Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
51 Cards in this Set
- Front
- Back
|
What is the Adrenal Cortex derived from?
What is the Adrenal Medulla derived from? |
Cortex = Mesoderm
Medulla = Neural Crest |
|
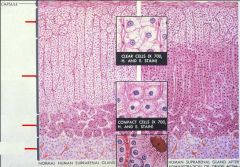
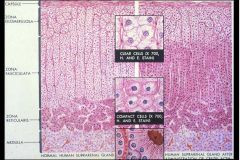
Label the layers of the Adrenal Glands
|
-
|
|
|
List the hormone secreted from each layer of the Adrenal Gland
|
Glomerulosa = Aldosterone = increases Na+ reabsorption; increase K+ & H+ secretion
Fasciculata = Cortisol Reticularis = Sex Hormones = Testosterone, DHEA, Androstenedione Medulla = Catecholamines |
|
|
What are the stimulators & inhibitors of release of each layer of the Adrenal Glands?
|
Glomerulosa
-Stimulators = Angiotensin II; hyperkalemia; ACTH Fasciculata -Stimulator = ACTH -Inhibitor = Cortisol Reticularis -Stimulator = ACTH -Inhibitor = Cortisol Medulla -Stimulator = ACh from SNS |
|
|
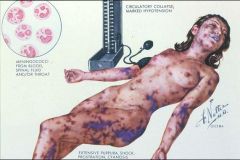
Another name for "Acute Bilateral Hemorrhagic Adrenal Infarction"
|
Waterhouse-Friderichsen Syndrome
|
|
|
What is Waterhouse-Friderichsen Syndrome usually associated with?
|
Septicemia from Neisseria Meningitidis
|
|
|
What bacteria can cause Waterhouse-Friderichsen Syndrome?
|
1. N. menigitidis
2. Pneumococcus 3. Staph 4. Strep 5. Hemophilus |
|
|
What virus can cause Waterhouse-Friderichsen Syndrome?
|
Herpes
|
|
|
Other than infections, what are other causes of Acute Adrenocortical Insufficiency?
|
1. abrupt withdrawal of Corticosteroids
2. Stress 3. Surgery |
|
|
What is the mechanism of Waterhouse-Friderichsen Syndrome?
|
release of tissue Thromboplastin due to Endotoxin causes DIC
|
|
|
Waterhouse-Friderichsen Syndrome due to N. menigitidis
|
What is this called?
|
|
|
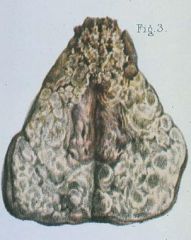
Waterhouse-Friderichsen Syndrome = Acute bilateral adrenal hemorrhage
|

What is the name of this condition?
|
|
|
Waterhouse-Friderichson Syndrome = DIC
|
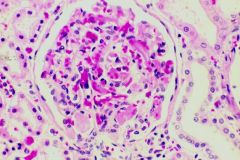
This is a Glomerulus. What adrenal condition is associated with this?
|
|
|
Chronic Adrenocortical insufficiency = ?
|
Addison Disease
|
|
|
What are the clinical features of Addison's Disease?
|
Insidious onset
Signs of decreased Glucocorticoids -weakness & fatigue -GI disturbances -HYPOGLYCEMIA -SKIN HYPERPIGMENTATION = due to MSH, a by-product of increased ACTH production Decreased Alodsterone -HYPOTENSION -Hyperkalemia -Hyponatremia |
|
|
Addison's disease = primary adrenocortical insufficiency
Low Cortisol does not produce feedback inhibition on ACTH production = high ACTH yields MSH as a by-product of ACTH production from POMC |

What adrenal condition would cause this? What is the mechanism?
|
|
|
What are the causes of Addison's disease?
1. 60% = ? 2. 25% = ? 3. 15% = ? |
1. Autoimmune destruction of Adrenal Gland = Autoimmune Adrenalitis
2. Granulomatous Adrenalitis due to TB or Histoplasmosis 3. Other = trauma, metastatic tumor, amyloidosis |
|
|
Tuberculous granulomas
|
What would be the cause of this Addison's diseased adrenal gland?
|
|
|
Autoimmune Adrenalitis
|

What would be the cause of this Addison's diseased adrenal gland?
|
|
|
Addison's Disease due to Autoimmune Adrenalitis
-atrophied cortex with lymphocytic infiltration |

What are these pictures showing?
|
|
|
What are the clinical features of Cushing Syndrome
|
Weight gain = due to hyperinsulinism fom hyperglycemia (due to Cortisol)
-truncal obesity, moon facies, buffalo hump Hypertension = due to increase in weak mineralcorticoids & glucocorticoids = Na+ retention Osteoporosis = due to high cortisol Lymphopenia & Eosinopenia |
|
|
What are the lab findings in Cushing Syndrome?
|
1. increased Cortisol levels
2. increased 17-hydroxycorticoids & Cortisol in urine |
|
|
Cushing Syndrome
|

What syndrome are these clinical findings associated with?
|
|
|
List the causes of Cushing Syndrome
|
Iatrogenic = Corticosteroid therapy
Cushing Disease = ACTH-secreting Pituitary adenoma Adrenal Cortical Adenoma/Carcinoma = decreased ACTH; increased Cortisol Ectopic ACTH = Small Cell Carcinoma of Lung = markedly increased ACTH & Cortisol |
|
|
A 45 yoa woman presents complaining of increased urination over the past several months. She has also gained 35 lbs. over the past year, bruises easily, & has grown hair on her chin. While speaking with her, you note that she has moon facies & increased fat pads on the back of her neck. Blood tests reveal hyperglycemia, increased Cortisol levels, & increased ACTH levels. Dexamethasone suppression test causes decreased Cortisol levels
|
Cushing Syndrome caused by Pituitary Adenoma secreting ACTH
|
|
|
How do you differentiate b/w the different causes of Cushing Syndrome?
|
Pituitary Adenoma
-Cortisol suppression with Dexamethasone suppression test -high ACTH & Cortisol Paraneoplastic Syndrome -markedly high ACTH; high cortisol -no cortisol suppression by Dexamethasone Adrenocortical Adenoma -high Cortisol; low ACTH -No cortisol suppression by Dexamethasone |
|
|
What would 17-alpha-hydroxylase deficiency cause?
|
low Sex hormones & Cortisol
high Mineralcorticosteroids Hypertension, Hypokalemia Phenotypically female but no maturation |
|
|
What would 21-beta-hydroxylase deficiency cause?
|

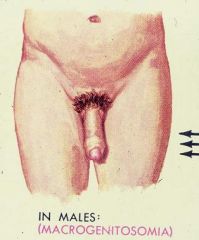
low Cortisol & Mineralcorticoids
high Sex Hormones Masculinization Hypotension Hyperkalemia Salt wasting can lead to Hypovolemia Ambiguous genitalia in females Precocious puberty in males |
|
|
What would 11-beta-hydroxylase deficiency cause?
|

low Cortisol & Aldosterone
high Sex hormones & 11-deoxycorticosterone Hypertension = due to increased 11-deoxycorticosterone Masculinization |
|
|
Congenital Adrenal Hyperplasia due to 21-hydroxylase deficiency
-Clitoral enlargement |

What is the cause of this?
|
|
|
Congenital Adrenal Hyperplasia (21-hydroxylase deficiency)
-Adrenal gland is under constant stimulation by ACTH but only the Reticularis can responds b/c it contains the only cells that do not need 21-hydroxylase to make their product = Sex hormones |
What is the cause of this?
|
|
|
Primary Hyperaldosteronism due to a benign adenoma in the Zona Glomerulosa
|
Conn's Syndrome
|
|
|
What are the clinical features of Conn's Syndrome?
|
-Hypertension = due to Aldosterone causing Na+ retention
-Metabolic Alkalosis & Hypokalemia = due to increase K+ & H+ secretion -Decreased Renin levels -decreased Serum Potassium |
|
|
List the causes of Conn's Syndrome
1. 90% 2. 10& 3. very rare |
1. Cortical Adenoma = Aldosteronoma
2. Nodular Cortical Hyperplasia 3. Adrenocortical Carcinoma |
|
|
Adrenal Cortical Adenoma as seen in Conn's Syndrome = Primary Hyperaldosteronism
|

What is seen here?
|
|
|
Lipid-filled Adrenal Cortical cells in a Benign Adrenal Adenoma = Conn's Syndrome
|
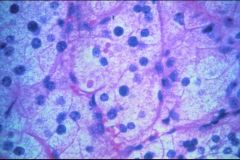
What is seen here?
|
|
|
Describe a Neuroblastoma
|
Small cell malignant neoplasm arising in the Adrenal Medulla
|
|
|
Neuroblastoma:
1. Most common presenting age? 2. How does it present? 3. What are the frequent metastasis sites? 4. Who has a better prognosis? 5. What do the tumor cells secrete? 6. What is increased in the urine? |
1. 1-10 years of age
2. large abdominal mass 3. lungs & marrow 4. pts under 1 year of age 5. Epi or NE 6. VMA |
|
|
Neuroblastoma = malignant tumor of Adrenal Medulla
|

What is seen here?
|
|
|
Neuroblastoma
-small, hyperchromatic malignant cells -"rosettes" Neural Ectoderm |
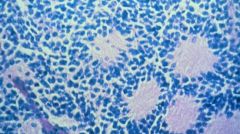
What is this? What is it derived from?
|
|
|
Ganglioneuroma = Neuroblastoma that has reverted to a benign state
|
What is seen here?
|
|
|
What gene is Neuroblastoma associated with?
|
N-myc oncogene
|
|
|
Define Pheochromocytoma
|
Neoplasm of Chromaffin cells of the Adrenal Medulla that produces Catecholamines
|
|
|
Pheochromocytoma
1. peak incidence? 2. what do tumor cells secrete? 3. unilateral or bilateral 4. benign or malignant? |
1. 30-50
2. Epi &/or NE = cause surgically-correctable HTN 3. Unilateral 4. Benign |
|
|
What conditions are Pheochromocytomas associated with?
|
1. Neurofibromatosis
2. MEN II = Medullary Thyroid CA + Pheochromocytoma + Parathyroid Hyperplasia or Adenoma 3. von Hippel-Lindau disease |
|
|
What are the clinical manifestations of Pheochromocytoma?
|
Intermittent attacks of HTN, headache, palpitations
Anxiety Drenching sweats |
|
|
What are the laboratory findings in Pheochromocytomas?
|
increased 24-hour urinary VMA & Metanephrine levels
increased urinary & plasma Catecholamines |
|
|
Pheochromocytoma
-expanded Medullary space in the Adrenal gland |
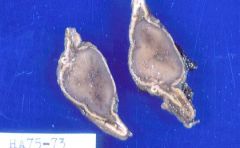
What is seen here?
|
|
|
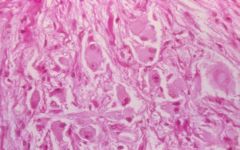
Pheochromocytoma
-nests of polygonal chromaffin cells containing catecholamine-rich granules |
What is this from?
|
|
|
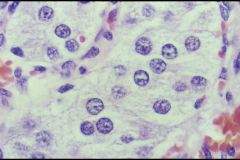
Pheochromocytoma
-secretory granules staining brownish with the chromate stain |
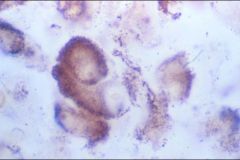
What is seen here?
|
|
|
List the "Rule of 10's" associated with Pheochromocytomas
|
1. 10% occur in children
2. 10% are bilateral 3. 10% occur outside the Adrenal Gland = Paraganglioma 4. 10% are malignant 5. 10% are familial (MEN II & III) |