Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
103 Cards in this Set
- Front
- Back
|
Define "Restrictive Lung Diseases"
|
reduced total lung capacity in the presence of a normal or reduced expiratory flow rate
|
|
|
Define Extrinsic Restrictive lung disease
|
reduced expansion of lung parenchyma and decreased total lung capacity
|
|
|
Define Intrinsic restrictive lung disease
|
involves the space between the epithelial and endothelial basement membranes (interstitium)
|
|
|
Give 4 examples of Extrinsic Restrictive Lung disease (chest wall disorders in the presence of normal lungs)
|
1. Poliomyelitis
2. Severe Obesity 3. Pleural disease (mesothelioma) 4. Kyphoscoliosis = abnormal curvature of the spine in both a coronal and sagittal plane |
|
|
Give an example of an Acute Interstitial Lung disease
|
ARDS
|
|
|
2 synonym names for Usual Interstitial Pneumonia
|
Idiopathic Pulmonary Fibrosis
Cryptogenic Fibrosing Alveolitis |
|
|
What is the most common type of Idiopathic Chronic interstitial pneumonia?
|
Usual Interstitial Pneumonia
|
|
|
Type of onset associated with Usual Interstitial Pneumonia
|
Insidious (slow) = hard to diagnose
|
|
|
Age range and mean age for Usual Interstitial Pneumonia
|
40-70 years old
Mean = 55 years |
|
|
T or F: Usual Interstitial Pneumonia has no gender preference?
|
True
|
|
|
What have been demonstrated in the blood of patients with Usual Interstitial Pneumonia?
|
ANA or Rheumatoid Factor
|
|
|
Explain the pathogenesis of Usual Interstitial Pneumonia
|
-Repeated cycles of Alveolitis triggered by an unknown agent
-Alveolitis -> Fibrosis -> distorted fibrotic lung with Cystic spaces (honeycomb lung) |
|
|
What immune response is associated with Usual Interstitial Pneumonia?
|
Th2
|
|
|
Abnormal activation of Wnt-beta catenin signaling pathway within mesenchymal cells of the fibroproliferative lesions is associated with this Diffuse Interstitial Lung Disease
|
Usual Interstitial Pneumonia
|
|
|
What is the prognosis for UIP?
|
Chronic progressive downhill course
Average survival < 5 years |
|
|
What is the treatment for UIP?
|
Steroids and Cyclophosphamide
|
|
|
What is the mean survival time for UIP?
|
3 years
|
|
|
What are complications of UIP?
|
Chronic lung disease
End stage lung (honeycomb lung) Pulmonary Hypertension |
|
|
How is Non-specific interstitial pneumonitis (NSIP) distinguished from other lung diseases?
|
uniform appearance (in all areas of biopsy) of interstitial inflammation, typically lymphocytes with rare plasma cells
|
|
|
What is Non-specific Interstitial Pneumonitis treated with?
|
Steroids
|
|
|
T or F: UIP has a better prognosis than NSIP
|
False: NSIP has a better prognosis
|
|
|
What do NSIP patients present with?
|
Dyspnea (shortness of breath)
Dry Cough *both of several months duration |
|
|
Cryptogenic Organizing Pneumonia (COP) alternate names
|
Bronchiolitis Obliterans Organizing Pneumonia (BOOP)
Allergic Alveolitis |
|
|
Define Cryptogenic Organizing Pneumonia
|
- Allergic/inflammatory process involving BRONCHIOLES and ALVEOLAR spaces rather than large airways, as opposed to asthma
- Bronchioles eventually become totally fibrotic |
|
|
Describe the pathogenesis of Bronchiolitis Obliterans (COP)
|
Type III hypersensitivity rxn and perhaps a component of Type IV
- Immune complex |
|
|
List 4 occupational hazards associated with Cryptogenic Organizing Pneumonia
|
1. Farmer's lung
2. Sugar cane residue 3. Bird fancier's lung 4. Maple bark stripper's disease |
|
|
What is Farmer's lung due to exposure from?
|
Thermophilic actinomycete spores in moldy hay
-Saccharopolysporia |
|
|
Distinctive type of patchy fibrosis composed of polypoid irregular plugs of fibrous tissue filling bronchioles, alveolar duct, and alveoli
|
Cryptogenic Organizing Pneumonia (COP) (BOOP)
|
|
|
Define Pneumonconioses
|
NON-neoplastic reaction of the lung to inhaled mineral or organic dust
|
|
|
In Pneumonconioses, the reaction in the lung will vary with these 5 things
|
1. properties of the dust
2. size and shape of inspired particles 3. length of exposure 4. individual susceptibility 5. possible additional effects of other irritants |
|
|
What is the most important factor in Pneumonconioses?
|
the capacity of the mineral or dust to stimulate inflammation and fibrosis
|
|
|
What is Coal Worker's Pneumoconiosis caused by?
|
inhalation of coal dust
|
|
|
List the 3 stages of Coal Worker's Pneumonconioses
|
1. Pulmonary Anthracosis
2. Simple CWP 3. Complicated CWP |
|
|
What characterizes CWP Pulmonary Anthracosis?
|
-usually asymptomatic
-anthracotic pigment in interstistial tissue and hilar nodes -alveolar macrophages with anthracotic pigment are called "dust cells" |
|
|
What characterizes Simple CWP?
|
fibrotic opacities are smaller than 1 cm in upper lobes and upper portions of lower lobes
- little to no pulmonary dysfunction |
|
|
What characterizes Complicated CWP?
|
- Fibrotic opacities larger than 2 cm with or without necrotic centers
- Black Lung disease - Compromised lung function |
|
|
What can Complicated CWP lead to?
|
1. Bronchiectasis = abnormally dilated bronchi filled with mucus and N0
2. Pulmonary HTN 3. Cor pulmonale = dilation and hypertrophy of the right side of the heart due to pulmonary HTN |
|
|
What is the most common occupational disease in the world?
|
Silicosis
|
|
|
What is Caplan's Syndrome?
|
- Coexistence of Rheumatoid arthritis with a Pneumoconiosis (CWP)
- characterized by formation of large cavitating rheumatoid nodules in the lungs |
|
|
What is inhaled in Silicosis?
|
Crystalline Silicon dioxide
|
|
|
In what occupations is Silicosis most prevalent?
|
Mine workers
Sandblasters Glass workers |
|
|
Explain the Pathogenesis of Silicosis
|
- quartz is highly fibrogenic and deposits in the UPPER lungs
- quartz activates and is cytolytic to alveolar MO - MO release cytokines that stimulate fibrogenesis |
|
|
What is Silicosis associated with an increased susceptibility to?
|
Tuberculosis
|
|
|
In Asbestosis, where does diffuse pulmonary interstitial fibrosis start first?
|
Lower lobes and subpleurally
|
|
|
In what 2 locations in the world has asbestos been linked?
|
Metsoya area in Greece
Turkey *both related to mineral dust used in white stucco and wall paint |
|
|
Why are the most dangerous asbestos particles 1-5 microns in diameter?
|
b/c they can reach the terminal small airways and air spaces and settle in their linings
|
|
|
What is the most common feature of Asbestos exposure?
|
Pleural plaques
*they do not contain asbestos bodies |
|
|
What are Ferruginous bodies?
|

Asbestos fibers coated with Hemosiderrin and protein from MO
|
|
|
What 2 cancers are associated with Asbestos and which one's risk is increased with smoking?
|
1. Mesothelioma
2. Bronchogenic Carcinoma (Smoking) |
|
|
What does Malignant Mesothelioma arise from?
|
Serosa of the pleura
|
|
|
What is the most common Asbestos-related cancer?
|
Bronchogenic Carcinoma
|
|
|
What are the 2 geometric forms of Asbestos and which is most dangerous?
|
1. Serpentine = curly, flexible
-more prevalent 2. Amphibole = straight, stiff -most dangerous |
|
|
What special stain can be used to identify Asbestos?
|
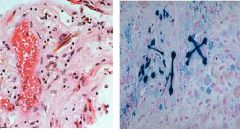
Prussian blue
|
|
|
What are 6 Asbestos-related diseases?
|
1. Pleural plaque
2. Pleural effusions 3. Pulmonary parenchymal interstitial fibrosis (asbestosis) 4. Bronchogenic carcinoma 5. Malignant mesothelioma 6. Laryngeal neoplasms |
|
|
Most common sites for Pleural plaques in Asbestosis
|
1. anterior and posterolateral aspects of the Parietal Pleura
2. domes of the diaphragm |
|
|
In contrast to other inorganic dusts, asbestos can also act as what 2 things?
|
1. tumor initiator
2. tumor promoter *oncogenic effects are mediated by reactive free radicals |
|
|
List 5 groups of drugs associated with Interstitial Fibrosis
|
1. Bleomycin and Bulsufan
2. Amiodarone 3. Cyclophosphamide 4. Methotrexate and Methysergide 5. Nitrosurea and Nitrofurantoin |
|
|
What is the definition of Sarcoidosis?
|
disease of UNKNOWN etiology characterized by NON-CASEATING GRANULOMAS found in many organs and tissues
|
|
|
What is the Clinical presentation of Sarcoidosis in 90% of all cases?
|
-Bilateral hilar lymphadenopathy
-bilateral interstitial infiltrates |
|
|
Sarcoidosis has a 10-fold higher incidence in this group of people
|
Black americans
*higher in females than males |
|
|
What can Sarcoidosis be mistaken for?
|
Tuberculosis
|
|
|
When diagnosing Sarcoidosis, why must you be absolutely sure?
|
b/c treatment is Steroids and if the patient actually has TB, steroids will make it drastically worse
|
|
|
What do you see histologically in Sarcoidosis?
|
-Sarcoid non-caseating granuloma with epithelioid cells and MNGC's
|
|
|
In Sarcoidosis, what are the non-caseating granulomas usually in close proximity to?
|
Bronchioles
|
|
|
What laboratory values are associated with Sarcoidosis? (4)
|
1. increased Angiotensin-converting enzyme (ACE)
2. Hypercalcemia 3. Hypergammaglobulinemia 4. Increased ESR |
|
|
A 24-year-old African-American woman presents with fatigue unchanged by sleep, lack of energy, aches and pains, blurry vision, dry eyes and shortness of breath. A physical exam reveals small cutaneous bumps, uveitis and an enlarged liver by palpation. Other pertinent results were abnormal X-Rays, restrictive lung findings, increased serum angiotensin converting enzyme (ACE), and increased 24-hour calcium excretion. A bronchioloalveolar lavage revealed a CD4/CD8 ratio of >2.5 and a CD3/CD4 ratio of < 0.31.
|
Sarcoidosis
|
|
|
What is the prognosis for Sarcoidosis?
|
-unpredictable clinical course
-overal, 65-70% of patients recover with minimal sequelae |
|
|
Dyspnea, uveitis, enlarged liver, skin lesions
|
Sarcoidosis
|
|
|
What is the most common symptom in Sarcoidosis?
|
Dyspnea
|
|
|
Describe the pathogenesis of Sarcoidosis
|
1. disorder in immune regulation
2. CD4 Th cells interact with an unknown antigen 3. release of cytokines causing formation of noncaseating granulomas |
|
|
A 16-year-old bird owner presents with a history of 1 year of shortness of breath, particularly on exertion, productive cough, fatigue and weight loss. A physical examination revealed an increased respiratory rate, mild cyanosis, but notably there is no clubbing or fever. Chest X-Rays revealed reticular opacities in the upper lobes with reduced lung volumes and honeycombing. Bronchoalveolar labage revealed increased numbers of T lymphocytes, both CD4 and CD8.
|
Hypersensitivity Pneumonitis
|
|
|
Describe the pathogenesis of Hypersensitivity Pneumonitis
|
1. exposure to antigen
2. patient develops IgG Ab's 3. 2nd exposure 4. Ab's combine with inhaled allergens to form immune complexes |
|
|
Explain 2 ways in which Desquamative Interstitial Pneumonia (DIP) is different from UIP
|
1. patients are usually younger (42 vs. 55)
2. most patients respond to Steroid with means survival of 12 years compared to 5 for UIP |
|
|
What does a biopsy show in DIP?
|
- instersitial inflammation
-striking accumulation of intra-alveolar Macrophages |
|
|
What is the final common pathway in all Restrictive Lung diseases?
|
Honeycomb lung
|
|
|
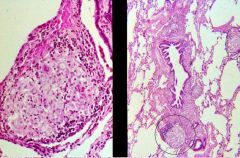
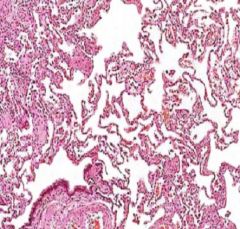
What are the hallmark histologic findings of Usual Interstitial Pneumonia?
|
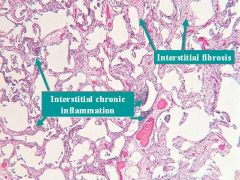
1. Chronic Interstitial INflammation
2. Interstitial Fibrosis |
|
|
Usual Interstitial Pneumonia
|

What is this showing?
|
|
|
A 60-year-old man presented with a 3-year history of cough and progressive dyspnea. His past medical history of was notable only for heavy smoking. He was not taking any drugs and his occupational and family history were unremarkable. One year prior to admission he noted the gradual appearance of dyspnea on exertion, which worsened with time and was associated with a dry cough, but no pain, fever or other systemic symptoms. On physical exam he had an elevated respiratory rate and bi-basilar “velcro” rales. No cyanosis, clubbing or organomegaly. 2 years later he presented with worsening symptoms and clubbing of his fingers.
|
Usual Interstitial Pneumonia
|
|
|
Usual Interstitial Pneumonia
|
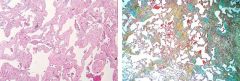
What lung disease?
|
|
|
Usual Interstitial Pneumonia = Idiopathic Pulmonary Fibrosis
|
What lung pathology?
|
|
|
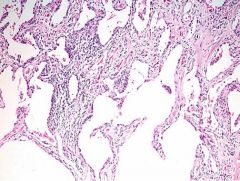
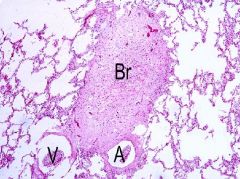
Non-specific Interstitial Pneumonitis
|
This is distinguished from other causes by its uniform appearance of interstitial inflammation
|
|
|
Bronchiolitis Obliterans = Cryptogenic Organizing Pneumonia
|
What is this?
|
|
|
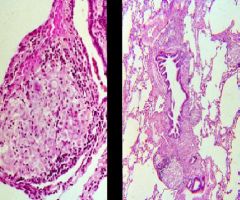
Cryptogenic Organizing Pneumonia = Allergic Alveolitis
-fibrous plugs are seen |

What do these 2 slides show?
|
|
|
Coal Worker's Pneumoconiosis
|
What are these?
|
|
|
Silicosis
Obstruction of airways and blood vessels |
What is this disease?
What can be a complication of these nodules? |
|
|
Asbestos
|

What is this?
|
|
|
Asbestos
|
What is this?
|
|
|
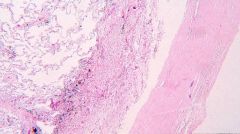
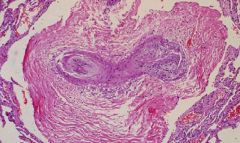
Pleural Plaques
Asbestos |

What are these called?
What is the cause? |
|
|
What type of occupation typically exposes one to Asbestos?
|
Construction -> insulation
|
|
What is this picture showing?
|
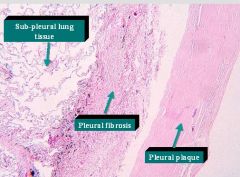
Pleural Plaque caused by Asbestos
|
|
|
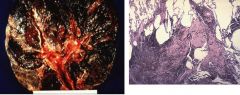
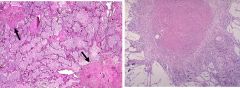
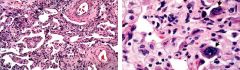
Malignant Mesothelioma caused by Asbestos
|

What is this picture showing?
|
|
|
Mesothelioma caused by Asbestos
|
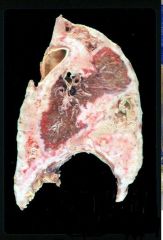
What is this?
|
|
|
Bleomycin
Bulsufan |
What 2 drugs could cause this fibrotic reaction in the lungs?
|
|
|
Multisystem non-caseating granulomatous disease of unknown etiology
-Lung -Liver -Spleen -Eyes -Lymph nodes |
Sarcoidosis
|
|
|
Sarcoidosis
-Bilateral Hilar Lymphadenopathy |

A 32 year old African-American woman presents with malaise, fever, and dyspnea. She also has a nodular rash on all extremities and has been suffering arthalgias in both knees.
|
|
|
Sarcoidosis non-caseating Granulomas
|
These lesion tend to be near Bronchioles
|
|
|
A 25 year old black woman presents with Dyspnea, Hepatosplenomegaly, and erythema nodosum.
Lab values indicate increased ACE activity |
Sarcoidosis
|
|
|
A 40 year old man presented with a cough that began 2 years ago and has progressively gotten worse. He also complains of dyspnea. Histology revealed a striking accumulation of Macrophages in the Alveoli. He was prescribed Steroids and his symptoms subsided.
|
Desquamative Interstitial Pneumonia
|
|
|
Desquamative Interstitial Pneumonia
-Intra-alveolar macrophages |

What is this Lung pathology?
|
|
|
Pulmonary HTN
Cor Pulmonale = Right sided heart failure due to Lung pathology |
What is this?
What could it lead to? |
|
|
End-stage lung = Honeycomb lung
-dilated abnormal airways containing mucinous gray secretions |
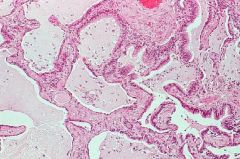
What is this showing?
|
|
|
Chronic condition characterized by the abnormal bilateral enlargement of glands in the head and neck, including those near the ears (parotids) and those around the eyes (lacrimal) and mouth (salivary) due to sarcoidosis
-Parotid, Submaxillary, Sublingual -Lacrimal gland -Salivary |
Mikulicz syndrome
|
|
|
This is characterized by the INSIDIOUS development of FIBROTIC PULMONARY NODULES containing quartz crystals in the UPPER ZONES of the lungs
|
Silicosis
|