Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
177 Cards in this Set
- Front
- Back
|
what are the circulatory changes once baby is born?
|
the three shunts ductus arteriousus, ductus venous and foramen oval functuionnaly close during a newborns transition to extrauterine life with the flow of the oxygenated blood in the lungs and readjustment of atrial blood pressure in the heart
|
|
|
what do the scores mean for apgar not the actual scale
|
once in 1 min and then once 5 min of life
o-3 indicates severe distress 4-6 indicates moderate distress 7-10 indicates no distress |
|
|
the actual scoring of the apgar what it is?
|
HR: 0: absent, 1: less than 100, 2: greater than 100
RESP: 0 absent, 1: slow weak cry, 2: good cry MUSCULE TONE: 1: flaccid, 2: some flexion, 3: well- flexed REFLEX IRRITABILITY: 1: none, 2: grimace, 3: cry COLOR: 1: blue pale, 2: pink body cyanotic hands and feet ( acrocyanosis), 3: completely pink |
|
|
wbat euipment do you need for a newborn assessment?
|
bulb syringe: WHY? for suctioning excess mucus from mouth and nose
stethoscope: why ? used evaluate HR, breath sounds and bowel sounds axillary thermometer: WHY? to monitor temperature and prevent hypothermia, rectal emp are avoided WHY? Because it can injure rectal mucosa, initial rectal temp can be used to see if they have any rectal anomalies blood pressure cuff 2.5 cm WIDE: WHY? palpation or electronic mthord, it can be done in all four extremities if evaluating the newborn for cardiac problems tape measure in CM: WHY? measure from crown to hell of foot for length measure head circumference at greatest diameter from occipital to frontal, measure the chest from beginning of the nipple line and abdominal circumference above the umbilicus clean gloves: worn for all physical assessment until discharge |
|
|
what do you check for if your doing an quick assessment?
|
external assessment: Skin color, peeling, birthmarks, foot creases, breast tissue, nasal patency, and meconium staining (may indicate fetal hypoxia)
Chest – Point of maximal impulse location, ease of breathing, auscultation for heart rate and quality of tones and respirations for crackles, wheezes, and equality of bilateral breath sounds ◯ Abdomen – Rounded abdomen and umbilical cord for one vein and two arteries ◯ Neurologic – Muscle tone and reflex reaction (Moro reflex); palpation for the presence and size of fontanels and sutures; assessment of fontanels for fullness or bulge ◯ Other observations – Inspection for gross structural malformations |
|
|
why is the ballard scale important and what are the ranges for it?
|
estimation of gestation age and a baseline to asses growth and development Neonatal morbidity and mortality are related to gestational age and birth weight.
■ Weight – 2,500 to 4,000 g ■ Length – 45 to 55 cm (18 to 22 in) ■ Head circumference – 32 to 36.8 cm (12.6 to 14.5 in) ■ Chest circumference – 30 to 33 cm (12 to 13 in) |
|
|
whats the new abllard scale
|
newborn maturit rating scale that asses neuromuscular and physical maturity, each individual parameter displays at least six ranges of development along a continuum they are from -1 to 5, then those are added to see if they are mature or not so a score of 35 me ands that they are 38 weeks of gestation
|
|
|
neuromusuclar matturity asseses:
|
Posture ranging from fully extended to fully flexed (0 to 4).
☐ Square window formation with the neonate’s wrist (-1 to 4). ☐ Arm recoil, where the neonate’s arm is passively extended and spontaneously returns to flexion (0 to 4). ☐ Popliteal angle, which is the degree of the angle to which the newborn’s knees can extend (-1 to 5). ☐ Scarf sign, which is crossing the neonate’s arm over the chest (-1 to 4). ☐ Heel to ear, which is how far the neonate’s heels reach to her ears (-1 to 4). |
|
|
ohysical maturity asseses:
|
☐ Skin texture, ranging from sticky and transparent, to leathery, cracked, and wrinkled (-1 to 5).
☐ Lanugo presence and amount, ranging from none, sparse, abundant, thinning, bald, or mostly bald (-1 to 4). ☐ Plantar surface creases, ranging from less than 40 to 50 mm to creases over the entire sole (-1 to 4). ☐ Breast tissue amount, ranging from imperceptible, to full areola with a 5 to 10 mm bud (-1 to 4). ☐ Eyes and ears for amount of eye opening and ear cartilage present (-1 to 4). ☐ Genitalia development, ranging from flat smooth scrotum to pendulous testes with deep rugae for males (-1 to 4), and prominent clitoris with flat labia to the labia majora covering the labia minora and clitoris for females (-1 to 4). |
|
|
after the physical assessment the classification of the newborn gestation age and birth weight is then detmeined by? age, sag, lag, lbw, igur, term, preterm posers, post mature
|
Appropriate for gestational age (AGA) – Weight is between the 10th and 90th percentile.
■ Small for gestational age (SGA) – Weight is below the 10th percentile. ■ Large for gestational age (LGA) – Weight is above the 90th percentile. ■ Low birth weight (LBW) – Weight of 2,500 g or less at birth. ■ Intrauterine growth restriction (IUGR) – Growth rate does not meet expected norms. ■ Term – Birth between the beginning of week 38 and prior to the end of 42 weeks of gestation. ■ Preterm or premature – Born prior to the completion of 37 weeks of gestation. ■ Postterm (postdate) – Born after the completion of 42 weeks of gestation. ■ Postmature – Born after the completion of 42 weeks of gestation with evidence of placental insufficiency. |
|
|
in what order are vial signs checked?
|
Vital signs are checked in the following sequence: respirations, heart rate, blood pressure, and temperature. The nurse observes the respiratory rate first before the newborn becomes active or agitated by use of the stethoscope, thermometer, and/or the blood pressure cuff.
|
|
|
what are the norma parameters for the vital signs for RESP
|
resp rate: 30-60 with short periods of apnea less than 15 seconds, during REM sleep, crackles and wheezing are symptoms of infection in the lungs grunting and nasal flaring are signs of resp distress
|
|
|
normal parroters for heart rate
|
heart rate should be 100 to 160 min with brief fluctuations above and below the range depending on the activity like if the baby is crying or sleeping, pulse rate is assessed for a a full minute, the pediatric stethoscope head is placed on the fourth or fifth intercostal space at the left midclavicular line over the apx of the newborns heart, HR murmurs should be documented
|
|
|
normal parameters for blood pressure
|
should be 60 to 80 mmhg systolic and 40 to 50 mmhg diastolic
|
|
|
normal parameters for temperature
|
temperature should be 36.5 to 37.2 axillary or 97.7 to 98.9 F
* newborn at risk for hypothermia and hyperthermia until thermoregulation * if baby is cold--> o2 demands increase--> acidosis |
|
|
physical assessment after being born
|
more extensive physical assessment after being born in 24 HOURS
HEAD TO TOE posture: lying in curled up position with arms and legs in moderate flexion resitant to extension of extremities skin: should be pink or acrocyantic with no jaundice present on the first day third day---> bilirubin--> jaundice--> then decreases skin turgor: present, spring back immediately when pinched texture: should be dry, soft, smooth, showing good hydration, cracks may be present, newborns--> desquamation peeling occurs a few days after birth vernix caseosa : protective, thick, cheesy covering amounts vary with more present in creases and skin folds lanugo: fine downy hair varies regarding the amount present, found in pinnas, forehead, and shoulders |
|
|
what are some normal skin deviations when doing the head to toe assessment?
|
milia--> small raised white spots on the nose chin and , these spots disappear spent. --> tell parents not squeeze spots
mongolian sports: bluish purple sports of pigmentation are on shoulders, back, buttocks, sports are frequently present on newborns who have dark skin telangiectacti nevi ( stork bites): are flat pink or red marks easily blanch are found on the back of the neck, nose, upper eyelids, and middle of the forehead ---> fade by second year nevus flammeus (port whine) capillary angioma below the surface of the skin that is purple or red, commonly seen on face--> does not blanch or disappear - erthema toxic ( erythema neonatorum) a paink rash appears suddenly anywhere on the body of term newborn in the first---> no treatment is required |
|
|
what are you looking for when assesing the nose?
|
- midline flat and board with lack of a bridge
- some mucus should be present with no drainage - newborns --> nose breathers--> even with obstruction --> after 3 weeks than open mouth - newborns sneeze to clear nasal passages |
|
|
what are you asseing for when looking at the mouth
|
Assess for palate closure and strength of sucking.
■ Lip movements should be symmetrical. Saliva should be scant. Excessive saliva may indicate a tracheoesophageal fistula. -Epstein’s pearls (small white cysts found on the gums and at the junction of the soft and hard palates) are expected findings. They result from the accumulation of epithelial cells and disappear a few weeks after birth. - tongue should move freely symmetrical in shape, not protude--> protruding? sign of down syndrome - soft and hard palate should be intact - gums and tongue should be pin, gray white patches on the tongue and gyms can indicate thrush a fungal infection caused by candida albicans---> from mom vaginal secretions |
|
|
normal assessment of the neck
|
■ Neck should be short, thick, surrounded by skin folds, and exhibit no webbing.
■ Neck should move freely from side to side and up and down. ■ Absence of head control may indicate prematurity or Down syndrome. |
|
|
normal assessment of the chest
|
■ Chest should be barrel-shaped.
■ Respirations are primarily diaphragmatic. ■ Clavicles should be intact. ■ Absence of retractions. ■ Nipples should be prominent, well formed, and symmetrical. ■ Breast nodule should be approximately 6 mm. |
|
|
normal assessment of the abdomen
|
◯ Abdomen
■ Umbilical cord should be odorless and exhibit no intestinal structures. ■ Abdomen should be round, dome-shaped, and nondistended. ■ Bowel sounds should be present 1 to 2 hr following birth. |
|
|
assessment of the anogenital
|
■ Anus should be present, patent, and not covered by a membrane.
■ Meconium should be passed within 24 hr after birth. ■ Genitalia of a male newborn should include rugae on the scrotum. ■ Testes should be present in scrotum. Male urinary meatus is located at penile tip. ■ Genitalia of a female should include labia majora covering the labia minora and clitoris, and are usually edematous. ■ Vaginal blood-tinged discharge may occur in female newborns, which is caused by maternal pregnancy hormones. This is an expected finding. ■ A hymenal tag should be present. ■ Urine should be passed within 24 hr after birth. Uric acid crystals will produce a rust color in the urine the first couple of days of life. |
|
|
when checking for extremities and spine
|
Assess for full range, symmetry of motion, and spontaneous movements.
■ Extremities should be flexed. ■ Assess for bowed legs and flat feet, which should be present because lateral muscles are more developed than the medial muscles. ■ No click should be heard when abducting the hips. ■ Gluteal folds should be symmetrical. ■ Soles should be well-lined over two-thirds of the feet. ■ Nail beds should be pink, and no extra digits are present. ■ Spine should be straight, flat, midline and easily flexed. |
|
|
reflexes you better know this lol
|
sucking and rooting reflex: birth to 4 months touch the side of the mouth and see if the want to suck
palmar grasp: birth to 6 months put something in they palm, will grab it plantar grasp: birth 8 months toes touched curled downward moro reflex: birth to 4 months arms legs extrand and abduct while fingers spread to, happens--> lying sitting in semipostion startle reflex: birth to 4 months make a loud noise tonic neck reflex: birth to 3 or 4 months extends arm and leg on the side the head is turned and flexed on the opposite side babinskine reflex: stroking outer edge of the sole of the foot, moving up toward toes, toes will fan upward and out - stepping: elected by holding the newborn upright with feet touching a flat surface, newborn responds with stepping movements -- birth to 4 months |
|
|
senses of physical ssesemnt vision
|
visionL should be able to focus on objects 9 to 12 inches away from face, same distance as mothers face when the newborn is breastfeeding, eyes are sensitive to lint, therefor dim light, pupils--> reactive to light, and then blink reflex is easily stimulated, newborn can track high contrast objects and prefers bright colors and patterns
|
|
|
senses hysical assessment what are you looking for inhering touch, taste, smell, habitation?
|
hearing: similar to adult once the amniotic fluid drains form the ears, newborns exhibit selective listening to familiar voices and rhythms of intrauterine life
touch: responds to tactile messages of pain and touch, mouth is the area most sensitive to touch in the newborn taste: can taste and prefers sweets over salty, sour, bitter smell: highly developed sense of smell, prefer sweet smells and regonize smell of mother habitation: protective mechanism--> environmental stimuli, repetitive or constant stimuli--> decreased, promotes continued learning avoiding overload |
|
|
what are the diagnostic and therapeutic procedures following birth?
|
*umbilical cord blood is collected during birth to determine ABO blood type and RH status if the mothers blood type is O or is she RH negative. a cvc may be done by a capillary stick to evaluate for amenia, polcycrthemia, infection, or clotting problems, and hypoglycemia
|
|
|
what are the expected lab values
|
hgb 14 to 24 g/dl
HCT 44% to 64% RBC COUNT 4800 to 7.1 million leukocytes 9000 to 30000 platelets 150000 to 300000 glucose 40 to 60 bilirubin 0-6 on day 1, 8mg or less on day 2, and 12 mg or less on day 3 |
|
|
what are some complications that can happen during postpartum period to the baby
|
airway obstruction--> mucus
--> mouth or nose are suctioned with a bulb syringe, gentle percussion over the chest can help loosen secretions hypothermia--> monitor for an axillary temperature of less than 36.5 C 97.7 F - if temp is unstable place the newborn in a radiant warmer, maintain skin temperature at approx 36.5, 97.7 - asses axillary every hour if temp is unstable - all exams should be done under a radiant warmer inadequate oxygen supple---> poorly functiioning cardiopulmonary system, obstructed airway - monitor resp and skin color for cyanosis - stabilize body temp or clear airway administer oxygen prepare for resuscitation |
|
|
how often should vital signs be checked
|
every 30 min x2, every 1 hr x 2, and then every 8 HR
|
|
|
what are the physical assessment your gonna do like a fast one what do look for
|
weight should checked daily at the same time
inspect the clients umbilical cord and observe for any bleeding from the cord and ensure that the cord is clamped to prevent any hemorrhage - in the first 6-8 hours of life as body systems stabilize and pass through periods of adjustment observe for periods of reactivity |
|
|
first period of reactivity
|
first period of reactivity: the newborn is alert, exploring activity, makes sucking sounds, rapid heart rate, and resp rate
HR: 160 to 180 min, but will stabilize to 100 to 120 during a period that lasts 15 to 30 min after birth |
|
|
period of relative inactivity
|
the newborn will become quiet and begin to rest and sleep the HR and resp will decrease and this period will last from 30 min to 2 hours after birth
|
|
|
second period of reactivity
|
when the newborn reawakens it becomes responsive again, and often gags and chokes on mucus in mouth, this period occurs 2-8 hours after birth and may last 10 min to several hours
|
|
|
using facility pain assessment tool
|
do a pain assesment on the newborn every 8-12 hour and following painful procedures
|
|
|
lab tests ordered after birth
|
hgb, HCT, blood glucose for hypoglycemia, metabolic screening
|
|
|
newborn genetic screening
|
newborn genetic screening is mandated in all states, a capillary heel stick should be done 24 hours following birth, for results to be accurate the newborn must have received formula or breast milk for at least 24 hours, if newborn is dischargeed before 24 hour the test should be done in 1 or two weeks
|
|
|
pku testing
|
all states require PKU testing--> defect in protein metabolism in which the accumulation of amnio acid phenyl aline can result in mental retardation
|
|
|
what are other tests that can be done besides heels tsick and PKU
|
galactosemia, cystic fibrosis, maple syrup urine disease, hypothyroidism, and sickle cell disease, hearing--> mandatory
|
|
|
how to collecting blood samples
|
heel stick blood samples are obtained by the nurse---> clean gloves
- warm newborn heel first to increase circulation - clean the area with an appropriate antiseptic and allow for drying -a spring activated lancet is used to that the skin incision is made quickly and painlessly - the outer aspect of the heel should be used and the lancet should go no deeper than2.4 mm to prevent nectrozing osteochondritis - apply pressure with dry gauze--> DO NOT USE USE ALCOHOL BECAUSE IT WILL CAUSE BLEEDING TO CONTINUE, UNTIL BLEEDING STOPS COVER WITH ADHEVSIVE - cuddle and comfort the newborn when the procedure is completed |
|
|
patient centered care as a nurse what can you do and asses for? when the newborn has resp complications
|
◯ Stabilize and/or give resuscitation to the newborn.
◯ Monitor for signs and symptoms of respiratory complications. ■ Bradypnea – respirations less than 25/min ■ Tachypnea – respirations greater than 60/min ■ Abnormal breath sounds – expiratory grunting, crackles, and wheezes ■ Respiratory distress – nasal flaring, retractions, grunting, and labored breathing |
|
|
what interventions can you do as nurse if the the newborn needs stabilization and resuscitation of airway
|
the newborn is able to clear most secretions in the air passages by cough reflex---> routine suctioning of the mouth first, then nasal passages with bulb syringe to remove excess mucus in the resp tract
---> if unsuccessful--> mechanical suction or back blows and chest thrusts may be used ---> compress bulb before insertion into one side of the mouth--> avoid center of the mouth to prevent stimulating gag reflex ---> aspirate mouth first, one nostril then second nostril |
|
|
safety idenfitcation band
|
mom has one newborn has one
- finger and foot prints - alarm sound - ID |
|
|
thermoregulation REASon WHY
|
neutral thermal environment that helps a newborn maintain a normal core temperature with minimal oxygen consumption and caloric expenditure
WHY DO NEWBORNS GET COLD SO FAST? - large surface to weight ration, reduced metabolism per unit area, blood vessels closer to the surface, and small amounts of insulation - newborn keeps warm by metabolizing brown at - becoming bold can increase the newborns oxygen demands and rapidly use up fat reserves |
|
|
whne monitoring for hypothermia what are you checking for?
|
☐ Axillary temperature of less than 36.5° C (97.7° F)
☐ Cyanosis ☐ Increased respiratory rate |
|
|
what are some nursing interventions to maintain thermoregulation
|
☐ Core temperature varies within newborns, but it should be kept around 36.5° C (97.7° F).
Heat loss occurs by four mechanisms: |
|
|
heat loss conduction
|
loss of body heat resultg from direct contact with a cooler surface
intervetions: preheat radiant warmers warm a stethoscope and other instruments - pad a scale before weighing the newborn - place newborn on womans abdomen with blanket |
|
|
heat loss convection
|
flow of the heat from the body surface to cooler environmental air
interventions: place the bassinet out of direct line of a fan or air conditioning - swaddle the infant in blanket - keep head covered - all procedures should be done under the radiant warmer |
|
|
heat loss: evaporation
|
loss of heat as surface liquid is converted to vapor
intervetnions: gently rub the newborn with a dry warm sterile blanket - if temp unstable--> postpone the initial bath until the newborns skin ten is 36.5 C 97.7 F - when bathing expose only one part of the body in a timely manner |
|
|
heat loss radiation
|
loss of heat from the body surface to a cooler solid surface that is close but not in direct contact
interventions: keep the newborn and examine tables away from windows and air conditioners temperatures stabilizes at birth within 4 hours after birth if chilling is prevented |
|
|
bathing can begin once the newborns temp has stabilized
|
complete sponge bath should be given within the first 1 to 2 hours after birth under a radiant heat source to prevent heat loss
- gloves should be worn until newborn first bath to avoid exposure to body secretions |
|
|
feedings following immediately after birth
|
Breastfeeding is initiated as soon as possible after birth as part of baby-friendly initiatives.
■ Formula feeding usually is started at about 2 to 4 hr of age. A few sips of sterile water may be given to assess sucking and swallowing reflexes and ensure that there are no anomalies, such as a tracheoesophageal fistula, prior to initiating formula. ☐ The newborn is fed on demand, which is normally every 3 to 4 hr for bottle-fed newborns and more frequently for breastfed newborns. |
|
|
sleep wake estates
|
* variation sof consciousness in the newborn of six states: deep sleep, light sleep, drowsy, quiet alert, active alert, and extreme irritability (crying).
- newborns sleep approx 17 hours a day an average of 4 hors at a time - newborns should be supine--> SIDS - no bumper pads, loose linels, toys--> bassinet - mothers should sleep in close proximity but not in a shared space |
|
|
elmiantion habits
|
newborns should void once within 24 hours of birth, they should void 6 to 19 times a day after 4 days of life
- meconium should be passed within the first 24 hour after birth - newborn--> 3 or 4 stools a day depending on whether day are breastfed or not - stools are lighter in color and looser than stools of newborns who are formula fed |
|
|
output
|
keep the perineal area clean and dry
WHY? ammonia--> diaper rash - after each diaper change cleanse the perineal area with clear water or water with a mid soap---> no alcohol wipes should be used - pat dry and apply triple antibiotics ointment, pretoluem jelly, zinc oxide, |
|
|
before entering the unit its important to do what?
|
* HANDWASH *
All personnel caring for a newborn should scrub with antimicrobial soap from elbows to finger tips before entering the nursery. In between care of the newborn, the nurse should follow facility hygiene protocols. Cover gowns or special uniforms are used to avoid direct contact with clothes. |
|
|
what are some medications that we are going to give etheromycin WHY
|
prophylactic eye care
- mandatry antibiotic ointment into the eyes to prevent ophthalmia neonatorum - infections tranmistted from birth canal - optherlamia neonatorum---> gonorrhoeae or Chlamydia nursing interventions: erthymocyin or tetracycline - use single dose to avoid cross contimation - apply 1 to 2 cm ribbon of ointment to the lower conjuctival sac of each eye starting from the inner can thus and moving outward side effect is chemical conjunctivitis, causing redness, swelling, drainage, and temporarily blurred vision for 24 to 48 hr---> will resolve |
|
|
vitamin K adminsitration
|
■ Administered to prevent hemorrhagic disorders. Vitamin K is not produced in the gastrointestinal tract of the newborn until around day 8. Vitamin K is produced in the colon by bacteria that forms once formula or breast milk is introduced into the gut of the newborn.
■ Nursing Considerations and Client Education ☐ Administer 0.5 to 1 mg IM into the vastus lateralis (where muscle development is adequate) within 1 hr after birth. |
|
|
hep B immunixzation
|
Recommended to be given to all newborns; informed consent must be obtained.
☐ For newborns born to healthy women, recommended dosage schedule is at birth, 1 month, and 6 months. ☐ For women infected with hepatitis B, hepatitis B immunoglobulin (HBIG) and the hepatitis B vaccine is given within 12 hr of birth. The hepatitis B vaccine is given alone at 1 month, 2 months, and 12 months. ☐ It is important NOT to give the vitamin K and the hepatitis B injections in the same thigh. Sites should be alternated. |
|
|
topical antimicrobial therapy
|
may be used for prevention of infection and promote during of the umbilical cord stump
nursing interventons ☐ Assess stump and base of cord for edema, erythema, and drainage with each diaper change. - care for the for cord as prescribed by the provider, triple dye or cleanse with neutral ph cleanser and sterile water - bathing infant by submerging water---> NOT ALLOWED UNTIL IT FALLS OFF |
|
|
complications thermoregulation
|
can lead to hypoxia, acidosis, and hypoglycemia.
-■ Monitor for manifestations of cold stress (cyanotic trunk, depressed respirations). ■ The newborn should be warmed slowly over a period of 2 to 4 hr. Correct hypoxia by administering oxygen. Correct acidosis and hypoglycemia. |
|
|
what do if the newborn has hypoglycemia
|
occurs from few hours of life secondary to the use of energy to establish respirations and maintain body heat
- newborn of mothers who diabetes -LGA - nursing actions: ■ Monitor for jitteriness; twitching; a weak, high-pitched cry; irregular respiratory effort; cyanosis; lethargy; eye rolling; seizures; and a blood glucose level less than 40 mg/dL by heel stick. ■ Give formula immediately or have the mother breastfeed to elevate blood glucose. Brain damage can result if brain cells are depleted of glucose. |
|
|
hemorrhage can occur WHY?
|
due to improper cord care or placement of clamp
Nursing Actions ■ Ensure that the clamp is tight; if seepage of blood is noted, a second clamp should be applied. ■ Notify the provider if bleeding continues. |
|
|
newborn weight loss and gain
|
› Loss of 5% to 10% immediately after birth (regain 10 to 14 days after birth) › Gain of 110 to 200 g/week for first 3 months
|
|
|
how much nutrition do newborns need
|
fluid intake 100 to 140 ml/kg/24 HR
- NO WATER - for the first 3 months the newborn needs 110 kcal/kg/day from 3 to 6 moths the requirement decreases to 100 kcal/kg/ day both great and milk formula provide 20 kcal/oz - carbs: 40% to 50% of the newborns total caloric inane - 15% must come from fat - need 2.25 to 4g/kg of protein a day |
|
|
breast milk
|
contains the vitamins necessary to provide adequatee nutrition
- 400 IU of vitamin D in the first week of life - infant formula has vitamins added to the formulation - vitamin D supplements are recommended vitamin B 12---> mothers who are breastfeeding and exclude meat, fish, and dairy products |
|
|
iron
|
iron is low in all forms of milk, but absorbed better from breast milk
- newborns breastfed for the first 6 months--> adequate hgb levels and do not need any additional iron supplementation - after 6 months of age all newborns are fed iron fortified cereal and other foods - newborns whoa re formula fed should receive iron fortified newborn formula until 12 months of age - mothers who breastfeed their newborns are encouraged to do for the newborns first 12 months of life |
|
|
fluoride levels
|
low--> if not in water should be given a fluoride supplement
|
|
|
when are solis introduced?
|
6 MONTHS OF AGE! IF EARLIER FOOD ALLERGIES CAN DEVELOP
|
|
|
BREASTFEDDING
|
should be optimal source of nutrition for the first 6 months of life
- newborns should be breastfeed every 2 or 3 hours - paretns should try to feed at least every 3 hours during the day and at least 4 hours during the night until the newborn is feeding well and gaining weight - breastfeeding --> 8 to 12 times a day |
|
|
colosturm
|
secreted from the mothers breast during postpartum days 1 to 3 it contains the IGA immunoglobulin that provides passive immunity to the newborn
|
|
|
nursing intervetnipns for beastfeding
|
provision of adequate calories and fluids to support breastfeeding
- rooming in allowing mothers and newborns to remain together - lactation consultants |
|
|
what are the advantages of breastfeeding?
|
******IMPORTANT*********
- reduces infection how? --? provides ig A antibodies, lysozymes, leukocytes, macrophages, and lactoferrin that prevents infections. - promotes rapid brain growth due to large amounts of lactose - provides protein and nitrogen for neuolrogical cell bulling and improves the newborns ability to regulate calcium and phosphorus levels - contains electrolytes and minerals - breast milk is easy for newborns to digest - breastfeeding is convenient and inexpensive - reduces incidence of SIDS allergies and childhood obesity - promotes maternal infant bonding |
|
|
nrusing interventions to promote successful breastfeeding
|
place the newborn skin to skin on the mothers abdomen immediately after birth
- initiate breastfeeding as soon as possible within the first 30 min following delivery - explaiin breastfeeding techniques to the mother---> wash hands before - don't drink alcoholic drinks or caffeine drinks - explain let down reflex stimulation of maternal nipple releases oxytocin that causes the let down of milk - reasure the mother that uterine cramps are normal--> oxytocin - express a few drops of colostrom or milk and spread it over the nipple to lubircate the nipple and entice the newborn - show mother proper latch on position |
|
|
how to properly latch one
|
- have her support breast in one hand with the thumb on top and four fingers underneath
- with the newborns mouth in from of the nipple the newborn can be stimulated to open his mouth by tickling his lower lip with the top of the nipple - the mother pulls the newborn to the nipple with his mouth covering part of the areola as well as the nipple - when the newborn is latched on when nose, cheeks and chin will be touching the breast |
|
|
what are the four breastfeeding positions
|
football, cradle or modified cradle, across the lap, and side lying
|
|
|
bhow long should the mother breastfeed for?
|
15 to 20 min per breast to ensure that the newborn receives adequate fat and protein which is richest in the breast milk as t empties the breast
but don't set a time for the mother sings that the newborn doesn't want to eat anymore: slowing of the newborn sucking, softened breast, sleeping will nurse one demand |
|
|
insert a finger, burp, next feeding, how many diapers, soots, pacifiers
|
- show mother how to insert a finger in the side of the newborns mouth to break the suction from the nipple prior to removing the newborn from the breast to prevent nipple trauma
- how to burp: burped either over the shoulder or in an upright position with his chin supported the mother should gently pat the newborn on his back to elicit a burp - tell the mother to begin the newborns next feeding with the breast she stopped feeding him with the previous feeding - tel the mother how to tell if her newborn is receiving adequate feeding---> 6 to 8 wet diapers a day - explain to mother that the newborn may have loos, pale, or yellw stools--> breastfeeding - tell mother to avoid nipple confusion in the newborn by not offering supplemental formula pacifier or soothers, supplementation can be provided using a small ending or syringe feeding if needed |
|
|
herbal producets
|
fenugreek
- metoclopramide reglan have reported to increase breast milk production - thee is insufficient at a to confirm or deny their effect on lactation |
|
|
breat puomp
|
Breast pumps can be manual, electric, or battery-operated and pumped directly into a bottle or freezer bag.
■ One or both breasts can be pumped, and suction is adjustable for comfort. |
|
|
how can you stow breast milk?
|
can be stored in room temp for up to 8 hour maybe in bottles for 8 days or may be frozen in sterile containers in the freezer compartment of a two door refrigerator for up to 6 months
- breast milk may be stored in a depp freezer for 12 months -thawing milk best way to preserve the immunoglobins present in it --> DO NOT MICROWAVE because it destroyed the immune factors lysozmes contained in the milk |
|
|
botle feeding
|
teach parents to wash before after
- can be refrigerated for up to 48 hours - flow of formula its not too fast or too slow - show parents how to cradle the newborn arms in semi upright position best angle 45 degrees - nipple should be under the newborns tongue - keep the nipple filled with formula to prevent the newborn from swallowing air - always hold the bottle and never proper the bottle for feeding - newborns should be burped several during a feeding after 1/2 to 1 oz of formula or breast milk - always keep the bottle nipple filled on top because it prevents the newborn from swallowing air - should be voiding 6-8 times per day, and 1-2 bowel movements |
|
|
risk factors for failure to thrive
|
Inadequate breastfeeding
■ Illness ■ Infection ■ Malabsorption ■ Other conditions that increase the newborn’s energy needs |
|
|
matneral factors that causes the newborn not be able to breastfeeding right
|
Inadequate or slow milk production
■ Inadequate emptying of the breast ■ Inappropriate timing of feeding ■ Inadequate breast tissue ■ Pain with feeding ■ Maternal hemorrhage ■ Illness ■ Infections |
|
|
weights are done dily in the newborn
|
usually at 2 days of age after discharge for newborns who are breastfed and 6 weeks of age for newborns who are formula fed, growth is assessed by placing the newborns weight on a growth chart, adequate growth should be within 10 to 90 percentile
|
|
|
newborn reasons why she wouldn't want to breastfeed
|
■ Maturity level
■ History of labor and delivery ■ Birth trauma ■ Maternal risk factors ■ Congenital defects ■ Physical stability ■ State of alertness ■ Presence of bowel sounds ***ALWAYS CALCULATE THE NEWBORN 24 HOUR I AND O****** |
|
|
maternal resons not to breastfeed
|
■ Previous experience with breastfeeding
■ Knowledge about breastfeeding ■ Cultural factors ■ Feelings about breastfeeding ■ Physical features of breasts ■ Physical/psychological readiness ■ Support of family and significant others |
|
|
INTERVENING FOR NWBORN NITRITINON WHAT ARE are some cues
|
Hand-to-mouth or hand-to-hand movements
◯ Sucking motions ◯ Rooting ◯ Mouthing |
|
|
what are the complications for newborn nutrition of those who are sleepy
|
■ Unwrap the newborn.
■ Change the newborn’s diaper. ■ Hold the newborn upright and turn him from side to side. ■ Talk to the newborn. ■ Massage the newborn’s back, and rub his hands and feet. ■ Apply a cool cloth to the newborn’s face. |
|
|
complications of breastfeeding for newborns whoa re fussy
|
Swaddle the newborn.
■ Hold the newborn close, move, and rock him gently. ■ Reduce the newborn’s environmental stimuli. ■ Place the newborn skin to skin. |
|
|
complications of those infants who are failure to thrive a slow eight gain what can you do?
|
■ Evaluate positioning and latch-on during breastfeeding.
■ Massage the breast during feeding. ■ Determine feeding patterns and length of feedings. - if the newborn is spitting up he or she maybe allergic to diary products ( mother might need to get rid of diary products, if newborn is spitting up or vomiting he may have an allergy or interlace to cow milk based formula and require soy based formula |
|
|
how soon can a mother in postpartum be discharged?
|
6 to 48 hour hold * but you gotta give serious discharge teaching
|
|
|
assessment of the family's readiness to care for the newborn at home
|
previous newborn experience and knowledge
- parent newborn attachment - adjustmnet to the parental role - social support - educational needs - sibling rivalry issues - readiness of the parents to have their home and lifestyle altered to accommodate their newborn - parents ability to verbalize and demonstrate newborn care following teaching |
|
|
aha tot teach parents about crying
|
newborns cry: when hungry, need to be burped, overstimulated, wet, cold, hot, tired, or bored
- do not feed baby every time he or she cries, overfeeding can lead to stomach aches and diarrhea |
|
|
how to quite a infant
|
-swaddle
-close skin contact -nonnutritive sucking with pacifier -rhythmic noises to stimulate utero sounds -movements -placing the newborn on stomach across a holders lap while gently bouncing legs - enface postion for eye contact - stimulation |
|
|
sleep wake cycle
|
- reinforce the parents placing the newborns in supine position for sleeping greatly decreases the risk of sids
- most newborns sleep 17 out of every 24 hour periods of wakefulness - don't add solids to the baby diet for 6 months because it will not help newborn sleep better - by 4 to 5 months newborns sleep without feeding - bath newborn in the evening, bring out into the center of action in the afternoon - when awae the newborn can be placed on his abdomen to promote muscle development for crawling - for nighttime fedings and diaper changes keep a night light on to avoid having to turn on bright lights |
|
|
4 basic ways to hold the newborn
|
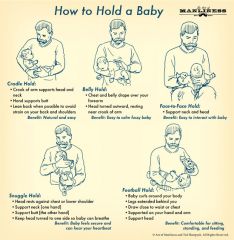
cradle hold: cradle the newborn head in the bend of the elbow, this permits eye to eye contact and is a good position for feeding
upright position: hold the newborn upright, and face him toward the holder while supporting his head, upper back, and buttocks football hold: support half of the newborn body n the holders forearm with the newborns had and beck resting in the palm of the hand , this is good for breastfeeding and when shampooing the newborns hair colic hold: place the newborn facedown along the holders forearm with the hand firmly between the newborns legs, newborn cheek--> holders elbow on the outside, the newborn should be able to see the ground |
|
|
swaddling
|
swaddling the newborn snugly in a receiving blanket helps the newborn feel more secure, swaddling brings the newborns extremities in closer to his trunk--> intrauterine position
|
|
|
bathing
|
- 2 or 3 times a week using mild soap that does not contain hexachlorophene
- not done until cord is fallen off - clean from cleanest to dirtiest part of the newborns body, beginning with his eyes, face and head, proceed to chess, arms, legs, and wash the groin area last - never newborn alone in tub - make hot water is set at 49 C or 120.2 F or less the room should be arm and bath water should be 98 to 99 F - newborns eyes should be cleaned using a clean portion of the wash cloth, clear water should be used to each eye moving from inner to the outer canthus - to clean uncircumcised penis: wash with soap and water and rinse the penis, foreskin should not be forced back or constriction may result - females: wash the vulva wiping from front to back to prevent contamination of the vagina or urthra from rectal batercia - do not use lotions, oils or powders--> bacterial growth, no powder: bacterial growth |
|
|
feeding elmination
|
- mothers breastfeeding---> see lactation consultant
- newborn is offered 15-20 min per breast and a total feeding of 30-40 min - feedings should be 8-12 times in a 24 hour period - feeding for a newborn who is breastfeeding should be on demand every 2-3 hours - newborns formula fed should be on demand every 3-4 hours - the mothers milk supple is equal to the demand of the newborn 5 to 10 min---> empty breast - should have 6-8 wet diapers and 3-4 stools per day |
|
|
cord care
|
- before discharge cord is removed
- prevent cord infection by keep the cord dry, and keep the top of diaper folded underneath it - sponge baths are given until the cord falls--> 10-14 days - cord infection--> red, foul odor, purulent drainage |
|
|
cirucmcision care
|
newborns with hypospadias---> contraindication
- level of vitamin K--> not done - minimizes risk of phimosis, reduces penile cancer, and cervical cancer in sexual partner - anesthesia required: ring block, dorsal penile nerve block, or topical anesthetic - give oral sucrose, acetaminophen, nonpharmological methods swaddle, nonnutrive uscking - yellen, mogen, gomco clamp |
|
|
what should you asses for before the baby gets circumcision
|
- history of bleeding tendencies, hemophilia, clotting disorders
- hyposapdias, epispadias - ambiguous genitalia - illness or infection postprocedure: - bleeding very 15 min for 1st hour, and then ever hour for 12 hours - first voiding |
|
|
nursing interventions for pre, and post procedure
|
- signed informed consent
- the baby will not be able to be bottle feed for up to 4 hours prior to the procedure to prevent vomiting and aspiration - place newborn on restraining board, provide radiant heat source - monitor for bleeding and voiding, apply gauze lightly to penis if bleeding or oozing - teach parents to keep area clean--> clean with warm water after each diaper change - apply petroleum jelly with each diaper change for at least 24 hours--> clamp procedures - do not give tub bath until circumcision is healed - notify if there is redness, discharge, strong odor, tenderness, decrease in urination, excessive crying - fim of yelloowish mucus may form over the glans by day 2 DO NOT WASH |
|
|
how to monitor for newborn that has cold stress and hypoglycemia
|
increased resperiations and lowered body temp
- swaddle and feed the newborn as sons as procedure is over - |
|
|
s safety and immunizations what should they get?
|
mattress should be firm not soft
- newborns cirb: space between mattress and sides of the crib should be less than 2 fingerbreathds, crib slats no more than 2.25 in apart - carseat rear facing, preferably in the middle checkups: 2 weeks to 6 weeks and every 2 months until 6 months should get diphtheria, tetanus, pertussis, hepatitis B, Haemophilus influenzae, polio, measles, mumps, rubella, influenza, rotavirus, pneumococcal, and varicella. |
|
|
what are the signs of an illness that needed to be reported
|
a fever--> above 38 C, 100.4 F or a temp below 36.6C or 97.9
- poor feeding, doesn't like food - vomiting - decreased urination - diarrhea or decreased bowel movements - labored breathing with flared nostrils or an absence of breathing for greater than 15 seconds - jaundice - cyanosis - lethargy - inconsoablble crying - difficulty waking - bleeding or purulent drainage around umbilical cord circumcision - drainage developing in eyes |
|
|
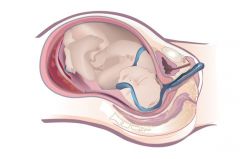
prolapsed umbilical cord
|
umbilical cord is displaced, preceding part of the fetus or protruding through cervix
|
|
what are the risk factors for prolapsed cord
|
- ROM
- abnormal fetal representation other than vertex - transverse lie - SGA - long umbilical cord - multifetal prgenancy - cephalopelvic disproportio: due to unusual space between maternal pelvis - placenta previa - interaturine tumor: prevents engagement of presenting part - hydramnios or polyhydramnios |
|
|
what are you gonna asses for prolapsed cord??
|
- client"feels like something coming through her vagina"
- visualization or pal pation of the umbilical cord protruding from introits - FHR monitoring shows variable or prolonged deceleration - excessive fetal activity follow by cessation of movement, suggestive of severe fetal hypoxia |
|
|
what are you gonna do as nurse for a patient who has prolapsed cord?
|
call for assistance right away
- notify the provider - use a sterile gloved hand, insert two fingers into vagina*** and apply pressure on either side of the cord to elevate cord - reposition the client in a knee chest, trendelenburg or side lying position with a rolled towel under the clients right or left hip to relieve pressure on the cord - apply warm, sterile, saline- soaked towel to the visible cord to prevent drying and minting blood flow - provide continuous electronic monitoring of FHR for variable decelerations which indicate asphyxia and hypoxia - administer o2 at 8 to 10 L min to improve fetal oxygenation - intiate I've access and administer IV bolus - prepare for C section |
|
|
meconium stained amniotic fluid
|
fetus has an espidoe of loss of sphincter control allowing meconium to pass into amniotic fluid
risk factors: after 38 weeks of gestation, fetus is mature - umbliccal cord compression results in fetal hypoxia stimulates vagal nerve in mature fetuses - hypoxia stimulates the vagal nerve which induces peristalsis of fetal GI tract and relaxation of the anal sphincter |
|
|
assessment of amniotic fluid meconium stained
|
amniotic fluid---> greenish, yellow or brown
- often present in breech presentation--> may not indicate fetal hypoxia - present with no changes in FHR - stained clid by variable or late decelerations in FHHR |
|
|
what kind of nursing care are you gonna for meconium stained amniotic fluid
|
- document color and consistency of stained amniotic fluid
- neonatal rescusiction team - asses neonate resp efforts, muscle tone, and HR - suction mouth and nose using bulb syringe if resp efforts strong, muscle tone good, and HR greater than 100/min - suction below vocal cords using endotracheal tube before spontaneous breaths occur if resp is depressed, mucle tone is decrease, and HR is less than 100 min |
|
|
fetal distress what does it mean?
|
- FHR is below is 110 or above 160 min
- FHR shows decreased or no variability - there is fetal hyerpacitvity or no fetal activity |
|
|
what what are the risk factors for fetal distress
|
- fetal anomalies
- uterine anomalies - complications of labor and birth |
|
|
as a nurse what are you gonna asses for fetal distress?
|
- non reassuring FHR pattern with decreased or no variability
- and also use diagnostic procedures: - monitor uterine contractions - monitor FHR - monitor findings of ultrasound and any other prescribed diagnostics |
|
|
patient centered care for fetal distress
|
- monitor vital signs and FHR
- position the client in a left side lying position with leg elevated - administer 8 to 10 L of o2 via mask - DC oxytocin pitocin - increase IV fluid rate to treat hypotension if there is - prepare the client for an emergency c section |
|
|
dystocia dysfunction labor
|
- dystocia or dysfuncional labor is abnormal related to five powers of labor passenger, passageways, powers, position, psychological response
- atypical uterine contractions prevent normal process of labor and its progression ( weak hypotonic), strong uterine relaxation |
|
|
what are the risk factors for dystocia
|
short stature, over weight sttus
- age---> 40 older - uterine abnormalities - pelvic soft tissues obstructions or pelvic contracture - cephalopelvic disproportion (fetal head larger than maternal pelvis) - fetal macrosmia - fetal malpresentation, malpostion - multifetal pregnancy - hypertonic or hypotonic uterus - maternal fatigue, fear, or dehydration - inapprpriate timing of anesthesia or analgesics |
|
|
how to asses for dystocia
|
- lack of dilation, effacement, or fetal descent during labor
- hypotonic uterus is easily indentable, even at peak of contractions - hypertonic uterus cannot be intended, even between contractions - no voluntary urge to bear down - occiput post presentation toward the prost maternal pelvis rather the anterior pelvis - presisent occiput post position prolongs labor and client reports greater back pain as the fetus presses against maternal sacrum |
|
|
what are some diagnostic or theraputeitc procedures your gnna for dystocia
|
■ Ultrasound
■ Amniotomy or stripping of membranes if not ruptured ■ Oxytocin (Pitocin) infusion ■ Vacuum-assisted birth ■ Cesarean birth |
|
|
what kind of care are you gonna give with dystocia
|
fetal scalp electrode and or interaturerine pressure catheter
- assist with amniotomy AROM - encourage client to engage in regular voiding to empty her bladder - encourage position changes to aid in fetal descent to open up the pelvic outlet -assist client to a position on her hands and knees to help the fetus rotate from a posterior to anterior position -encourage ambulation to enhance the progression of labor - encourage hydrotherapy and other relaxation techniques - apply counter pressure using fist or heel of hand to sacral area to alleviate discomfort** pub supra - assist in beneifical position for pushing and coach to bear down - prepaare for a possible focep assisted, vacuum assisted or cesarean birth - continue monitoring FHR in repsone to labor |
|
|
when patient has dystocia and has hypotonic contractions what can you do?
|
- maintain hydration
- promote rest and relaxation, provide comfort measures between contractions - place the client in a lateral position and provide oxygen by mask - medications: - oxytocin pitocin: augment labor and strengthen urterine contractions --> * only administer oxytocin if prescribed to augment labor, not for hypertonic contractions --> administer analagesics for hypertonic contractions |
|
|
precipitous labor
|
a labor that lasts 3 hours or less from the onset of contractions to the time of the delivery
|
|
|
risk factors
|
hypertonic uterine dysfunction
- nonproductive, uncoordinated, painful, uterine contractions they are too frequent and too long in duration and do not allow for relaxation of the uterine muscle between contractions (uterine tetany) - hypertonic contractions do not help to the progression of labor (cervical, effacement, dilation, fetal descent) - hypertonic contractions can result in uteroplacental insufficiency leading to fetal hypoxia oxytocin---> increases intensity and duration of contractions - can lead to hypertonic uterine contractions multiparous--> why?--> may move through the stages of labor more quickly |
|
|
assessment of precipitous labor
|
low backache
- abdominal pressure and cramping - increased bloody vaginal discharge - palpable uterine contractions - progress of cervical dilation and effacement - diarrhea - fetal presentation, station, posit - status of amniotic membranes - asses for perineal area for signs of trauma or lacerations - asses neonate color and signs for hypoxia - asses for signs of trauma to presenting part of the neonate especially cephalic presentation |
|
|
preciptious labor what can you do as a nurse
|
- do not leave the client unattended
- provide reassurance and emotional support to help the client remain calm - prepare for emergency delivery of the neonate - pant--> with an open mouth between contractions to control the urge to push - encourage the client to maintain a side lying position to optimize ueroplacenalt perfusion and fetal oxygenation - prepare for ROM upon crowning - do not stop the delivery - control rapid delivery by applying light pressure on perineal area and fetal head--> press upward toward the vagina, eases the rapid expulsion of the fetus and prevents cerebral damage to the newborn and perineal lacerations to the client - deliver the fetus between contractions assuring the cord is not around the fetal neck - if the cord is around the fetal neck, attempt to gently slip over the head --> if not possible--> clamp cord with two clamps and cut between clamps - suction mucus from fetal mouth and nose with a bulb syringe when the head appears |
|
|
after precipitous labor what are you checking for?
|
☐ Cervical, vaginal, and/or perineal lacerations
☐ Resultant tissue trauma secondary to rapid birth ☐ Uterine rupture ☐ Amniotic fluid embolism ☐ Postpartum hemorrhage Fetal hypoxia due to hypertonic contractions or umbilical cord around fetal neck ☐ Fetal intracranial hemorrhage due to head trauma from rapid birth |
|
|
rupture of the uterus
|
complete rupture involves the uterine wall, peritoneal cavity, and or broad ligament, internal bleeding
- incomplete rupture occurs with dehiscence at the sitre of a prior scar C section surgical intervention, internal bleeding may not be present |
|
|
what are the risk factors for rupture of the uterus
|
- congential uterine abnormality
- uterine trauma due to accident or sugary of previous multiple cesarean births - over distention of the uterus from a fetus who is large for gestational age, multifetal gestation or polydramnios - hyper stimulation of the uterus either spontaneous or from oxytocin pitocin administration - external or internal fetal version done to correct malposition of the fetus - forceps assisted birth - multigravida clients |
|
|
what are you gonna asses for as a nurse when there is rupture of the tuerus
|
client reports sensation of ripping, tearing or sharp pain client resorts abdominal pain, uterine tenderness
- nonreasurring FHR with signs of distress, bradycardia, variable and late decelerations, and absent or minimal variability - change in uterine shape and fetal parts palpable - cessation of contractions and loss of fetal station - manifestations of hypovolemic shock tachypnea, hypotension, pallor, and cool and clammy skin |
|
|
what are you gonna do as a nurse with rupture of the uterus
|
- admnister IV fluids
- a minister blood products - prepare the client for an immediate C section--> lapartomy and hysterectomy |
|
|
anaphylactioid syndrome of pregnancy (amniotic fluid embolism )
|
an amniotic fluid embolism occurs when there is a rupture in the amniotic sac or maternal uterine veins accompanied by high intrauterine pressure that causes infiltration of the amniotic fluid in the maternal circulation, the amniotic fluid then travels to and obstrucs pulmonary vessels and causes resp distress and circulatory collapse
- serious coagulation problems such as disseminated intravasuclar coagulopathy DIC can occur |
|
|
meconium stained amniotic fluid
|
can cause maternal damage because it clogs pulmonary veins completey
|
|
|
ris factors for amniotic fluid embolism
|
Multiparity and advanced maternal age
◯ Tumultuous labor ◯ Placenta previa or abruptio placentae ◯ Preeclampsia ◯ Oxytocin (Pitocin) administration ◯ Fetal macrosomia ◯ Hydramnios ◯ Fetal demise ◯ Meconium-stained amniotic fluid |
|
|
assessment of amniotic fluid embolism
|
resp distress indications:
- restlessness - cyanosis - dyspnea - pulmonary edema - resp arrest - indications of coagulation failure - bleeding from incisions and venipuncture sites - petechiae and ecchymosis - uterine atony indications of circulatory collapse - tachycardia -hypotension -shock - cardiac arrest |
|
|
patient centered care for amniotic fluid embolism
|
administered oxygen via mask at 8 to 10 L min
- assist with intubation and mechanical ventilation as indicated -erform caridopulmonary resuscitation if necessary - administer IV fluids - position the client on her side with her pelvis titled at 30 degree angle to displace the uterus 0 administer blood products prescribed to correct coagulation failure - insert indwelling catheter and measure hourly urine output - monitor maternal fetal status - prepare for emergency C section |
|
|
reasons for preterm birth
|
- prior preterm birth
- history of second trimester loss -cerclage - IVF pregnancy - multiple gestation - uterine/cervical abnormalities - hydramnios, oligohydramnios - infection--> periodontal and UTI - premature rupture of membranes - short pregnancy interval less than 9 months - HTN, diabetes, and vaginal bleeding - inadeqaute nutrition, low BMI, low pre pregnancy weight, or poor weight gain - age young than 17 or older than 35 years old - late prenatal care or no - obestiy, high BMI, excessive weight gain - LOW BMI - working long hours, long periods of standing - african american - maternal unmarried status - partner violence--> domestic violence - smoking, alcohol, illicit drug use - lower education and lower socioeconomic status |
|
|
how to predictive preterm labor?
|
cervical length---> more than 30= excludes preterm labor, less than 20= strong positive predictive value
- fetal fibronectin has a low positive predictive value but a high negative predictive value, thereby making it a useful test to predict those women who will not deliver preterm ---> results---> neg= will not deliver, pos= will deliver |
|
|
drugs to slow delivery for a couple of days
|
TOCOLYTICS--> SUPPRESS CONTRACTIONS
terbuline---> no research that shows it works magnesium sulfate, prostagladin , calcium channel blocker, terbutaline, |
|
|
megnesium sulfate
|
mangnesium sulfate: not for long term, administered through pump, side effects: flushing, lethargy, headache, muscle weakness, diplopia, may reduce cerebral palsy
what can happen to fetus? lethargy, hypotonia, resp depression, demineralization signs of toxicity: absent DTR, resp rate less than 14, severe hypotension, muscle relaxation, decreased level of consciousness, pulmonary edema, check I& O output less than 30 ml/Hr |
|
|
prostagaldin
|
depresses synthesis of prostaglandins, effective in delaying 48+, used short term--> fetal effects
contraindications: renal or hepatic impairment, thrombocytopenia side effects: nausea, vomiting, GI upset, serious side effects are uncommon fetal effects: constriction of ductus arteriousus, pulmonary hypertension, reversible decrease in renal function with oligohydramnios, inter ventricular hemorrhage, hyperbilrubinemia, nectrozing enter colitis monitor FHR and UC treat nausea and heartburn |
|
|
terbutaline
|
can delay delivery for 3 days IV or SubQ
side effects: cardiac, cardiopulmonary arrthymias, pulmonary edema, myocardial ischemia, hypotension, tachycardia, hypokalemia, maternal glocus fetal: tachycardia, hyperinuslinemnia, hyperglycemia, spetal hypertrophy, myocaridal ischemia monitor FHR,, UC, and monitor I and O - auscultate lungs for pulmonary edema -monitor maternal HR and may hold dose for heart rate greater than 120 - monitor glucose - life throning complications are pulmonary edema, myocardial failure and fluid overlaid |
|
|
cotricosteriod therapy, perterm labor
|
antenatal seriods remcommend
- betamethasone is one antenatal steroid given to women to accerlaeralte fetal lung maturity, decreasing the severity of resp distress syndrome and other complications of prematurity in the neonate such as resp distress syndrome, cerebroventricular hemorrhage, nectroizing enterocolitis, and infectious morbidity given at 24 or 34 weeks of gestation will raise blood sugar and may require temporary insulin coverage to maintain euglycemia in diabetic woman |
|
|
what are the contraindications to treating preterm labor?
|
active hemorrhage
severe maternal disease fetal compromise chorioamniotis fetal death previable gestation and prom |
|
|
what are the contraindications for tocoloysis
|
preeclmapsia, placental abruption, interatuerine infection, lethal congential, chromosomal anromlaties, advanced cervical dilation, masythenia gravis, concurrent treatment with nifedeipine , terbutaline in the pervious 4 hours and evidence of fetal compromise or placental insufficiency, renal disease, HTN disease
|
|
|
nursing actions when dealing with preterm labor
|
if there is 5 UC per hour or less than they can go to a less intensive care setting or even home
- assses the woman for signs and symptoms of: vaginal and urinary infection - rupture of the membranes - ** a sterile speculum exam may be performed to asses for ferrying oft he amniotic fluid - asses FHR and uterine contractions--> report fetal tachycardia or increased uterine contractions to the health care provider - obtain vaginal and urine cultures per order - obtain fFN ( fetal fibrinogen) as per order contraindicated if: ROM, bleeding, sexaul intercourse, or prior collection in the last 24 hours - maintain I and O - provide IV hydration - may restrict total intake to 3000 ml per 24 hr if on tocolytics - monitor for tocolytics and behamsone - postiiont the client on their side to increase uteroplacental perfusion and decrease pressure on the maternal inferior vena cava - auscultate lungs for evidence of pulmonary edema - asses cervical status |
|
|
nursing actions continued when dealing with preterm labor
|
asses vital signs: if 90/50 or greater than 140/90 and temp is greater than 100.4 let the health care provider know
- ausculatate lungs for evidence of pulmonary edema - asses cervical status with a sterile vaginal exam unless contraindicated by ROM or bleeding - monitor baseline and variability and uterine contractions - WBC elevated when given corticosteriods not indicative of infection |
|
|
signs of pulmonary edema:
|
SOB, chest tightness, cough, o2 less than 95%, increased resp, and heart rates
|
|
|
what are the warning signs of preterm labor
|
bag of water breaks
baby stops moving you more than 5 contractions in one hour you a low backache, menstrual cramp like pelvic pressure, intestinal cramps with or without diarrhea increased discharge from vagina fever of 100.4 F something is not right |
|
|
home care instructions of preterm labor
|
baby movements and contractions--> lie on your side for 1 hour and count number of times your baby kicks
activity restrictions: indicate restrictions on physical activity and be specific sexual relations: gotta stop diet: small meals and snacks high fiber, calcium, and iron fluids 8 ounces medication schedule: tocolytic, prenatal vitamin, pnV, iron sulfate, stool softeners |
|
|
premature rupture of membranes
|
less than 37 weeks
risk factors: - previous PROM - preterm delivery - hydramnios - multiple gestation up to 15% of twins and up to 20% of triplets - STDS - smoking maternal infecion - increased rates of C section - complications of prematurity - hypoxia or asphyxia because of umbilical cord compression due to decreased fluid - fetal deformities if preterm Prom before 26 weeks gestation |
|
|
interventions for PROM
|
groub B strepococcus
- IV ampicillin and erthomycin - digital cervial examinations should be avoided - LS ratio - asses FHR - maternal tachycardia, and 100.4F - uterine tenderness - vaginal discharge - do a NST and BPP |
|
|
incompétent cervix
|
mechanical defect in the cervix that results in painless cervical dilation in the second trimester that can profess to ballooning of the membranes into the vagina and delivery of the premature fees in related second trimester abortions
|
|
|
the reason for incompetent cervix
|
repeated second trimester or early third trimester births
- reccurent pregnancy losses preterm delivey ROM infection |
|
|
assessment of incompetent cervix what are you ognna find
|
pelvix pressure
- increase mucoid vaginal discharge - shortned cervical length or funneling of the cervix - obstetrical history of second trimester cervical dilation or fetal losses live fetus and intact membranes |
|
|
nursing actions of an incompetent cervix
|
obtain an ultra sound to evaluate the cervix
- cervical cultures for chlamydia, gonorrheea, and other cervical infections - treatment of incompetent cervix is cerclage between 12 to 16 weeks - rescue cerclage for 24 weeks if there is not contractions - administer antibitoics and tocolytics postop: monitor for uterine activity - monitor for bleeding - maternal fever, uterine tenderness administer tocolytics discharge teaching: rupture of membranes, uterine activity, bleeding and infection |
|
|
multiple gestation
|
monozygotic twins: from one zygote that divides in the first week of gestation--> genetically identical and similar in appearance and always the same gender
dizygotic twins: fertilization of two eggs same or differing genders, if the fetuses are differing gender they are dizygotic |
|
|
monochorionic and dichorionic
and what are the risk for multiple gestation |
monochorionic: one chorion
dichorionic: two chorions risks for multiple gestation: - preterm labor and delivery - premature prolonge d rupture of membranes related to over distention - HTN and preclampsia - gestational diabetes - antepartum hemorrhags - placenta previa - anemia - pulmonary edema |
|
|
what are the risk for multi gestational for fetus
|
- fetal morbidity and mortatility
- delivery before term --> 90 % higher - increase in low birth weight - increase in intrauterine growth restriction - twin to twin blood transfusion - post partum hemorrhage - abruptio |
|
|
what are you assessing for mutlipal gestation
|
HCG---> nausea and vomiting
uktrasound fundal height is greater in size maternal blood expansion is 50 to 60% (rather 40 to 50) increased cardiac output increased plasma volume 50-100 increased iron deficiency anemia increased lower back and ligament pain increased dermatosis |
|
|
what kind of antepatral medical management are you gonna do for multi gestational pregnancy
|
ultrasounds---? IUGR
genetic testing for anomalies monitor for preterm labor and prevent birth corticosteriods for fetal lung maturity reducing RDS - monitor for maternal anemia fetal surveillance including NST bpp - mintor for HTN preeclmapsia - monitor for hydramnios - monitor for antepartal hemorrhage - monitor for interatuerine fetal demise - cross match blood - EFM -fetal postions presentations - nst and AFI, BPP - give educations and signs and symptoms preecalmpsis - woman needs increased iron, calcium, magnesium |
|
|
hyperemesis graviduram
|
vomiting during pregnancy that is so severe it leads to dehydration, electrolyte and acid base imbalance, starvation ketosis and weight loss
- rapdily serum rising |
|
|
assesementt findings
|
vomitin is prolonged
dry mucus membranes poor skin turgor malaise low blood pressure |
|
|
medical management of hyperemsis graviduram
|
treatment of nausea and vomiting with vitamin B or vitamin B 6 pulse doxylamine is safe
- IV hydration---> dextrose, vitamins thiamine, - antihistamine H1 receptor blockers - kidney and liver fucntion - correction of ketosis and vitamin defiency should be strongly considered |
|
|
what nursing actions are you gonna take for hyperesmis gravid arum?
|
treatment of Nausea and vomting
- Iv hydration - daily weight - I AND O - npo - vitamin B6 |
|
|
diabetes mellitus and placenta how does it spare
|
type one: autoimmunity of beta cells of the pancreases resulting in absolute insulin deficiency and managed with insulin
tyep two: insulin resistance and inadequate insulin production --> controlled with--> exercise, diet, oral glycemic agents antigoizing hormones: HPL***, progeserone, grwoth hormone, corticotrpin releasing hromone |
|
|
pregestational diabetes risks for woman
|
- hypoglycemia and hyperglycemia
doabetic ketoacidosis - HTN disorders - preterm - hyerpeemsis nausea - polyhdramnion, olgihydrmanuos - C section, chroinc diabetes related conditions, rentipathy,nephropathy and neurpathy - infectin on related to hyperglycemia - induction of labor |
|
|
risks for fetus for gestationl diabetes
|
congetial defets
growth disturbances - hypoglycemia - hypocalcemia and hypomagnesia - hyperinsulemia - IGUR - asphaxia RDS plychtemia hyperbilirubeniama macrsomia STILL BIRTH **** |
|
|
how to self manage for diabetes
|
4-8 times a day read the score
- morning fasting ketones ---> urine - exercise for 20 minutes blood glucose goals: am fasting less than 90 pre meal less tun 105 1 hour postprandial less than 140 mean blood glucose is less than 100 by third trimester: may need 3 or 4 times more insulin |
|
|
delivery issues of pre gestation diabetes and nursing actions
|
STILLBIRTH AND MACROSOMIA
delayed lung maturity monitor: abdominal pain, nausea and vomiting, polyuria, polydispia, fruity breath, leg cramps, altered mental status, and rapid respirtations when to call the provider: 200 glucose level, moderate ketones, nuase sand vomiting, decreased fetal movement, - glucose level should be checked every 1 to 2 hours and ketones every 4 hours - 28 weeks of gestation---> NSt and bpp |
|
|
gestational diabetes mellitus
|
HCG, cortisol, and progesterone, HCG--> glucose in fetus
|
|
|
oral glucose testing
|
24-28 weeks for all pregggo women
- nonfasting---> 1 hr oral glucose 50 g sucrose--> postive test 130 mg/dl or 140 mg/dl postive--> a 3 hour glucose tolerance test is done after the women ingest a 100 g lucose load , plasma levels are drawn at 1, 2 and 3 post glucose load if two or more glucose are above threshold a diagnosis of GDM can be made fasting >95, 1 hour > 180, 2 hour> 155, 3 hour >140 |
|
|
risk factors for GDM
|
hypoglecmia
- preeclamspia - C section - development of non gestation diabetes - macrsomia - hypoglycemia during the first few hours post birth - should dystocia - hypperilirubienima - RDS - |
|
|
hypertension/ preeclampsia
|
HTN: systolic pressure of 140 or more and diastolic pressure of 90 mmhg
preeclampsia: systemic disease with HTN 20 th week of gestation eclmapsia: convulsions |