Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
33 Cards in this Set
- Front
- Back
|
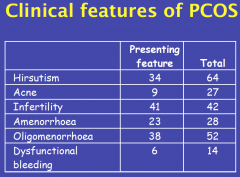
• Clinical features
|
|
|
|
• Definition
|
The presence of two of three:
• Clinical and/or biochemical signs of hyperandrogenism • Oligo and/or anovulation • The appearances on ultrasound of “polycystic ovaries” Exclusion of other known causes |
|
|
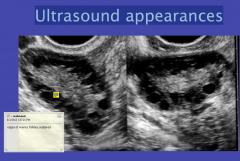
Ultrasound appearances
|
|
|
|
- Definition/Dx
|
The Polycystic ovary should have at
least one of the following: • 12 or more follicles measuring 2-9mm in diameter • Increased ovarian volume (>10cm2) If there is a dominant follicle or corpus luteum, the scan should be repeated. |
|
|
• Pathophysiology
|
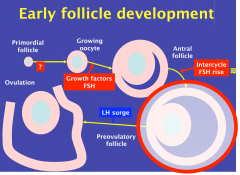
1. May have excess primordial follicles in PCOS
2. INTERCYCLE FSH RISE: cruical for one egg to be selected - transiently rised only long enough for one follicle to mature (IVF: high FSH, thus can stimulate 10-12 follicles to stimulate) - Women on the pill are on it to avoid this FSH rise (but everything else is normal) 3. LH surge is an automatic step that follows FSH rise (thus the FSH rise is most important) IN PCOS: they dont have the FSH rish thus no dominant follicle forms |
|
|
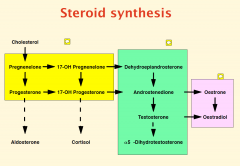
Steriod Synthesis
|
|
|
|
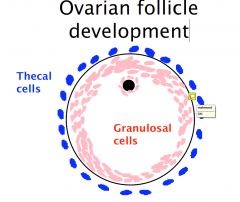
Ovarian follicle
development 1 |
|
|
|
Steriod Synthesis in follicle
|
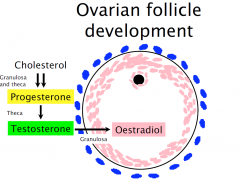
the FSH selects the follicle
|
|
|
The follicle in PCOS
|
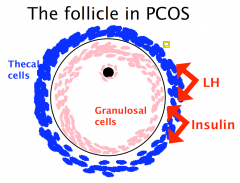
thus excess testosterone
|
|
|
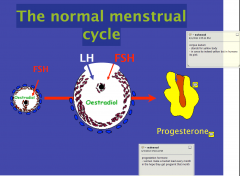
The normal menstrual
cycle |
|
|
|
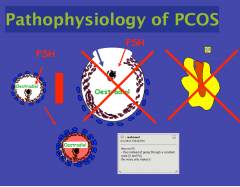
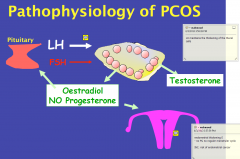
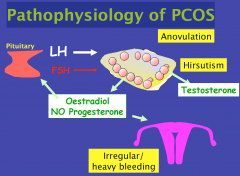
Pathophysiology of PCOS
|
|
|
|
Pathophysiology of PCOS: LH and FSH levels
|
|
|
|
Pathophysiology of PCOS: Sx Mechanism
|
|
|
|
Why is the LH concentration increased?
|
Physiology
Prolonged exposure to unopposed estradiol increased GnRH pulse frequency ?? Antenatal programming? |
|
|
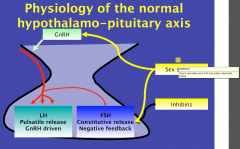
Physiology of the normal hypothalamo-pituitary axis
GnRH.. |
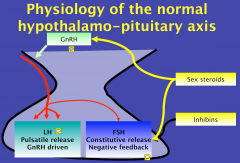
LH mainly driven from above
FSH mainly driven from below GnRH pulsatility is required for effective pituitary function - they speed up in the first half of the cycle - then slows down for PG phase of cycle |
|
|
Physiology of the PCOS
hypothalamo-pituitary axis |
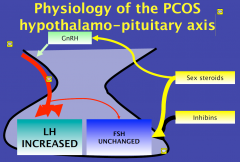
Estrogen: drive the pulsatility (SPEED)
Progesterones: slow it done and because in the PCOS there is no PGs the Es effect keeps getting faster and faster insulin makes the thecel cells grow and make more testosterone (thus makes the problem) thats why women overweight they develop PCOS |
|
|
Why is the insulin concentration increased?
|
• Obesity
• Insulin resistance • ?? Androgen effect in utero |
|
|
• Investigation
|
• Ultrasound scan: important to collaborate
• LH, FSH, PRL • Gestogen withdrawal bleed if amenorrheic • Ovulation check if menstruating • Testosterone • Oral glucose tolerance test with fasting insulin If clinically hyperandrogenic • DHEAS • 17OH progesterone |
|
|
PRL
|
need to exclude amenorrhea due to prolatinoma
|
|
|
Anti-mulleriane Hormone
|
anti-maliraina hormone
- previously guess the amount of egges a women had - this hormone estimates how many eggs the women has - high MAH levels DDx amenorrhea from PCOS |
|
|
Gestogen withdrawal bleed
|
because they dont have normal periods (no PG levels normally)
|
|
|
Testosterone
|
important to check testosterone level (only slightly increased in PCOS) other conditions >5 more serious condition (adrenal gland problems or tumours)
|
|
|
DHEAS
|
one androgen exclusively from adrenal gland
- exclude congenital adrenal hyperplasia |
|
|
Treatment
|
- Clinical Features of PCOS, there is no cure, but then you need to ask the patient what she wants to achieve and what Sx to concentrate on
- However you do need to treat, to red. the risk of endometrial cancer |
|
|
Hirsutism
|
Anti-androgen or 5 alphareductase inhibitor
- blocks the conversion of 5DHT to Testosterone - BUT CANT use them, because it will affect gender selection in pregnagnyc (we are all destined to become females until the testosterone comes along and with a series of long and sophicitated steps, turns us into the sophisticated males that we are - thus never allowed to use this in young women (by drug companies- to protect themselves) |
|
|
Irregular/ heavy bleeding
|
Progestogens or the contraceptive pill
|
|
|
Anovulation
|
Anti-estrogens or aromatase inhibitor
|
|
|
Ovulation induction:
|
Clomiphene citrate
• Use Days 2-6 • Careful instruction and tight monitoring the key to success • Generally not more than 6 months |
|
|
Clomifene citrate: the problems
|
• Side-effects include hot flushes and headaches
• Induces ovulation in 70% but pregnancy in only 30-40% • Adverse effects on endometrium and mucus • Aromatase inhibitors promising but no large randomised controlled trial available for comparison (to block estradiol synthesis) |
|
|
Effects of Metformin
|
not as clear cut
-HOWEVER they do have SE. Side effects; not pleasant stuff to take so need a good reason for taking it • Effective in ovulation induction • May be helpful in IVF • Side-effects can be problematic • NO data on long-term benefits or risks in women with PCOS |
|
|
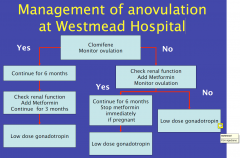
Management of anovulation at Westmead Hospital
|
|
|
|
Low dose gonadotrophin treatment
|
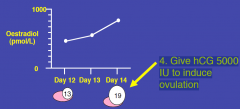
1. Give gestogen to induce withdrawal bleed.
- period 7-10 days later 2. Give slowly increasing doses of gonadotrophin until oestradiol > 400pmol/L. Injections given daily 3. Daily oestradiol measurements and alternate day scans until one (two max.) follicle(s) seen greater than 17mm diameter 4. Give hCG 5000 IU to induce ovulation |
|
|
Ultrasound appearances
|

laser holes into the ovaries that seems to work (but we dont know how it works)
|