![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
118 Cards in this Set
- Front
- Back
|
Epidermis |
tough, outer layer has melanocyte and kerantinocyte cellsuu
|
|
|
dermis |
|
|
|
function of the skin |
|
|
|
which vitamin is synthesized on the skin? |
vitamin D |
|
|
what does vitamin D help with metabolizing? |
calcium and phosphate |
|
|
What effects can aging have on the skin? |

↓ elasticity
↓ fluids more comorbidities |
|
|
types of burns |
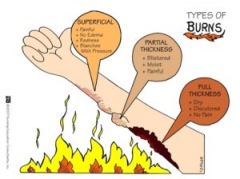
superficial partial thickness full thickness |
|
|
superficial thickness burns |
|
|
|
superficial partial thickness burns |
|
|
|
deep partial thickness burns |
|
|
|
full thickness burn |
|
|
|
if all dermis structures are destroyed, what will the patient have the inability to do? |
|
|
|
where do 3rd degree burns occur most often? why? |
|
|
|
why would a 3rd degree burn not be painful? |
lack of nerve endings |
|
|
where would a 3rd degree burn be painful? |
at the wound margins; nerve endings are still there |
|
|
what would be required to close a 3rd degree burn wound? |

skin graft |
|
|
escharotomy |
removal of eschar in wound to promote healing |
|
|
fasciotomy |
incision usually made into the fascia usually done opposite of wound to relieve pressure and promote circulation |
|
|
what conditions would complicate performing an escharotomy or fasciotomy? |
diabetes elderly patients patients on blood thinners |
|
|
what type of burn can compromise a patient's ability to breathe? |

circumferential burns |
|
|
what is a circumferential burn? |
"Circumferential deep full thickness burns of an extremity or around the chest or abdomen should be carefully monitored. Edema and swelling in the tissue deep to the burn cause the unyielding overlying burnt skin ('eschar') to act like a tourniquet." |
|
|
criteria for a minor burn |
|
|
|
facility for a minor burn |
ER/outpatient |
|
|
criteria for a moderate burn |
|
|
|
facility for a moderate burn |
hospital or maybe burn unit |
|
|
criteria for a major burn |
partial thickness >25% full thickness >10% true electrical injuries includes hands, face, eyes, ears, feet, perineum inhalation, fracture, or other trauma other comorbidities |
|
|
facility for a major burn |

burn unit |
|
|
what type of burn is most frequent in toddlers? |
hot water scalds :( |
|
|
most common burn with older children? |
flame-related burns |
|
|
how many documented cases of child abuse include burns? |
10-20% |
|
|
what accounts for 10% of house fires? |
children playing with lighters or matches |
|
|
way to assess the extent of a burn? does not apply to children |
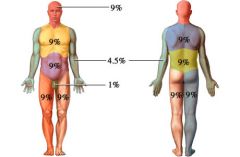
rule of nines |
|
|
types of burns |
thermal electrical chemical radiation |
|
|
Thermal burn |
also called heat burn due to
|
|
|
electrical burns |
|
|
|
How does electrical burns affect body systems? |
|
|
|
what type of electrical burns are see in children and why? |
burns of the mouth: due to children biting or sucking on electrical cords |
|
|
the amount of damage of chemical burns depends on what? |
|
|
|
what chemical binds with calcium and magnesium in the body? |
hydrofluoric acid |
|
|
what is a MSDS? |
material safety data sheet "a document that contains information on the potential health effects of exposure to chemicals, or other potentially dangerous substances, and on safe working procedures when handling chemical products." |
|
|
how do we treat chemical burns? |
|
|
|
how do we treat radiation burns? |
|
|
|
emergent phase of a burn injury |
most acute phase; most chance to die lasts for approx. 48 hrs severity of symptoms depend on severity of burn may see: oliguria hypoproteinemia: protein in 3rd spacing or urine hyperkalemia hyponatremia ↑ HCT r/t hemoconcentration metabolic acidosis |
|
|
most burns result in what type of acid/base imbalance? |
metabolic acidosis |
|
|
what type of shock develops quickly after a major burn injury? |
hypovolemic shock r/t massive fluid loss ↓ circulating volume ↓ ↓ venous return ↓ ↓ stroke volume ↓ ↓ CO ↓ ↓ cellular O2 supply ↓ impaired tissue perfusion ↓ impaired cellular metabolism |
|
|
which diagnostic test determines acid-base balance? |
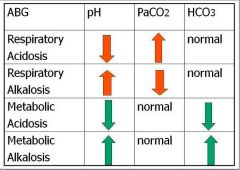
ABG's |
|
|
when does the diuretic phase begin? |
approximately 48 hours after onset of injury or whenever diuresis starts |
|
|
what occurs during the diuretic phase? |
|
|
|
nursing assessments for acute and intermediate phase |
|
|
|
nursing interventions for acute and intermediate phase |
|
|
|
what else should we be doing as we do our interventions? |
teaching as we go along so the patient understands everything we are doing to them we need to assess if our patient understands what we are teaching |
|
|
nursing interventions in rehab phase |
|
|
|
Speaking of eschar....here's a really bad joke A snail slides into a car dealership to buy a car. The snail looks around and finally decides which car he will buy. He then proceeds to tell the salesman that he wants a custom paint job. He tells the salesman "I want you to paint a giant S on each side of the car, including the hood, the trunk, and the roof." The salesman says "sure we can do that, but why on earth would you want an S on each side of your car?" |

The snail smiles and says "because when I drive down the street, I want everyone to look my way and say, "wow! look at that S car go!" 😁 😂 |
|
|
what is the most important thing to assess with hyponatremia? |
changes in LOC |
|
|
what type of issues are monitored with ↑ or ↓ K+? |
cardiac issues |
|
|
major buffer system in extracellular fluids |
carbonic acid to sodium bicarbonate |
|
|
ratio that must be maintained to stay in acid base balance |
1 part carbonic acid to 20 parts sodium bicarbonate |
|
|
respiratory regulation |
regulates acid base balance by eliminating or retaining CO2 |
|
|
causes of respiratory acidosis |
|
|
|
acute manifestations of respiratory acidosis |
|
|
|
chronic manifestations of respiratory acidosis |
weakness dull headache |
|
|
causes of respiratory alkalosis |
|
|
|
clinical manifestations of respiratory alkalosis |
|
|
|
if patient has metabolic acidosis, the respiratory system compensates by: |
hyperventilating |
|
|
if the patient had metabolic alkalosis, the respiratory system responds by: |
hypoventilating |
|
|
carbon monoxide poisoning |
|
|
|
s/s of carbon monoxide poisoning |
bright red lips and tongue carboxyhemoglobinemia: skin turns red dyspnea headache tachypnea confusion impaired judgement cyanosis respiratory depression |
|
|
treatment for CO poisoning |
100% O2 via nonrebreather mask intubation hyperbaric O2 therapy |
|
|
ultimate regulator of acid base balance |
the kidneys |
|
|
renal tubules response to alkalosis |
↑ amount of bicarb excretion
|
|
|
renal tubules response to acidosis |
reabsorption of bicarb and excretion of acid |
|
|
changes in renal function with a burn injury |
|
|
|
causes of metabolic acidosis |
|
|
|
clinical manifestations of metabolic acidosis |
|
|
|
causes of metabolic alkalosis |
|
|
|
clinical manifestations of metabolic alkalosis |
|
|
|
hyperkalemia due to damaged cells cause what to be seen on EKG? |
|
|
|
what happens to the GI system with a burn? |
↓ GI motility
paralytic ileus caused by ↓ blood flow and sympathetic stimulation at risk for Curling's ulcer |
|
|
five primary objectives for management of the burn patient |
|
|
|
emergent or resuscitative phase of burn care |
from injury until physiologically stable (about 36-48 hours) |
|
|
acute or diuretic phase of burn care |
lasts until all full thickness burns covered with skin |
|
|
rehabilitation phase of burn care |
return to highest possible level of functioning |
|
|
treatment of the burn patient primary survey |
A= Airway B= Breathing C= Circulation D= Disability, neurological deficit E= Exposure and evaluation F= Fluid resuscitation |
|
|
most important factor of airway treatment |
|
|
|
important aspects of neuro assessments |
|
|
|
Fluid resuscitation formula for 1st 24 hours |
TBSA x Kg x 4mL lactated ringers |
|
|
when is fluid resuscitation calculated? |
from the time of injury, NOT from arrival time at the hospital |
|
|
objectives of fluid therapy |
|
|
|
goals for fluid resuscitation |
keep urine output 30-50mL/hr for adults and older kids, Na+ at 140meq/L for kids <30kg = urine output of 1mL/hr/kg |
|
|
what fluid is used after 1st 24 hours? |
colloids |
|
|
single most efficient indicator for fluid resuscitation adequacy? |
urine output during 1st 24 hours (at least 30mL/hr) |
|
|
cushing's ulcer (stress ulcer) |
an acute gastritis erosion resulting as a complication from severe burns when reduced plasma volume leads to ischemia and cell necrosis (sloughing) of the gastric mucosa |
|
|
what is the drug of choice for pain and anxiety for adults and children? |
morphine: allows body to relax and promote circulation |
|
|
nutritional goals for burn patient |
increased calories increased protein needs vary according to the size of the burn TPN or may need G tube feed GI system when bowel sounds are heard |
|
|
what do we worry about before we worry about the wound itself? |
ventilatory and hemodynamic stability |
|
|
objectives of wound treatment |
|
|
|
preventative efforts regarding infection |
|
|
|
sulfamylon |
|
|
|
silvadene |
|
|
|
silver nitrate |
|
|
|
petroleum/mineral oil based |
|
|
|
non surgical treatment of wounds |
|
|
|
debridement |
|
|
|
tangential excision |

remove successive thin layers of eschar to a level of tissue viability |
|
|
fascial excision |
|
|
|
meshed autograft |
|
|
|
sheet autograft |
excellent cosmetic appearance requires more donor sites used on face and hands if possible difficult to apply on irregular surfaces |
|
|
sign of graft rejection |
curling edges sloughing could be from infection |
|
|
CEA cultured epidermal autograft |
skin cells from patient grown in a lab very costly smooth, seamless surface, but thin 18-25 days to grow |
|
|
biological and synthetic dressings |
can cover partial thickness wounds to promote healing or serve as temporary wound covers after burn excision when no autografts are available |
|
|
allograft |
cadaver skin becomes vascularized and creates a favorable environment body will begin to reject in 7 days - normal |
|
|
xenoderm |

pig skin does NOT become vascularized, but does create a favorable subgraft environment body begins to reject in 7 days |
|
|
biobane |
synthetic skin cover of collagen designed to accelerate healing will turn opaque as healing occurs change q 7-10 days manmade silicon film with nylon fabric great for depp partial thickness burns less pain, ↑ flexibility, ↓ r/f infection |
|
|
complications of burns |
infection keloid formation contracture formation |
|
|
keloid formation |

also called hypertrophic scar abnormal fibrous proliferations of the dermis most common in darker skinned people treatment os surgical removal with possible steroid injections or low-dosed radiotherapy hard to counteract |
|
|
contractures |

fibrosis of connective tissue in skin, fascia, muscle or a joint capsule that prevents normal mobility |
|
|
how to prevent contractures |
abduct limbs away from body splay fingers and toes if on hands and feet maintain patient in neutral position with minimal flexion use splints if necessary range of motion 3 times a day if possible, if the burn is on hands, have pt. perform active ROM q hr while awake |
|
|
pressure therapy |
used for the prevention of hypertrophic scar development and contractures pressured delivered by
|