Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
40 Cards in this Set
- Front
- Back
|
What 4 things does the Obstetric examination contain beyond the standard physical examination?
|
1. Maternal abdominal examination for contractions & the fetus (Leopold maneuvers)
2. Cervical examination 3. Fetal heart tones 4. sterile speculum examination if rupture of membranes is suspected |
|
|
This procedure determines the position of a fetus in a pregnant woman
|
Leopold maneuver
|
|
|
Explain how to do a Leopold maneuver
|
1. Palpate first at the fundus of the uterus in the maternal upper abdominal quadrant
2. Palpate on either side of the uterus 3. Palpate just above the pubic symphysis |
|
|
What does the Leopold maneuver determine?
|
Fetal lie = whether the infant is longitudinal or transverse within the uterus
|
|
|
Define Fetal Presentation
|
either breech or vertex positioning of the fetus
|
|
|
Define Premature Rupture of Membranes (PROM)
Define Prolonged Premature Rupture of Membranes -what does it put the mother & infant at increased risk for? |
1. fetus rupture of membranes at least 1 hour prior to the onset of labor
2. When PROM occurs more than 18 hours before labor -INFECTION |
|
|
What is PPROM?
|
Preterm, Premature Rupture of Membranes
-before 37 wks gestational age |
|
|
What makes one suspect a diagnosis of Rupture of Membranes?
|
history of a gush or leaking of fluid from the vagina
|
|
|
How does one confirm a diagnosis of ROM?
|
Pool test = + if there is a collection of fluid in the vagina
-can be augmented by asking the patient to cough or bear down Nitrazine = amniotic fluid is basic & turns nitrazine paper blue as opposed to the acidic vaginal secretions Fern test = estrogens in the amniotic fluid cause crystallization of the salts in the amniotic fluid when it dries |
|
|
What may cause a false positive in the Fern test?
|
taking a sample directly from the cervix b/c cervical mucus also ferns
Also blood, semen, & vaginitis |
|
|
What examination allows the obstetrician to determine whether a patient is in labor, the phase of labor & how labor is progressing?
|
Cervical examination
|
|
|
What are the 5 components of the Cervical Examination? What do these 5 components comprise?
|
1. Dilation
2. Effacement 3. Station 4. Cervical position 5. Consistency of Cervix Bishop Score **DESC-P |
|
|
A Bishop Score greater than what is consistent with a cervix favorable for both spontaneous & induced labor?
|
8
|
|
|
How is Dilation assessed in Bishop Scoring?
|
by using either one or two fingers of the examining hand to determine how open the cervix is at the level of the INTERNAL OS
-Closed = 0 cm -1 score = 1-2 cm -2 score = 3-4 cm -3 score = < 5 cm |
|
|
What centimeter dilation on average is necessary to accomodate the term infant's biparietal diameter?
|
10 cm
|
|
|
Describe Effacement
|
is a subjective measurement made by the examiner & determines how thinned out the cervix is
Eg. the typical cervix is 3-5 cm in length; thus, if the cervix feels like it is about 2 cm from external to internal os = 50% effaced Complete or 100% effacement occurs when the cervix is as thin as the adjoining lower uterine segment |
|
|
Define Station in the Bishop Scoring system
|
relation of the head to the Ischial Spines of the female pelvis
-level of Ischial Spines = 0 -head higher than Ischial Spines = negative # -head below level of ischial spine = positive # |
|
|
Describe Cervical Constitency in the Bishop Scoring system
|
Firm = 0
Medium = 1 Soft = 2 |
|
|
Describe the Cervical Position in the Bishop Scoring system
|
Posterior = 0
Midposition = 1 Anterior = 2 |
|
|
List the 3 types of Fetal Position
|
1. Vertex = head down
2. Breech = buttocks down 3. Transverse = neither down |
|
|
How is Fetal Position in the vertex presentation determined?
|
by palpation of the sutures & fontanelles
|
|
|
How does one identify the Anterior Fontanelle?
How does one identify the Posterior Fontanelle? |
Larger & diamond-shaped
-jxn b/w the 2 frontal bones & 2 parietal bones Smaller & more triangular-shaped -jxn b/w the 2 Parietal bones & Occipital bone |
|

Vertex presentations
|

-
|
|
|
In the setting of extensive molding of the fetal skull (Asnclitism), where the sagital suture is not midline within the maternal pelvis, palpation of what can be used to determine position?
|
Fetal Ear
|
|
|
With face presentations, what is used as the reference point?
|
Fetal chin or mentum
|
|
|
What is the reference point for Breech presentations?
|
Fetal Sacrum
|
|
|
What is the strict definition of labor?
|
regular uterine contractions that cause cervical change
|
|
|
Describe the difference b/w Induction of labor & Augmentation of labor
|
Induction = the attemp to bein labor in a NON-laboring patient
Augmentation = intervening to increase the already present contractions |
|
|
What 4 general things can labor be induced by?
|
1. Prostaglandins
2. Oxytocic agents 3. mechanical dilation of the cervix 4. Artificial rupture of membranes |
|
|
List 5 indications for induction of labor
|
1. Postterm pregnancy
2. Preeclampsia 3. Premature ROM 4. Nonreassuring fetal testing 5. Intrauterine growth restriction |
|
|
What are 2 maternal contraindications for use of Prostaglandins?
|
1. Glaucoma
2. Asthma |
|
|
What are 2 Obstetric contraindications for Prostaglandin use?
|
1. having had more than one prior C-section
2. nonreassuring fetal testing |
|
|
Induction is usually done pharmacologically with ______
How is it administered? |
Pitocin = synthetic but identical version of the octapeptide Oxytocin normally released from the Posterior Pituitary
IV since it is rapidly metabolized |
|
|
Other than Pitocin, what else can be done to induce labor? What is this? What are the precautions?
|
Amniotomy
Performed with an Amnio hook to tear the Amniotic sac around the fetus & release some of the Amniotic fluid After Amniotomy is performed, examination should be performed to ensure that prolapse of the umbilical cord has not occurred -when doing Amniotomy, it is important not to lift the fetal head b/c cord prolapse may occur |
|
|
What is the normal range for the fetal heart rate?
What should be suspected if the rate is above this range? (3) Any bradycardia of greater than what length of time & HR are of great concern? |
Normal = 110 - 160
1. Infection 2. Hypoxia 3. Anemia > 2 min & HR < 90 |
|
|
What are External Tocometers most useful for measuring?
|
FREQUENCY of contractions & comparing the fetal heart rate tracing to determine the type of decelerations occurring
|
|
|
What 4 things are considered when determining if FHT's are reassuring?
|
1. Baseline (normal = 110-160 bpm)
2. Variations from the baseline 3. there should be atleast 3-5 cycles per minute of the HR around the baseline 4. 2 ACCELERATIONS OF ATLEAST 15 BPM over the baseline that last for 15 SECONDS within 20 minutes |
|
|
Describe an Early Deceleration
What do they result from? |
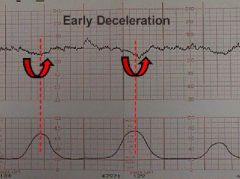
begin & end at approximately the same time as contractions
Head compression |
|
|
Describe Variable Decelerations
What do they result from? |
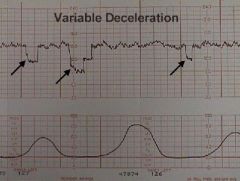
occur at any time & tend to drop more precipitously than either early or late decels
Umbilical cord compression during contractions |
|
|
Describe Late Decelerations
What are they the result of? What may they degrade into? |
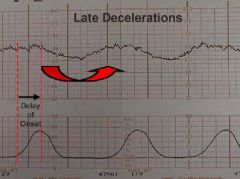
Begin at the peak of contractions & slowly return to baseline after the contraction has finished
Uteroplacental insufficiency = most worrisome type Bradycardias as labor progresses, particularly with stronger contractions |