Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
12 Cards in this Set
- Front
- Back
|
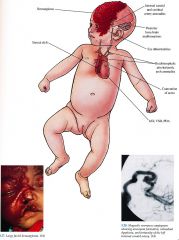
Clinical PHACES
|
|
|
|
Synonym
|
Posterior fossa brain malformation
Hemangioma, large facial Arterial anomalies Cardiac anomalies and Coarctation of the aorta Eye abnormalities Sternal clefting and/or supraumbilical raphe |
|
|
Inheritance
|
Sporadic; x linked dominant transmission with male lethality proposed given large predominance of female cases
|
|
|
Prenatal
|
First trimester ultrasound may pick up early intracranial structural defects
|
|
|
Incidence
|
Rare may be underreported because of misdiagnosis as vascular malformation/Sturge Weber syndrome; F > M
|
|
|
Age at Presentation
|
Birth to first few weeks of life
|
|
|
Clinical
|
Skin
Large, facial, plaque like hemangioma in a V1 distribution alone or in combination with V2 and V3; unilateral left sided most common, can be bilateral, more exten¬sive lesions have greater CNS vascular/structural involvement; ulceration common Sternal cleft/pits, supraumbilical raphe Central Nervous System Posterior fossa malformations including Dandy Walker malformation (most com¬mon), hypoplasia/agenesis of the cerebellum, cerebellar vermis, corpus callosum; anomalous branches/aneurysmal dilatation of the internal carotid arteries and cere¬bral arteries with occlusion/stenosis/cerebral infarct; secondary seizures, develop¬mental delay, contralateral herniparesis, headache Cardiac/Aorta Coarctation of the aorta (most common), anomalies of the brachiocephalic arteries and aortic arch, patent cluctus arteriosus, ventral septal defects, atrial septal defects. cor triatriaturn, tricuspid and aortic atresia Eye lpsilateral microphthalmos, optic atrophy, optic nerve hypoplasia, cataracts, in¬creased retinal vascularity, strabismus, exophthalmos |
|
|
D/Dx
|
Sturge Weber syndrome (p. 100) Segmental hemangioma without extracutaneous findings Tufted angioma Kaposiform hemangioenclothelioma
|
|
|
Lab
|
Cranial ultrasound, MRI, MRA Aortagraphy, echocardiogram
|
|
|
Management
|
Close follow up with pediatric dermatologist, neurologist, cardiologist, and ophthalmologist
|
|
|
Prognosis
|
May have shortened life span depending on severity of extracutaneous findings
|
|
|
Pathogenesis
|
Unknown; may be secondary to a developmental error at 6 to 8 weeks' gestation caused by defects in morphoregulatory genes
|