Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
51 Cards in this Set
- Front
- Back
|
OB HPI focus on what?
|
types contraception
menstrual hx + pregnancy test sx of pregnancy |
|
|
Describe the GXpX system and give an example of twins.
|
G - # pregnancies
P - outcome of pregnancy => G1P2 is twins after birth http://en.wikipedia.org/wiki/Parity_(biology) |
|
|
TPAL system
|
When this is used drop the P term so G(x)P(tpal)
T- EDD+/-2wks P- 20wks-36wk6d A- <20wks L- Offspring living |
|
|
What is conjugate diameter
|
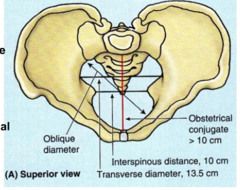
Lower pubic symphysis to sacral promontory
- palpate up & back for sacral promontory (often not felt) - Not felt then CD > length hand |
|
|
What is the approximate location of ischial spine on palpation?
|
2" into vagina at 4 & 8 O'Clock position
|
|
|
What is transverse diameter?
|
distance between ischial tuberosities
|
|
|
What questions should be asked for LMP based dating?
|
-1st day of LMP
(assess integrity of LMP dating) -Length/variability of menstrual cycles -Use of OCPs/breast feeding 6mo prior to conception |
|
|
When and where are we able to 1st hear FHT ?
|
By fetoscope - 17-20wks
By US - 12wks typically located midline through wk 28 |
|
|
What are the cut off in wks for trimesters of pregnancy?
|
1 Tri - 0-12wks (13wk)
2 Tri - 13-28wks (16wk) 3 Tri - 29-39wks (11wk) |
|
|
What is measured for dating by US in each trimester ?
|
1 Tri - crown rump length
2 Tri - biparietal diameter or femur length 3 Tri - not helpful accuracy is +/- 3wks |
|
|
What is used for dating LMP or US?
|
LMP is used unless >1wk from the US dating. Then dating is based on US
|
|
|
What constitutes referral to high risk OB?
|
-h/o preterm delivery
-h/o IUFD -h/o loss betw/ 14-20wks -multiple gestation -3rd tri bleeding or placenta previa (>26wks) -isoimmunization -h/o serious medical prob -h/o DVT or PE |
|
|
what is the ROUTINE Ob visit schedule?
|
Q4wks until 28wks
Q2wks until 36wks Q1wk until birth |
|
|
What is typical weight gain during pregnancy?
|
based on pre pregnancy BMI
0.5lb/wk until 28wks 1lb/wk after 28wks |
|
|
Why are we concerned about massive wt gain near the end of pregnancy ? Like 5lbs/wk.
|
could be a sign of pregnancy induced HTN
|
|
|
What is the general trend of BP in pregnancy? What values make us concerned?
|
Drop in 2nd Tri -AND- Rise in 3rd Tri
>140/90 concerns us >160/110 warrants emergent steps be taken |
|
|
What should be done is proteinuria is 2+ on a routine visit ?
|
Repeat with a clean catch midstream sample.
-Culture should be checked if UTI is suspected. -BP checked to r/o pregnancy induced HTN |
|
|
What should you do if urine comes back suspect for Glucose ?
|
Perform 2nd trimester DM screening earlier then normal 24-28wks
|
|
|
How should we assess edema ? Treatment ?
|
Assess
-Seen in 75% of women. No longer in triad for preg induced HTN. -Sudden onset -OR- >3lb/wk gain suspect dz process Treatment -Sitting legs up/lying down during day (often not practical) |
|
|
Why is GDM more common late in pregnancy? What was the old days outcome?
|
-Often 2y to HPL secreetion which is proportional to the wt of the placenta
-Seen in 1-2% pregnancies AND prior to use of Insulin 50% moms died |
|
|
What is screening for GDM ?
|
1H GTT - want <140mg/dl
|
|
|
What is dx for GDM ?
|
Abnormal 3H GTT
Fasting - 105mg/dl 1H - 190mg/dl 2H (drops 25) - 165mg/dl 3H (drops 20) - 145mg/dl |
|
|
What are the letter/number classifications for GDM ?
|
A1 - fasting <105mg/dl
A2 - fasting >105mg/dl B1 - fasting >130mg/dl B2 - T2DM prior pregnancy C - DM onset age 10-19 D - DM onset prior age 10 -OR- >20y F/R/H - w/ nephropathy/retinopathy/heart probs |
|
|
Relationship of GDM and T2Dm ?
|
about 50% of GDM will develop T2DM later in life. Recommend screening.
|
|
|
24-28wk screening tests ?
|
CBC for Hct
-Anemia defined as <11mg/dl in trimesters 1-2 -AND- <10.5 in 3rd trimester |
|
|
Rh negative mothers when recieve RhoGam ?
|
28wks given to prevent Hemolytic Disease of Newborn for subsequent Rh+ babies
-Given for any procedure like amniocentesis/post-partum/abortion |
|
|
Why is Rubella iGG routinely measured ?
|
Often the German Measls dz is subclinical but may cause cataracts, cardiac defects, deafness in the fetus
|
|
|
What is tx for reducing vertical transmission of HIV ?
|
14-34wks initiate ZDZ 100mg 5/day + IV during labor + 6wks treat baby
|
|
|
Why screen for HBV ?
|
Vertical transmission can be decreased.
90% transmission rate when mom + E Ag -AND- S Ag reduced to 10% with IVIG in newborn -AND- starting HBV vaccines early in child |
|
|
When and why screen mAFP levels ?
|
15-20wks gestation
-Higher then expected levels = open NT defect/ IUFD = incorrect gestational age = twins -Lower then expected =chromosomal abnormalities (downs syn.) |
|
|
What is the f/u to abnormal QUAD screen ?
|
Gestational age/twins confirmation by US
Remains abnormal - amniocentesis + genetic screening + US for anomalies |
|
|
What is time frame for amniocentesis ?
|
Performed betw/ 14-18wks
Take 2-3wks culturing to et enough mass for Karyotype analysis |
|
|
What is CVS ?
|
Chorionic Villous Sampling
-10-12 wks (earlier then amniocentesis) - Fetal karyotype ascertained - Does NOT screen for NT defects - Slightly higher risk for loss pregnancy/limb reduction abnormalities compared to amniocentesis |
|
|
What is the indication for a NST ?
|
Decreased fetal movement after 28wks
|
|
|
What STI's should be screened for? Treatments?
|
Chlamydia, Gonnorhea - Erythromycin
Metronidazyl after 1st trimester |
|
|
What Abxs should be avoided in pregnancy?
|
-Sulfa near birth - displace bilirubin from carrier resulting in kernicterus
-Tetracycline - teeth discoloration -Nitrofuratoin - worsens hemolytic anemia |
|
|
What are the signs of labor?
|
>24wks
>4ctx/hr with pain for 2H or more |
|
|
What is round ligament pain?
|
Tender on lateral aspects Uterus
Roughly correlates to location of round ligament Tx - tylenol and heating pads |
|
|
Leg cramps
|
want to r/o DVT
-unilateral, erythema, painful swelling |
|
|
Pregnancy circulation obstruction?
|
Observed during labor but NOT prior to this time. Ok to sleep on your back
|
|
|
What is critical in L&D triage ?
|
-EGA if >36wks shouldn't be serious
-Presenting complaint MC are SROM + Contractions |
|
|
How determine if SROM and f/u questions?
|
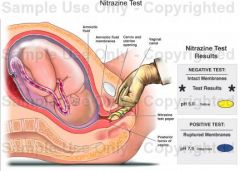
+Fern test
Positive Nitrazine test + when pH is 7.1 to 7.4. 90% women have acidic urine (10% FP from urine) - Ask about quality (meconium/clear) |
|
|
What does active labor include?
|
-Contractions
-Dilation of cervix -Effacement |
|
|
What is Friedman's curve?
|
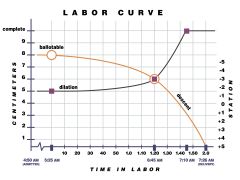
Not used for detail level but gives sense of progression
|
|
|
What divides 1st and 2nd stage of labor ?
|
Complete dilation marks end of the 1st stage and beginning of 2nd stage
|
|
|
How is the 1st stage of labor divided?
|
Often hard to differentiate in real time. Shift occurs when dilation rate increases. Generally occurs around 4cm
Latent - Cervical change w/ regular ctx Active - Rapid cervical change w/ regular ctx |
|
|
What marks beginning and end of 3rd stage of delivery?
|
3rd stage - ma take up to 30min
-Beginning = birth of baby -End = delivery of placenta |
|
|
What are majority fetal orientations and presentations?
|
96% are Vtx (head first)
95% are OA (looking at the ground) |
|
|
What is slang for OP?
|
Sunny side up - since looking up to mom's urethra
-labor is prolonged -May have more back pain |
|
|
How long from time 100% effacement to delivery?
|
This is stage 2 of labor and timing depends...
Primnup - 2.9H Multip - 1.1H |
|
|
How long is active labor ?
|
This is a portion of stage 1 of labor. Time depends but generally about 50% of latent labor. Multips are typicall about half the time for stage 1 labor.
Primnup - 11.7H active labor Multip - 5.2H active labor |