Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
49 Cards in this Set
- Front
- Back
|
Overview of the renal anatomy.
|
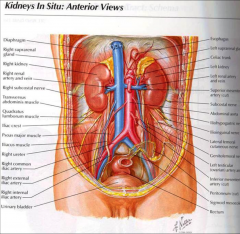
*Paired ovoid organs: both retroperitoneal.
*Right kidney – Anterior is liver, duodenum at hilum, hepatic flexure inferiorly. *Left kidney: spleen is superior and lateral, pancreas at hilum, jejunum inferiorly. *Posterior to both are quadratus lumborum and psoas muscles. *Capping both are the adrenal glands. |
|
|
Review the external anatomy relationship to kidney location.
What do the kidneys weigh? |
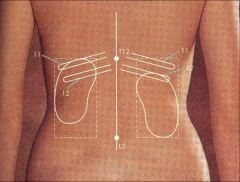
*Male kidney 150 grams; female kidney 135 g.
*More superior on the left. *11th rib on left. *11th interspace on right. *Both are embedded in fat. |
|
|
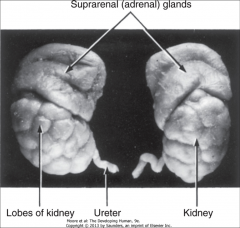
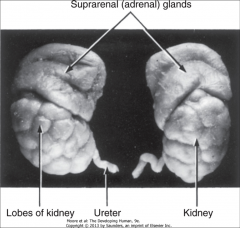
Anatomy of infant and adult kidneys:
|
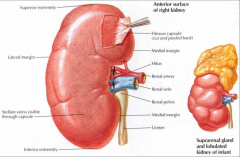
*Infants' are lobular; adrenal is very large.
*Hilus is the medial margin. *Whole thing is surrounded by a fibrous capsule. |
|
|
Longitudinally sectioned anatomy of the kidney:
|
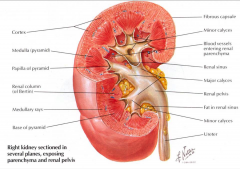
*Outer is cortex; Inner is medulla.
*Medullary pyramids--> papilla *Renal columns are b/t pyramids (collections of tubules). *Renal pelvis is proximal part of ureter. *Calyces feed into the pelvis. *Papilla--> calyx--> pelvis--> ureter. *Renal sinus is normally filled with fatty tissue. |
|
|
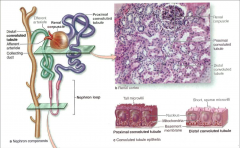
Anatomy of the nephron:
|
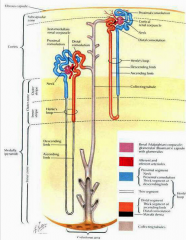
*Two types of nephrons, distinguished by location!
*Renal corpuscle consists of glomerulus and Bowman’s capsule. *PCT, loop of Henle, DCT. *Connecting tubule. *Collecting tubule connects the two 'types' of nephrons, although they don't communicate; they just both empty into the papilla via the same collecting tubule. *JG apparatus consists of wall of afferent arteriole and macula densa of DCT. *Macula densa is key to regulating GFR. |
|
|
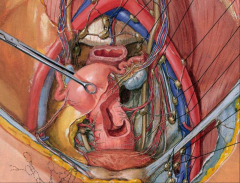
Vascular supply of the kidneys:
|
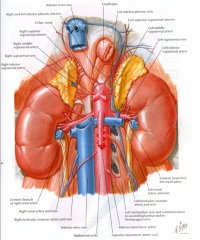
Aorta to left of and slightly posterior to IVC.
Renal arteries arise directly from aorta just below the superior mesenteric artery. RRA longer; passes posterior to IVC, RRV, and head of pancreas. LRA posterior to LRV and body of pancreas. At hilum – order anterior to posterior – vein, artery, renal pelvis. |
|
|
Blood supply TO the kidney:
|
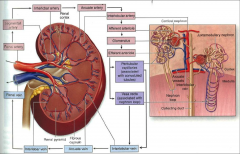
Juxtaglomerular nephrons: Renal artery--> segmental--> interlobar--> arcuate--> interlobular--> afferent arteriole to glomerulus--> efferent arteriole--> peritubular capillary system--> interlobular vein.
Juxtamedullary nephrons: Renal artery--> segmental--> interlobar--> arcuate--> interlobular--> afferent arteriole to glomerulus--> efferent arteriole--> peritubular capillary system AND vasa recta--> interlobular vein. |
|
|
Venous outflow of the kidney:
|
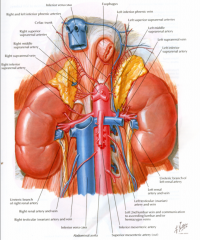
At hilum veins are anterior to arteries.
Left longer than Rt. LRV receives left ovarian or testicular vein and left adrenal vein. On right these veins enter directly into IVC. |
|
|
Anatomy of the ureters:
|
Ureters are retroperitoneal structures. Note close relationship to uterine arteries and veins and parametrium.
|
|
|
How does the ureter get to the bladder?
|
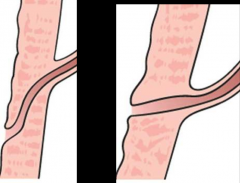
The ureter follows an oblique course through the bladder wall to open in the TRIGONE at a point (in the distended adult bladder) about 5 cm. from the opening of the contralateral ureter. The normal oblique course is NEEDED to prevent VU reflux.
|
|
|
Anatomy of the Renal cortex:
|
*Corpuscle= glomerulus + BC. Space is urinary space.
*Proximal tubules have pinkish cytoplasm. *Distal ones have smaller diameter. |
|
|
RENAL CORPUSCLE anatomy:
|

|
|
|
JUXTAGLOMERULAR APPARATUS anatomy:
|
|
|
|
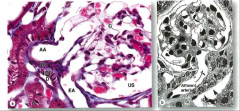
Glomerulus anatomy:
|
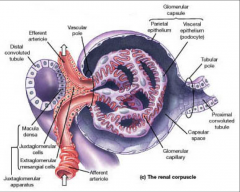
*Afferent arteriole--> glomerular capillary--> efferent arteriole.
*JG cells produce RENIN! *Glomerulus has a VASCULAR pole opposite a TUBULAR pole. |
|
|
Anatomy of GLOMERULAR CAPILLARIES AND PODOCYTE:
|
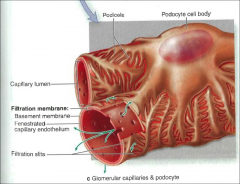
*Note processes of the podocytes (pedicels).
|
|
|
Anatomy of the MESANGIUM:
|
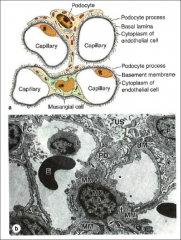
*This is a xs of the glomerular capillaries.
*Podocyte processes are "hairy" looking. *Mesangial cells are structural cells of the glomerulus. |
|
|
Anatomy of the normal GLOMERULAR FILTRATION BARRIER:
|

*Note hairy looking foot processes.
*Proteinuria and "minimal change disease" will lead to fusion of the processes! *Bottom pic: lower portion is a capillary lumen. Cytoplasm of an endothelial cell is to the left of the arrowhead. Gap indicated by arrowhead is a fenestrae. Basal lamina looks quite dense. Note foot processes. *Filtration slit and "slit diaphragm" indicated by arrow. |
|
|
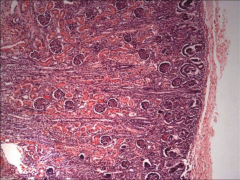
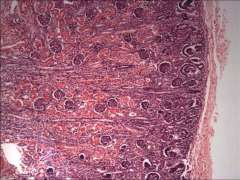
Histology of normal RENAL CORTEX:
|
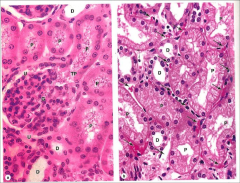
*TP = tubular pole.
*Arrow points to a capillary b/t cells. |
|
|
Histology of normal RENAL MEDULLA:
|
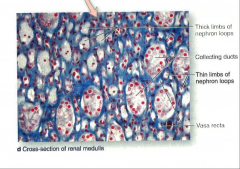
*CDs, thin and thick loops. Identifying specific components isn't terribly important.
|
|
|
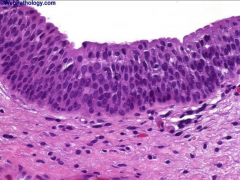
Histology of URETERS:
|

*Transitional epithelium here.
|
|
|
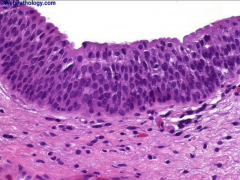
Ureter. Transitional epithelium lines all of the urinary tract from the calyces to the distal urethra.
|
|
|
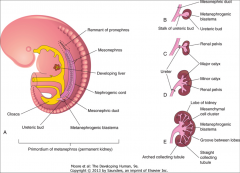
Describe Renal Embryology-- the pronephros and the mesonephros:
|

1) Pronephros:
-Appears in early 4th week. -Transient and NON-functional. 2) Mesonephros: -Appears in late 4th week. -Connects to mesonephric (Wolffian) duct (originally pronephric ducts). -Ducts open into CLOACA. -Functions for a SHORT time. *Paramesonephric ducts = Mullerian ducts (female). *Mesonephric ducts= Wolffian ducts (male). |
|
|
Describe Renal Embryology-- the metanephros:
|
*Metanephros: the definitive kidney!
*Begins to develop in the 5th week. *Functions in the early fetal period. *Formation of permanent kidney requires contact b/t the ureteric bud and the metanephric mesoderm. |
|
|
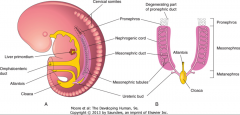
What does the kidney system look like during the 5th week of development?
|
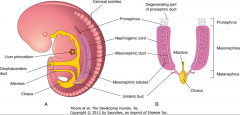
*Pro- and meta- are still there.
*Metanephros just getting started. *Cloaca in place. |
|
|
Describe the DEVELOPMENT OF the MESONEPHROS between the 5th - 11th WEEKS:
|
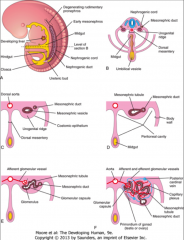
*Note that the mesonephros, while only functional for a short time, has its own system of glomeruli and ducts.
|
|
|
Describe the DEVELOPMENT OF the PERMANENT KIDNEY between the 5th and 8th WEEKS:
|
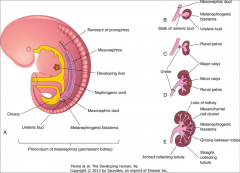
B: Ureteric bud interacts with metanephrogenic blastema.
*Kidney "proper" is derived from metanephrogenic blastema. *The system of ducts/tubules is actually developed from the outpouching of the mesonephric duct. |
|
|
Discuss the Ureteric Bud:
|
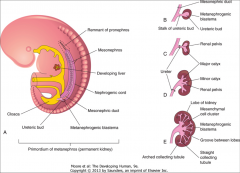
*A.k.a. metanephric diverticulum.
*Arises from Wolffian duct, near the entry into the cloaca. *The ureteric bud acts as the primordium of the ureter, renal pelvis, calyces, and collecting tubules. |
|
|
Discuss the Metanephric Mesoderm:
AKA? |
*A.k.a. metanephrogenic blastema.
*Derived from the nephrogenic cord in the urogenital ridge. *Will form nephrons. *Forms the Wilms Tumor! |
|
|
What are some pathologies of the Ureteric Bud and Metanephric Mesoderm?
|
*Absence of one or both or failure to meet and properly interact results in renal AGENESIS.
*Incomplete or aberrant juxtaposition and/or interaction results in renal dysplasia with or without cysts. |
|
|
How do the ureteric bud and metanephric mesoderm interact?
|
*Ureteric bud is induced to undergo tree-like branching giving rise to ureter, pelvis, calyces and collecting tubules.
*Cells of the metanephrogenic blastema are induced to take on a stem cell phenotype. |
|
|
What do nephrons arise from?
What do CTs arise from? |
*Nephrons from metanephric mesoderm.
*CTs from ureteric bud which is derived from the mesonephric duct. |
|
|
Describe the development of nephrons:
|
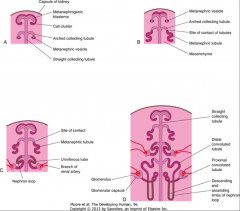
*Branches of the renal artery form glomeruli.
*There's more activity occurring toward the medulla than there is toward the cortex. |
|
|
How does the Formation of nephrons occur?
|
*The stem cells of the innermost portion are the first to undertake glomerular formation and tubular formation.
*As they mature the next outermost layer goes to work, etc. *Mesenchymal cells become mature epithelial cells of the tubules by gaining a basement membrane, cell-cell junctions, and cellular apico-basal polarity. |
|
|
When is the formation of nephrons complete?
|
*During embryonal and fetal life the formation of additional nephrons continues until about the 35th week of gestation in a standard fashion that allows rough DATING of gestation on the basis of the NUMBER of LAYERS seen microscopically in renal sections.
*When the process is complete there is usually NO RESIDUAL metanephrogenic blastema remaining in the kidney. |
|
|
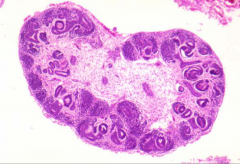
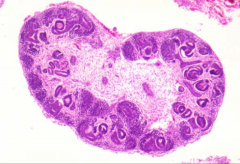
*A kidney at 6-7 weeks. Some early tubular structures.
*The really dark cells clustered in the outer layer are the metanephrogenic blastema. They will ultimately form the proximal and convoluted tubules. |
|
|
*Kidney at 27 weeks.
*Cortex is to the right; medulla to left. You can see primitive tubules and nephrogenic activity in the cortex region. |
|
|
Describe the ROTATION AND RELOCATION OF the KIDNEYS. When does it occur?
|

*Occurs in weeks 6-9.
*They begin development low and move up. |
|
|
*Kidney at 28 weeks. Note the lobules; they define the locations of renal pyramids.
|
|
|
What are the Derivatives of Mesonephric Tubules in males and females?
|
*In Male: Efferent ductules of testis.
*In Female: Tubules of epoophoron and paroophoron. |
|
|
List the Derivatives of the Wolffian (Mesonephric) Duct:
5 in males. Females? 2 |
*In Males:
-Epididymis -Vas deferens -Seminal vesicle -Ejaculatory ducts -Appendix epididymis (can undergo torsion) *Only vestigial structures in females: -Gartner’s duct -longitudinal duct of epoophoron |
|
|
List the Derivatives of the Müllerian (Paramesonephric) Duct:
Females? 3 Males? 2 |
*In Females:
-Fallopian tubes and hydatids of Morgagni -Uterus -Upper vagina *Only vestigial structures in males: -Appendix testis -Prostatic utricle |
|
|
What is the Cloaca?
What does it become? In males and females? |

*The urorectal septum divides the cloaca into ventral and dorsal portions.
*The dorsal portion (hindgut) becomes the rectum and part of anal canal. *The ventral portion is the UG sinus which forms bladder and urethra in both sexes, prostate in male, and vagina in female. |
|
|
How does the urinary bladder develop?
|

*Note the allantois and the cloaca.
*The bladder, urethra, prostate, and bulbourethral glands form from the UG sinus. *The distal portion of the mesonephric duct which is now part of the vas deferens enters the prostatic urethra. *The seminal vesicle is an outpouching from the vas deferens. *The caudal portion of the ureteric bud (now the distal portion of the ureter) loses connection with the mesonephric duct and enters the bladder directly through a process of wall incorporation. *Faulty development of the entry into the bladder leads to vesicoureteral reflux. |
|
|
What does the UG sinus give rise to?
|
The bladder, urethra, prostate, and bulbourethral glands form from the UG sinus.
|
|
|
Where does the bladder's epithelium come from?
What pathology can result if something goes wrong? |
*Bladder epithelium is derived from endoderm of the UG sinus.
*There is caudal migration of mesoderm from the umbilical region to form the anterior abdominal wall. *Deficiencies of such migration will cause bladder exstrophy. |
|
|
Immunologic diseases affect the _____.
Toxic and infectious diseases affect the ____ and ____. |
*Immunologic diseases usually affect glomeruli.
*Toxic and infectious agents usually affect tubules and interstitium. *End result of severe disease starting in any unit is destruction of all units--> end-stage kidney. |
|
|
What do the renal pelvis, ureters, and the bladder all have in common? What's a pathologic implication of this?
|
*Epithelium is the same as that of bladder and is subject to the same TUMORS and INFECTIONS.
|
|
|
How does pathological diagnosis of renal disease happen?
|
*Clinical pathology .
*Cytopathology. *Anatomical pathology: 1) Biopsy; needle or open 2) Nephrectomy 3) Autopsy |
|
|
What are some Special Stains and Techniques used to see the kidney in pathology?
|
*Periodic acid Schiff (PAS) stains mesangium, GBM, TBM pink.
*Silver impregnation stains GBM and TBM black. *Trichrome and lipid stains. *Other special stains for fibrin and amyloid. *Especially important to see the BASEMENT MEMBRANE! *Immunofluorescence and immuno-peroxidase for immunoglobulins, antigens, and complement. *Electron microscopy for ultrastructure of glomerulus including immune complex deposits. |