![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
72 Cards in this Set
- Front
- Back
|
Possible faults with fissure sealants (7) |
- completely debonded - not fully extended - not set - air blow at surface - air blow through to enamel - underfilled - over filled |
|
|
Possible faults with fissure sealants (7) Why is it caused What to do to resolve it |
- completely debonded Poor moisure control Start again from beginning - not fully extended Poor moisture control Remove fragments & start again - not set Incorrect position of curing light Wipe off and start again - air blow at surface Due to too much mixing or used a microbrush to apply Polish with a white stone - air blow through to enamel Due to too much fixing ot used a microbrush to apply Reseal area of air blow - underfilled Wrong instrument used to apply Start again or add more sealant - over filled Wrong instrument used to apply Polish with white stone |
|
|
What causes & How to manage fault of fissure sealant - completely debonded |
Due to poor moisture control Start again from beginning |
|
|
What causes & How to manage fault of fissure sealant - not fully extended |
Due to poor moisture control Remove fragments and start again |
|
|
What causes & How to manage fault of fissure sealant - not set |
Incorrect position of curing light Wipe off and start again |
|
|
What causes & How to manage fault of fissure sealant - air blow at the surface |
Due to too much mixing of fissure sealant Using a microbrush to apply Polish air blow with white polishing stone |
|
|
What causes & How to manage fault of fissure sealant - air blow through to enamel |
Due to too much mixing of fissure sealant Using a microbrush to appy Reseal the air blow Re etch if moisture control is lost |
|
|
What causes & How to manage fault of fissure sealant - too little material used |
Due to using the wrong instrument to apply Add more material or start again |
|
|
What causes & How to manage fault of fissure sealant - too much material used |
Due to using the wrong instrument to apply Reduce with white stone |
|
|
Process to conplete a fissure sealant (6) |
1. Prophylaxis 2. Tooth isolation and moisture control 3. Etch 4. Replace cotton wool 5. Apply fissure sealant 6. Cure |
|
|
What is used to etch tooth for fissure selant |
37.5% phosphoric acid |
|
|
What materials are used to isolate tooth & do moisture control for a fissure sealant (3) |
Dry tip Salvia ejector Cotton wool |
|
|
What materials can be used as a fissure sealnt (2) |
Unfilled resin GIC |
|
|
Process of using GIC as fissure sealant |
1. Prophylaxis 2. Apply directly to tooth 3. Adapt with pear shaoed burnisher 4. Self cure - cover with wax 5. Set for 5 mins 6. Remove wax & apply varnish |
|
|
Why is a BPE done (2) |
Screening tool for perio disease Provudes basic guidance of treatment needs |
|
|
What does doing a BPE tell us |
Basic guidance on treatment needs |
|
|
How is a BPE done |
- Detention divided into 6 - WHO probe walked around the sulcus at 6 sites per tooth - Highest score recorded for each sextant - Don't include 8s unless 6 or 7 is missing - If sextant only has 1 tooth include it in another sextant |
|
|
Results on BPE - 0 |
Pockets <3.5mm No calculus No bleeding on probing |
|
|
Results on BPE - 1 |
Pockets <3.5mm No calculus Bleeding on probing |
|
|
Results on BPE - 2 |
Pockets <3.5mm No calulus Sub/supragingival calculus |
|
|
Results on BPE - 3 |
Probing depth 3.5-5mm (Black band partially visible) |
|
|
Results on BPE - 4 |
Probing depth >5.5mm (Black band disappears) |
|
|
What actiob is needed for a BPE score of 0 |
Nothing |
|
|
What actiob is needed for a BPE score of 1 |
OHI |
|
|
What actiob is needed for a BPE score of 2 |
OHI Remove plaque retentive factors (calculus) |
|
|
What actiob is needed for a BPE score of 3 |
OHI Plaque retentive factors removed (calculus) Root surface debribement |
|
|
What actiob is needed for a BPE score of 4 |
OHI Root surface bebridment Assess need for further treatment - refer |
|
|
When would a full mouth detailled perio chart done |
When BPE gives a max score of 4 |
|
|
Criteria for posterior approximately prep (8) |
- smoooth outline form - rounded internal angles - retentive vertically - undercut - retentive horizontally - key? - 90 degree cavo surface angles - contact point cleared - pulp not compromised - no damage to tbe adjacent tooth - no unsupported enamel |
|
|
Posterior approximal restoration criteria (8) |
- no ledges - well condensed - marginal ridge created - consistent with morphology of tooth -contract point restored - no excess amalgam/flash - not over carved/undefilled - doesn't impede occlusion |
|
|
Anterior approximal prep criteria (10) |
- cavity in the middle 1/3 of crown - wider buccally than palatally - not grossly destructive to buccal/labial surface - no unsupported enamel - smooth outline form - contact point cleared - not endangering pulp - minimally destructive to palatal tissues |
|
|
Criteria for an access cavity (5) |
- mininallt destructive - floor or walls of pulp chamber not perforated - pulp chamber fully unroofed in occlusal and lateral directions - cavity has clean walls in continuity to pulp chamber - cavity provides sufficient retention for temporary dressing |
|
|
Criteria for cusp replacement (12) |
- retention vertically - retention horizontally - retsores occlusion - not over cavrved - well condensed - restores contact point - marginal ridge restored - no unsupported enamel -reproduces morphology - no ledges - not overfilled - smooth matt finish |
|
|
Criteria for GIC restoration (12) |
- no voids at margin - not dehydrated - smooth glossy finish - not bulbous - not underfilled - fully set - no flash at margins -no ledges - thin layer of varnish - no foreign bodies - colour match - restores contour of tooth |
|
|
Criteria for incisal edge repair (9) |
- colour match - restores morphology of tooth - no voids - smooth margins (no ledges) - restoration supports occlusion - doesnt impede occlusion - no damage to adjacent tooth - contact point restored - smooth finish |
|
|
Criteria for preformed metal crown (8) |
- reduced occlusion by 1-1.5mm - occlusal anatomy maintained - 10-15 degree mesial & distal taper - 1-1.5mm depth into gingival margin - contact area cleared - smooth peripheral bevel - no sharp angles - no preparation of buccal or palatal walls |
|
|
Systematic check for headpiece faults (7) |
1. Handle sleeve 2. Head 3. Back cap 4. Spray cap 5. Bur chuck 6. Bearings 7. Coupling connection |
|
|
Headpiece faults (7) Significance |
- loose handle sleeve Exposes internal elements = cross infection risk - loose head Come off = choke Reduced accuracy - loose backcap Choke - loose spraycap Choke Stop proper water spray = burning of tissues - broken chuck Reduced accuracy - worn bearings Handpiece over heats Reduced accuracy - broken coupling connection Headpiece unstable in use |
|
|
Proper handwashing technique |
Aycliffe 40-60 secs |
|
|
5 moments to hand wash |
Before patient contact After patient contact Before aseptic task After direct exposure to body fluid After contact with patient surroundings |
|
|
What NOT to ask when giving VBA to stop smoking (4)
|
- How much they smoke - What they smoke - If they want to stop - Dont advise to smoke |
|
|
3 steps of VBA
|
1. Ask 2. Advise 3. Act |
|
|
What to say in 1st stage of VBA ASK |
Are you (still) smoking?
|
|
|
Why must check of started smoking again after stopped?
|
Because 70% of those who quit start again within 3 years
|
|
|
How many of those who stop smoking start again within 3 years |
70%
|
|
|
What to say in 2nd stage of VBA ADVISE |
Say best way to stop smoking is a combination of support & medical treatment - Its hard tgo stop alone - Provides help to stay quit |
|
|
What to say in 3rd stage of VBA ACT |
Refer to stop smoking services - Provide the number If want to quit but dont want to talk to someone, prescribe (not the most effective alone) - Prescribe Varenicine/patches/gum - Ask them to eturn every 2 weeks to assess their progress |
|
|
Which meducations are best to stop smoking (2)
|
Varenicine Fast acting - nicotine gum/patches |
|
|
What to do if smoker doesn't want to stop smoking
|
Say thats fine Support will always be available if you ever want to quit |
|
|
What to do if patient wants to go into a lengthy chat about thwir smoking
|
Stooping smoking is such an important decision that requires dedicated time to discuss Why not make another appointment or call the stop smoking services to talk about it properly |
|
|
How long after a paient stops smoking hould you keep asking about their smoking status
|
3 years
|
|
|
What wall of maxillary sinus are you looking for
|
Posterior wall of maxillary sinus
|
|
|
Tear drop next to the posterior wall of the maxillary sinus
|
Pterygoid palatine fossa
|
|
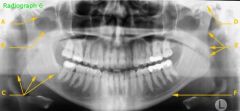
What is F? Significance if resorbed |
Cortical bone Resorned = oestoporosis |
|
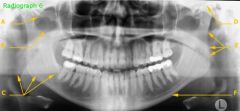
What is A
|
Zygomatic arch
|
|
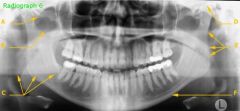
What is B
|
Zygomatic notch
|
|
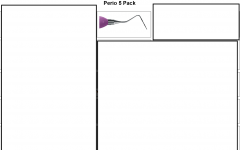
What part of perio pack 5 is this
|
BPE probe
|
|

What park of perio pack 5 is this
|
Macfarlane 2/3
|
|

What park of perio pack 5 is this What does it do |
Anterior Jacquette of Macfarlane 2/3 Anterior teeth All sufaces |
|

What park of perio pack 5 is this What does it do |
Push scaler of Macfarlane 2/3 Interproximal of anterior teeth |
|

What park of perio pack 5 is this What does it do |
Mini sickle Anterior teeth All surfaces |
|

What park of perio pack 5 is this What does it do |
Macfarlane 4/5 All teeth All sufaces |
|

What park of perio pack 5 is this What does it do |
Columbia 2L 2R All teeth All surfaces Subgingival |
|
|
Which teeth do you fissure seal (4)
|
- 6's & 7s as they erupt - Hypoplastic/hypomineralsied teeth - Anterior teeth with deep palatal pits - Primary teeth if patient has very high caries risk |
|
|
When would GIC be used for a fissure sealant instead of unfilled resin
|
Moisture control is not adequate Uncooperative Partially erupted teeth PTOCEEDURE MUST BE DONE QUICKLY eleases F - benifit |
|
|
How to take patient history
|
1. Introduce self 2. Patient repeat name & age 3. Patent goves consent 4. Signpost 5. Medical hisroty 6. Social hostory 7. Dental history 8. Signpost session 9. Open question - " Any issues?" "What can I do for you today?" 9. ICE 10. Chunk & Check 11. Summarise & close session |
|
|
Purpose of placing rubber dam (5)
|
- Airways protected - Protects from sodium hyochloride/chemicals - Psychological barrier - Soft tissure retraction - Reduce aerosols in mouth |
|
|
Limitations to rubber dam (7)
|
- Dentist can lose orientation - Latex allergy risk - Technique sensitive - Anxious patients worry about choking - Barrier to communication - Uncomfortable - Can damage tooth/tissue if poorly placed |
|
|
How d=to decde whether to place fissure sealant for stained fissures
|
Enamel biopsy = staining enamel deep then fissure seal PRR = staining to dentine, fill will with resin, unless in load bearing area, then use conventional resoration |
|
|
Which upper teeth dont have 1 root canal? How many do they have? (3) |
Upper 4 = 2 canals, buccal & palatal Upper 6 = 3 canals, 2 buccal 1 palata Upper 7 = 3 canals, 2 buccal 1 palatal |
|
|
Which lower teeth dont have 1 root canal? How many do they have? (5) |
Lower 1 = 2 canals Lower 2 = 2 canals Lower 3 = 2 canals Lower 6 = 4 canals, 1 mesial, 2 distal Lower 7 = 3 canals, 1 mesial, 2 distal |
|
|
|
|