![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
94 Cards in this Set
- Front
- Back
|
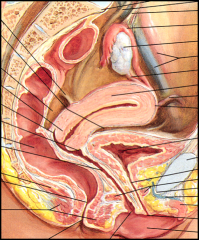
Space of Retzius |
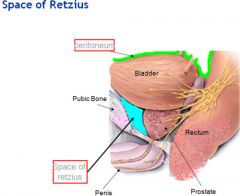
AKA Retropubic space -formed by transversals & extraperitoneal fascia -Anterior to bladder |
|
|
Abdominal or pelvic masses will displace the bladder where? |
Anteriorly or inferiorly |
|
|
Vesicouterine Pouch |
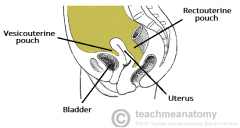
AKA anterior cul-de-sac -space posterior to bladder, anterior to uterus |
|
|
Posterior Cul-de-sac |
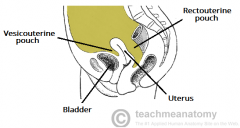
AKA Pouch of Douglas or Retctouterine
-formed by peritoneum extending to posterior fornix of vagina -posterior to uterus |
|
|
Sacrum |
-posterior to pelvis (spine) |
|
|
Coccyx |
-posterior to pelvis (very end of spine) |
|
|
Innominate Bones |
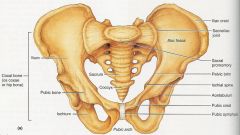
AKA Iliac Bones -anterior and lateral to pelvic space |
|
|
True and False Pelvis |
made up by drawing an imaginary line from sacral prominence to upper portion of symphysis pubis |
|
|
False Pelvis |
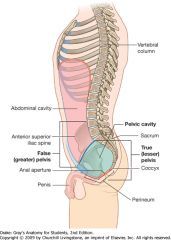
-above plane; bounded by iliac wings -support the intestines |
|
|
True Pelvis |
-below plane -pelvic inlet: bounded by pubic bones ant and sacral prominence post -pelvic outlet: bounded by ischial tuberosities laterally and coccyx posteriorly |
|
|
What's located in the true pelvis in a nongravid patient? |
-uterus -ovaries -anexa |
|
|
In a nongravid patient the uterus is posterior to what? |
-bladder & small bowel |
|
|
How can we create a window for pelvic anatomy sonographically? |
-as the bladder fills, the dome extends into false pelvis and displaces bowel |
|
|
Osseous ligament & the four kinds |
-pelvic ligament that support boney structures -sacroiliac: attaches sacrum and iliac -sacrosciatic: sacrum, iliac& coccyx -sacrococceygeal: sacrum& coccyx -pubic: attaches pubic uterus |
|
|
Suspensory ligament & the four kinds |
-support the uterus -cardinal -broad -sacro-uterine (uterosacral) -round |
|
|
Cardinal (suspensory ligament) |
-primary support system for uterus -superior and lat from uterus -inferior from vagina |
|
|
Broad (suspensory ligament) |
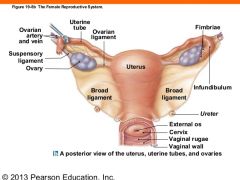
-attach to each pelvic side wall -laterally from each side of uterus |
|
|
Sacro-uterine (suspensory ligament) |
-attaches to the uterus at the internal os (opening) to the sacrum |
|
|
Round (suspensory ligament) |
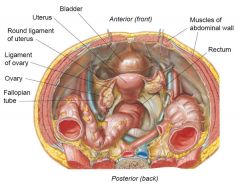
-attaches uterine cornu to ant pelvic wall -btw broad ligaments ant and inf to fallopian tubes (should not see these!) |
|
|
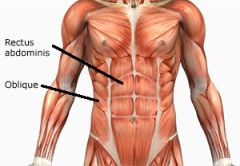
What are the three False Pelvis Muscles (Abdomen-pelvic) |
-Rectus Abdominis -Psoas Major -Iliacus |
|
|
What are the four True Pelvis Muscles? |
-Levator Ani -Coccygeus -Obturator Internus -Piriformis |
|
|
Rectus Abdominis |
-from costal margin to symphysis pubis |
|
|
What is the major cause of "mirror imaging artifact" in gravid patients? |
Rectus Abdominis |
|
|
Iliacus |
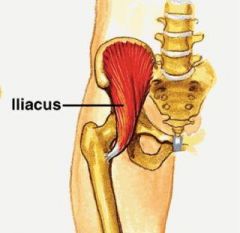
-forms iliac fossa on both sides -arises at iliac crest, extends inf until merges with p. major |
|
|
Psoas Major |
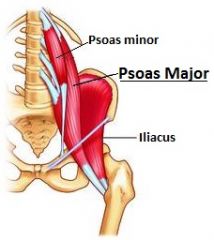
-extends from T12 lat and ant through lower abd -originates in abd into true pelvis -In TRV: bullseye appearance |
|
|
What's the primary purpose of the true pelvis? |
Hold pelvic organs in place |
|
|
What's the most inferior structure of the pelvic cavity? |
Pelvic diaphragm -can be visualized on TA if angle inf |
|
|
Levator Ani |
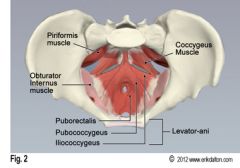
-bilateral muscle -coccygeus, lleococcygeus, pubococcygeous -attaches to pelvic side wall, then extends medially and fuses to opp side -forms pelvic floor |
|
|
Obturator Internus |
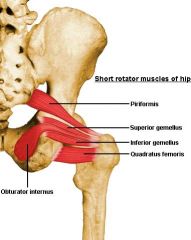
-triangular muscle on lateral pelvic wall -from anterolateral, passes through lesser sciatic foramen, inserting into greater trochanter |
|
|
Piriformis |
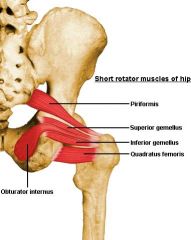
-found on pelvic side wall -from sacrum btw pelvic sacral foamen -inserting into greater trochanter -US: viewed post within pelvis |
|
|
CIA (Common Iliac Artery) |
-ant and medially to psoas m. |
|
|
What does the CIA bifurcate into? |
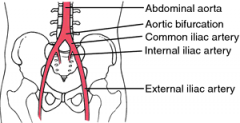
EIA (exteral) and IIA (internal) (aka hypogastric A.) |
|
|
What does the EIA feed? IIA? |
EIA: lower limbs IIA:pelvic viscera, wall, perineum |
|
|
Do the EIA & IIA have a high or low impedance flow? |
high |
|
|
Uterine Artery |
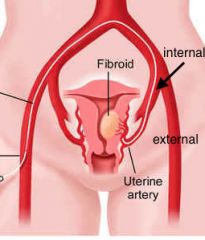
-terminal branch of IIA -ascends along lat portion of ut giving off several branches to feed myometrium -high velocity, high resistance |
|
|
Uterine plexus of veins |
AKA Venous Plexus -"varicose veins" on US -along uterine body -much longer than corresponding artery |
|
|
Ovarian Artery |
AKA Gondal Arteries -primary blood supply to ovaries -dop waveform vary with cycle |
|
|
Just before ovulation and secretory phase, do we have a high or low resistance? |
low |
|
|
High or low resistance for a Dormant Ovary? |
high |
|
|
Urinary bladder |
-musculomembranous sac serves as reservoir for urinary -inferior -distends with filling into true pelvis displaying pelvic structures |
|
|
What are the three tissue layers of the urinary bladder? |
-outer epithelial layer (skin) -middle musculaus layer -inner mucosal layer |
|
|
What does the urinary bladder look like on US? |
-wall is echogenic with uniform thickness |
|
|
Can you see the eval mucosa of the urinary bladder with a full or empty bladder? |
-empty -when empty should be very thick |
|
|
Urethra |
-excretion of urine -arises inf mid portion of UB |
|
|
Internal Urethral Sphincter |
-thickened area of bladder wall surrounding urethra at bladder wall |
|
|
Ureters |
-muscular tubes 25-30cm long -course is important bc surrounding pelvic structures can cause problems in UB and kidneys |
|
|
Vagina |
-hypoechoic tubular structure with echogenic lumen 7-10cm long -extends from Cx to Introitus (ext entrance to vag) -composed of smooth muscle, elastic, connective tissue |
|
|
Fornices |
-blind pouch (goes nowhere) |
|
|
Posterior Fornix |

-posterior aspect of external cx -most common site for free fluid |
|
|
Lateral Fornix |
-lateral aspects of external cx -cause shadowing on transverse cx image |
|
|
Anterior Fornix |
-anterior aspect of external cx |
|
|
Ovaries |
-ovoid shaped -suspended by ligaments -location is variable |
|
|
Nulliparous |
-someone that's never been pregnant -ovaries are situated in ovarian fossa AKA Fossa of Waldeyer |
|
|
How many blind pouches do we have? |
-posterior (most common spot for free fluid) -anterior -2 lateral |
|
|
Suspensory ligament |
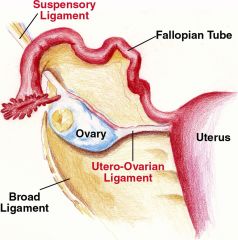
-fold of peritoneum that arises from pelvic sidewall and contains ovarian vessels& nerves |
|
|
Ovarian ligament |
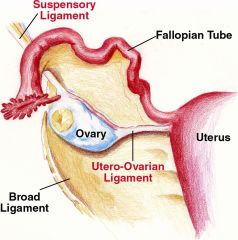
-extends between pole of ovary and ipsilateral uterine body |
|
|
Mesovarium |
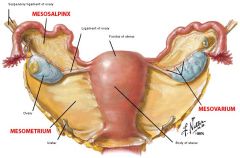
-attach ovary to posterior layer of broad ligament |
|
|
What are some things that cause different size ovaries? |
-age -menstrual cycle -parity |
|
|
What is the size of an ovary for pre-menarche patient? |
3.0cm3 |
|
|
What is the size of an ovary for post-menstrual patient? |
5.8 cm3 |
|
|
Uterus |
-muscular, suspended by ligaments in midline of true pelvis |
|
|
Fondus |
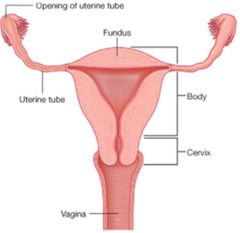
-most superior aspect of uterus above insertion of FT; lateral portions form cornu (horns) of uterus |
|
|
Body |
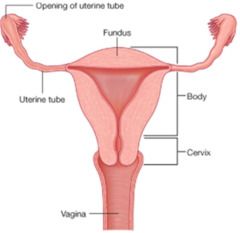
AKA Corpus -largest portion of uterus |
|
|
Cervix |
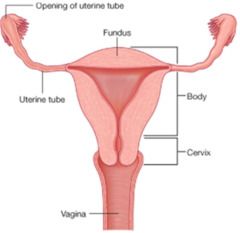
-uterine neck; more fibrous, less muscular 2-3 cm long in nulliparous patient -anchored at angle of bladder, less moveable than body of uterus Dual blood supply: uterine & ovarian artery |
|
|
Size of prepubescent uterus |
2.8 cm long 0.8 cm AP |
|
|
Size of uterus birth to 4 years |
decreases in size |
|
|
Size of uterus at 8 years |
-begins to grow for many years |
|
|
Size of uterus by reproductive age? |
7 cm long, 4 cm wide |
|
|
Size of uterus Parity Multiparity |
-increases in size for parity -8.5 *5.5 cm |
|
|
Size of uterus in Postmeno |
-usually small 3.5-6.5 cm long 1.2-1.8 cm AP |
|
|
What are the three uterine layers |
-perimetrium (outermost layer) -myometrium (middle layer) -endometrium (innermost layer) |
|
|
Serosa |
AKA Perimetrium (outer layer) -covering of uterus, covers fundas& most of body (Retroperitoneum- anything behind the peritoneum) |
|
|
Muscularis |
AKA Myometrium (middle layer) -inner layer: hypoechoic (subendometrial halo) -middle layer: thicker, more echogenic -outer layer: separated from middle layer by arcuate plexus of arteries&veins |
|
|
Mucous |
AKA Endometrium (inner layer) -varies in thickness and echogenicity dependent on phase of menstrual cycle, parity, age& HRT |
|
|
What's the range of normal thickness of endometrium? |
1 mm - just after menses 6 mm - just before menses |
|
|
The thickness of the endometrium should not exceed what size in a premenopausal women |
14-16 mm |
|
|
The thickness of the endometrium should not exceed what size in a postmenopausal women |
8 mm (4-5 mm with no hx of bleeding/symptoms) (8 mm if on HRT or has had bleeding) |
|
|
Early Proliferative Phase |

Day 5-9 -thin echogenic line |
|
|
Late Proliferative Phase |
Day 10-14 -functional zone thickens due to estrogen -hypoechoic compared to echogenic basal layer |
|
|
Secretory Phase |
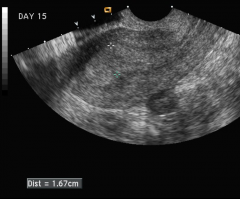
Day 15-28 -functional layer becomes thickened, soft and edematous due to progesterone -increased echogenicity of functional layer, becomes isoechoic to basal layer |
|
|
Version |
-relationship btw cervix and vagina anteversion- form 90 degree angle |
|
|
Flexion |
-relationship btw cervix and uterine body anteflexion- corpus flexed ant on cervix -find uterus with empty bladder |
|
|
Anteverted/Anteflexed |
-corpus, fundus & cx in normal position (NORMAL APPEARANCE) |
|
|
Retroverted |

-corpus/fundus normal position; cx tilted backwards |
|
|
Retroflexed |

-corpus/fundus tilted backwards; cx normal position |
|
|
Retroverted/Retroflexed |

-corpus/fundus and cx all tilt backwards |
|
|
Retroversion& uterine body tilting right or left |
-obscure evaluation of TV on endo and fundus -can appear to have fundal fibroid -normal variant until 14-16 weeks |
|
|
How can you differentiate between a uterus having fundal fibroid and dropout artifact? |
-if there is a lack of displacement of endometrium then yes -lack of contour abnormality |
|
|
Incarcerated Uterus
|
-when fundus fails to rise into flse pelvis from sacral hollow during pregnancy |
|
|
What are the signs and symptoms of a patient with a incarcerated uterus?
|
-multiple ER visits btw 13-17 wks (UTI, severe pelvic pain/abdominal pain) |
|
|
What are the three findings on ultrasound of a patient with a incarcerated uterus? |
-mom UB ant to uterus (should be inf) -soft tissue structure (cx) visualized btw UB and pregnancy |
|
|
What will happen if a incarcerated uterus is not diagnosed& what will happen if it is?
|
Not diagnosed: spontaneous abortion or uterine rupture Diagnosed: manual reposition of uterus |
|
|
Fallopian tubes
|
-10 cm long -lies sup potion of broad ligament |
|
|
What are the four parts of the Fallopian tubes |
-Isthmic-longest portion; connects intramural and ampullary -Ampullary: (fimbriated) open portion of tube adjacent to ovary -fimbria: surround ovary and capture ovum -ostium: open end into peritoneal cavity -Infundibulum: inner, funnel shaped cavity of ampullary portion |