![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
276 Cards in this Set
- Front
- Back
|
We went over several side effects of topical steroid therapy. Name some examples? Which is the most common? |
1. Atrophy (most common) 2. Striae (rubra distaensae) 3. Steroid Rosacea 4. Steroid Acne 5. Perioral Dermatitis 6. Hypopigmentation 7. Aggravation of cutaneous infections (tinea incognito, herpes sinplex, molluscum, scabies) 8. Glaucoma and cataracts |
|
|
What are the two intracellular nuclear receptors for Retinoids? |
RAR, RXR (each has 3 isoforms) |
|
|
What is the most common retinoid dimer receptor in the epidermis? |
RARgamma/RXRalpha |
|
|
What are the characteristics of the three generations of retinoids? What retinoids are included in each generation? |
First Generation (non aromatic): tRETINOIN, iroTRETINOIN, aliTRETINOIN
Second Generation ( monoaromatic): acitretin, eretinate
Third Generation (polyaromatic): tazarotENE, adapalene, bexarotene (ENE= three letters, third generation) |
|
|
What's the deal with acitretin and etretinate? |
Etretinate is a lipophilic second generation retinoid that was discontinued in 1998 because of a narrow therapeutic index and a long half life. |
|
|
Three clinical stages of eczema and their features? |
1. Acute- vesicles, blisters, intesne redness
2. Subacute- redness, scaling, fissuring, parched/scalded appearance
3. Chronic- thickened skin, lichenification, excoriation, fissuring |
|
|
BASIC treatment regimens for each stage of eczema. |
1. Acute- wet compresses, oral corticosteroids, antihistamines
2. Subacute- discontinue wet compresses, topical corticosteroids, calcineurin inhibitors, bleach baths
3. Chronic- topical steroids, phototherapy |
|
|
What is pompholyx? |
aka dishydrosis: symmetric vesicular hand/foot dermatits, moderate to severe pruritis followed by vesicles
|
|
|
buzzword 'crazy paving' |
asteatotic eczema
|
|
|
Lichen Simplex Chronicus? |
habitual scratching of a localized area, pleasure in the relief that comes form scratching
(nuchae) |
|
|
Where is chloracne most common? |
face, postauricular surfaces, genitals
|
|
|
What is the triple response of Lewis? |
1. Vasodilation 2. Axon reflex (nerve stimulation --> pruritis) 3. Vascular permeability |
|
|
Urticaria vs. Angioedema? |
Urticaria- whealing of the skin in the superficial dermis, comes and goes within 24 hours
Angioedema- swelling that occus deeper in dermis and subcutis or mucosal tissue, lasts 2-3 days |
|
|
Newly formed vs preformed mediators of urticaria? |
Newly formed are all super long words: prostaglandins D2, leukotrienes C4/D4, platelet activating factor
Preformed are all simple: histamine, heparin, tryptase, chymase |
|
|
What is the mechanism of a Type I hypersensitivity reaction? |
Cross linking high affinity IgE receptors (Fcε)-- > this results in increased cysteinyl leukotrienes |
|
|
Examples of drugs that are direct mast cell degranulators? |
PIANO Polymyxin, IV contrast, ASA, NSAIDS, Opioids |
|
|
SSX of Urticarial Vasculitis? What workup is warranted? |
VAsculitis that produces initial lesions that look like urticaria but last more than 24 hours, burn, heal with purpura, scaling and hyperpigmentation
Labs: complement levels, CBC, ESR, BUN, ANA, cryoglobulins, PFT |
|
|
What are the two types of hereditary angioedema? |
Type I: not enough C1-INH produced (85%)
Type II: Normal amount of C1-INH, but dysfunctional
You tell these two apart with labs by looking at the C1-INH quant... duh |
|
|
What are the two types of acquired angioedema? |
Type I: malignancy causes increased catabolism of C1-INH (lymphoproliferative, breast ca)
Type II: autoimmune |
|
|
Why would we prescribe danazol for prophylaxis in acquired angioedema? |
androgens increase liver production of C1-INH
**note- estrogens can precipitate an attack** |
|
|
Whats the difference between a polymorphous light eruption (PMLE) and solar uritcaria? |
Solar Urticaria develops within minutes of UV, goes away in less than an hour
PMLE lesions usually aren't urticarial, takes longer to develop (hours) and stays longer (days) |
|
|
Two types of Urticarial Vasculitis? |
LOOK AT DIFFERENT IN COMPLEMENT LEVELS!
Normocomplement: can be idiopathic, monoclonal gammopathy, neoplasm, cold exposure, UV light sensitivity |
|
|
What are the 4 main factors in the pathogenesis of acne? |
1. alteration in the keratinization process 2. sebum production 3. p. acnes follicular colonization 4. release of inflammatory mediators |
|
|
What is the first step in the production of acne? Where does this occur? |
formation of microcomedo in the infundibulum |
|
|
Micro of P.acnes? What porphyrin does it produce?
|
gram positive rod, anaerobic, produced Copropophyrin III (P. acnEE produces cp thrEE) |
|
|
Which pattern recognition receptor is actived by P acnes? |
TLR 2 |
|
|
Where are androgen receptors found in the pilosebaceous subunit? |
basal layer of the sebaceous gland |
|
|
Increased levels of what hormon in prepubescent children is associated with increased sebum production and acne? |
dehydroepiandrosterone sulfate (DHEAS) |
|
|
Go to page 220-221, read through the basic acne treatment algorithm and drug MOA |
Read it? YOU GO GIRL/GUY! |
|
|
Most topical and oral treatments for acne are category B-C (1 or 2 D's in there). Which ones are category X? |
Topical- tazarotene |
|
|
All retinoids are photolabile except which one? |
ADAPALENE |
|
|
When patients start isotretinoin, we recommend that they d/c all using all other products and pills, especially minocycline... why? |
pseudotumor cerebri |
|
|
Name that tooth stain! Stains gingival portion? Stains incisal portion? |
Tetracycline stains the Top, Minocycline stains the bottom (minnows on the bottom of the lake) |
|
|
What antiobiotics will affect OCPs? |
rifampin, griseofulvin |
|
|
Side effects of spironolactone that you want to warn/council your patient on so you don't get a T con? |
VTE, elevated K, menstrual irregularities, breast tenderness, decreased libido, feminization of the male fetus (category D), headache |
|
|
Follow up questions for your patient who has been on Isotretinoin x 1 month? |
Pregnancy? (teratogen, mc craniofacial, cardiac, cns- get HCG) GI upset/blood in stool? (IBD) Dryness? Headaches? Vision changes? (pseudotumor) Uncontrolled bleeding? (CBC, check platelets) Psych issues
** also get a lipid panel to check TG, LFTs
|
|
|
Goal dose of Isotretinoin? |
120-150mg/kg total |
|
|
How do we differentiate between acne fulminans and acne conglobata? |
Acne fulminans is an abrupt onset acne with painful, oozing, friable plaques with hemorrhagic crusts and systemic symptoms (fever, weight loss, arthralgia, myalgia, HSM)
Acne conglobata is really bad acne too, without any systemic symptoms |
|
|
Where are the osteolytic bone lesions in acne fulminans? |
clavicle and sternum |
|
|
What neutrophilic dermatosis can be ssociated with acne fulminans? |
SAPHO (synovisis, acne, pustulosis, hyperostosis, osteitis |
|
|
Which lab abnormalities are seen in acne fulminans? |
elevated ESR, proteinuria, leukocytosis, anemia |
|
|
Pregnant woman comes in for her acne. What can you give her? |
azeaic acid, clindamycin, erythromycin, azithromycin, blue light, chemical peels |
|
|
What is the follicular occlusion tetrad? |
dissecting cellulitis of the scalp, hidradenitis suppuritiva, pilonidal disease, acne conglobata |
|
|
What is PAPA syndrome? What gene mutation is implicated? |
Pyogenic arthritis, pyoderma gangrenosum (my favorite disease!), acne (conglobata)
PSTPIP1 aka CD2 antigen binding protein 1 (they said don't know this part... but it doesn't hurt to see it!) |
|
|
ADSM comes in with acne localized under where his chin strap would go... |
Acne Mechanica |
|
|
Patient comes in with acne that he states started after he began to roid rage... how can we know clinically if this is drug induced acne? |
Drug induced acne is monomorphous as oppsed to heterogenous
**steroids, phenytoin, lithium, isoniazid, iodides, bromides can also cause drug induced acne |
|
|
Whats the difference between neonatal acne and infantile acne? |
Neonatal acne- 2 weeks to 3 months of life, no treatemnt necessary, d/t malassezia and sebum production
Infantile acne- 3 to 6 months, more comedone formation, treat with topical tretinoin, benzoyl peroxide, oral isotretinoin |
|
|
What is Fabre-Racouchot? |
Nodular elastosis with cysts and comedones
OLD PEOPLE |
|
|
What are the four rosacea subtypes? Which is most common? |
Erythematotelangiectatic (most common) Papulopustular Glandular Ocular |
|
|
Cardinal features of rosacea? |
erythema, edema, papules, pustules, telangectasias, NO COMEDONES |
|
|
Treatments for rosacea |
Orals: cyclines, isotretinoin (anti inflammatory effects), **Oracea is QD doxy
Topicals: Metrogel, sulfacetamide, azelaic acid, clinda, retinoids |
|
|
rosacea pathogenesis, which organism? |
demodex mite common in follicle |
|
|
Ocular rosacea... MMP-9 is elevated in patient's eye fluid... doxycycline decreases MMP-9... |
not sure how important this is, but ocular rosacea has an up to 50% associated in opthalmological literature and is underappreciated by derms... |
|
|
Histologically, what is parakeratosis? |
Retention of pyknotic keratinocyte nuclei within stratum corneum (it's moving too fast!) |
|

What comorbidity do you need to ask? |
This is pustular psoriasis of the sole (also seen in palms)... ask about smoking history (95% of people with this are smokers) and bone pain (association with bone lesions) |
|
|
Psoriasis of the penis is called... |
Balantitis circinata (highly characteristic psoriasiform lesion occuring in reiters syndrome)
|
|
|
Psoriatic arthritis affects what percent of patients with Psoriasis? What does this arthritis typically look like? |
5-30%, most common is oligoarticular, asymmetric arthritis (keep in mind that you can have all different kinds per the Moll and Wright classification) |
|
|
Which drugs can exacerbate psoriasis? |
LABS LABS LABS LABS LABS!
Lithium Antimalarials Beta Blockers Systemic Steroids
(terbinifine and interferon can, too) |
|
|
What types of treatments can we pursue for psoriasis? How do we dictate treatment? |
Less than 20% BSA --> topical steroids are first line, then tazorac, tar, anthralin, ILK
More than 20% BSA or any arthritis --> NBUVB, PUVA, methotrexate, biologics, cyclosporine, soriatane (acitretin!!! remember this drug and pregnant people?)
So there were about 489309038 pages on the different drugs and whatnot for treatment in Habif... perhaps glance it over? ** rotational therapy seems sweet** |
|

What is it? What are the most effective therapies? |
Pityriasis rubra pilaris- rare, chronic disease of unknown etiology, bimodal in first and fifth decades of life
notice the islands of sparing
eruptions last for months to years
Methotrexate and retinoids are the most effective therapies |
|
|
Seborrheic Dermatitis has a characteristic pattern for different age groups... Infants, kids and adults are mostly affected where? |
Infants- cradle cap, greasy adherent scale on vertex of scalp, tx is frequent shampoo with sulfur or sal acid, stopical steroids
Kids- tineal amiantacea and blepharitis- thick greasy scales on scalp tx with frequent sulfur shampoo, topical steroids
Adults and adolescents- fine, dry, white to yellow scale in seborrheic distribution (scalp, eyebrows, eyelashes, NLF, ear canals, posteroir auricular fold, presternal areas), tx with sulfur, sal acid shampoos, occ oral antifungals, topical steroids |
|
|
Seb Derm is influenced by genetics and environmental factors, but what yeast is probably a causative factor as well? |
Malasezia ovalis |
|
|
5P's of Lichen Planus? What areas are most common? Tx? |
Pruritis, purple, planar, polygonal papules
Tons of different patterns ( localized, hypertrophic, generalized, follicular, oral, genital, vaginal)
Localized papules most common on flexor surfaces (wrists, forearms, legs, lumbar region)
TX: super potent topcial steroids, phototherapy |
|
|
30 year old male patient presents with 4cm oval, red lesion on trunk... 1 week later erupts into smaller lesions located over trunk (kind of Christmas tree looking) and extremities that are salmon pink in color... what probably caused this? What do we need to check? How are we going to treat this? |
Pityriasis Rosea- started with a Herald patch
most likely reactivation of HHV 6 and 7
PR = RPR, rule out secondary syphilis
Usually clears in 1-3 months spontaneously |
|
|
What changes are seen with psoriasis of the nales? |
oncholysis, subungual debris, pitting, oil spot lesion |
|
|
Take a look on page 278, table 8-3 |
review differentiating PsA, RA, OA
** RA spares DIP, PsA affects DIP** |
|
|
Most common locations of oral lichen planus (OLP)? |
80-90% on buccal mucosa 30-50% on tongue |
|
|
What are the nail findings in lichen planus? |
Longitudinal ridging and splitting are most common
Onycholysis
Dorsal pterygium formation
**I highlighted this and wrote THIS WILL BE A TEST QUESTION** so there... |
|
|
What is delling? |
White to brown, horny follicular plugs of the a lesion
This is commonly seen in LIchen sclerosis et atrophicus |
|
|
How to we treat lichen sclerosus et atrophicus? Why are we worried about it? |
Increased risk for SCC
treat with high potency topical steroids or systemics |
|
|
White, hour glass shaped plaque over vulva? |
lichen sclerosus et atrophicus |
|
|
What group and phage types of staph aureus cause bullous impetigo? |
group 2, phage 55&71
(listed as second year question)
**this is the same a staph scalded skin syndrome** |
|
|
Bullous impetigo is toxin mediated by which toxin? |
staph aureus exfoliatoxin A- this toxin causes intraepidermal cleavage below or within the stratum granulosum
**this is the same a staph scalded skin syndrome** |
|
|
Most likely target for exfoliative toxin A in bullous impetigo is? |
Desmoglein 1
**this is the same a staph scalded skin syndrome** |
|
|
What is the difference between cellulitis and erysipelas? |
Erysipelas is a type of cellulitis that involves the superficial layers of the skin and cutaneous lymphatics (causes prominent lymphangitic streaking), cellulitis extends into the subcutaneous tisues
|
|
|
Cellulitis and erysipelas most common causes by what? |
STREP |
|
|
Perianal cellulitis MCC? |
group A beta hemolytic STREP |
|
|
Necrotizing Fasciitis MCC? |
trick question! most are polymicrobial! (type I) |
|
|
What is Fournier's Gangrene? |
Gangrene of the penis, scrotum, perineum d/t group A strep or mixed infection with enteric bacilli and anerobes |
|
|
treatment for KP? |
ammonium lactate, urea |
|
|
A 56 year old fisherman presents wtih a 2 day history of a dull, red, patchy erythema over his right hand with some burning and itching |
FISHERMAN!! |
|
|
What is Ritter's Disease? Cause? |
Staph Scalded Skin Syndrome
d/t staph group 2, types 71&55 **this is the same a bullous impetigo** |
|
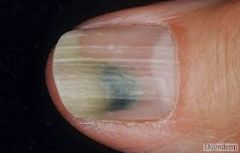
What is causing the green color? |
Green Nail Syndrome--> infection with Pseudomonas
Pyocyanin is reponsible for the green color
Pyoverdin is reponsible for the green fluorescence with a wood's lamp |
|
|
What is the cutaneous manifestation of pseudomonas septicemia? |
Ecthyma gangrenosum-- will see gray-black-green eschar, common seen in burn patients, immunosuppressed, heme malignancy |
|
|
Patient presents wtih stiff neck, headache, papular nonhemorrhagic rash involving the axillae, trunk, wrists and ankles |
Meningococemia-- treat him now! early abx with PCN, cefotaxime, ceftriaxone, chloramphenicol IV or IM |
|
|
BUZZ PHRASE: gun metal gray, angulated, stellate purpura |
MENINGOCOCCEMIA
... guns are BAD and will kill you, acute mengiococcemia kills faster than any other disease apparently (hours) |
|
|
DDX of painless genital ulcer? |
Syphilis, lymphogranuloma venereum, granuloma inguinale |
|
|
DDX of painful genital ulcer? |
Chancroid, HSV |
|
|
Syphilis facilitates the transmission of what disease? How does it do this? |
HIV! early syphilic lesions have increased expression of CCR5, which is a co receptor of HIV |
|
|
Describe the progression of syphilis. |
Primary syphilis- single, painless, hard genital ulcer acquired within 10-90 days (average 21) by direct contact (risk 10-60%), this lesion will heal in 3-6 weeks
Secondary syphilis- muco-cutaneous lesions, flu like symptoms, alopecia (moth eaten), adenopathy; lesiosn are polymorphic and can really resemble anything
Latent syphilis- seroreactivity without any evidence of the disease
Tertiary syphilis- about 1/3 of untreated patients, CV disease (aneurysm), tabes dorwalis, argull robinson, gummas |
|
|
What conditions can cause a false positive RPR? |
vaccinations, infections, pregnancy, lupus, liver dz, IVDU, old age |
|
|
What conditions can cause a false negative RPR? |
Prozone phenomenon- large amount of Ab blocks the antibody/antigen causing, false negative, most common in secondary syphilis and pregnancy |
|
|
How do we treat syphilis? |
Depends on the stage!
Primary and Secondary: IM PCN x 1 Tertiary: weekly PCN x 3
f/u RPR at 3,6,12 months, look for a 4 fold decrease in titre to signal effective therapy |
|
|
Congenital syphilis findings? |
Early congenital syphilis- snuffles (most frequent finding), morbiloform skin eruption, pemphigus syphiliticus, FTT
Late congenital syphilis- frontal bossing, saddle nose, short maxilla, hutchinsons teeth, Higoumenakis sign, rhagades, hutchinsons triad |
|
|
What is Hutchinson's Triad? |
pathognomonic of late congenital syphilis: hutchinsons teeth, interstitial deratitis, CN VIII deafness |
|
|
What is the cause of lymphogranuloma venereum? |
Chlamydia Trachomatis L1-L3 |
|

Patient presents with a painless penile ulcer. |
Groove Sign of LYmphogranuloma venereum, from inguinal lymphadenopathy
** I'm willing to bet money that this will be a test koda |
|
|
Treatment for lymphogranuloma venereum? |
Doxy 100mg BID x 21d |
|
|
Treatment for chancroid? |
ZITHROMAX 1G X 1 |
|
|
Painless broad, superficial ulcer with beeft red granulation tissue? |
granulation tissue = Granuloma inguinale aka. donovanosis |
|
|
What organism causes Granuloma inguinale? |
Klebsiella granulomatis
organisms likve in macrophages (donovan bodies) |
|
|
TX for granuloma inguinale? |
doxy 100mg BID x 3 weeks |
|
|
If a patient has a gonorrhea, what riskfactors increase their risk of progressing to gonococcemia? |
Menstruation and C5-C9 complement deficiency |
|
|
Treatment of gonococcal urethritis/cervicitis? |
ceftriaxone 250mg X1 IM
also treat for chlamydia with azithromycin 1g PO x1 or doxy 100mg BID x 7 days |
|
|
HPV strains in genital warts? |
HPV 6, 11 (and 16) |
|
|
HPV strains in genital dysplasia? |
HPV 16, 18 |
|
|
What is the cellular target of Imiquimod used to treat genital warts? |
TLR 7 |
|
|
What is bowenoid papulosis? |
Papules that are asymptomatic, small, flat, reddish to brown, coalescent and have a smooth velvety surface. Many patients have ahistory of genital infection with viral warts or herpes. HPV 16 >18 have been found
Check female partners, they are at higher risk of cervical dysplasia |
|
|
Giant Condyloma of Buschke-Lowenstein? |
verrucous carcinoma, commonly HPV 6>11 (elevenstein)
cut this out! |
|
|
Who can get the gardasil vaccine? |
Girls 11-26, Boys 9-26
Against 6, 11, 16, 18 |
|
|
Risk of recurrence of HSV? |
GHSV2 >> OHSV1 >> GHSV1 >> OSHV2 |
|
|
What sequelae are associated with congenital HSV infection? |
Congenital HSV (intra-uterine)- fetal skin lesions, microcephaly, encephalitis, chorioretinitis, intracranial calcifications |
|
|
What sequelae are associated with neonatal HSV infection? |
Neonatal HSV (transmission at birth or right after)- encephalitis, hepatitis, PNA, coagulopathy, corneal blindness |
|
|
Top three most common skin disorders in HIV + patients? |
1. pruritic papular eruption 2. HSV 3. Kaposi's sarcoma |
|
|
HSV acyclovir treatment for primary, recurrent (episodic vs long term) |
Primary: 400mg TID x 7-10 days Recurrent episodic: 400mg TID x 5 days Recurrent long term: 400mg BID x FOR-EV-ER
There are other acyclovir doing regimens listed on 468 |
|
|
What is the most worrisome complication of varicella infection? |
varicella PNA- mortality rate for adult PNA is 10% in immunocompetent populations, 30% in immunocompromised populations |
|
|
Life time risk of herpes zoster? |
10-20% risk, second attack is 5% |
|
|
What is Hutchinson's sign with regards to Herpes Zoster Ophthalmicus? |
Vesicles on the side or tip of the nose that occur during an episode of zoster are associated wtih the most serious complications |
|
|
What is Ramsay Hunt Syndrome? What are the symptoms? |
peripheral facial nerve palsy accompanied by a esicular rash on the ear (zoster oticus) or in the mouth, caused by zoster of the geniculate ganglion
ssx include tinnitus, hearing loss, nausea, vomiting, vertigo, nystagmus |
|
|
Half moon shaped plaques with scaling border on right upper thigh, does NOT fluoresce with woods lamp? Pathogen? |
Tinea cruris, Tricophyton rubrum
**remember- tinea respects the penis and scrotum, candida does not
If you had this same scenario and the lesion DID fluoresce... think Erythrasma |
|
|
MCC of tinea pedis? |
TRICOPHYTON RUBRUM |
|

pathogen? |
Pitted Keratolysis- bacterial infection from Micrococcus sedentarius |
|
|
Brown, scaly plaque on right groin. Fluoresce coral red with wood's lamp. Pathogen? |
It's fluorescing... so it's erythrasma!
Corynebacteria minutissimum |
|
|
This distinct form of inflammatory tinea caused by trichophyton rubrum is most commonly found on the lower legs (shaving areas) |
Majocchi's granuloma |
|
|
Which dermatophytes are primarly responsible for ectothrix invasion? Endothrix invasion? |
Ectothrix: most of the Microsporums, Cats And Dogs Fight and Growl Sometimes --> m. canis, m. audouinii, m. distortum, m. ferrugineum, gypseum, t. schoenleinii
Endothrix: most of the Trichophytons, TV'S R in the house --> t. tonsurans, t.violaceium, t. soudanese, t. rubrum
**T. rubrum can actually do either |
|
|
MC pathogens for black dot tinea capitis? |
T. tonsurans, T violaceum (these are both endothrix infections) --> hair cortex replaced by spores (endothrix) and shaft weakens and shears at the scalp surface |
|
|
What is a Kerion? |
a form of scaring alopecia secondary to inflammatory reaction to fungal reaction (mc T tonsurans, m canis) |
|
|
MC pathogen for tinea unguium? |
Trichophyton rubrum (same as tinia pedis) |
|
|
How do you differentiate Candidal vs. Tinea infection on KOH prep? |
On KOH prep, candida will have pseudohyphae
Tinea will have tru hyphae |
|
|
DOC for Candidal infection? MOA? |
Nystatin is the drug of choice --> irreversibly binds cell membrane sterols and increases permeability |
|
|
toe vs fingernail onychomycosis treatment? |
12 weeks v 6 weeks with oral terbinafine |
|

What is your DDX? What would you use to treat this if you scraped it and you saw spaghetti and meatballs? |
DDX: tinea versicolor, vitiligo, pityriasis alba, tinea corporis, seb derm, syphilis (as always), pityriasis rosea
If you dx tinea versicolor (pityrosporum obicularis/ovale), use an azole... I'd probably do selenium sulfide shampoo too |
|
|
What oral antifungal agent is associated with an SCLE like reaction and an exacerbation of psoriasis? |
Terbinafine (side note--- track these guys LFTs) |
|
|
What antifungal is the best choice for a paitent with mucocutaneous candidiasis who is currently taking antacids? |
Fluconazole (itraconazole and ketoconazole have better absorption in acidic environments) |
|
|
Basics of woods lamp examination of hair tinea? Which type fluoresces? |
Examination will show green fluorescence with ectothrix organisms M. audouinii, M. canis, m.distortum, m. ferruginueum/gypseum, t.schoenleinii
No fluorescence with endothrix organisms |
|
|
This organism produces an endothrix tinea capitis:
T. mentagrophytes M. gypseum M. nanum T. verrucosum T. soudanense |
T. soudanense |
|
|
Which dermatophyte is not an anthropophilic organism?
t. rubrum e. floccosum m. gypseum |
M. gypseum- geophilic! |
|
|
Dermatophyte responsible for tinea corporis gladiotorum? |
T. tonsurans |
|
|
How does the rash of Rubeola spread and when does it appear? Another name for Rubeola? |
Measles (Rubeola)- Child will experience a prodrome 1-3 days peior to rash with cough, congestion, conjunctivitis, fever --> on 4th or 5th day morbiliform rash will start on head and spread down entire both |
|
|
What is the most common cause of death in Measles? |
PNA is mcc of death
other complications include blindness, encephalitis, SAB |
|
|
What live vaccines do we give? |
"Live! One night only! See small yellow chickens get vaccinated with Sabin's and MMR!"
small pox, yellow fever, chicken pox, sabins polio, mmr |
|
|
What is the management of measles? |
mostly supportive and treating any bacterial infections
**also give vitamin A
If it's within 72 hours, can given live vaccine |
|
|
What viruses are HFMD associated with? |
coxsackievirus A16, enterovirus 71 |
|
|
Blue gray spots on buccal mucosa in a 4 year old unvaccinated child with fever? |
Koplick spots---> think measles (rubeola) |
|

What is an important question to ask about this patient's history? |
These are Beau's lines- ask about any recent illness over the past few months, can be d/t any illness causeing a hypermetabolic state |
|
|
You see a child who has a postive rapid strep, they have been sick and currently have a whole body rash (very sandpapery)... how do you treat and what do you warn mom about? |
Scarlet fever produced by Exotoxin A from Strep pyogenes
Treat with PCN, cephalosporins, erythromycin
Warn mom that after the rash and fever resolve, they will have desquamation of the rash that can last 4-8 weeks. Also have her keep an eye on the childs urine for a few weeks (tea colored GN) |
|
|
Cause of scarlet fever? |
Exotoxin A produced by strep pyogenes |
|
|
Pastia's lines and forchheimer spots are associated with... |
scarlet fever (look at these kodas) |
|
|
Rubella is most devestating to the fetus if acquired in which trimester? What problems will they have? |
Most devestating if in 1st trimester
Deafness, cataracts, eye problems, PDA, blueberry muffin |
|
|
What is the main target of parvovirus B19 in erythema infectiosum? |
RBC globoside (P antigen) of erythroid progenitor cells of the BM
|
|
|
Child went to her pediatrician with fever, sore throat, and slapped cheek rash and was diagnosed with 5th disease... the child should stay home to prevent spread to her pregnant teacher... right? |
WRONG-O!
by the time these kids get the rash, they aren't infectious anymore... BUT the other kids in the class are probably harboring the virus (incubation period 13-18 days), so the TEACHER should stay home |
|
|
What arthropathies are associated with parvovirus B19? |
Women develop RA like arthritis- look for antiparvovirus B19 IgM and/or IgG (IgM may be gone after a few months)
Kids can get knee arthritis lasting up to 4 months |
|
|
Why are we worried about pregnant women and exposure to B19? |
anemia, CHF, generalized edema (hydrops) and death
1st trimester infection associated with 10% fetal loss |
|
|
Cause of Roseola Infantum? What does the rash look like? |
HHV 6 remains latent in monocytes and macrophages, the rash is SUDDEN (examthem subitum) and appears everywhere (no spread) as pale pink, almond shaped macules |
|
|
How do you clinically diagnose Kawasakis? |
CRASH and burn
Fever for at least 5 days, conjunctivitis, rash, arthritis/adenopathy, strawberry tongue, hands desquamate |
|
|
What are the three phases of Kawasakis? Why are we so worried about it? |
Acute: CRASH and burn symptoms Sub acute: desquamation of palms and soles Convalescent: good to go
It is a major cause of acquired heart disease in children (coronary aneurysm) |
|
|
What are superantigens? |
Antigens that stimulate T cells without first being processed by antigen presenting cells... so they are activating 5-30% of T cells insteat of conventional 0.01%
Examples include: staphylococcal enterotoxins A-E, **TSST-1, **Exfoliating toxin, strep M protein, strep pyrogenic exotoxins A-C |
|
|
Time between drug and acute generalized exanthemaous pustulosis (AGEP)? |
Usually 24-48 hours.. 1mm white monomorphic pustules, STOP THE DRUG |
|
|
What are our typical culprits for a fixed drug eruption? Where is it normally seen? |
Tetracyclines, bactrim are the most common medications.. most ocmmon location is on the glans penis or vulva |
|
|
Where are the lesions of a fixed drug eruption secondary to Pseudoephedrine usually located? |
non pigmented, on oral mucous membranes |
|
|
What makes people more susceptible to drug induced lupus? |
HLA-DRW4, women, slow acetylator status |
|
|
What drugs are notorious for causing a drug induced lupus? How can you prove it? |
SHrIMP!! Sulfasalazine, hydralazine, (r), isoniazid, minocycline, procainamide **MC in US
Anti-histone antibodies are seen in 95% of drug induced SLE
|
|
|
progression of hyperpigmentation drug reaction from minocycline? |
I- acne scars/inflammation II- skin on anterior shin and forearms III- muddy brown discoloration in sun exposed areas IV- thryoid deposits
**I have thyroid deposits starred a few times**
|
|
|
What is the difference between the Nokolsky sign and Asboe-Hanson sign? |
Nikolsky: pressure on normal or perilesional skin causes the upper layers to sluff off
Asboe: pressure on an intact bullae forces the fluid to spread under the skin away from the site of pressure
Asboe = as above |
|
|
Bullous diseases resulting in a subcorneal split? |
Pemphigus foliaceus, bullous impetigo, SSSS, drug induced pemphigus |
|
|
Bullous diseases resulting in an intraepidermal split? |
Pemphigus vulgaris, paraneoplastic pemphigus, dariers disease, Hailey-Hailey, insect bites, friction blister |
|
|
Bullous diseases resulting in a subepidermal split? |
bullous pemphigoid, dermatitis herpetiformis, linea IgA, PCT, epidermolysis bullosa diaseases, sucking blisters |
|
|
70 year old man with DM presents with fluid filled blisters on his right shin. He states he's had them before and they always go away in a few weeks. What's going on? Treatment? |
Bullous Diabeticorum ** know this **
Spontaneous healing, just watch out for infection |
|
|
55 year old Jewish male presents with painful, flaccid blisters on his chest and groin that will rupture and sluff with slight pressure. What associated conditions do you need to be on the look out for? |
Pemphigus Vulgaris- old people, oral lesions, flaccid blisters, nikolskys sign
antigens to Desmoglein 3 (130kd) and Desmoglein 1 (230kd)
Associated conditions: THYMOMA, MG |
|
|
What is the Desmoglein Compensation Theory? |
Skin Dsg 1 >> Dsg 3
Mucous membranes Dsg 3 >> Dsg 1
1. Pemphigous foliaceus: anti Dsg1, so more skin blisters, no mucosal lesions
2. Mucosal dominant PV subtype: anti Dsg 3, so more mucousal lesions, no skin lesions
3. Mucocutaneous PV: anti Dsg 3 and Dsg 1, so both skin blisters and mucosal erosions |
|
|
What drugs induce pemphigus? What pattern of pemphigus is it most commonly? |
Usually a pemphigus foliaceus pattern (skin lesions only)
Penicillamine **** Captopril **** pemphigus/pemphigACEi Enalapril PCN |
|
|
What are the two types of pemphigus vegatans? |

This is Neumann. This will haunt you forever :( Fungating papillomatous plagues with hypertrophic granulation tissue
1. Neumann- the worst one!!
2. Hallopeau- more mild |
|
|
Which subtype of pemphigus shows 'chickenwire' on DIF? |
Pemphigus foliaceus (anti- Dsg 1) |
|
|
Pemphigus Erythematosus has immunologic features that are shared between... |
pemphigus vulgaris and lupus!
IgG and C3 deposition on keratinocytes as well as BMZ in addition to antinuclear antibodies
so check for both ** I have this starred as a test question ** |
|
|
What is pemphigus erythematosus? |
Localized variant of pemphigus foliaceus distributed on nose, cheeks, ears and other seborrheic areas (aka senear usher syndrome)
**note, check for regular PV AND LUPUS when you see this |
|
|
Rat bladder substrate is used for IIF in what disease? |
Paraneoplastic pemphigus
that rat bastard gave me cancer!
Intractable stomatitis, erosions of oropharynx, conjunctivitis |
|
|
What cancers are paraneoplastic pemphigus associated with? What antigens are present in paraneoplastic pemphigus? |
Non hodgkins lymphoma (42%) CLL (29%) Castleman's (10%)
Paraneplastic pemphigus attacks EVERYTHING (except BPAG2) |
|
|
What is the most sensitive marker in dermatitis herpetiformis? |
Anti-TG3
these levels DO correlated with the extent of small bowel pathology, and can thus be used to assess compliance with a gluten free diet |
|
|
Why is it so important for patients with Dermatitis Herpetiformis to be compliant with a gluten free diet? Can't we just given them Dapsone and call it a day? |
Dapsone does not change the risk of GI lymphoma, only the diet does!
CROPS: corn, rice, oats, potatoes, soy |
|
|
patient with gluten insensitivity has a rash, take a biopsy and see a ton of neutrophils stuffed into the dermal papillae... |
DH |
|
|
patient has DH, what do you need to look for? |
IDDM, thyroid issues (hasimotos), lymphoma |
|
|
Molecular weights of: Desmoglein 3 Desmoglein 1 BPAg1 BPAg2
|
Desmoglein 3 (PV) 130kDa Desmoglein 1 (PV) 160kDa BPAg1 (BP) 230kDa BPAg2 (BP) 180kDa |
|
|
Causes of drug induced bullous pemphigoid? |
CLiPS: Captopril, lasix, PCN/penicillamine, sulfa
remember, those ACEis and PCN/penicillamine can also induce pemphigus |
|
|
Which antigens are associated with Bullous Pemphigoid? |
BPAg1 (230kDa) hemidesmosome BPAg2 (180kDa) pathogenic **remember this is the only thing that isn't attacked with paraneoplastic pemphigus |
|
|
Pregnant woman in second trimester comes in with pruritis urticarial/bullous eruption on her belly and in her umbilicus. Do you just tell her its PUPP and send her on her way? What is your next step? |
NOPE! THIS AIN'T PUPP!
PUPP doesn't involve the umbilicus. If the belly button is involved, you have to to think of gestational pemphigoid.
Gestational pemphigoid has a high association with Graves Disease, so next you need to get her TFT's (this will be a test question) |
|
|
What antibodies are present in gestational pemphigoid? Will baby get it? |
Antibodies to BPAg2 (pregnant women can eat for 2)
10% chance that baby will have BP lesions at birth |
|
|
Which type of pemphigoid can present with symblepheron? |
Cicatricial pemphigoid
Symplepheron: fibrous tracts between bulbar and palpebral conjunctival survaces |
|
|
Which antigens are present in cicatricial pemphigoid? |
BPAg2, laminin 5 (solid tumors), a6B4 (ocular only)
CP, think eyes |
|

60 year old female with hx of Chrons and LSE admitted for PNA and was given IV antibiotics. Now she has this rash and Derm is consulted... |
Notice the 'crown of jewels' pattern- this is most likely drug induced LInear IgA Bullous Dermatosis- causes include Vanc, PCN, cephalosporins, sulfa |
|
|
Antigens associated with Linear IgA Dermatosis? |
LAD-1, BPAg1, BPAg2
this can really be d/t anything, even drugs |
|
|
What is Brunsting-Perry? |
Cicatricial Pemphigoid of the head and neck with scarring alopecia |
|
|
Hailey-Hailey Disease is also known as... |
Benign familial pemphigus (inheritance pattern is AD) |
|
|
What genetic defect is associated with Hailey-Hailey disease? Inheritance pattern? |
ATP2C1
2 C 1 is to see them all, AD inheritance |
|
|
30 year old Asian male with blisters on his hands for the past 3 months. Says that when they heal, it leaes behind a little white papule. He also has bloody poop. |
Epidermolysis bullosa acquisita- acral blisters that heal with milia, association with Chrons disease, more common in Asians |
|
|
Types of Epidermolysis bullosa? This is a packed slide. |
Epidermolysis bullosa simplex- no scar, think of new recruits who are constanting marching and present with a crap load of blisters!! Keratin 5, 14
Junctional epidermolysis bullosa- super crappy, Herlitz type is the severe type (Herlitz hurtz more), extensive involvemnt of mouth, larynx, eyes, laminin 332
Dystrophic epidermolysis bullosa-mitten deformities, COL7A1 (collagen 7)
Epidermolysis bullosa acquisita- asians with chronis disease, blisters heal with milia, collagen VII |
|
|
Erythema Toxicum neonatorum and transient neonatal pustular melanosis differ how in their diagnostic studies? |
Erythema Toxicum Neonatorum: Eosinophils on wrights stain
Transient Neonatal Pustular Melanosis: PMN |
|
|
Criteria for SLE? |
I'M DAMN SHARP
Immune (dsDNA, smith...) Malar rash Discoid rash ANA+ Mucous ulcers Neuro Serositis Heme Arthritis Renal Photosensitivty
|
|
|
Side effects of Terbinafine? |
dysguesia, hepatotoxicity, agranulocytosis, SJS, SCLE like rash, psoriasis flare |
|
|
cross reactivity with latex? |
BACK passion
Bananas, avacados, chesnuts, kiwi, passion fruit |
|
|
What antibody is present in discoid lupus when it is widespread? |
ssDNA |
|
|
What type of skin cancer can develop in scars from discoid lupus? |
SCC |
|
|
What is the most common antibody with subacute cutaneous lupus erythematous? |
ANTI RO (SSA) |
|
|
What antibodies are associated with acute cutaneous (systemic) lupus erythematous? |
ANA, dsDNA, Ro, La, Smith |
|
|
What antibodies are associated with neonatal lupus erythematous? |
Maternal passage of Ro and/or La or U 1-RNP |
|
|
What antibodies are associated with drug induced systemic lupus erythematous?
What about drug induced subacute cutaneone lupus erythematous? |
SLE: Anti histone, ssDNA |
|
|
What are the major differences between drug induced SLE and drug induced SCLE?
|
Drug induced SLE: NO skin eruption, lots of systemic symptoms, resolution after drug is stopped
Drug induced SCLE: papulosquamous or annular polycyclic eruption, NO systemic symptoms, lesions may persist after discontinuation of drug |
|
|
What drugs cause drug induced SLE? drug induced SCLE? |
drug induced SLE: SHrIMP- sulfonamides, hydralazine, isoniazid, minocycline, procainamide
drug induced SCLE: HCTZ, NSAIDS, terbinafine, diltiazem |
|
|
What nail changes are associated wtih dermatomyositis? |
Dermatomyositis has Dilated or Dropout nail fold capillaries |
|
|
What are the most common cancers associated with dermatomyositis? |
lung, ovary, heme |
|
|
What antibody seen in dermatomyositis can be associated with lung disease? What is the finding on physical exam? |
Anti-Jo 1
Mechanics hands |
|
|
What is Parry Rhomberg a sequelae of? |
Feared compication of scleroderma/coup de sabre --> hemifacial atrophy with ophtho and neuro complications |
|
|
What organ is the leading cause of death in patients with Scleroderma? |
LUNGS- pulmonary artery hypertension |
|
|
MC treatment for sebaceous hyperplasia? |
electrocautery: set at 2-3.5 |
|
|
Multiple DFs could be a sign of... |
SLE, immunosuppression |
|
|
Which sign does a dermatofibroma not exhibit, Retraction, Dimple, or Firzpatrick's? |
it shows all of them!! they are all the same freaking thing. |
|
|
Multiple SKs recently erupted in elongated streaks across body? |
Sign of Lesser Trelat --> could be indicative of GI carcinoma |
|
|
Eruptive syringomas can be associated with? |
Downs syndrome |
|
|
Clear cell syringomas can be associated with? |
diabetes mellitus |
|
|
What growth factor is elevated in keloids? |
TGFB |
|
|
What is the most common mutation in epidermal nevi? |
FGFR3 |
|
|
What secondary neoplasia is most common in adult nevus sebaceus? |
trichoblastoma!! |
|
|
What is sebaceous nevus syndrome? |
AKA Schimmelpenning syndrome: in babies (in your SON) skeletal anomalies, ocular colobomas, neurologic complications (MR) |
|
|
Child presents with a ton of EICs. What do you need to be on the lookout for? |
Gardner's syndrome- colon polyps and adenocarcinoma |
|
|
What is Muir Torre syndrome? |
at least 1 sebaceous tumor and 1 visceral malignancy |
|
|
What viceral malignancy is most common in Muir Torre? |
Colorectal |
|
|
What is the lifetime risk of BCC in Caucasians? Most common place? |
30% lifetime risk, MC spot is the nose |
|
|
How likely is BCC to metastasize? If it does metastasize, where does it usually go? |
Risk is 0.0028% to 0.55%
MC is lymph nodes > lungs |
|
|
What viruses are implicated in Bowenoid papulosis? |
hpv 16/18 |
|
|
What is the deal with sun exposure in BCC vs. SCC? |
BCC is due to intermittent/recreational sun exposure
SCC is due to cumulative/occupational sun exposure |
|
|
Cutaneous metastasis in men usually occurs where? |
LUNG
LADS! ITS GOES TO YOUR LUNGS! |
|
|
Cutaneous metastasis in women usually occurs where? |
BREAST |
|
|
What infections are classically associated with erythema multiform? |
Herpes simplex virus 1&2 Mycoplasma pneumonia |
|
|
Which drugs are most often associated with SJS/TEN? |
SATAN!!!! NSAIDS
know that 40% is due to the antibiotics |
|
|
What are the SCORTEN variables? |
HUGS BAM! No, hugs won't make you better (sorry psychiatry), but it will help you remember the criteria...
HR >120 Urea > 10 Glucose >14 Skin sluff >10%
Bicarbonate <20 Age >40 Malignancy history!
Each one gives you a point and if you have 5 or more, you have a 90% mortality rate |
|
|
What are some of the more common causes of Erythema Nodosum? (infectious, drugs, systemic illness) |
Infectious: streptococci, URI, cat scratch :<(
Drugs: OCP, sulfa |
|
|
Wegner was apparently a Nazi, so we're calling it by it's real name! Wegner's granulomatosis is... |
Granulomatosis with polyangitiis |
|
|
Churg Strauss may have been a Nazi too... So what's the real name? |
Eorinophilic granulomatosis and polyangitiis |
|
|
What antibody is classically associated with granulomatosis with polyangitiis (Wegners)? |
Wegners: C-ANCA (PR3) think of C3PO!
Churg Strauss: P-ANCA (mpo) |
|

Several days of fever and malaise and THIS:
What questions do you want to ask? How can you treat him?
|
This is HSP. Ask about abdominal pain, bloody stool, scrotal swelling, dark urine, arthralgia. |
|
|
What is the most common type of heme cancer associated with Sweet's Syndrome? |
AML is the most common cancer
G-CSF is common associated with Sweet's |
|
|
Why is it important to follow up with a diagnosis of Sweet's Syndrome if a cause is not identified? |
Causes can include strep infection, IBD, leukemia, heme cancers, pregnancy
Diagnosis of heme disease can take 3mo - 6 years to manifest |
|
|
A collegue asks you to give the nuts and bolts of Erythema elevatum diutinum (EED) as a family member of his was just diagnosed... what would you tell him? |
Persistent, brown-red to putple papules, nodule and plaques distributed on extensor surfaces of the extremities with a preference for joint regions
This is most likely caused by immune complex deposition in response to exposure to antigens (strep) or wituations in which high levels of antibodies occur (paraproteinemias)
Paraproteinemias- myelodysplasia, MM, hypergammaglobulinemia |
|
|
What diseases are associated with pyoderma gangrenosum? |
UC, chrons, RA, hronic active hepatitis, heme/lymph malignancies
Treat the skin stuff with oral steroids or cyclosporine |
|
|
A patient comes in with a rash and says 'DOC! It looks like someone dropped a full bottle of Cayenne Pepper on my legs!! What's going on and what can I put on it to make it go away?!' |
CAYENNE PEPPER- SCHAMBERGS PURPURA
Patient has some leaky capillaries near the skin, allowing some RBCs to slip through and deposit some hemosiderin... sorry bro, but there isn't anything we can do except wait for the pigmentation to diffuse. Don't worry, no association with anything scary. |
|
|
Common moles are, well, common. What is the progression of a common mole? |
During childhood, nevi begin as flat junction nevi, cellus are located at the DEJ.
You will make these from 6mos into your 30s... then you typically don't make anymore new ones |
|
|
What can cause an increase in the number of common nevi? |
they will increase naturally from 6mos to 30s. Increase in size/pigment in puberty and pregnancy, increase # with sun |
|
|
How do we classify congenital nevi? Why do we worry about them?! They're just MOLES!! |
Congenital nevi are present at BIRTH or prior to 6mo (after that you start making common nevi)
Small Congenital Nevi- <1.5cm, low risk melanoma (2.6-4.9%), don't need to prophylactially remove, if you want to remove it, do it after puberty
Medium Congenital Nevi- 1.5cm- 20cm, controversial risk of MM, you could really go either way, just watch it or do a small bx
Large Congenital Nevi- >20cm, 1.8-7.1% chance of transformation to MM (1/2 by age 5); REMOVE ASAP |
|

|
Nevus spilus, follow clinically |
|
|
Halo nevi are associated with what? |
TURNER'S SYNDROME
no melanocytes in the halo (doi), T lymphs CD8>CD4 in the halo |
|
|
Why are blue nevi blue? |
Tyndall Effect- brown looks blue deep in the skin, absorbs the longer wavelengths of light and scatters blue light
GNAC mutations most common!!! GNAC reminds me of gnats... which are annoying... and it would probably be annoying to have a blue mole, right? |
|
|
When do people start growing atypical nevi? |
Atypical (dysplastic) nevi can appear during puberty, and you continue to grow these well past your thirties
|
|
|
What criteria must be met, clinically, to diagnose an atypical nevus? |
Must meet 3/5 features:
>6mm irregular borders variable color (red is dead) ill defined margins papular/macular components |
|
|
What criteria need to be met for atypical mole syndrome? |
(1) MM in at least 1 1st/2nd degree relative (2) large number of melanocytic nevi (50+) (3) histologic atypical nevus |
|
|
What is the risk of melanoma in an average caucasian person in the US?
How is that risk changed in a patient with: (A) h/o atypical mole syndrome without a FH of MM? (B) h/o atypical mole syndrome WITH a FH of MM? (C) h/o atypical mole syndrome with personal MM? |
Risk of melanoma in average caucasian person in the US? 0.8%
(A) h/o atypical mole syndrome without a FH of MM? 6%
(B) h/o atypical mole syndrome WITH a FH of MM? 15%
(C) h/o atypical mole syndrome with personal MM? 10% |
|
|
What are the four major clinical-histopathologic subtypes of melanoma? |
1. Superficial spreading (70%)- slower growth 2. Nodular (15-20%)- rapid growth 3. Lentigo Maligna (4-15%)- usually on face 4. Acral Lentiginous (2-8% in whites, 30-75% in AA, A, H) |
|
|
What are the Clark Levels for MM? |
Measure tumor invasion anatomically
1. Intraepidermal 2. In papillary dermis 3. Fills papillary dermis 4. Reticular dermis 5. Enters fat
**this wasn't in lecture |
|
|
Given MM thickness, what is the surgical managment?
In Situ <1.0mm 1.1-4.0mm >4.0mm
|
In Situ --> 0.5cm <1.0mm --> 1.0cm 1.1-4.0mm --> 2.0cm >4.0mm --> 2.0-3.0cm |
|
|
When do you perform a sentinel node biopsy in a melanoma patient? |
ANY TIME THE DEPTH IS >1MM |
|
|
LOOK AT PAGE 876 FOR THE MELANOMA STAGING TABLE. |
He said there will be a question on this. |
|
|
T classification for MM? |
T1 1.0mm T2 1.01-2.0mm T3 2.01-4.0mm T4 <4.01mm
and remember a vs b is whether it's ulcerated or not |
|
|
N classification for MM? |
N1 1 node N2 2-3 nodes N3 4+ nodes |
|
|
M classification for MM? |
M0 nothing M1a distant skin and nodes M2b lungs M3c everything else |
|
|
Hair anatomy from outside to inside: |
OUTER LAYERS FIRST
Outer root sheath (ORS) Inner root sheath (IRS --> Henle --> Huxle --> cuticle of IRS) Hair Cuticle Hair Cortex (synthesize and accumulate protein, melanosomes) Hair Medula (melanosomes) |
|
|
Average hair growth cycle for scalp hairs? |
Anagen 1000 days Catagen 10 days Telogen 100 days |
|
|
What happens in Anagen? How many hairs are in this phase? what does the bulb look like? |

85-90% of scalp follicles, growth phase, lasts 1000 days, bulb looks like a hockey stick
|
|
|
What happens in Catagen? How many hairs? |
Less than 1% of hairs, involution phase, 10 days |
|
|
What happens in Telogen? How many hairs? What does the bulb look like? |

5-10% of hairs (up to 50% on trunk), resting phase, 100 days, bulb looks like a club, white base |
|
|
What is the pathogenesis of androgenetic alopecia? |
Progressive shortening of successive anagen cycles, TERMINAL HAIRS ARE MINIATURIZED AND REPLACED BY VELLUS HAIRS |
|
|
What are the non scarring alopecias? |
Telogen effluvium Androgenetic Alopecia Alopecia areata Traction alopecia |
|
|
Where are the androgen sensitive hairs on the scalp? The androgen independent ones? |
ANDROGEN SENSITIVE HAIRS ON VERTEX FRONTAL SCALP
ANDROGEN INDEPENDENT SIDES AND BACK |
|
|
Aside from varying degrees of hair loss in alopecia areata, what is another common finding? |
NAIL CHANGES- pitting or dystrophy |
|
|
Hair pull test shows increase number of telogen hairs... first how do you know they are telogen hairs? Differential? |
The telogen hairs have white bulbs that look like a club
DDX includes telogen effluvium (nonscarring), diffuse alopecia areata (nonscarring), syphilis (nonscarring) |
|
|
What is the DDX for scarring alopecias? |
TRIPLE D, TRIPLE C and some sweet LP!
Discoid lupus
Central Centrifugal Cicatricial Alopecia (CCCA)
Lichen Planopilaris (frontal fibrosing alopecia)
and acne keloidalis nuchae, but that didn't fit in the rhyme |
|
|
How are the scarring alopecias further classified? |
Lymphocytic, Neutrophilic, Mixed
Lymphocytic: discoid lupus, lichen planopilaris, central centrifugal cicatricial alopecia (CCCA)
Neutrophilic: dissecting cellulitis
Mixed: acne keloidalis |
|
|
What drugs can cause hypertrichosis? |
CYCLOSPORINE, glucocorticoids, phenytoic, minoxidil |
|
|
Hair shaft coated wtih firm, yellow concretions? |
Trichomycosis- corynebacterium |