Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
70 Cards in this Set
- Front
- Back
|
write the 4 principles of Osteopathic Philosophy
look for 4 blank lines... |
The body is a unit; the person is a unit of body, mind, and spirit
The body is capable of self-regulation, self-healing, and health maintenance Structure and function are reciprocally interdependent Rational treatment is based upon an understanding of the basic principles of body unity, self-regulation, and the interrelationship of structure and function |
|
|
define somatic dysfunction
|
the impaired or altered function of related components of the somatic (body framework) system
|
|
|
define Osteopathic manipulative treatment (OMT)
|
the therapeutic application of manually guided forces by an osteopathic physician to improve physiologic function and/or support homeostasis that has been altered by somatic dysfunction
|
|
|
define Facilitation:
|
the maintenance of a pool of neurons in a state of partial or sub threshold excitation ; in this state, less afferent stimulation is required to trigger the discharge of impulses
|
|
|
what is TART
|
Tissue texture abnormalities
Asymmetry Restriction of motion Tenderness |
|
|
what are the 3 motion barriers? define them..
|
Anatomic: the limit of motion imposed by anatomic structure; the limit of passive motion
Physiologic : the limit of active motion Direct: may also see it called the restrictive barrier; a functional limit that abnormally diminishes the normal physiologic range |
|
|
define how you would perform counterstrain
|
Find and label tender point 10/10
Position to relieve tenderness (2/10 or less) Fine-tune to 0/10 if possible Hold position for 90 seconds (some schools teach 120 seconds for the ribs) Slow passive return to neutral Retest tender point |
|
|
define how you would apply MFR
|
Diagnose restricted motion
Slowly move into position of laxity and follow release until completed (indirect) Slowly move into restriction and stretch until tissue give completed (direct) Retest motion |
|
|
what is unique in ME?
|
requires pt activity
Diagnose restriction Move into restrictive barrier Isometric contraction 3-5 seconds Stretch until give stops Repeat 3-5 times Retest motion |
|
|
define traction, kneading, inhibition, effleurage, and petrissage
|
Traction – longitudinal muscle stretch
Kneading – lateral muscle pressure Inhibition – sustained muscle pressure Effleurage – stroking pressure to move fluid Petrissage – squeezing pressure to move fluid |
|
|
give the acute vicerosomatic findings for
temp tissue texture red reflex |
hot
Moisture, fullness, edema, tension Increased or prolonged redness |
|
|
give the chronic vicerosomatic findings for
temp tissue texture red reflex |
cool
thickness, dryness, ropiness, pimples prolonged blanching |
|
|
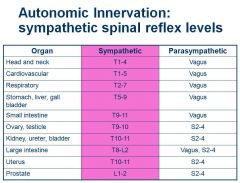
write out the autonomic chart
|
|
|
|
where is the chapmans point for the appendix
|
tip of the 12th rib
|
|
|
what is the difference btw a chapman's point, counterstrain, and triggerpoint
|
Chapman’s point: viscerosomatic reflex
Conterstrain point: locally tender Trigger point: referred pattern of pain, motor dysfunction, autonomic phenomenon |
|
|
what are the rotatorcuff muscles?
WHEELHOUSE! |
supraspinatus, infraspinatus, teres minor, subscapularis
|
|
|
movements of scapula
|

|
|
|
The ulnohumeral joint moves in what direction with flexion/extension?
what will this do to the carrying angle |
The ulnohumeral joint passively adducts with flexion and passively abducts with extension
This cause the hand to deviate to the mouth during flexion It is also responsible for the carrying angle |
|
|
describe ulnar abduction
|
Restricted adduction (lateral glide)
Patient may present with pain or restriction at endpoint of flexion Increases the carrying angle |
|
|
describe Ulnar Adduction
|
Restricted abduction (medial glide)
Patient may present with pain or restriction at endpoint of extension Decreases the carrying angle |
|
|
With a posterior radial head somatic dysfunction: (give ease and restriction)
how does this normally occur |
Ease of motion is posterior glide
Restricted motion is anterior glide with supination A posterior radial head somatic dysfunction is often caused by a fall forward onto an outstretched hand |
|
|
Common elbow and wrist problems
|
Carpal tunnel syndrome
Thoracic outlet syndrome Double crush syndrome |
|
|
what are thoracic outlet syndrome, carpal tunnel, and double crush syndrome
|
Thoracic Outlet Syndrome
Pain and/or paresthesia in the upper extremity from brachial plexus compression Neural compression is more common than vascular compression Carpal Tunnel Syndrome Median nerve compression in the carpal tunnel associated with numbness, and pain in the arm and hand along the median nerve distribution Double Crush Syndrome mixture of above |
|
|
what is the Scalene compression test (Adsons maneuver)? shows the pt has?
|
Positive test = diminished pulse and/or reproduction or exacerbation of symptoms
Thoracic Outlet Syndrome |
|
|
Patient usually complains of pain of the palmar surface of the thumb, index and middle finger
|
Carpal tunnel syndrome
Compression of the median nerve within the carpal tunnel |
|
|
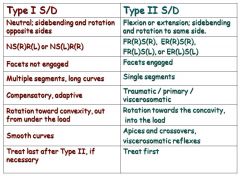
describe fryette type I
|
Law I = when the spine is in neutral (easy normal), sidebending and rotation are in opposite directions. (Type I Mechanics)
Occurs in neutral (facets not engaged) Found in thoracic and lumbar spines Forms long curves, multiple segments Compensatory |
|
|
describe fryette type II
|
Law II = when the spine is flexed or extended (non-neutral), sidebending and rotation are in the same directions. (Type II Mechanics)
Occurs in flexion or extension Facets engaged Occurs in thoracic and lumbar spines Type II-like motion in cervical spine Usually single segments Found at apices and crossovers and/or sites of viscerosomatic reflexes Primary somatic dysfunction Due to strain or viscerosomatic reflex |
|
|
describe fryette law III
|
Law III = when motion introduced in one plane it modifies (reduces) motion in other two planes
When a segment is brought up to a restrictive motion barrier it will move in the position of greatest ease in the other two planes. Restriction = direction it won’t go. Somatic dysfunction = defined by direction it will go with ease. |
|
|
flip for examples of t1 and t2 s/d
|
|
|
|
ant lumbar counterstrain points
|
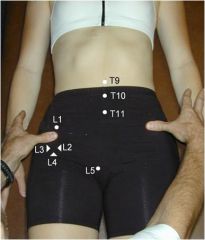
Occur in 2 sets
Midline (T9-T11) Along the ilium (T12-L5) L2, L3, and L4 are all clustered around the AIIS and are differentiated by the direction in which you push Treated in similar manner |
|
|
what are the key fascial diaphragms?
|
Pelvic diaphragm (L5-S1)
Thoracic diaphragm (T12-L1) Thoracic inlet (T1, 1st rib) Suboccipital region (OA, AA) |
|
|
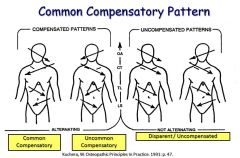
diaphragm compensatory patterns
|
|
|
|
Patient presents with a positive left standing flexion test. Left ASIS is cephalad. Left PSIS is cephalad. What is pelvic diagnosis?
|
Left superior Innominate Shear
|
|
|
Patient has positive ASIS compression test
on the left. Both left ASIS and left PSIS are caudad. What is your diagnosis? |
Left inferior innominate shear
|
|
|
Positive Standing tests on the left. Positive ASIS compression test on the left. What does this tell you? Left ASIS caudad. Left PSIS cephalad.
What is the diagnosis? |
Left Anterior Innominate rotation
|
|
|
Positive Standing test left. Left ASIS is cephalad and left PSIS is caudad
What is the diagnosis? |
Left Posterior Innominate Rotation
|
|
|
Positive ASIS compression test on right. Right ASIS closer to midline relative to left. What is the diagnosis?
|
Right innominate inflare
|
|
|
Positive ASIS compression test left. Left ASIS further from midline relative to right. What is your diagnosis?
|
Left innominate outflare
|
|
|
during inhalation, how does the sacral base move
|
sacral base goes posterior
this is the S1 axis |
|
|
during cranial flexion, how does the sacral base move
|
Cranial FlexionSacral base extends/ counter-nutates/posterior
Cranial Extension sacral base flexes/nutates/ anterior |
|
|
what does a positive spring test show you?
negative? |
Lumbar Spring Test
Positive Test Resistance to springing sacral extensions (ie LUE) or backward rotation on oblique axis (ie L on R) Negative Test Ease of Springing sacral flexions (ie LUF) or forward rotation/torsion (R on R) |
|
|
what does a pos/neg backward bend test show you?
|
Positive Test
increased sacral base asymmetry sacral extensions (ie LUE) or backward rotation on oblique axis (ie R on L) Negative Test decreased sacral base asymmetry sacral flexions (ie LUF) or forward rotation or torsion (ie L on L) |
|
|
Patient presents with sacroiliac pain. She has a positive seated flexion test on the right. She has a negative spring test. L2-5 are NRRSL. The right sacral base is anterior and the Left ILA is posterior. What is her sacral diagnosis?
|
Seated flexion test positive on Right:
What does this tell you? Right SI joint is restricted and has Left oblique axis if engaged Negative spring test: What does this tell you? L/S junction can flex, ie forward rotation L5 rotated right: Sacrum rotates left L5 sidebent left: Left oblique axis Right base anterior Left ILA posterior What is your diagnosis? Left on Left Sacral Torsion |
|
|
Seated flexion test positive on left. Negative backward bending test (findings become more symmetrical). L3-5 are NRLSR. Assuming physiologic motion between lumbar and sacrum, can you give diagnosis?
|
Seated flexion test positive on left:
What does this tell you? Left SI joint is restricted and has Right oblique axis if engaged Negative backward bending test (findings become less asymmetrical): What does this tell you? sacrum can flex (ie forward torsion) L5 rotated Left: Sacral rotation right L5 is sidebent to right Right oblique axis Left base would be anterior Right ILA would be posterior What is your diagnosis? Right on Right Sacral torsion |
|
|
Seated flexion test positive on right with positive spring test. L5 is rotated left. The right sacral base is posterior and the Left ILA anterior. What is the diagnosis?
|
Seated flexion test positive on Right
What does that tell you? Left sacral axis Positive spring test What does that tell you? L/S junction is extended (can’t flex) backward torsion L5 rotated left: What does that tell you? sacral rotation right on oblique axis Right base posterior Left ILA anterior What is the diagnosis? Right on left torsion |
|
|
Seated flexion test positive on left with positive spring test. L5 is FRSL. Assuming normal mechanics, what is the sacral diagnosis?
|
Seated flexion test positive on Left
What does that tell you? Right sacral axis Positive spring test What does that tell you? L/S junction is extended (can’t flex) backward torsion L5 rotated right: sacral rotation left L5 sidebent right: Right oblique axis What is the diagnosis? Left on Right torsion |
|
|
Seated flexion/ASIS compression test positive on Left.
Negative Backward Bending Test (findings become less asymmetrical) Left base is anterior and left ILA is posterior and inferior. What is your diagnosis? |
Seated flexion/ASIS compression test positive on Left
What does that tell you? Left SI restriction Negative Backward Bending Test (findings become more symmetrical) What does that tell you? Sacrum prefers flexion Left base is anterior Left ILA posterior and inferior What does this tell you? Not a torsion What is your diagnosis? Left Unilateral Sacral Flexion |
|
|
tx for Left on Left Sacral Torsion (forward)
|
Forward Torsion Muscle Energy
Pt lying on the axis side with the chest down on the table; Flex the knees and hips until motion is felt at the lumbosacral junction, usually at least 90° hip flexion; Allow the legs to hang down off the table with thighs supported by your leg Monitor the anterior sacral base and ask the patient to push the feet toward the ceiling for 3-5 seconds against your equal resistance; Slowly move the legs toward the floor to a new restrictive barrier; Repeat 3-5 times or until return of sacral mobility; Retest sacroiliac motion or sacral symmetry. |
|
|
tx for Left on Right torsion
|
Backward Torsion Muscle Energy
Technique (lateral recumbent): Sit or stand in front of the patient who is lying on the axis side with the upper back on the table; Extend the leg on the table until motion is felt at the lumbosacral junction; Flex the top leg and place the foot behind the other knee; Hold the shoulder to prevent the patient from rolling and allow the flexed knee to hang down off the table; Ask the patient to push the flexed knee toward the ceiling for 3-5 seconds against your equal resistance; Slowly move the knee toward the floor to a new restrictive barrier; Repeat 3-5 times or until sacral mobility returns; Retest sacroiliac motion or sacral symmetry. |
|
|
tx for Right Unilateral Sacral Flexion
|
Stand facing the patient’s head on the side of the unilateral flexion;
place your thenar or hypothenar eminence on the involved inferior lateral angle and push it anteriorly and superiorly by leaning into it; Use your other hand to slightly abduct and internally rotate the lower extremity on the involved side; While the patient takes a deep breath, push the sacrum into extension during inhalation and resist sacral flexion during exhalation; Repeat 3-5 times or until sacral mobility returns; Retest sacroiliac motion or sacral symmetry. |
|
|
Seated flexion test positive on left with positive spring test. L5 is FRSR. Assuming normal mechanics, what is the sacral diagnosis?
|
Seated flexion test positive on Left
What does that tell you? Right sacral axis Positive spring test What does that tell you? L/S junction is extended (can’t flex) backward torsion L5 rotated right: sacral rotation left L5 sidebent right: Right oblique axis What is the diagnosis? Left on Right torsion |
|
|
Seated flexion/ASIS compression test positive on Left.
Negative Backward Bending Test (findings become less asymmetrical) Left base is anterior and left ILA is posterior and inferior. What is your diagnosis? |
Seated flexion/ASIS compression test positive on Left
What does that tell you? Left SI restriction Negative Backward Bending Test (findings become more symmetrical) What does that tell you? Sacrum prefers flexion Left base is anterior Left ILA posterior and inferior What does this tell you? Not a torsion What is your diagnosis? Left Unilateral Sacral Flexion |
|
|
Seated flexion/ASIS compression
test positive on Left. Positive Spring test. Left base posterior (or right anterior) and Left ILA anterior (or right posterior). What is your diagnosis? |
Seated flexion/ASIS compression
test positive on Left: What does that tell you? Left SI restriction Positive Spring test: What does this tell you? L/S junction is extended (can’t flex) Left base posterior (or right anterior) Left ILA anterior (or right posterior) What is your diagnosis? Left unilateral sacral extension |
|
|
tx for unilateral sacral extension?
|
Stand facing the patient’s feet on the side of the unilateral extension;
Place your thenar or hypothenar eminence on the involved sacral base, and push it anteriorly and inferiorly by leaning into it; Use your other hand to slightly abduct and internally rotate the lower extremity on the involved side. While the patient takes a deep breath, resist sacral extension during inhalation and push the sacrum into flexion during exhalation; Repeat 3-5 times or until sacral mobility returns; Retest sacroiliac motion or sacral symmetry. |
|
|
what is normal rate and amplitude of CRI
|
Rate = cycles/min (10-14)
Amplitude = distance from flexion to extension (0- 5) |
|
|
how do unpaired and paired cranial bones move?
|
Unpaired bones move in flexion and extension.
Paired bones move in external rotation and internal rotation. Flexion of unpaired bones - external rotation of paired bones. Extension of unpaired bones - internal rotation of paired bones |
|
|
flip to see Conventions in naming cranial strain patterns
|
Torsions are named for the superior greater wing of the sphenoid.
Sidebending rotations are named for the side of head convexity. Sphenobasilar strains are named for the direction of basisphenoid movement (which is opposite to greater wing movement). |
|
|
in a lateral static postural exam, what are the 6 points The weight bearing line should normally pass through?
|
1) just anterior to lateral malleolus;
2) middle of tibial plateau; 3) greater trochanter; 4) body of L3 (center of body mass); 5) middle of humeral head; 6) external auditory meatus; |
|
|
describe the hip drop test
|
Ask the standing patient to shift weight onto one leg, allowing the other knee to bend which induces lumbar sidebending toward the weight bearing leg;
Observe lumbar sidebending and amount of hip drop which is normally ≥ 25°; Hip drop < 25° (positive test) indicates restricted lumbar sidebending toward the side of the weight bearing leg. Test is named for the bent leg side (+ right hip drop test indicates restricted left lumbar side bending) |
|
|
define scoliosis
Two reversible causes of idiopathic scoliosis? |
Scoliosis is defined as a curve > 10°
Short leg syndrome with compensatory scoliosis (scoliotic posture) Trauma to the spine causing strain & resultant deformity in immature skeleton, if treated before skeletal maturity |
|
|
what are the most reliable Prognostic Indicators for scoliosis?
|
Most reliable
Future growth potential Age at diagnosis Menarche in females Risser sign Curve severity at diagnosis |
|
|
Functional impairment with thoracic curves
Possible respiratory impairment >? Possible cardiac impairment >? |
Functional impairment with thoracic curves
Possible respiratory impairment >50 ° Possible cardiac impairment >75 ° above 50, tx is surgery |
|
|
heel lift protocal?
|
1/8 inch lift and lift at a rate no faster than 1/16 per week or 1/8 inch every 2 weeks
Fragile patients (arthritic, osteoporotic, aged, acute pain) 1/16 lift and lift no faster than 1/16 every 2 weeks Start low and go slow |
|
|
Mix & Match “Rib Basket”
Rib 1 Ribs 2-5 Ribs 6-10 Ribs 11-12 with the following: caliper motion bucket handle pump handle elevated or depressed subluxation inhalation or exhalation |
Rib 1: elevation/ depressed
Ribs 2-5: pump handle Ribs 6-10 :bucket handle Ribs 11-12: inhale/exhale |
|
|
What is the key rib?-
inhalation? Exhalation? |
What is the key rib?- refers to the rib in a group
Inhalation- the bottom rib is the key rib Exhalation- the top rib is the key rib |
|
|
Reminders on Sequencing Trx
|
First treat thoracic
type II, then type 1 Treat subluxed rib before a respiratory rib For a group of respiratory ribs, treat the key rib: top rib for exhaled ribs bottom rib for inhaled ribs may still have to treat individually |
|
|
Palpatory findings:
right ribs 2-4 exhalation dysfunction left ribs 5-9 inhalation dysfunction left rib 5 posterior rib subluxation T4-8 N S left R right T8 Flexed R left S left What is the sequence of treatment? |
in order:
t8 T4-8 N S left R right left rib 5 posterior rib subluxation then inhalation/exhalation |
|
|
of is C2-C7 diagnosed
|
not fryettes
ex: rotate left sidebend left |
|
|
50% of cervical flexion and extension occurs at the
50% of cervical rotation occurs at the |
50% of cervical flexion and extension occurs at the OA joint
50% of cervical rotation occurs at the AA (C1-2) joint |
|
|
please list C5-T1 DTRs/Strength test
|
C5 DTR-biceps, strength- biceps
C6 DTR-brachioradialis, strength- wrist extensors C7 DTR-triceps, strength- wrist flexors C8 DTR-none, strength- finger flexors T1 DTR-none, strength- interossei |