types of carotid body tumors? |
Familial Sporadic Hyperplastic |
|
|
What does low pO2 in blood do to ventilation and how does it do that? |

O2 regulation by peripheral chemorecetpors to increase O2 1) Low pO2 detected in blood vessel and glomus cell in carotid body 2) K+ channels close 3) Cells depolarizes 4) Votlaged gated Ca2+ channels open 5) Ca2+ entry 6) Exocytosis of dopamine-containing vesicles where released dopamine binds to dopamine receptors in sensory neuron 7) An action potential signal sent to medullary centers to increase ventiatlion |
|
|
How does hypoxia mediates carbon dioxide chemosensitivity? A) Hypoxia decreases the slope of the carbon dioxide chemosensitvity B) Hypoxia increases the slope of the carbon dioxide chemoseitivity C) Hypoxia is shifting the metabolic hyperbola to the right D) Hypoxia shifts the carbon dioxide chemosentivity to the right E) B and D |
B)
|
|
|
Which of these statement is (are) correct about central chemoreceptors? A) Central chemoreceptors are located closed to capillaries B) The Botzinger Complex contains important central chemoreceptors C) The retrotrapezoid nucleus (RTN) detects changes in carbon dioxide and oxygen D) Neurons of the medullary raphe are serotoninergic E) A and D |
E) |
|
|
Who is Jean-Charles Leggallois? |
1813, french physiologist Noticed after decapitation, the convict's mouth was still showing breathing movements |
|
|
What cranial nerves does the phrenic nerve consist of? |
C3, C4 and C5 |
|
|
What nerve innervates the diaphragm muscle? |
Phrenic nerve |
|
|
What nerve innervates the upper airways muscles? |
Hypoglossal nerve |
|
|
What nerve innervates the scalenes? |
Cervical nerve |
|
|
What nerve innervates the abdominal muscle? |
Thoracic spinal nerve |
|
|
What is the nucleus tractus solitarius (NTS)? |
Receives input from carotid bodies Can increase respiratory rate |
|
|
What is sudden unexplained death in epilepsy (SUDEP)? |
Sudden, unexpected, non-traumatic and non-drowning death of patients with epilepsy Can be an uncontrolled epilepsy SUDEP commonly occurs during or after a seuizure during the night |
|
|
What is the preBotzinger Complex (preBotC)? |
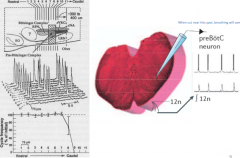
A unique site generating respiratory rhythm where when cut near this spot will cause breathing to completely stop
These inspiratory cells can produce pacemaker potentials PreBotC neurons selectively express receptors for substance P (via NK1R receptors) and opioids (via uOR receptors), whereas other cells in the ventral respiratory group (VRG) does not Activation of the NK1R and uOR receptors (via substance P and opiods) on PreBotC neurons changes respiratory frequency |
|
|
Can preBotC produce pacemaker potentials? |
Yes |
|
|
What happens if you cut the preBotC? |
Breathing completely stops |
|
|
What happens if you destroy the preBotzinger complex neurons in conscious animals? |

Can destroy these neurons by using the saporin method The results with injections of saporin tagged to the NK1R antibody into the PreBotC destroys neurons that express this receptor Normal breathing pattern is affected by saporin injections into the PreBotC (breathing is still occurring, but it is NOT normal) |
|
|
What is saporin? |
Ribosomaltoxin that interferes with the synthesis of new proteins (this toxin willselectively target and kill NK1R containing cells) |
|
|
What happens when substance P binds to an NK1R receptors?
|
An increase in firing rate of the inspiratory preBotC neurons (i.e. increasing breathing frequency) |
|
|
What happens when opioids bind to uOR receptors? |
Decrease firing rate of preBotC Decrease breathing frequency |
|
|
What happens when you add an antagonist for opioids to the preBotC? |
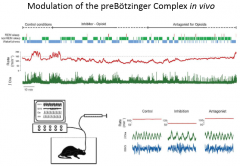
Firing rate in preBotC increases Breathing freuqency starts to increase |
|
|
Is respiratory depression by opioid analgesics lethal? |
Yes |
|
|
What are the symptoms of respiratory depression by opioid analgesics? |
Hypoventilation or cessation of breathing (low rate and tidal volume) Increased sleep-disordered breathing (obstructive or central sleep apneas) Cardiac arrhythmia and low blood pressure |
|
|
What is the cause of respiratory depression by opioid analgesics? |
Inhibition of respiratory centers by opioid analgesics |
|
|
What is a treatment for respiratory depression by opioid analgesics? |
Naloxone |
|
|
What is naloxone? |
A micro-opioid receptor antagonist |
|
|
What are some things that can be used as preventions against respiratory depression by opioid analgesics? |
Ampakine (modulator of AMPA receptor) Serotonin (5-HT_2A receptor antagonist) |
|
|
What is Rett's syndrome? |
A neurodevelopmental disorder of the grey matter of the brain that almost exclusively affects females |
|
|
What are the symptoms of Rett's syndrome? |
Loss of purposeful use of hands, distinctive hand movements, slowed brain and head growth Problems with walking, seizures and intellectual disability Breathing difficulties while awake such as hyperventilation, apnea (breath holding) and air swallowing |
|
|
What is the cause of Rett's syndrome? |
Mutation in the methyl CpG binding protein 2 (MECP2) |
|
|
Where is MECP2 expressed? |
In the preBotzinger complex |
|
|
Of the respiratory rhythm generation models, what is the pacemaker hypothesis? |

Rhythm is produced by intrinsic pacemaker properties (pacemaker currents) of a population of cells Ionic currents have the property to promote spontaneous bursting of neurons which leads to pacemaker currents Membrane potential (Vm) is increasing due to the hyperpolarization-activated cation current (Ih) and the presistent sodium current (INaP) |
|
|
Of the respiratory rhythm generation models, what is the network hypothesis? |

Rhythm is produced by interaction of neurons in network with reciprocal/negative feedback |
|
|
What do irritant receptors cause in regulation of breathing? |
It creates coughing |
|
|
How does the diaphragm change from being awake to REM? |

Diaphragm does not change much but rather the change in the activityof the upper airway muscles |
|
|
If the total lung ventilation decreases from being awake to being in REM, how does that change the tidal volume and frequency? |
The product of the tidal volume and frequency decreases |
|
|
What is unique about lungfishes respiratory system? |

They have a dual respiratory system: Lungs to breath air when there is no water Gills for aquatic breathing |
|
|
What is fetal breathing? |

Before birth, foetal breathing can be observed and is characterized by rhythmic contractions of respiratory muscles including diaphragm and airway muscles Two separate neural structures generate rhythm before and after birth: parafacial respiratory group (red) and preBotzinger Complex (yellow/green) Necessary to form respiratory network Maintains lung liquid volume and hence lung expansion Use different (ancestral neuronal circuits) |
|
|
What has greater affinity for O2, fetal or maternal Hb and why? |
Fetal Hb Because when you have blood from mother, this oxygen needs to gointo fetal circulation but if fetal Hb is higher, it will steal all of the O2 from mother |
|
|
How is there respiratory transition to extra-uterine life? |
Fluid in the fetus lung are removed when thorax is squeezed during vaginal delivery. Also absorbed by pulmonary capillaries Infant born by caesarean section do not benefit from chest compression and may experience retention of fetal lung fluid known as transient tachypnea of the new born (clinicians need to remove fluid from newborn lungs manually) In first breaths, newborn must generate as high as ~70mmHg During parturition and when the umbilical cord is cut at birth, the neonate may become profoundly hypoexemic, hypercapnic and acidemic (this may stimulate the respiratory network to start generate breathing) Removal of circulating inhibitory or suppressive substances that originate in the placenta may contribute to onset of continuous breathing |
|
|
What happens to a newborn's lungs if born by c-section? |
Transient tachypnea of the newborn No chest compression and may experience retention of fetal lung fluid May need clinicians to remove fluid from newborn lungs manually |
|
|
What is apnea of prematurity? |
Occurs 85% of premature (<34 week) babies Due to immaturity of brainstem Apparition of apneas (cessation of breathing) |
|
|
What is a treatment of apnea of prematurity? |
Caffeine |
|
|
What is idiopathic apnea of prematurity? |
Cessation of respiratory airflow |
|
|
What happens to breathing during exercise? |
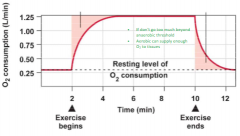
Oxygen consumption increases during exercise to provide more oxygen to the muscles Tremendous increase in O2 demand as exercising muscle O2 consumption can increase Because the O2 consumption is increasing, will provide energy for exercising muscles O2 needed for ATP synthesis In terms of cardiorespiratory system, must respond by delivering more O2 to the right place, the tissues that are exercising Helps if can divert blood away where there is no movement going on so that you are delivering O2 to exercising tissues |
|
|
What happens to ventilation of breathing during exercise? |
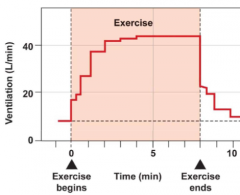
Ventilation rate increases as soon as exercise happens (very fast response) Drops down after exercise Ventilation matched to the O2 demand that is incurred with exercise This is due to the same feed-forward effects, the feedforward slide applies to BOTH CARDIOVASCULAR AND RESPIRATORY |
|
|
What is VO2 max? |
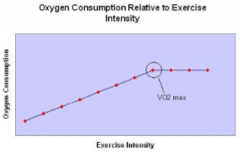
Highest rate of oxygen consumption attainable during maximal or exhaustive exercise |
|
|
What do you require when measuring VO2 max? |
Maximal effort while measuring breathing and oxygen levels using open-circuit spirometry |
|
|
What is erythropoietin (EPO)? |
Glycoprotein hormone that controls red blood cell production |
|
|
What does training in altitude or hypobaric chamber do to the body? |
Increase red blood cell production and muscle metabolism |
|
|
What does blood doping or blood transfusion do to the body? |
Increase number of red blood cells |
|
|
What causes abrupt increase in ventilation? |
Psychic stimuli (anticipation of exercise) Simultaneous cortical motor activation of the skeletal muscles and the respiratory centers Excitatory impulses from proprioceptors in moving muscles, tendons and joints to the respiratory centers |
|
|
How can being at high altitude affect the human body? |
Psychomotor impairment detectable with FFT/pegboard Complex reaction time slows AMS and HACE possible |
|
|
What is commercial aircraft pressurized to an altitude equivalent of? |
150--2500m |
|
|
How can being at very high altitude affect the human body? |
Learning and spacial memory impaired |
|
|
How can being at extreme altitude affect the human body? |
32% of climbers have hallucinations above 7500m MRI changes, including white matter hyperintensities and cortical atrophy above 7000m Memory retrieval impaired |
|
|
What are the respiratory responses in high altitude in aspects of pH, PO2, PCO2, and ventilation? |
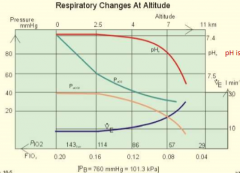
pH increases pO2 decreases in pressure pCO2 decreases in pressure Ventilation increases |
|
|
When ventilation is increased, what happens to CO2 and pH? |
CO2 gets washed out of the body pH goes up |
|
|
What is chronic hypoxia at high altitude? |
Hypoxia increases ventilation Increased ventiliation decreases pCO2 Hypoxia increases CO2 chemosensitivity |
|
|
What chronic changes happen if you speed weeks at high altitude? |
Release of erythropoietin that stimulates red blood cell production Increase of hematocrit by 50% Synthesis of 2,3-DPG in red blood cells Muscle size decreases after 4-6 weeks (loss of appetite) |
|
|
What chronic changes happen if you speed years at high altitude? |
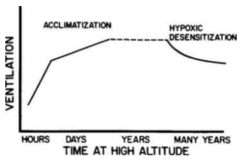
Hypoxic desensitization |
|
|
What is 2,3-DPG? |
2,3-diphosphoglycerate Made by red blood cells during chronic hypoxia An intermediate of glycolysis pathway Increased 2,3-DPG decreases the affinity for Hb for O2 2,3-DPG degrades when blood is stored |
|
|
What happens at very high altitude to respiratory? |
Hyperventilation is very high
pCO2 is very low pH is very high Oxygenation-Hb dissociation is shifted to the left |
|
|
What happens to O2 and CO2 when you hyperventilate? |
As you're hyperventilating, you're attempting to get more O in body
CO2 will get expelled into the air from the lungs, as a result, the equilibrium (Henderson Hasselbach equation) will shift to the left, raising the pH making the blood more alkaline so the O2 dissociation curve will shift from normal place to the left O2 dissociation curve will shift to the left That means there will be tendency for hemoglobin to hang onto O2 when want more O2 delivered to tissue The problem is compensated by the fact that the tissues will have lower than normal O2 levels Tissue O2 will be down around 20mmHg, this can compensate for the shift to the left on the O2 dissociation curve Will have phenomenon happening as you are hyperventilating t |