Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
217 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
What is a double uterus with a double vagina
|
A congenital anomaly that results from the complete lack of fusion of the paramesonephric ducts and the sinovaginal bulbs
|
|
|
|
A 32 year old female presents for evaluation of infertility. Imaging studies reveal a uterus with two horns entering a common vagina. What is this condition called
|
Bicornuate uterus, the most common congenital uterine anomaly
|
|
|
|
What is the defect that results in a bicornuate nucleus
|
The partial fusion of the paramesonephric ducts
|
|
|
|
What is a bicornuate uterus with a rudimentary horn
|
A condition that develops due to the retarded growth of one of the paramesonephric ducts and results in a uterus with one normal and one abnormal horn
|
|
|
|
What defect results in the absence of the uterus or vagina
|
The failure of the paramesonephric ducts and the sinovaginal bulbs to develop
|
|
|
|
What is atresia of the vagina
|
A condition where the vaginal lumen is blocked due to failure of the vaginal plate to canalize and form a lumen
|
|
|
|
What is an imperforate hymen
|
A condition resulting when only the inferior part of the vaginal plate fails to canalize
|
|
|
|
What is gonadal dysgenesis
|
A condition that occurs when the primordial germ cells migrate into the gonad but later degenerate
|
|
|
|
What causes gonadal dysgenesis
|
Chromosomal abnormalities
|
|
|
|
A 16 year old femal presents to your clinic concerned about her lack of menstruation and breast development. Upon examination, you notice that she possesses infantile secondary sexual characteristics and has a webbed neck. What condition is this patient likely to have
|
Turner’s syndrome
|
|
|
|
What is a Bartholin cyst
|
A fluid-filled cyst resulting from an inflammatory obstruction of the Bartholin duct
|
|
|
|
What is lichen sclerosus
|
A benign, chronic inflammatory dermatosis of the vulva that results in a white, patch-like lesions with epidermal atrophy
|
None
|
|
|
What are the clinical characteristics of lichen sclerosus
|
Pruritus and leukoplakia
|
|
|
|
What is a papillary hidradenoma
|
A benign tumor arising from modified apocrine sweat glands that presents as a sharply circumscribed nodule
|
|
|
|
How do you treat papillary hidradenoma
|
Surgical excision
|
|
|
|
What is condyloma acuminatum
|
A wart-like, verrucous lesion that can occur on the vulva, perineum, vagina, and cervix
|
|
|
|
What causes condyloma acuminatum
|
HPV infection, frequently types 6 and 11
|
|
|
|
What is the key histological feature of condyloma acuminatum
|
Koilocytosis (expanded epithelial cells with perinuclear clearing)
|
|
|
|
What is the most common malignant tumor of the vulva
|
Squamous cell carcinoma
|
|
|
|
What usually precedes squamous cell carcinoma of the vulva
|
Vulvar dystrophy and premalignant changes graded as vulvar intraepithelial neoplasia (VIN) 1-3
|
|
|
|
What are the HPV types associated with squamous cell carcinoma
|
HPV types 16, 18, 31, or 33
|
|
|
|
What is extramammary Paget’s disease
|
A condition similar to Paget’s disease of the breast characterized by inflammatory, eczema-like changes affecting the epidermis of the genital or perianal skin and other cutaneous sites
|
|
|
|
What condition is often associated with extramammary Paget’s disease
|
Adenocarcinoma of the apocrine sweat glands
|
|
|
|
What skin malignancy may occur on the vulva
|
Malignant melanoma
|
|
|
|
What is candidiasis
|
The most common form of vaginitis, caused by Candida albicans
|
|
|
|
What conditions are frequently associated with candidiasis
|
Diabetes mellitus, pregnancy, broad-spectrum antibiotic therapy, oral contraceptive use, and immunosuppression
|
|
|
|
How does candidiasis typically present
|
With a thick, white discharge and vulvovaginal pruritis
|
|
|
|
What is trichomoniasis
|
A sexually transmitted type of vaginitis caused by Trichomonas vaginalis
|
None
|
|
|
What is bacterial vaginosis
|
An infection caused by excessive growth of bacteria that are normally present in the vagina
|
|
|
|
What do you characteristically find on a smear preparation of a patient with bacterial vaginosis
|
Clue cells
|
|
|
|
What is toxic shock syndrome
|
A syndrome that occurs secondary to exotoxin release by Staph aureus
|
|
|
|
What is the clinical presentation of toxic shock syndrome
|
Fever, diarrhea, nausea, diffuse erythema, and shock
|
|
|
|
What are the extragenital infections associated with gonorrhea
|
Pharyngitis, proctitis, purulent arthritis, and in the newborn, ophthalmia neonatorum
|
|
|
|
What is the most common sexually transmitted disease
|
Chlamydia trachomatis infection
|
|
|
|
What is a serious sequela of untreated chlamydial infection
|
Pelvic inflammatory disease with the potential for infertility
|
None
|
|
|
What is lymphogranuloma venereum
|
A sexually transmitted disease caused by C. trachomatis L1, L2, or L3 serotypes
|
|
|
|
What is the clinical presentation of lymphogranuloma venereum
|
Genital lesion with swelling of the lymph nodes in the groin
|
|
|
|
Which of the herpes simplex viruses is associated with genital herpes and spreads via sexual contact
|
Herpes simplex virus type 2
|
|
|
|
What is the key cytologic feature of HSV infections
|
Multinucleate giant cells with viral inclusions
|
|
|
|
What are the key features of the three stages of syphilis
|
Primary syphilis—chancre formation
Secondary syphilis—rash (75-100%), lymphadenopathy (50-85%), condyloma lata (10-20%) Tertiary symphilis—gumma formation in any tissue and neurosyphilis |
None
|
|
|
What is chancroid
|
A sexually transmitted disease caused by Haemophilus ducreyi that is characterized by painful, ulcerated lesions
|
|
|
|
What is granuloma inguinale
|
A sexually transmitted infection caused by Donovania granulomatosis, a gram-negative rod
|
None
|
|
|
What is the key histopathologic feature of granuloma inguinale
|
The presence of Donovan bodies, or large histiocytes containing multiple organisms
|
|
|
|
Though primary carcinoma of the vagina is rare, what is the most common type of neoplasm affecting the vagina
|
Squamous cell carcinoma
|
|
|
|
What is vaginal adenosis
|
A benign condition characterized by the overgrowth of glandular-type cells in areas normally lined by stratified squamous epithelium
|
|
|
|
Vaginal adenosis can be a precursor to what condition
|
Clear cell adenocarcinoma
|
|
|
|
If a female patient tells you that her mother was given diethylstilbestrol (DES) therapy while she was pregnant, what condition is this patient at risk for
|
Clear cell adenocarcinoma of the vagina
|
|
|
|
What is sarcoma botryoides of the genital tract
|
A rare variant of rhabdomyosarcoma that occurs in children under the age of 5
|
|
|
|
How does sarcoma botryoides typically present
|
It presents as a polypoid mass resembling a bunch of grapes that projects into the vagina and often protrudes from the vulva
|
|
|
|
Define cervicitis
|
An inflammation of the cervix caused by a number of different organisms including staphylococci, enterococci, Garnerella vaginalis, Candida albicans, Trichomonas vaginalis, Chlamydia trachomatis, and Niesseria gonorrhoeae
|
|
|
|
What are the symptoms of cervicitis
|
Vaginal discharge, bleeding, itching/ irritation of the external genitalia, pain during intercourse, and lower back pain
|
|
|
|
How is cervicitis diagnosed
|
A Pap smear and culture for causative organisms is performed
|
|
|
|
What is the treatment for cervicitis
|
It depends on the causative organism, but initially involves broad-spectrum antibiotics
|
|
|
|
What are cervical polyps
|
Inflammatory proliferations of the cervical mucosa not associated with malignancy
|
|
|
|
What is cervical dysplasia
|
Disordered epithelial growth marked by the loss of polarity and nuclear hyperchromasia
|
|
|
|
Can cervical dysplasia lead to cancer
|
Cervical dysplasia can progress to carcinoma in situ or invasive cancer. The different stages of progression are classified as cervical intraepithelial neoplasia (CIN) 1,2 and 3
|
|
|
|
What is carcinoma in situ
|
It is synonymous with CIN 3 and involves dysplastic changes extending through the entire thickness of the epithelium but not invading the basement membrane
|
|
|
|
What are the most common types of cervical cancer
|
Squamous cell cancer (arising from the ectocervix) and adenocarcinoma (arising from the endocervix)
|
|
|
|
What are the epidemiologic risk factors for invasive cervical cancer
|
Early sexual activity
Multiple sexual partners Being economically deprived Cigarette smoking |
None
|
|
|
HPV DNA sequences are often integrated into the genome of dysplastic or malignant cervical epithelial cells. What is the molecular mechanism associated with this process
|
HPV viral proteins E6 and E7 bind and inactivate the gene products of p53 and Rb, both tumor suppressor genes, thus allowing the cells to accumulate DNA damage
|
|
|
|
What is endometritis
|
Inflammation of the endometrium secondary to intrauterine trauma from instrumentation, intrauterine devices, or complications of pregnancy
|
|
|
|
What bacteria are most often associated with endometritis
|
Staphylococcus and streptococcus species
|
|
|
|
What is endometriosis
|
A nonneoplastic condition caused by the ectopic dissemination of endometrial tissue to the ovaries or other structures outside the uterus
|
|
|
|
What are the ectopic endometrial foci sensitive to
|
Hormonal variations in the menstrual cycle
|
|
|
|
What are chocolate cysts
|
Blood-filled cysts in the ovaries that occur because of menstrual-type bleeding into ectopic endometrium
|
|
|
|
What is often associated with endometriosis
|
Infertility and painful menstrual periods
|
|
|
|
What is adenomyosis
|
A condition characterized by the extension of endometrial tissue into the myometrium
|
|
|
|
What causes endometrial hyperplasia
|
Excess estrogen stimulation caused by anovulatory cycles, polycystic ovarian syndrome, estrogen-secreting ovarian tumors, and estrogen replacement therapy
|
|
|
|
A woman in her late forties comes to the clinic complaining of prolonged uterine bleeding. What is a reasonable diagnosis to consider in this patient
|
Endometrial polyps
|
|
|
|
What are endometrial polyps
|
Small, sessile projections of the endometrium that are composed of edematous stroma and cystically dilated glands
|
None
|
|
|
What is a leiomyoma
|
The most common, benign smooth muscle tumor of the uterine wall
|
|
|
|
Leiomyomas are usually estrogen sensitive. Would you expect tumor size to vary throughout a woman’s lifetime
|
Yes, tumor size would be expected to increase during pregnancy and decrease during menopause
|
|
|
|
What is the most common complaint of women with leiomyomas
|
Menorrhagia or increased menstrual bleeding
|
|
|
|
Do leiomyomas commonly transform into malignant neoplasms (leiomyosarcomas)
|
No, leiomyosarcomas typically arise de novo and are almost never caused by malignant transformation of a leiomyoma
|
|
|
|
Leiomyosarcomas are malignant tumors that occur infrequently. What population has an increased incidence of this type of tumor
|
African-American females
|
|
|
|
Describe the gross morphologic characteristics of a leiomyosarcoma
|
It is a bulky, malignant smooth muscle tumor with areas of necrosis and hemorrhage
|
|
|
|
What are the conditions that predispose a woman to endometrial carcinoma
|
Nulliparity
Age Prolonged estrogen stimulation Systemic conditions such as obesity, diabetes, and hypertension |
None
|
|
|
Why is obesity associated with endometrial cancer
|
Estrone can be synthesized in peripheral adipose tissue causing prolonged estrogen stimulation which is a strong risk factor for endometrial cancer
|
|
|
|
What is salpingitis
|
Inflammation of the fallopian tubes secondary to infection, trauma, or surgical manipulation
|
|
|
|
Salpingitis can result from infections caused by what organisms
|
N. gonorrhoeae, C trachomatis, various anaerobic bacteria, and other pyogenic organisms (Staphylococcus and Streptococcus)
|
|
|
|
What are common complications of salpingitis
|
Pyosalpinx (tube filled with pus), hydrosalpinx (tube filled with watery fluid), and tubo-ovarian abscess
|
|
|
|
What are two common tumors of the fallopian tubes
|
Adenomatoid tumor (benign) and adenocarcinoma (direct extension or metastasis)
|
|
|
|
What causes follicular cysts
|
Distension of an unruptured graafian follicle
|
|
|
|
What are follicular cysts associated with
|
Hyperestrinism and endometrial hyperplasia
|
|
|
|
What causes corpus luteum cysts
|
Hemorrhage into a persistent mature corpus luteum
|
|
|
|
A patient with a corpus luteum cyst would present with what sign and symptom
|
Menstrual irregularity
|
|
|
|
What causes a theca-lutein cyst
|
Gonadotropin stimulation
|
|
|
|
What causes polycystic ovarian syndrome (PCOS)
|
Poor regulation of a variety of enzymes involved in androgen biosynthesis, insulin resistance, excess luteinizing hormone, and androgens
|
|
|
|
What are the clinical characteristics of polycystic ovarian syndrome
|
Amenorrhea, infertility, obesity, and hirsutism
|
|
|
|
Women who present with PCOS are at an increased risk of developing what disease
|
Type II diabetes mellitus due to increased insulin resistance
|
|
|
|
How is PCOS described morphologically
|
Enlarged ovary with thickened ovarian capsule
Multiple small follicular cysts Cortical stromal fibrosis |
None
|
|
|
Ovarian tumors are classified into various categories based on what feature determined by the WHO
|
Cell of tumor origin
|
|
|
|
Ovarian tumors of surface epithelial origin include what types of tumors
|
Serous tumors
Mucinous tumors Endometroid tumors Clear cell tumors Brenner tumors |
None
|
|
|
What is a serous cystadenoma
|
A benign cystic tumor lined with fallopian tube-like epithelium (frequently bilateral)
|
|
|
|
What is a serous cystadenocarcinoma
|
An aggressive, epithelium-lined cystic neoplasm filled with serous fluid that accounts for approximately 50% of all ovarian carcinomas (frequently bilateral)
|
|
|
|
What is a mucinous cystadenoma
|
A benign tumor characterized by multilocular cysts lined by mucus-secreting epithelium
|
|
|
|
What is a mucinous cystadenocarcinoma
|
Malignant tumor that can cause intraperitoneal accumulation of mucinous material (pseudomyxoma peritonei)
|
None
|
|
|
What is a Brenner tumor
|
A benign tumor of transition epithelium
|
|
|
|
Tumors of germ cell origin typically occur in what age group
|
Women younger than 20 years of age
|
None
|
|
|
What is a dysgerminoma
|
The most common malignant germ cell ovarian neoplasm
|
|
|
|
A dysgerminoma is homologous to what testicular germ cell tumor
|
Testicular seminoma
|
|
|
|
Yolk sac (endodermal sinus) tumors of the ovaries are homologous to yolk sac tumors of the testes. What tumor marker is typically found in serum
|
Alpha-fetoprotein
|
|
|
|
Ovarian choriocarcinoma is a highly malignant tumor that is associated with what tumor marker
|
hCG
|
|
|
|
What is the difference between immature and mature teratomas
|
Immature teratomas are typically malignant, while mature teratomas (dermoid cysts) are usually benign
|
|
|
|
What is a struma ovarii tumor
|
A teratoma containing thyroid tissue as the predominant tissue type
|
|
|
|
Tumors of ovarian sex-cord-stromal origin include what tumors
|
Thecoma-fibroma group tumors, granulosa cell tumors, and Sertoli-Leydig cell tumors
|
None
|
|
|
What is an ovarian fibroma
|
A solid tumor consisting of bundles of spindle-shaped fibroblasts
|
None
|
|
|
What is Meigs’ syndrome
|
A syndrome characterized by the triad of ovarian fibroma, ascites, and hydrothorax
|
|
|
|
What are thecomas
|
Solid tumors of spindle-shaped fibroblasts with round, lipid-containing cells
|
|
|
|
What are granulosa cell tumors
|
Estrogen-secreting tumors that often cause precocious puberty in children and are associated with endometrial hyperplasia/ carcinoma in adults
|
None
|
|
|
What is pathognomonic of granulosa cell tumors
|
Call-Exner bodies
|
|
|
|
What are Call-Exner bodies
|
Small spaces filled with eosinophilic fluid and basement membrane material between granulosa cells in both maturing ovarian follicles and ovarian tumors of granulosal origin
|
None
|
|
|
What are Sertoli-Leydig cell tumors
|
Androgen-secreting tumors associated with masculinization
|
|
|
|
Where are the primary tumors that metastasize to the ovaries usually located?
|
Gastrointestinal tract, breast, and endometrium
|
|
|
|
What are Krukenberg’s tumors
|
Bilateral tumors of the ovaries characterized by mucin-secreting signet-ring cells from gastric (or other gastrointestinal) adenocarcinoma metastases
|
|
|
|
What is a placental abruption (abruption placentae)
|
The premature detachment of the placenta from the wall of the uterus causing severe antepartum bleeding and potentially fetal death
|
|
|
|
What is a risk factor for placental abruption
|
Cocaine use
|
|
|
|
What condition is associated with placental abruption
|
DIC
|
|
|
|
What is a placenta accrete
|
The abnormal attachement of the placenta directly into the myometrium due to a defective decidual layer
|
|
|
|
What conditions typically predispose to a placenta accrete
|
Prior cesarean section and endometrial inflammation
|
None
|
|
|
What will you see after delivery of a baby in a patient with placenta accrete
|
Massive hemorrhage
|
|
|
|
What is a placenta previa
|
The abnormal attachment of the placenta to the lower part of the uterus, partially or completely covering the cervical os
|
|
|
|
How does placenta previa usually present
|
Painless bleeding in any trimester
|
|
|
|
A 12 week G1P0 female with a history of pelvic inflammatory disease presents to the ER with severe lower abdominal pain. US fails to reveal an intrauterine pregnancy. There is no history of bleeding. Diagnosis?
|
Ectopic pregnancy, most often in the fallopian tubes
|
|
|
|
How can you verify that an ectopic pregnancy is present
|
Check serial hCG levels which should increase if the patient is pregnant
|
|
|
|
What are the complications of an ectopic pregnancy
|
Hemosalpinx and tubal rupture
|
|
|
|
What is preeclampsia
|
A condition that develops after the 20th gestational week and is characterized by increased blood pressure, proteinuria, and edema
|
|
|
|
What is the definitive treatment of preeclampsia
|
Delivery of the fetus as soon as viable
|
|
|
|
What is HELLP syndrome
|
A condition that is often associated with preeclampsia and includes Hemolysis, Elevated LFTs, and Low Platelets
|
|
|
|
What are the clinical features of preeclampsia
|
Headache, blurred vision, abdominal pain, edema of the face and extremities, altered mental status, and hyperreflexia
|
|
|
|
What are common lab findings in preeclampsia
|
Thrombocytopenia and hyperuricemia
|
|
|
|
What is eclampsia
|
A severe form of pregnancy-induced hypertension resulting in seizures
|
|
|
|
How do you treat eclampsia
|
It is a medical emergency that requires IV magnesium sulfate and diazepam
|
|
|
|
A 16 week G2P1 female presents to the ER with high blood pressure, proteinuria, and edema. Diagnosis?
|
Hydatidiform mole. Preeclamptic symptoms prior to 20 weeks should raise your index of suspicion
|
|
|
|
What is a hydatidiform mole
|
A pathologic ovum that results in the cystic swelling of chorionic villi and proliferation of chorionic epithelium
|
|
|
|
What are the genotypes of complete hydatidiform moles and partial hydatidiform moles
|
The genotype of a complete mole is 46, XX and is completely paternal (no associated fetus). The genotype of a partial mole is triploid or tetraploid and may contain fetal parts
|
|
|
|
What tumor marker do hydatidiform moles secrete
|
hCG
|
|
|
|
Hydatidiform moles are precursors of what cancer
|
Choriocarcinoma of the endometrium
|
|
|
|
What is choriocarcinoma
|
A highly malignant neoplasm that arises from the cells in the chorion layer of the placenta. It is typically composed of both cytotrophoblastic and syncytiotrophoblastic elements
|
|
|
|
What is fibrocystic change/ disease of the breast
|
The most common disorder of the breast characterized by multifocal fibrosis and cyst formation. It is a painful condition common to patients between the ages of 25 and 50 years
|
|
|
|
What are the various histologic types of fibrocystic breast disease
|
Fibrotic—hyperplasia of breast stroma
Cystic—fluid filled Sclerosing—increased acini and intralobular fibrosis Hyperplastic—usually with atypia, increased risk of cancer |
None
|
|
|
What is a fibroadenoma
|
A benign breast tumor of the intralobular stroma that presents as a firm, rubbery, painless well-circumscribed lesion
|
|
|
|
What is a phyllodes tumor
|
A large, bulky tumor of variable malignancy that is found in the connective tissue of the breast
|
|
|
|
What is the typical presentation of an adenoma of the breast
|
It presents with serous or bloody discharge and a palpable mass
|
|
|
|
What is an intraductal papilloma
|
A benign tumor of the major lactiferous ducts
|
|
|
|
Where do most breast lesions occur
|
Upper outer quadrant of the breast
|
|
|
|
Who typically gets breast cancer
|
Mostly postmenopausal women and women predisposed by age, positive family history, personal history of breast cancer, early menarche or last menopause, obesity, nulliparity, first pregnancy after age 30, proliferative fibrocystic disease with atypical hyperplasia, and high animal fat diet
|
None
|
|
|
Describe the histology of breast cancer: Ductal carcinoma-in-situ
|
No basement membrane penetration
|
None
|
|
|
Describe the histology of breast cancer: Invasive ductal carcinoma
|
Firm, fibrous, infiltrating mass
|
None
|
|
|
Describe the histology of breast cancer: Comedocarcinoma
|
Intraductal carcinoma with central necrosis
|
None
|
|
|
Describe the histology of breast cancer: Inflammatory
|
Lymphatic involvement (poor prognosis)
|
None
|
|
|
Desribe the histology of breast cancer: Lobular-in-situ
|
May precede invasive cancer of either breast; often multifocal
|
None
|
|
|
Describe the histology of breast cancer: Invasive lobular
|
Multiple and bilateral
|
None
|
|
|
Describe the histology of breast cancer: Medullary
|
Fleshy, cellular with lymphocytic infiltrate (good prognosis)
|
None
|
|
|
Describe the histology of breast cancer: Paget’s disease of the breast
|
Eczematous patches on the nipples or areola; represents spread of ductal carcinoma through ducts to skin of nipple
|
None
|
|
|
Where can breast cancer metastasize to
|
Anywhere in the body, but especially the axillary lymph nodes, lung, liver, brain, and bone
|
|
|
|
What oncogene abnormality is routinely found in patients with breast cancer
|
Amplification of c-erbB2 (HER-2/neu)
|
|
|
|
What are the general treatments available to women with breast cancer
|
Surgery (breast conserving vs. mastectomy), radiotherapy, chemotherapy, hormone therapy, and pain management
|
|
|
|
Hormone therapy is a form of systemic treatment that can be combined with surgery or radiotherapy to destroy undetected cancer cells and cells outside the breast. What are examples of this therapy
|
Antiestrogens (tamoxifen), ovarian treatments (ovarian ablation), and aromatase inhibitors
|
|
|
|
What is the classic scenario at presentation for endometrial hyperplasia/carcinoma?
|
A peri- or postmenopausal woman with abnormal vaginal bleeding and leukorrhea. These women should have a pelvic examination and endometrial sampling.
|
|
|
|
Early menarche, late menopause, obesity (↑ peripheral estrogen), and anovulatory cycles all are thought to be risk factors for the development of endometrial adenocarcinoma. Why? Are there diseases of the ovary that could pose a related risk?
|
Prolonged estrogen stimulation leads to endometrial hyperplasia. Ovarian disease can also be a factor, e.g. polycystic ovarian disease (Stein-Leventhal syndrome) and estrogen producing ovarian tumors (granulosa cell tumor).
|
|
|
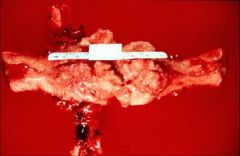
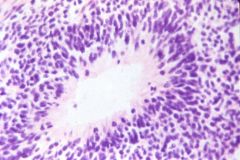
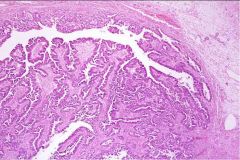
What does this picture demonstrate
|
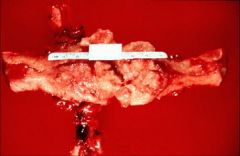
Uterus with extensive endometrial carcinoma. The irregular surface
represents areas of tumor breakdown, leading to bleeding. The tumor is usually diagnosed by biopsy or curettage. |
|
|
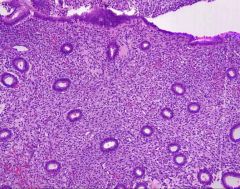
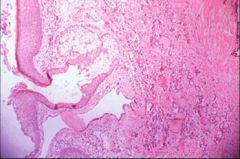
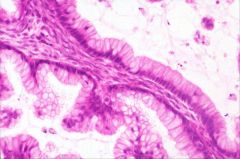
What does this picture demonstrate
|
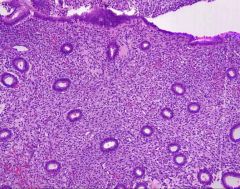
Normal endometrium. The glands are separated by stroma
|
|
|
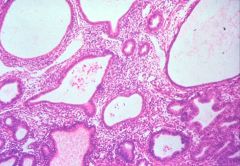
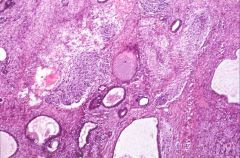
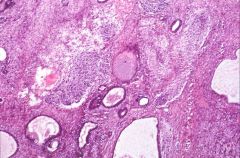
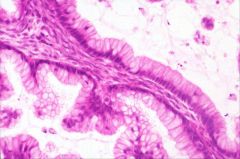
What does this picture demonstrate
|
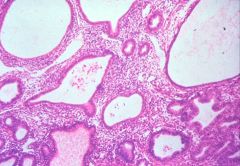
Endometrial hyperplasia
With unopposed estrogen, glands may increase in size and number, compressing the stroma, but without back-to-back architecture. These features comprise endometrial hyperplasia. |
|
|
|
What types/patterns of endometrium can be regarded as normal/physiologic?
|
Proliferative, secretory, menstrual, atrophic and gestational (including the Arias-Stella reaction).
|
|
|
|
A morphologic sequence is evident in the development of endometrial cancer from simple and complex hyperplasia without cytologic atypia, to those with atypia. What are the microscopic features of these entities?
|
Simple hyperplasia (cystic or mild hyperplasia): architectural changes in gland size and shape, with abundant stroma.
Complex hyperplasia: increased number and crowding of glands, and gland shape irregularity (budding). Atypical hyperplasia: gland architecture noted above with irregular epithelial lining, increased mitotic numbers and cytologic atypia with nuclear polarity loss, hyperchromasia, prominent nucleoli, cytomegaly and increased N/C ratio. Atypical endometrial hyperplasia may be difficult to distinguish from well differentiated adenocarcinoma on biopsy specimens. |
|
|
|
What is the risk (%) of developing endometrial cancer
|
Without atypia 1.6%
With atypia 22% |
|
|
|
Discuss the case management of endometrial hyperplasia is the patient if 38 years old
|
Periodic biopsies or curettage
|
|
|
|
Discuss the case management of endometrial hyperplasia if the patient is 40 years old and wants to try and have another child
|
Periodic biopsies or curettage, progestins (prior to conceiving) treatment
|
|
|
|
Discuss the case management of endometrial hyperplasia if the patient is 57 years old and her bleeding is not responding to hormone therapy
|
Hysterectomy
|
|
|
|
Discuss the case management of endometrial hyperplasia if the patient is 38 years old and wants to have a baby
|
Periodic biopsies and progestin suppression
|
|
|
|
Discuss the case management of endometrial hyperplasia if the patient is 41 years old
|
Periodic biopsies and progestin suppression, or hysterectomy
|
|
|
|
Discuss the case management of endometrial hyperplasia if the patient is 57 years old
|
Hysterectomy as first choice. Periodic biopsies and progestin suppression, if she is a surgical risk
|
|
|
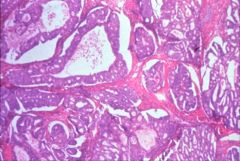
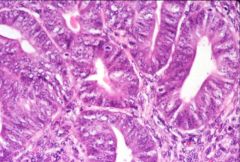
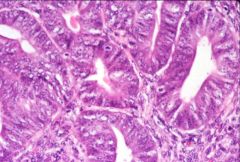
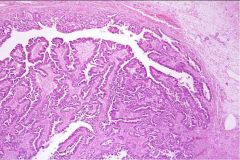
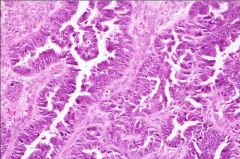
What does this picture demonstrate
|
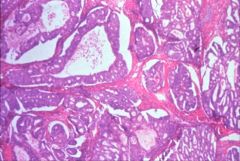
Low magnification of endometrial carcinoma with haphazardly distributed glands. In many areas, the glands are back-to back, without intervening stroma. Where stroma is present, it is markedly fibrotic (desmoplastic).
|
|
|
What does this picture demonstrate
|
Endometrial carcinoma
High power view showing malignant nuclear features |
|
|
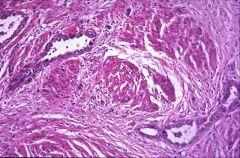
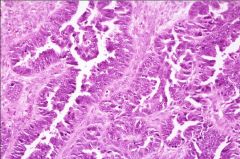
What does this picture demonstrate
|
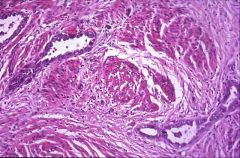
Endometrial carcinoma
Microscopic evidence of myometrial invasion by the tumor |
|
|
|
What are the risk factors for endometrial carcinoma
|
Obesity
Nulliparity Diabetes Hypertension Unopposed estrogen |
|
|
|
What are some conditions that predispose to ectopic pregnancy?
|
Salpingitis
Endometriosis Peritubal adhesions Presence of an IUD. |
|
|
|
What are some of the potential sites for an ectopic pregnancy?
|
Tubal (most common)
Uterine cornu Ovary Abdominal viscera |
|
|
|
In what portion of the fallopian tube are most ectopic pregnancies found?
|
In the ampulla (75-80%), followed by the isthmus (10-15%)
and fimbriae (5%). |
|
|

What does this picture demonstrate
|

Unilaterally enlarged and hemorrhagic fallopian tube characteristic of tubal ectopic pregnancy. Ectopic pregnancy may cause hemorrhage by growing into and rupturing through the wall of the tube.
|
|
|

What does this picture demonstrate
|

Fallopian tube lumen containing an ectopic pregnancy with a well developed embryo. Most ectopic pregnancies do not show this degree of development.
|
|
|
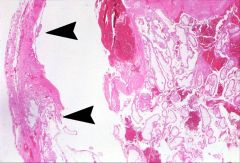
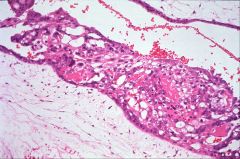
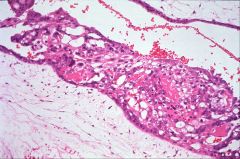
What does this picture demonstrate
|
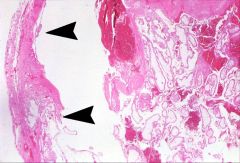
Fallopian tube lumen distended by blood clots and chorionic villi. Arrowheads show villi invading the wall of the fallopian tube, similar to how a normal placenta would implant into the uterus.
|
|
|
|
How would you treat a patient with ectopic pregnancy?
|
If it is a ruptured ectopic pregnancy your options are basically limited to surgery and the prevention or treatment of complications. If it is unruptured you can perform linear salpingostomy, or prescribe single-dose methotrexate, if early.
|
|
|

What does this picture demonstrate
|

Chronic salpingitis
Gross photograph of the uterus, tubes and ovaries. Both fallopian tubes are enlarged. The fimbriated ends are partially occluded and fibrous adhesions can be seen between the tubes and the uterus and ovary. These findings are consistent with chronic salpingitis (hydrosalpinx), a condition that predisposes to ectopic pregnancy. |
|
|
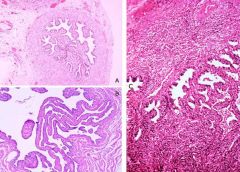
What do these pictures demonstrate
|
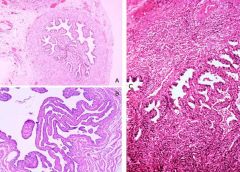
A & B. Normal histology of fallopian tube. C. Chronic salpingitis.
Chronic inflammatory cells are present within the muscularis. The mucosal infolding (plicae) are thickened and fused, and would not allow the normal descent of a fertilized egg. |
|
|

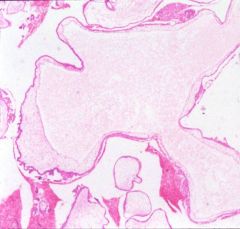
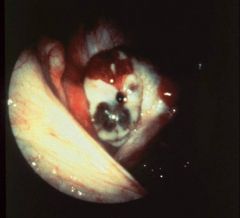
A patient thought she was pregnant but ended up with this. Diagnosis?
|
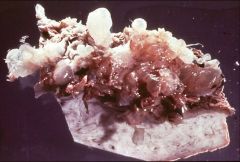
Complete (CHM) or partial (PHM) hydatidiform moles, and hydropic degeneration (HD).
The specimen appears as a collection of delicate, fluid- filled structures (bunch of grapes). |
|
|
|
Discuss the pathogenesis and genetics of molar gestations.
|
Molar gestations are associated with an excess of paternal haploid chromosomes.
In complete hydatidiform moles the genetic constitution is 46XX (both sex chromosomes androgenic). Partial hydatidiform moles are usually triploid, i.e. 69XXY, with two of the sex chromosomes being androgenic. Digynic conceptions do not develop molar changes. |
|
|
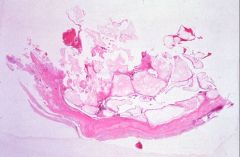
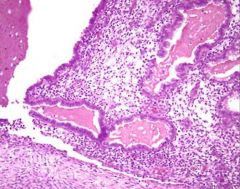
What does this picture demonstrate
|
Hydatidiform mole
The tissue consists of enlarged, edematous chorionic villi lacking vascular structures. Trophoblast proliferation on the surface of the villi is required for the diagnosis of hydatiform moles. |
|
|
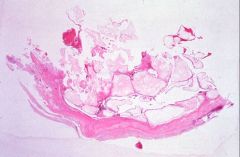
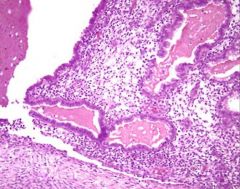
What does this picture demonstrate
|
Hydatidiform mole
Enlarged, edematous chorionic villi lacking vascular structures. Villous trophoblast proliferation is required for the diagnosis of hydatiform moles. |
|
|
|
Compare the morphology, karyotype and risk for subsequent
development of choriocarcinoma of complete and partial moles. |
Complete mole: diploid karyotype (46 XX , most) with fetal parts not
present, all villi are edematous, 2% develop choriocarcinoma, trophoblast proliferation is circumferential. Partial mole: triploid karyotype, fetal parts may be present, not all villi are hydropic, patients rarely develop choriocarcinoma, trophoblastic proliferation partial (syncytiotrophoblast) |
|
|
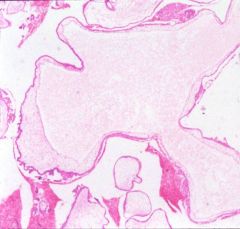
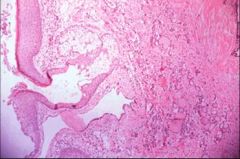
What does this picture demonstrate
|
Hydatidiform mole
There is increased proliferation of the trophoblastic cells on the surface of the villi, required for the diagnosis of hydatiform moles. Normal chorionic villus is 2 cells thick |
|
|

What does this picture demonstrate
|

Early complete hydatidiform mole with an empty gestational sac. No embryo identified on gross examination.
|
|
|
|
What is the treatment for hydatidiform moles
|
Curettage, oral contraceptives for 1 year. HCG should decline. If it plateaus or spikes, put on methotrexate
|
|
|
|
What is infertility?
|
Infertility is defined as the inability to conceive after 12 months
of unprotected sexual intercourse. |
|
|
|
A 38-year-old female who is seeing a reproductive endocrinologist is found to have bilateral adnexal masses.
She has complained of infertility since attempting pregnancy for the past 3 years. She has occasional dyspareunia. What general categories would you include in your differential? |
Ovulatory dysfunction, endometriosis, fallopian tube diseases
and …remember that the problem may be with him, not her. |
|
|
|
What is the etiology of endometriosis? What are the most common sites and symptoms of endometriosis?
|
Etiology: Unknown
Most common theories to explain the phenomena: retrograde menstruation, celomic (peritoneal) metaplasia, and lymphatic/hematogenous spread. Most common site: Ovary Additional common sites: para-ovarian ligaments, rectovaginal septum, uterine serosa, other pelvic peritoneum. Unusual sites: umbilicus, surgical scars, nose, skin and lung (endometriosis has been described in almost every body site). Symptoms include: dysmenorrhea (painful menses) and dyspareunia (painful intercourse). |
|
|
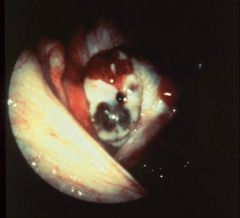
What does this picture demonstrate
|
Laparoscopic view of endometriosis on the peritoneal surface. An
area of brown pigmentation is present. The characteristic color, due to old hemorrhage, has given rise to the term powder burn for these lesions. |
|
|
|
What is endometriosis?
|
Endometriosis is the presence of
endometrial glands and stroma outside of the of the uterus. Endometriosis should not be confused with adenomyosis, which is the presence of endometrial glands and stroma within the uterine wall. |
|
|
|
What are some possible
complications of ovarian endometriosis or endometriomas? |
Mass effect, adhesions,
rupture, torsion and development of 2o malignancies. |
|
|

What does this picture demonstrate
|

Endometrioma (or chocolate cyst): accumulated blood from endometriosis enlarges the ovary
The center is filled with a chocolate brown material, formed by clotted blood. The surgeon must handle these cysts with care, or they will rupture, releasing the bloody fluid into the abdomen. |
|
|
What does this picture demonstrate
|
Histology of an endometrioma, formed by endometrial glands and
stroma with hemorrhage (hemosiderin laden macrophages) surrounded by normal ovarian stroma. The ectopic endometrium can react cyclically to external hormonal stimuli. Endometriosis will respond to suppression by exogenous progesterone or androgenic hormones. |
|
|

What does this picture demonstrate
|

Gross photograph of a mature cystic teratoma. The lumen is filled
with a cheesy thick material which is usually liquid at body temperature. Hair is also present. A solid area (Rokitansky's tubercle) is present, which contains most of the mature elements. Bone or teeth are often seen as a part of this tumor and can be identified on x-rays of the specimen or abdomen. |
|
|
What does this picture demonstrate
|
Some of the mature tissue encountered in teratomas (squamous
epithelium with keratin and sebaceous glands, thyroid tissue). Occasionally a teratoma can be composed of only one tissue type (monodermal teratoma); if the tissue is thyroid, the condition is known as struma ovarii. |
|
|
What does this picture demonstrate
|
Immature teratoma with mature elements and areas of embryonic neuroectoderm.
|
|
|
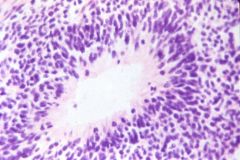
What does this picture demonstrate
|
Teratoma
Higher mag: typical cytologic features of neuroectodermal cells, small oval hyperchromatic nuclei surrounded by scant basophilic cytoplasm, palisading (lining up) perpendicular to a central vessel forming structures resembling neural tube. The amount of immature neuroepithelium is essential to assess histologically as it is used in predicting clinical behavior. |
|
|
|
What is the difference between a dermoid cyst (mature teratoma) that has undergone malignant transformation and an immature teratoma?
|
1% of dermoid cysts can undergo malignant transformation of their somatic component elements, with squamous cell carcinoma being the most commonly cited.
Immature teratoma, also a malignant neoplasm, is comprised of component tissue derived from tissue resembling fetus or embryo rather than adult/mature. |
|
|
|
What clinical findings would suggest that a dermoid cyst has
undergone malignant transformation? |
Rapid growth of tumor, weight loss, pain and systemic symptoms.
Diagnosis has to be confirmed by histology. |
|
|

This was removed from a woman. Diagnosis?
|

Gross photo of a multiloculated
mucinous cystadenocarcinoma. The areas of concern to sample are the solid, papillary areas where atypical cells are more likely to be found. |
|
|
What does this picture demonstrate
|
A papillary structure with tall,
mucinous cells. There is no significant atypia. These features are consistent with mucinous cystadenoma. |
|
|
What does this picture demonstrate
|
Serous cystadenocarcinoma with complicated glands and definite nuclear pleomorphism and hyperchromasia.
|
|
|
What does this picture demonstrate
|
Serous cystadenocarcinoma with complicated glands and definite nuclear pleomorphism and hyperchromasia.
|
|
|
|
What is pseudomyxoma peritonei?
|
A rare condition complicating mucinous ovarian neoplasms where
the abdominal viscera become encased in a mucinous matrix: mucinous ascites, cystic epithelial implants, and adhesions. Extra-ovarian, usually appendiceal, origin with secondary spread to ovary has been cited as the culprit in many cases. |
|
|
|
What is cancer antigen 125 (CA-125)?
|
Cancer antigen, CA-125 is a glycoprotein that is measured in the serum of women with ovarian tumors that is followed during the course of their therapy. It is elevated not only in ovarian neoplasms, but in other nonneoplastic conditions, therefore it is not used as a screening test.
|
|
|
|
List and describe the other surface epithelium tumors.
|
Endometrioid tumors are usually malignant, with a 40-50% 5-year survival. Up to 30% are associated with endometrial carcinoma. About 15% of cases coexist with endometriosis. Morphologically they resemble endometrial glands.
Clear cell adenocarcinomas may be solid or cystic and are probably a variant of endometrioid adenocarcinoma. They are aggressive and have a poor prognosis when spread beyond the ovary. Brenner tumors resemble urinary bladder epithelium and are usually found incidentally, often in association with mucinous cystadenocarcinomas. They consist of nests of transitional cells. |
|
|
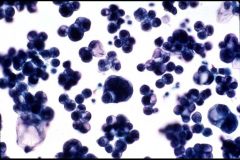
What does this picture demonstrate
|
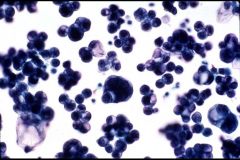
Cytologic examination of peritoneal fluid in a patient with known carcinoma of the ovary revealed the presence of metastatic carcinoma. This is important in staging and prognosis.
|
|
|
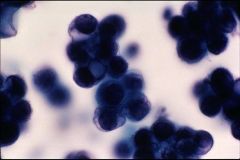
What does this picture demonstrate
|
Here you can see cytoplasmic mucin vacuoles (glandular cells usually contain mucin), further evidence of glandular differentiation. (Caution: not all cytoplasmic vacuoles are due to mucin production, vacuoles may be the result of degeneration.)
|
|