Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
32 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
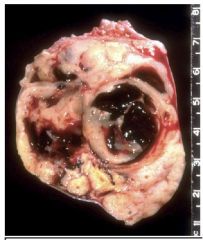
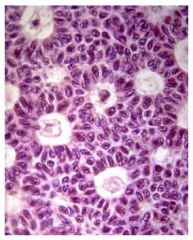
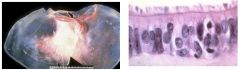
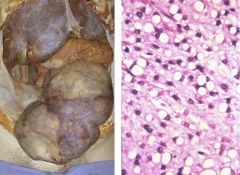
Granulosa Cell Tumor
|
10% malignant, post-menopausal, estrogen producing, result of loss of oocytes, cystic/hemorrhagic, grooved nuclei (Call-Exner bodies), may cause proliferative endometrial lesions
|
|
|
Granulose Cell Tumor
|
10% malignant, post-menopausal, estrogen producing, result of loss of oocytes, cystic/hemorrhagic, grooved nuclei (Call-Exner bodies), may cause proliferative endometrial lesions
|
|
|
Sertoli-Leydig cell tumors
|
produce androges, associated w/ virilization and hirsutism
|
|
|
|
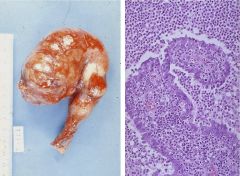
Gonadoblastoma
|
gonadal dysgensis, germ cells & primitive sex cord elements
|
|
|

|
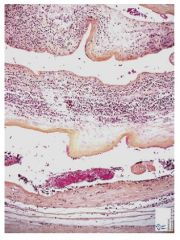
Chorioamnionitis
|
Infection of placental membranes resulting from ascending bacterial infection. Opaque edematous membranes w/ PMN infiltrate
May cause premature labor, fetal infections, intrauterine hypoxia |
|
|
Chorioamnionitis
|
Infection of placental membranes resulting from ascending bacterial infection. Opaque edematous membranes w/ PMN infiltrate
May cause premature labor, fetal infections, intrauterine hypoxia |
|
|
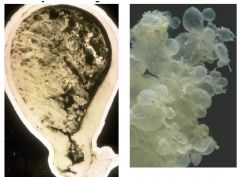
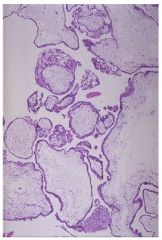
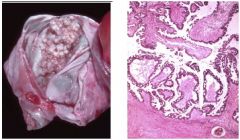
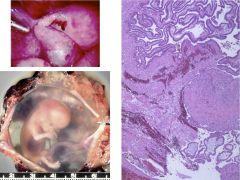
Complete Hydatidiform Mole
|
Fertilization of empty ovum (paternal 46XX), extremes of age & asian predispose. Uterine cavity fills with edematous villi w/ trophoblastic hyperplasia. 2% develop choriocarcinoma
Symptoms: markedly elevated HCG, excessive uterine enlargement, abnormal uterine bleeding |
|
|
Complete Hydatidiform Mole
|
Fertilization of empty ovum (paternal 46XX), extremes of age & asian predispose. Uterine cavity fills with edematous villi w/ trophoblastic hyperplasia. 2% develop choriocarcinoma
Symptoms: markedly elevated HCG, excessive uterine enlargement, abnormal |
|

|
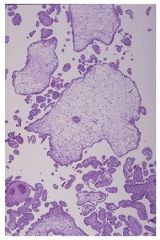
Partial Hydatidiform Mole
|
Fertilization of ovum by 2 sperm or diploid sperm (triploidy). no choriocarcinoma risk. mixture of normal & edematous villi, fetal parts present
|
|
|
partial hydatidiform mole
|
Fertilization of ovum by 2 sperm or diploid sperm (triploidy). no choriocarcinoma risk. mixture of normal & edematous villi, fetal parts present
|
|
|
invasive hydatidiform mole
|
villi invade uterine wall & vessels, may perforate uterus leading to heatogenous spread. difficult to distinguish from choriocarcinoma
|
|
|

|
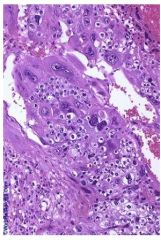
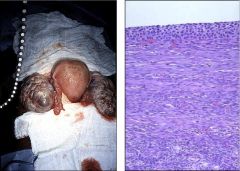
Choriocarcinoma
|
Malignant tumor of trophobloasts, same risk factors as mole. hemorrhagic/necrotic, atypical trophoblasts w/out true villus, METASTASIS, elevated HCG
|
|
|
Choriocarcinoma
|
Malignant tumor of trophobloasts, same risk factors as mole. hemorrhagic/necrotic, atypical trophoblasts w/out true villus, METASTASIS, elevated HCG
|
|

|
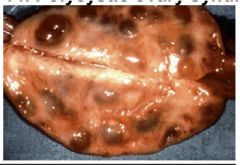
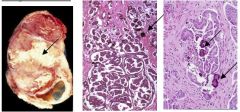
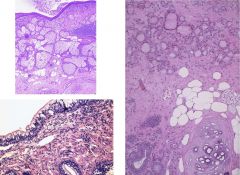
Polycystic Ovarian Syndrome
|
young obese women, increased androgen synthesis (abnormal 17alpha-hydroxylase activity), persistent anovulation, hirsutism, acne, male pattern alopecia, peripheral insulin resistance (disproportionate to degree of obesity), progesterone deficiency. increased estrogen levels may also lead to endometrial hyperplasia & adenocarcinoma.
Microscopically: numerous subcapsular follicular cysts |
|
|
Polycystic Ovarian Syndrome
|
young obese women, increased androgen synthesis (abnormal 17alpha-hydroxylase activity), persistent anovulation, hirsutism, acne, male pattern alopecia, peripheral insulin resistance (disproportionate to degree of obesity), progesterone deficiency. increased estrogen levels may also lead to endometrial hyperplasia & adenocarcinoma.
Microscopically: numerous subcapsular follicular cysts |
|

|
Polycystic Ovarian Syndrome
|
young obese women, increased androgen synthesis (abnormal 17alpha-hydroxylase activity), persistent anovulation, hirsutism, acne, male pattern alopecia, peripheral insulin resistance (disproportionate to degree of obesity), progesterone deficiency. increased estrogen levels may also lead to endometrial hyperplasia & adenocarcinoma.
Microscopically: numerous subcapsular follicular cysts |
|

|
Germ Cell Tumors (Mature cystic teratomas)
|
Similar to testicular tumors, mature cystic teratoma (dermoid cyst), 25% of all ovarian teratomas, occur in younger women or girls, 1% malignant transfomation
|
|
|
Serous Cystadenoma (benign ovarian epithelial cancer)
|
serous or mucinous, unilocular or multilocular. single layer of well-differentiated cliliated columnar epithelium (serous) or mucin producing glandular (mucinous)
|
|
|
Borderline ovarian epithelial cancer
|
serous or mucinous. epithelial atypia & increased mitotic activity. excellent prognosis following surgical removal
|
|
|
Serous adenocarcinoma
|
serous, papillary growth pattern w/ psammoma bodies and frank invasion. mucinous, endometrial, clear cell, & transitional cell types. lymphatic spread, poor prognosis
|
|

|
Mucinous Cystadenoma
|
serous or mucinous, unilocular or multilocular. single layer of well-differentiated cliliated columnar epithelium (serous) or mucin producing glandular (mucinous)
|
|
|
salpingitis
|
inflammation of the fallopian tube, typically due to an ascending infection (N. gonorrhea, E. coli, C. trachomatis, mycoplasma). Acute infection = PMNs. Chronic = plasma cells & lymphocytes, may lead to impaired fertility and/or ectopic pregnancies due to tubular damage. May lead to PID. Blocked tube may cause purulent or serous exudate.
|
|
|
ectopic pregnancy
|
Implantation of fertilized ovum outside the uterus (95% fallopian tubes). tubal wall typically perforated by 12th week, leads to severe intra-abdominal hemorrhage
|
|
|
Ovarian Follicle Cysts
|
Thin walled, <5cm diameter, develop pre-menopause, lined by granulosa cells w/ inner theca cells. Associated w/ precocious puberty, menstrual irregularities, & intraperitoneal bleeding
|
|
|
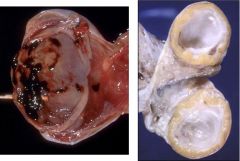
Ovarian Corpus Luteum Cysts
|
yellow wall w/ central hemorrhage, prolonged progesterone synthesis, menstrual irregularities
|
|
|
|
Ovarian Theca Lutein Cysts
|
multiple/bilateral proliferation of theca lutein cells, caused by high HCG levels, intra-abdominal hemorrhage secondary to rupture
|
|

|
Mature Cystic Teratoma
|
25% of ovarian tumors, caused by autofertilization, skin, hair, glands, teeth, often present, 1% malignant
|
|
|
Mature Cystic Teratoma
|
25% of ovarian tumors, caused by autofertilization, skin, hair, glands, teeth, often present, 1% malignant
|
|

|
Fibroma
|
Benigh, whitish, solid, well-differentiated fibroblasts & collagen
Meigs Syndrome = fibroma w/ ascites & pleural effusion |
|

|
Thecoma
|
Benign, post-menopause, estrogen producing, lipid laden theca cells yellowish solid tumor
|
|
|
Metastatic Tumor to the Ovary
|
mimics primary ovarian tumor. most common primary sites: breast, large intestine, endometrium, stomach
Krukenberg tumor - adenocarcinoma w/ signet ring morphology, metastatic to the ovary 75% gastric, 25% colonic |
|
|
epithelial ovarian tumors
|
most common ovarian tumor, result of repeated disruption and repair of surface epithelium (more common in nulliparous women, decreased incidence w/ birth control), increased incidence w/ BRCA-1
Presents as: Cystadenoma (benign), borderline, cystadenocarcinoma (malignant), may show serous, mucinous, endometrioid, clear cell, or transitional cell differentiation |
|