Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
104 Cards in this Set
- Front
- Back
|
What lipoproteins are found on cholesterol?
|
Apolipoprotein C, B100, E
|
|
|
What are the four major classes of cholesterol?
|
HDL, LDL, VLDL, Chylomicrons
size increases ----------------------------> density decreases ----------------------> cholesterol decreases -----------------> tag increases -----------------------------> |
|
|
What do apoplipoproteins do?
|
Provide structural stability and engage in biological functions (receptor recognition)
|
|
|
What do chylomicrons do?
|
transport exogenous trigylcerides from intestine to muscle and fat tissue
|
|
|
Where are chylomicrons taken up?
|
taken up in liver and secreted in bile
|
|
|
What are the possible fates of chylomicrons?
|
oxidation in the liver to bile acids or converted into VLDLs
|
|
|
What do VLDLs do?
|
transport endogenous triglycerides from liver to fat tissue
|
|
|
What is the fate of VLDL?
|
hydrolyzed by lipoprotein lipase to yield IDL then LDL
|
|
|
What do LDLs do?
|
transport cholesterol from liver to peripheral tissue
|
|
|
How are LDLs removed from circulation?
|
Taken up via LDL receptors that recognize apoB 100
|
|
|
What does HDL do?
|
transports cholesterol from tissues back to liver
|
|
|
How is cholesterol removed from the body?
|
billary excretion
|
|
|
What is the half-life of LDL?
|
2-4 days
|
|
|
What is a major risk factor of atheroscleorsis?
|
elevated LDL
|
|
|
How does LDL lead to athersclerosis?
|
LDL not taken up by LDL receptors is oxidized --> engulfed by macrophages --> become foam cells --> apoptosis and necrosis --> release of free radicals and proteolytic enzymes --> LOCAL INFLAMMATORY RESPONSE
|
|
|
What are CVD risk factors?
|
increased LDL
decreased HDL increased triglycerides smoking HTN type 2 DM age family hx |
|
|
What is the normal value of LDL
|
< 130mg/dl
|
|
|
what is the normal value of HDL?
|
35 mg/dl
|
|
|
what is the normal value of triglycerides?
|
150 mg/dl
|
|
|
What are the 4 types of dyslipidemia?
|
hypercholesterolemia
hypertriglyceridemia mixed hyperlipidemia disorders of HDL metabolism |
|
|
What is hypercholesterolemia?
|
increased total plasma cholesterol (TPC)
increased LDL normal triglyceride |
|
|
What is the major cause of hypercholesterolemia?
|
polygenic - no defined genetic cause
|
|
|
What is the genetic cause of hypercholesterolemia?
|
Familial (FH) - auto dominant involves defects/absences in LDL receptor
|
|
|
What clinical features distinguish a heterozygot from a homozygote of FH Type IIa?
|
heterozygote - tendon xanthomias, arcus cornea, TPC 275-500
homozygote - TPC >700, absence of LDL receptors, CDV @ < 20yrs |
|
|
What is familial defective apoB100?
|
auto dominant disease in which mutations decreases affinity of LDL particles for LDL-R
|
|
|
What is hypertriglycerideemia?
|
increased plasma triglyceride concentrations - 200-500 mg/dl
|
|
|
What is familial hypertriglyceridemia?
|
auto dominant, unknown genetics, common
|
|
|
What is familial lipoprotein lipase deficiency?
|
hypertriglyceridemia
absence of LPL auto dominant profound hypertriglyceridemia infants with pancreatitis, eruptive xanthomas, hepato-splenomegaly |
|
|
What is apoCII deficiency?
|
hypertriglyceridemia
rare autosomal disorder |
|
|
What is mixed hyperlipidemia?
|
increased total plasma cholesterol
increased LDL increased triglyceride decreased HDL |
|
|
What is familial combined hyperlipidemia?
|
mixed hyperlipidemia
common, moderately elevated of triglycerides and TPC but reduced HDL patients present with features of metabolic syndrome |
|
|
What is dysbetalipoproteinemia?
|
mixed hyperlipidemia
increased chylomicrons and VLDL remnants - hypertriglycerideemia and hypercholesterolemia males - symptoms at 30 females - symptoms at menopause |
|
|
What are some causes of decreased HDL metabolism?
|
rare genetic defects in:
apopA1, ABCA1, LCAT |
|
|
What physiological state leads to hypertriglyceridemia?
|
pregnancy
|
|
|
What should be done first to correct cholesterol levels in patients?
|
therapeutic lifestyle changes
can reduce TPC by 5-25% |
|
|
What are the anithyperlipidemic drugs?
|
HMG CoA reductase inhibitors (statins)
Niacin (vitamin B3, nicotinic acid) Fibrates Bile-acid binding agents Cholesterol absortption inhibitors Combination drug therapy |
|
|
When are HMG-CoA reductase inhibitors (statins) used?
|
First line and most effective treatment for elevated LDL
|
|
|
What are the statins?
|
lovastatin
pravastatin simvastatin fluvastatin atorvastatin rosuvastatin |
|
|
What is the MOA of statins?
|
inhibit activity of HMG CoA reductase
|
|
|
What are statins
|
analogues of HMG
|
|
|
What is the relative potency of the statins?
|
RAS LPF
rosuvastatin > atorvastatin > simvastatin > lovastatin > pravastatin > fluvastatin |
|
|
Which statins inhibit cytochrome P450 3A4?
|
LSA
lovastatin, simvastatin,, atorvastatin |
|
|
How is fluvastain metabolized?
|
by alternate CYP450 pathways
|
|
|
Which statins are not metabolized by CYP450s?
|
pravastatin and rosuvastatin
|
|
|
How do statins decrease TPC levels?
|
Inhibit production of cholesterol and increase LDL receptor expression
|
|
|
When is a case of hypercholesterolemia non responsive to statins?
|
in homozygotes of famial hypercholesterolemia - that lack LDL receptors
|
|
|
What are the adverse effects of statins?
|
myopathy and or myositis with rhabdomyosis
can get increases in serum transaminases + liver enzymes |
|
|
when is statin use cautioned?
|
in patients with liver disease?
|
|
|
What can statins be combined with?
|
1. bile acid binding agent or cholesterol absorption inhibitor - additive effects
2. with Niacin - increased risk of myopathy 3. with fibrates - increase risk of rhabdomyolysis |
|
|
Drug interactions to be aware of when taking statins?
|
Drugs metabolized by CTP450
|
|
|
What are the CI of statins?
|
Pregnancy
breastfeeding active liver disease |
|
|
When are inhibitors of bile acid reabsorption used?
|
Second line treatment for lipid reduction
|
|
|
What are the bile acid reabsorption inhibitors?
|
cholestyramine
colesevelam colestipol |
|
|
What is the MOA of inhibitors of bile acid production?
|
cationic polymer resins that bind to negatively charged bile acids in small intestine - prevents reabsoprtion
|
|
|
What is the effect of decreased bile acid reabsorption?
|
decreased bile acid reabsorption --> increased conversion of cholesterol to bile acids
LDL receptor expression increased --> increased removal of LDLs from circulation |
|
|
What are the pharmokinetics of inhibitors of bile acid reabsorption?
|
taken orally, water insoluble
uncomfortable to ingest - suspend in OJ excreted totally in feces |
|
|
Why do inhibitors of bile acid lower TPC levels?
|
because 90% of bile acid is reabsorbed
|
|
|
When should inhibitors of bile acid reabsorption be used?
|
They are the DOC for type IIa (familial hypercholesterolemia) and type IIIb (familial combined hyperlipidemia)
|
|
|
Why use cholestyramine?
|
releives pruritis caused by accumulation of bile acids in patients with billiary obstruction
|
|
|
What are the adverse effects of inhibitors of bile acid reabsorption?
|
constipation, nausea, bloating, flatulance
|
|
|
Which inhibitor of bile acid reabsorption has few side effects?
|
colesevelam
|
|
|
What are the drug combinations that can be used with inhibitors of bile acid synthesis?
|
combine with statins or niacin to reduce LDL
|
|
|
what are the drug interactions of inhibitors of bile acid synthesis?
|
decreased absorption of fat soluble vitamins
decreased absorption of Digoxin, Warfarin |
|
|
When are inhibitors of bile acid reabsorption CI?
|
hypertriglyceridemia - they can upregulate VLDL and triglyceride synthesis
|
|
|
Why use Niacin?
|
is the most effect agent for increasing HDL
also reduces VLDL, LDL, and triglyceride plasma levels |
|
|
What is Niacin?
|
nicotinic acid or vitamin B3
|
|
|
What is the MOA of Niacin?
|
at gram doses inhibits lipolysis in adipose tissue
|
|
|
What is the effect of Niacin?
|
leads to a decrease in lipolysis --> less substrates available for VLDL --> less substrate for LDL synthesis
|
|
|
What are the pharmokinetics of Niacin?
|
taken orally
converted to nicotinamide --> incorporated into NAD |
|
|
How is Niacin excreted?
|
niacin and its metabolites are excreted in urine
|
|
|
When is Niacin used?
|
when statins are CI
tx of familial hyperlipidemias in combo with other agents to treat severe hypercholesterolemia most potent increaser of HDL |
|
|
what are the adverse effects of Niacin?
|
1. cutaneous flush, pruritis - prevented with NSAIDs - occurs during first few weeks
2. hyperuricemia 3. hepatotoxicity 4. impaired insulin sensitivity 5. w/ statin increase risk of myopathy |
|
|
what drug interactions should one be aware of with Niacin use?
|
use with statins can increase risk of myopathies
|
|
|
When is Niacin use cautioned?
|
in diabetics
|
|
|
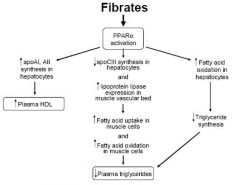
What do fibrates do?
|
reduce VLDL and TGs and increase HDL
|
|
|
what are the fibrates?
|
fenofibrate and gemfibrozil
|
|
|
What is the MOA of the fibrates?
|
bind to and activated perioxisome proliferator-activated receptor a (PPARa)
|
|
|
where is perioxisome proliferator-activated receptor a found?
|
hepatocytes, skeletal muscle, macrophages, heart
|
|
|
what is the effect of fibrates on cholesterol?
|
changes in lipid metabolism lead to decreased TGs and increased HDL
|
|
|
How are fibrates excreted?
|
in urine as glucuronide conjugates
|
|
|
What is the PK of fibrates?
|
completely absorbed after oral dose
widely distributed |
|
|
What is the MOA of fibrates?
|
|
|
|
When are Fibrates used?
|
for the treatment of hypertriglyceridemias
patients who do not respond to diet or other drugs |
|
|
when are fibrates the DOC?
|
for dysbetalipoproteinemia
|
|
|
What are the adverse effects of Fibrates?
|
mild GI effects
cholelithiasis myositis - patients w/ renal insufficiency |
|
|
When should fibrate used be cautioned?
|
in patients with renal insufficieny - could get myositis
|
|
|
What drug interactions exist with fibrate use?
|
competes w/ coumadin for plasma binding sites and potentiates anticoagulant activity
|
|
|
when are fibrates CI?
|
Pregnancy - safety not established
|
|
|
What do cholesterol absorption inhibitors do?
|
reduce LDL
(small decrease in triglycerides and small increase in HDL) |
|
|
What are the cholesterol absorption inhibitors
|
ezetimibe, plant sterols
|
|
|
What is the MOA of cholesterol absorption inhibitors
|
inhibit intestinal absorption of dietary + billiary cholesterol
reduce LDL cholesterol by inhibiting hepatic production of VLDL |
|
|
What is the effect of reduced hepatic cholesterol?
|
reduced hepatic cholesterol --> up-regulation of LDL receptor
|
|
|
What are the PK of cholesterol absorption inhibitors?
|
primarily metabolized in small intestine and liver
|
|
|
How are cholesterol absorption inhibitors excreted?
|
biliary and renal excretion
|
|
|
When to use cholesterol absorption inhibitors?
|
complimentary to statins so used in combination when response to statin is inadequate
hypercholesterolemia when statins CI |
|
|
what are the adverse effects cholesterol absorption inhibitors?
|
diarrhea, abdominal pain, headache
rash and angio-edema (rare) |
|
|
when are inhibitors of cholesterol absorption CI?
|
breastfeeding
|
|
|
What do omega-3 fatty acids do?
|
decrease triglycerides
|
|
|
what are the omega-3 fatty acids?
|
EPA and DHA
|
|
|
What is the MOA of omega-3 fatty acids?
|
reduce triglyceride biosynthesis and increase fatty acid oxidation
|
|
|
when are omega-3 fatty acids used as treatment?
|
when triglycerides > 500mg/dl
|
|
|
when is a single drug not enough?
|
patients w/ combined hypertriglyceriedemia and hypercholesterolemia
patients w/ high LDL and low HDL |
|
|
What are some combinations for reducing dyslipidemia?
|
-ezetimibe + statin - further reduce LDL 15-20%
-statins + resin -fibrate + statin - use less statin |
|
|
What is the rule of 6?
|
if statin dose is doubled, there is only a 6% decrease in LDL
but if combined it can be decreased by 12-15% |