![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
92 Cards in this Set
- Front
- Back
|
ECG chart Too fast |
- Increased myocardial O2 demand - Decreased ventricular filling time - Decreased coronary perfusion Resulting in decreased CO |
|
|
ECG chart Too slow |
- Slow ventricular rate Resulting in decreased CO |
|
|
ECG chart No P wave |
- Loss of atrial kick causing decreased preload Resulting in decreased CO - Risk for clot formation |
|
|
ECG chart ST changes |
- Potential ischemia/injury causing decreased contractility Resulting in decreased CO |
|
|
Pacemakers of the heart Rate of firing SA node |
60-100/min |
|
|
Pacemakers of the heart Rate of firing AV junction |
40-60/min |
|
|
Pacemakers of the heart Rate of firing Purkinje fibers |
20-40/min |
|
|
Stroke volume assessment Preload (5) |
- JVD - CVP - Crackles - Edema - Mucus membranes |
|
|
Stroke volume assessment Afterload (3 Vs) |
- Vessel diameter - Viscosity - Valves |
|
|
Stroke volume assessment Contractility (3) |
- Hx - EF (from ECHO) - Preload (Starling's law) |
|
|
ECG complex P wave |
- Represents atrial depolarization |
|
|
ECG complex PR interval |
- Represents the time it takes for the electrical impulse to leave the SA node, depolarize the atria, and pass through the AV junction - Measured from the beginning of the P wave to the beginning of the QRS complex - Normal range is 0.12-0.2 sec |
|
|
ECG complex QRS complex |
- Represents ventricular depolarization - Normal range is 0.04-0.1 sec |
|
|
ECG complex J point |
- The junction between the QRS complex and the ST segment |
|
|
ECG complex ST segment |
- Represents the time where the ventricles have depolarized and repolarization begins - Located from the end of the QRS complex to the start of the T wave |
|
|
ECG complex ST depression |
- Represents myocardial ischemia |
|
|
ECG complex ST elevation |
- Represents myocardial injury |
|
|
ECG complex T wave |
- Represents the time it takes for the ventricles to repolarize - Represents ventricular repolarization |
|
|
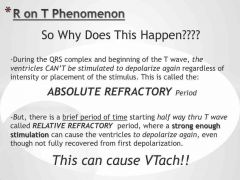
ECG complex QT interval |
- Represents ventricular activity (depolarization and repolarization - Prolonged QT may lead to life threatening dysrhythmias (R on T phenomenon leading to ventricular tachycardia) |
|
|
ECG chart Interventions Too slow (2) |
- Atropine - Pacemaker |
|
|
ECG chart Interventions Too fast (4) |
- CSM (carotid sinus massage) - Vagal maneuvers - Chemical (beta blocker, amiodarone, adenosine) - Electrical (cardioversion) |
|
|
ECG chart Interventions No P wave (2) |
- Chemical (amiodarone) - Electrical (cardioversion depending on rhythm) |
|
|
ECG chart Interventions ST changes (3) |
- MONA (morphine, oxygen, nitro, aspirin) - ? Thrombolytic - ? Cath lab |
|
|
Properties of Electrical Cells Automaticity |
- Ability to generate an electrical impulse spontaneously, without external stimulation |
|
|
Properties of Electrical Cells Excitability |
- Ability of cell to depolarize in a response to an electrical stimulus |
|
|
Properties of Electrical Cells Refractoriness |
- The period of time during which cardiac electrical cells are unresponsive to any stimulus, regardless of strength |
|
|
Properties of Electrical Cells Rhythmicity |
- Ability of cardiac pacemaker cells to fire at regular intervals |
|
|
Properties of Electrical Cells Conductivity |
- Spread of electrical activity from one specialized cardiac cell to another |
|
|
Junctional arrhythmias Rate Junctional escape rhythm |
40-60 bpm |
|
|
Junctional arrhythmias Rate Accelerated junctional rhythm |
60-100 bpm |
|
|
Junctional arrhythmias Rate Junctional tachycardia |
>100 bpm |
|
|
Junctional arrhythmias Criteria (3) |
1) No P wave, normal QRS, regular 2) Inverted P wave, normal QRS. regular 3) Normal QRS, inverted P wave, T wave |
|
|
Premature terms Unifocal |
- From one abnormal focus |
|
|
Premature terms Multifocal |
- From more than one abnormal foci |
|
|
Premature terms Bigeminy |
- Every second beat is abnormal |
|
|
Premature terms Trigeminy |
- Every third beat is abnormal |
|
|
Premature terms Quadrigeminy |
- Every fourth beat is abnormal |
|
|
Premature terms Couplet |
- Two abnormal beats occurring together |
|
|
Premature terms Triplet |
- Three abnormal beats occurring together |
|
|
Premature terms Run |
- More than three abnormal beats occurring together |
|
|
First degree heart block |
- PR interval >0.2 sec - P wave to QRS complex ratio is 1:1 - Regular |
|
|
Second degree heart block type I |
- PR interval consecutively lengthens - More P waves than QRS complexes - Irregular |
|
|
Second degree heart block type II |
- PR interval constant (normal or >0.2 sec) - More P waves than QRS complexes - Regular |
|
|
Third degree heart block |
- No consistent relationship between P wave and QRS complex - More P waves than QRS complexes - Regular |
|
|
Pacemaker definition |
- An electronic device that regulates HR and electronically stimulates the myocardium to depolarize, which then starts a contraction |
|
|
Indications for Pacemaker (3) |
- Pt with dysrhythmias - Decrease in CO - Unresponsive to drug therapy (due to acidosis, heart block) |
|
|
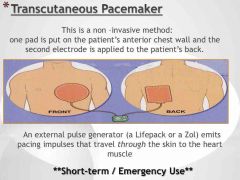
Stat Pacemakers |
- Can be either internal or external and are used for short term and or temporary "rescue" tx |
|
|
Other reasons for a pacemaker |
|
|
|
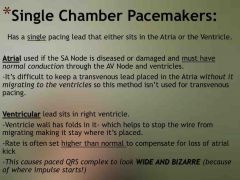
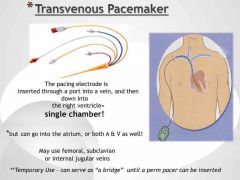
Single chamber pacemakers |
|
|
|
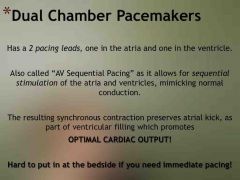
Dual chamber pacemakers |
|
|
|
Types of Temporary Pacers (3) |
- Epicardial - Transcutaneous - Transvenous |
|
|
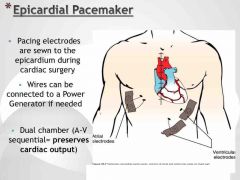
Epicardial pacemaker |
|
|
|
Transcutaneous pacemaker |
|
|
|
Transvenous pacemaker |
|
|
|
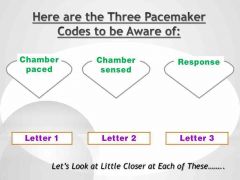
Pacemaker codes (3) |
|
|
|
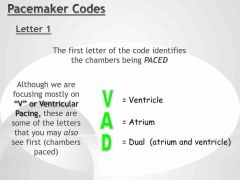
Pacemaker codes Letter 1 |
|
|
|
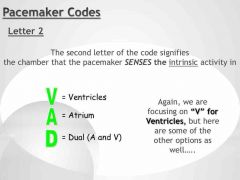
Pacemaker codes Letter 2 |
|
|
|
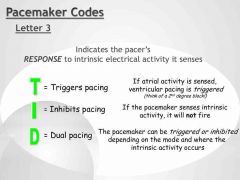
Pacemaker codes Letter 3 |
|
|
|
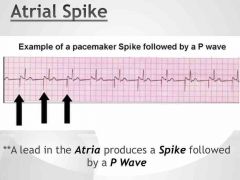
Atrial spike |
|
|
|
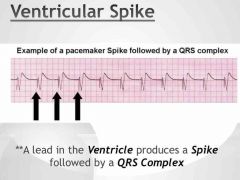
Ventricular spike |
|
|
|
Pacemaker malfunctions (3) |
- Failure to pace - Failure to capture - Failure to sense |
|
|
Failure to pace Definition |
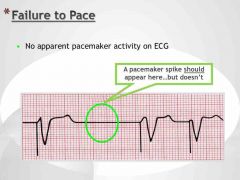
|
|
|
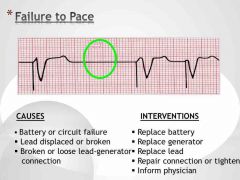
Failure to pace Causes (3) and Interventions (4) |
|
|
|
Failure to capture Definition |
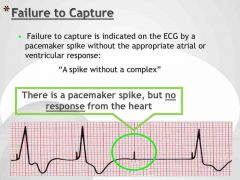
|
|
|
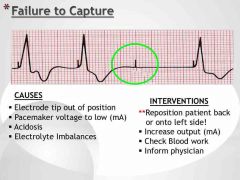
Failure to capture Causes (4) and Interventions (4) |
|
|
|
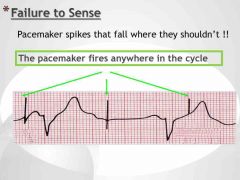
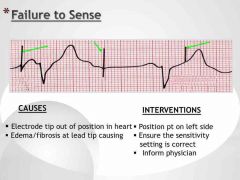
Failure to sense Definition |
|
|
|
Failure to sense Causes (2) and Interventions (3) |
|
|
|
R on T phenomenon |
|
|
|
Wandering atrial pacemaker |
3 different P waves in one rhythm |
|
|
Heart sounds S1 |
- Closing of mitral and tricuspid valves |
|
|
Heart sounds S2 |
- Closing of aortic and pulmonic valves |
|
|
Heart sounds Murmur (2) |
Whooshing sound - Regurgitation (leaky valve) - Stenotic (narrowed valve) |
|
|
Heart sounds S3 |
- Systolic failure - Fails to eject |
|
|
Heart sounds S4 |
- Diastolic failure - Fails to relax |
|
|
Wolff–Parkinson–White syndrome (WPW) |
- Electrical abnormality - Abnormal pathway between the atria and ventricles through the bundle of Kent - Narrow PR interval (<0.12 sec) - Widened QRS complex |
|
|
Antiarrhythmic Classification Class Ia |
- Inhibits fast Na channels - Prolongs repolarization time - Ex. quinidine, procainamide |
|
|
Antiarrhythmic Classification Class Ib |
- Inhibits fast sodium channels - Shortens repolarization time - Ex. lidocaine |
|
|
Antiarrhythmic Classification Class Ic |
- Inhibits fast sodium channels - Repolarization time unchanged - Ex. flecainide, propafenon |
|
|
Antiarrhythmic Classification Class II |
- Beta blockers - Repolarization time unchanged - Ex. propanolol, atenolol |
|
|
Antiarrhythmic Classification Class III |
- Markedly prolongs repolarization time, usually by K channel blockade - Ex. amidarone |
|
|
Antiarrhythmic Classification Class IVa |
- AV node and calcium channel blocker
- Repolarization time unchanged - Ex. verpamil, diltiazem |
|
|
Antiarrhythmic Classification Class IVb |
- Calcium channel openers - Repolarization time unchanged - Ex. adenosine |
|
|
Alpha receptor |
- Located in the vessels of the skin, muscles, kidneys, and intestines - Stimulation causes vasoconstriction of peripheral arterioles |
|
|
Beta 1 |
- Located in the cardiac tissue - Stimulation causes increased HR, conduction, and contractility |
|
|
Beta 2 |
- Located in vascular and bronchial smooth muscle - Stimulation causes vasodilation of peripheral arterioles and bronchodilation |
|
|
Beta blockers |
- Decreases HR, BP - Slows conduction through the SA and AV nodes - Decreases force of contraction - Decreases myocardial O2 consumption |
|
|
Calcium channel blockers |
- Negative inotropic effect - Slows AV node conduction - Dilates coronary and peripheral arterioles - Decreases O2 demand |
|
|
ACE inhibitors |
- Inhibits the conversion of angiotensin I to angiotensin II - Prevents sodium and water reabsorption - Prevents vasoconstriction |
|
|
Numbers method of calculating HR |
300, 150, 100, 75, 60, 50 |
|
|
Sinus pause |
< 3 sec |
|
|
Sinus arrest |
> 3 sec |
|
|
Sinus exit block |
If the regular rhythm can fit perfectly within the block |